
Abstract
Bone marrow lesions (BMLs) are typical findings in magnetic resonance imaging present in different pathologies, such as spontaneous insufficiency fractures, osteonecrosis, transient BML syndromes, osteoarthritis, and trauma. The etiology and evolution of BMLs in multiple conditions remain unclear. There is still no gold standard protocol for the treatment of symptomatic BMLs in the knee. The biologic augmentation by Osteo Core Plasty™ is a new treatment modality showing promising results reducing pain with the aim to stop the progression of the disease. The purpose of this prospective study is to report the clinical outcomes and safety of Osteo Core Plasty for the treatment of symptomatic BMLs in the knee. Fifteen patients with symptomatic BMLs of the knee treated with the Osteo Core Plasty technique were included and followed prospectively for a minimum of 12 months. Each patient was evaluated before the surgery and respectively at 6 and 12 months using the Tegner Score, Marx Score, the International Knee Documentation Committee, the Knee Injury and Osteoarthritis Outcome Score divided in pain, activity daily living and quality of life subscale, and the Visual Analog Scale for pain. All clinical scores except Tegner and Marx score showed an overall statistically significant improvement through the entire follow-up (P < 0.05) and a significant improvement (P < 0.05) between each follow-up period (T0 vs. T1; T0 vs. T2; T1 vs. T2). No complications were reported. These preliminary results confirm that biological subchondral bone augmentation by Osteo Core Plasty technique is a safe and effective minimally invasive treatment option for symptomatic BMLs in the knee at 1-year follow-up. There is still a need for high-quality randomized controlled trials studies and systematic reviews in the future to enhance further treatment strategies in preventing or treating BMLs of the knee.
Introduction
The subchondral bone is a structure present underneath articular cartilage. It is responsible for cartilage nutrition and plays an essential role in the healing of chondral lesions. It consists of two major parts: the bone plate and the spongiosa [1]. Focal changes in the subchondral bone, termed bone marrow lesions (BMLs), are features detected by magnetic resonance imaging (MRI). In patients with knee osteoarthritis (OA), BMLs can correlate with faster joint degeneration [2,3] and increased pain [4,5].
The initial changes that occur under the articular cartilage at the subchondral bone are highly relevant as they become possible mediators of pain and structural progression in OA and may aggravate pathology, including augmented subchondral bone thickness, diminished flexibility, and trabecular bone density underneath the subchondral plate. Once osteochondral integrity becomes fragile, the barrier between intra-articular and subchondral compartments is lost. This exposes the subchondral bone and its nerves to imbalanced biochemical and biomechanical influence [6,7]. Although the mechanisms are still debated, the pain also may result from impaired venous drainage due to repetitive microtrauma [8,9]. Biological interventions to osteochondral injuries are becoming increasingly researched and may prove beneficial in addressing common concerns [10,11].
High-quality bone marrow is a readily available source of mesenchymal stem cells (MSCs), hematopoietic and endothelial progenitor cells, monocytes, macrophages, lymphocytes, platelet, red blood cells, and growth factors, including the transforming growth factor-β, platelet-derived growth factor, and bone morphogenetic proteins (BMP-2 and BMP-7), which have anabolic and anti-inflammatory effects [8]. Although high-quality bone marrow is one of the most attractive sources of MSCs, several aspects, such as the amount of aspirate, need further exploration. Bone autograft augmentation can deliver structural support and biologically active tissue to the subchondral lesion.
Recent research has focused on using biologic therapeutics to help maintain and improve cartilage health [12 –15]. However, treatment options for subchondral bone are limited. Osteo Core Plasty is a new, minimally invasive procedure for treating subchondral pathologies that has the potential to prevent the progression of OA [16].
This study aimed to analyze the subchondral bone treatment with biologic Osteo Core Plasty™ in patients with symptomatic BMLs of the knee, including Subchondral Insufficiency Fracture of the knee (SIFK), Spontaneous Osteonecrosis of the knee (SONK), and early stages of knee OA. We hypothesize that the Osteo Core Plasty technique could be a safe and effective minimally invasive technique to treat the knee's BMLs, reporting pain relief and improving clinical outcomes at short-term follow-up.
Materials and Methods
Study design
Between December 2017 and January 2020, 15 patients with symptomatic BMLs of the knee, treated with the Osteo Core Plasty technique (core decompression plus a biological subchondral bone augmentation with autologous bone autograft and bone marrow aspirate [BMA]) were included and followed prospectively for a minimum of 12 months. Our institutional review board approved the study, and informed consent was obtained from all patients when they entered the study. The study was conducted following the STROBE Checklist for Case-Series Study [11].
Inclusion criteria: patients between 35 and 75 years with the presence of symptomatic BML on T2-weighted MRI in the subchondral region of the knee (SIFK, SONK, and OA Kellgren–Lawrence grade 2–3) that does not respond to conservative treatment (nonsteroidal anti-inflammatory drugs or physical therapy) for at least 3 months, patients who consented to either treatment modality as per the protocol, and normal blood results and coagulation profile.
Exclusion criteria: rheumatologic disorders, patients with blood diseases, systemic metabolic disorders, immunodeficiency, hepatitis B or C, HIV positive status, local or systemic infection. Smokers, patients with, immunodeficiency, hepatitis B or C, HIV positive status, local or systemic infection, knee malalignment >8°, Knee OA Kellgren–Lawrence grade 4, previous high tibial osteotomy, or cartilage transplantation.
Surgical technique
The procedure is initiated with the patient in the supine position for standard knee arthroscopy under sedation, aseptic conditions, and spinal anesthesia. After performing a small stab incision in the skin using an 11 blade, a BMA needle (Marrow Cellution, Aspire Medical Innovation, Germany) was advanced to the cortex of the iliac crest. The needle was inserted through the cortex using a small mallet. Once the needle passed through the cortex, the sharp stylet was exchanged for a blunt stylet. The needle was then manually advanced 4 cm into the medullary canal. The blunt stylet was replaced with a fenestrated aspiration cannula. The bone marrow was then aspirated following the manufacturer's recommended technique, retracting and aspirating ∼2 mL of bone marrow from five levels for a total of 10 mL of pure BMA.
An aliquot of BMA is used to characterize the product and quantify the total nucleated cells (TNC) using a hematology analyzer (Horiba ABX Micros 60), and also another sample is sent to the lab for counting the number of colonies forming units (CFU-f).
Additionally, an 8 G trephine needle with a sharp, unique tool (bone extractor) is used to harvest a couple of bone dowels using the same stab incision, depending on the severity and size of the lesion treated (Figs. 1 and 2).

Osteo Core Plasty surgical instruments [35].

Image showing the biological and structural components of the technique. The bone marrow aspirate and the bone dowels.
Before the BMA injection, any concomitant abnormalities such as chondral lesions, meniscal tears, and ligament lesions should be addressed and treated. Limb alignment plays a crucial role in treating BMLs; therefore, any abnormalities should be treated first. A 30° 4.0 mm arthroscope (Arthrex, USA) is used to perform a comprehensive arthroscopic examination and treatment of additional intra-articular pathologies. Anteroposterior and lateral fluoroscopic images of the treated knee joint, cross-referenced with the MRI study, are used to place the guide pin precisely in the subchondral bone pathology (Fig. 3). A cannula is then placed over the guide pin, which is subsequently removed. It is left for a few minutes in the bone to prevent BMA leakage and perform core decompression.

Intraoperative anteroposterior and lateral fluoroscopic images of the treated knee joint showing the trocar placed precisely into the bone marrow lesion.
Furthermore, two or three bone dowels are inserted into the cannula and pushed through into the subchondral lesion by a blunt trocar. Then, 7 cc of BMA are inserted through the cannula into the treated area. A final arthroscopic look is performed to confirm the lack of intra-articular leakage.
Postoperative protocol
The postoperative protocol must be adjusted according to the concurrent procedures conducted during surgery. The most important aspects of early postoperative rehabilitation are pain control, maintaining the range of motion, and preventing muscle atrophy. Touchdown weight-bearing is allowed at 3–4 weeks, postoperatively. Full weight-bearing is achieved at ∼6 weeks. After the procedure, continuous passive motion and cryo-cuff are immediately applied to lessen the pain and swelling and maintain the joint fluid motion. On the 2nd day after the procedure, isometric and isotonic exercises are introduced. Pool exercises can be initiated after the wounds are healed to regain a normal gait pattern.
Clinical evaluation
The clinical follow-up was performed by independent clinicians who were not involved in the index surgery. The clinical evaluation consisted of evaluating each patient's Tegner Score, Marx Score, the International Knee Documentation Committee (IKDC), the Knee Injury and Osteoarthritis Outcome Score (KOOS) divided in pain, activity daily living (ADL) and Quality of Life (QOL) subscale, and the Visual Analog Scale (VAS) for pain before surgery (T0) and respectively at 6 (T1) and 12 (T2) months after surgery.
Statistical analysis
A total sample of 15 patients was estimated to be adequate to detect a 1.5 change in Tegner Activity score among preoperative and two follow-up periods with an overall alpha of 0.05, a power of 0.80, a standard deviation of 1.5.
Summary statistics were reported as absolute frequency, and percent change for categorical variables or continuous variables, like the median and interquartile range (IQR), were not normally distributed. First, to assess whether scores differed during the study period, a Friedman test was performed. Second, to further investigate score differences between subsequent periods (T0 vs. T1, T0 vs. T2, T1 vs. T2), a Wilcoxon signed ranks test with Bonferroni adjustment for multiple time comparison was used. Third, subgroup analyses by body mass index (BMI) and age, both dichotomized at their rounded median value, were conducted. A Wilcoxon–Mann–Whitney test was performed to test score differences between young and old patients or between groups with low and high BMI, while a Wilcoxon signed ranks test with Bonferroni adjustment was used to evaluate score differences between subsequent periods (T0 vs. T1, T0 vs. T2, T1 vs. T2) within the same subgroup. Lastly, correlation among scores and sociodemographic characteristics were estimated and testing using Spearman rank correlation. A P value <0.05 was considered statistically significant. All analyses were performed in R version 3.6.1.
Results
A total of 15 patients with a median age of 54 years (IQR 51.99–70.97) were included in the study. Demographic data are reported in Table 1.
Demographic Data
BMI, body mass index; IQR, interquartile range; LFC, lateral femoral condyle; LTC, lateral tibial condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau.
Clinical outcomes
All clinical scores except Tegner and Marx score showed an overall statistically significant improvement through the entire follow-up (P < 0.05) and a significant improvement (P < 0.05) between each follow-up period (T0 vs. T1; T0 vs. T2; T1 vs. T2). Detailed results are reported in Table 2.
Clinical Outcomes
Statistically significant value.
ADL, activity daily living; IKDC, International Knee Documentation Committee; KOOS, the Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life; VAS, Visual Analog Scale for pain.
We did not find any adverse event or complication during the follow-up period in this cohort of patients, concluding that the procedure is safe.
Subgroups analysis
Age
No demographic differences were noted between the two groups divided by age (<55 vs. ≥55 years) (Table 3). Clinical comparison between the two groups showed a preoperative difference for Marx Score with higher value in younger patients. Furthermore, both groups showed significant improvement in IKDC and KOOS-QOL (P < 0.05), while the younger group reported a significant improvement in VAS, while the older group reported a significant improvement in KOOS, KOOS-pain, KOOS-ADL, and KOOS Sport.
Comparison Between Under and Over 55 Years of Age Groups
Statistically significant value.
ADL, activity daily living; IKDC, International Knee Documentation Committee; KOOS, the Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life; VAS, Visual Analog Scale for pain.
Body mass index
No demographic difference was noted between the two groups divided for BMI (<25 vs. BMI ≥25) (Table 4). Patients with higher BMI reported a higher IKDC at T1, a higher KOOS at T0 and T1, a higher preoperative KOOS-Pain and KOOS-Sport (P < 0.0.05). Both groups showed significant improvement in IKDC, KOOS, but only patients with BMI ≥25 reported improvement for KOOS-Sport, KOOS-QOL, and VAS (P < 0.05).
Subgroups Analysis Divided for Body Mass Index
Statistically significant value.
ADL, activity daily living; IKDC, International Knee Documentation Committee; KOOS, the Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life; VAS, Visual Analog Scale for pain.
Correlations
All the statistically significant correlations are reported in Fig. 4.
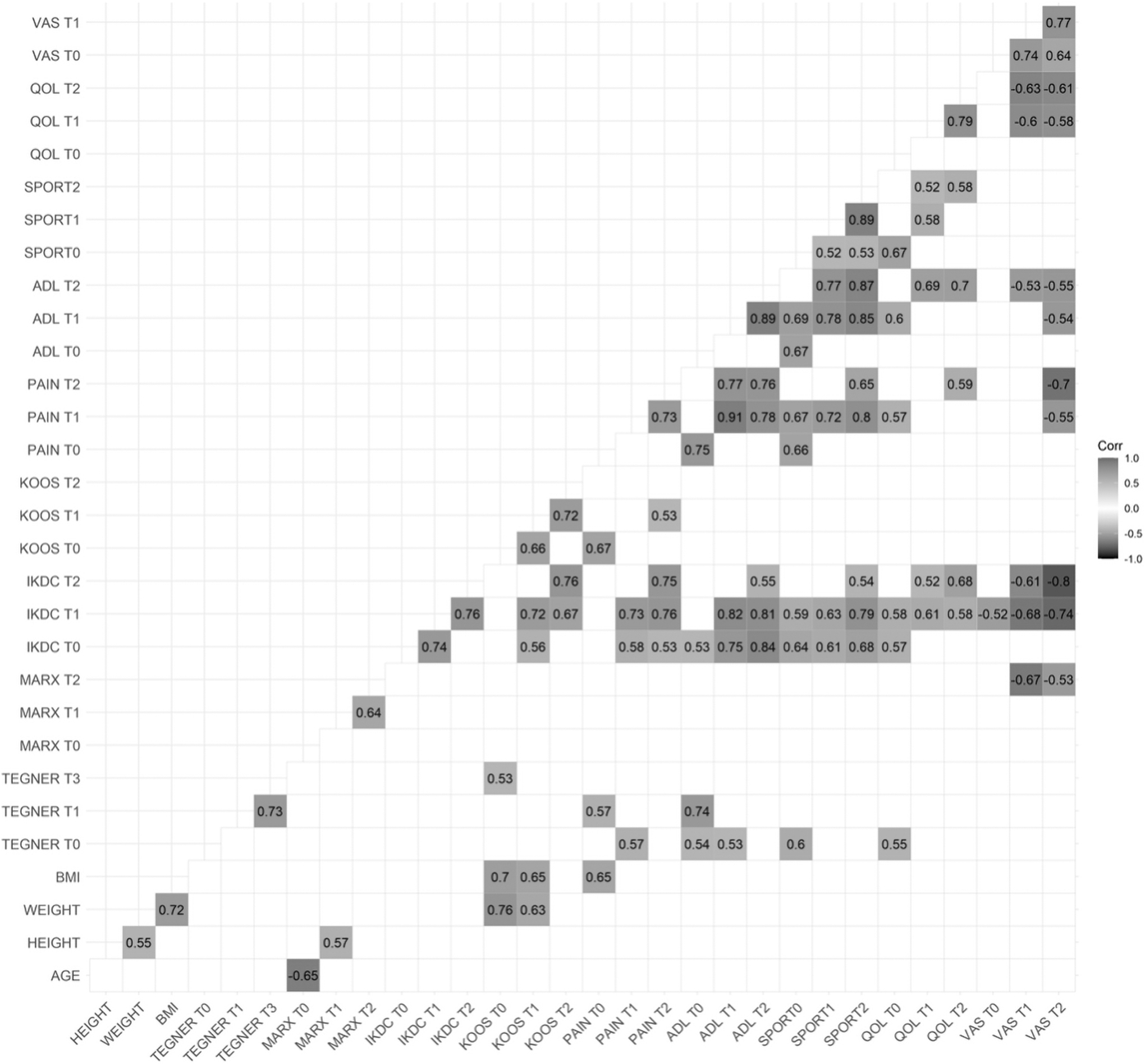
Graph illustrating significant correlations within the patient cohort. ADL, activity daily living; BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, the Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life; VAS, Visual Analog Scale for pain.
The MRI follow-up also demonstrated a significant improvement of the BML at 12 months after in all patients (Figs. 5 –7).

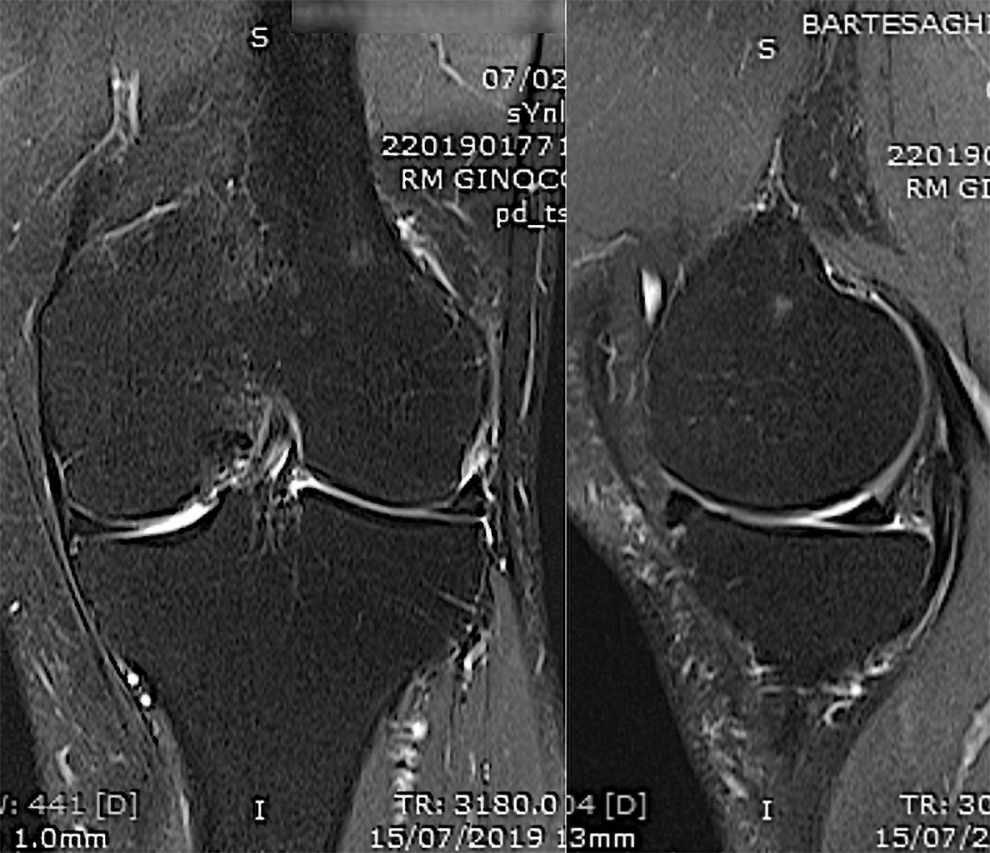
Pretreatment coronal and sagittal views of knee MRI. BML in the medial femoral condyle of the knee [35]. BML, bone marrow lesion; MRI, magnetic resonance imaging.

Two months post-treatment, coronal and sagittal views of knee MRI showed an improvement of the BML in the medial femoral condyle of the knee treated with Osteo Core Plasty [35].
One-year post-treatment, coronal and sagittal views of knee MRI showing the BML resolution in the knee treated with Osteo Core Plasty [35].
Discussion
This study's most important finding is that biological subchondral bone augmentation by the Osteo Core Plasty technique is a safe procedure with no adverse events and significantly reduced pain and better joint function. In addition, MRI showed resolution of the BMLs at 6 and 12 months follow-up, regardless of age and BMI. The current study supports the current trend of treating symptomatic BMLs. The natural history of BMLs is progressive joint degeneration. Its presence has been linked with pain, worsening cartilage degeneration, and other intraarticular pathologies [17].
The number of MSCs present in the subchondral bone decreases with age and the OA joint [18]. Patients with BMLs have a bad prognosis, with accelerated progression to the need for joint replacement [19 –21]. Approximately one-third of the patients with SIFK (66 of 223) progressed to total knee arthroplasty [21]. Baseline arthritis, older age, location of SIFK on the medial femoral condyle and medial tibial plateau, meniscal extrusion, and varus malalignment were all associated with progression to arthroplasty [21]. In adults with tibiofemoral OA, the radiographic severity is not the only predictor of symptom evolution. MRI-based research demonstrated that regression of subchondral BMLs after cell therapy had a greater likelihood of postponing total knee arthroplasty than synovitis changes [22]. Compagnoni et al. described a new topographic classification of BMLs into six anatomical regions concerning their location in the distal femur or proximal tibia based on the coronal T2 MRI image of 520 patients [23].
Treating subchondral BMLs comprises both biological and structural components. Some biologic approaches like core decompression, autologous platelet-rich plasma (PRP) injections [24,25], adipose derivatives therapy [11,26], and bone marrow cell injections [27,28] are recently utilized. The structural component consists of the subchondroplasty (SCP) aspects such as cement injections [29] or autologous cancellous bone core autograft (as described in the Osteo Core Plasty technique [16].
Sanchez et al. had a significant improvement in all KOOS and WOMAC subscales at 6 and 12 months in an observational study with 60 patients suffering from severe knee OA with a combination of intra-osseous and intra-articular infiltrations of PRP [24]. Gobbi et al. concluded in a recent 2-year international multi-centric study in 75 elderly individuals that 80% of the patients who had K–L grade 2 met Patient Acceptable Symptom State (PASS) treated with autologous microfragmented adipose tissue (AMAT) injection in the knee. The cost analysis of comparing AMAT to total knee arthroplasty demonstrated that total knee replacement (TKR) costs on average 2,000 USD more per point increase in KOOS-Pain; thus, AMAT is relatively cost-effective as a bridging procedure to TKR and should be considered as an option in well-selected patients [11].
Bone marrow aspirate concentrate (BMAC) contains increased amounts of MSCs, platelets containing growth factors, and hematopoietic cells [30]. Each of these more concentrated components contributes to the healing and repairing capabilities of BMAC, enabling it to be a helpful treatment method for subchondral bone and cartilage pathologies. A recent study by Everts et al. concluded that the CFU/f was significantly increased only in the first 10 mL of BMA [31]. This study supported the results by Hernigou et al., who showed that large volume aspirates tend to be infiltrated by significant amounts of peripheral blood, which contains fewer MSCs, leading to lower CFU/f counts [32].
Studies have shown that bone marrow samples containing a relatively high CFU-fs/mL and CD34+/mL can be attained without the need for centrifugation [33,34]. The level of CFU-fs/mL was significantly higher in the Osteo Core Plasty compared to BMACs in a side-by-side comparison from the same patients using the contralateral iliac crest [34]. Osteo Core Plasty had over twice as many CFU-f and only half as many nucleated cells compared to centrifugation techniques. Moreover, the Osteo Core Plasty showed the same numbers of CD34+ and CD117+ cells compared to centrifugation techniques [34].
The small dowels of autologous bone are injected into the affected area to fill the intertrabecular space, thereby inducing improved bone remodeling and delivering additional supportive and biologically active tissue to the subchondral lesion [35].
Hernigou et al., in an randomized controlled trial (RCT) in 120 knees, compared subchondral bone infiltrations with intra-articular injection of bone marrow concentrate MSCs in bilateral knee OA. They concluded that implantation of MSCs in the subchondral bone was more effective in postponing TKA than the intra-articular injection of the same dose in the contralateral knee with the same OA grade [27]. In a new pilot study of a combined subchondral and intraarticular BMAC injective treatment, Kon et al. [28] showed an overall positive outcome in patients with symptomatic knee OA associated with subchondral bone alterations. They presented a reduction of bone marrow edema in MRI at 12 months follow-up.
The SCP technique uses the synthetic bone substitute calcium phosphate to target and fill BMLs of the knee. Previous studies have demonstrated the technique's feasibility to reduce pain and improve function, with a small risk of complications [29]. However, calcium phosphate bone cement has not been shown to promote physiologic bone remodeling and repair in conjunction with natural healing [36,37].
The Osteo Core Plasty technique is a percutaneous subchondral bone augmentation approach that provides biological and structural components to optimize the environment for regeneration. This procedure's principles maintain core decompression to relieve increased intraosseous pressure and stimulate healing using bone marrow cell components, growth factors, and BMPs. In addition, autologous bone graft demonstrates osteoinductive, osteoconductive, and osteogenic properties [17].
Very few studies have evaluated the results after biological subchondral bone augmentation to treat symptomatic BMLs in the knee. This study may settle the basis for understanding the effectiveness and safety of Osteo Core Plasty, especially that it is a simple technique avoiding BMA manipulation.
Our study has some limitations that warrant discussion.
First, our research has no control group to compare patient-reported outcomes and clinical definitions of treatment failure (eg, Minimal Clinically Important Change Score, PASS) to protect the results against bias.
Second, the cohort is composed of a small group of patients.
Third, short-term follow-up. Fourth, we did not analyze the results of the characterization of the BMA's cell components but is planned for further investigation. Lastly, in a Phase 0 pilot study such as this, the initial findings here should be used to design more robust Phase I trials in the near future.
Conclusion
These preliminary results confirm that biological subchondral bone augmentation by Osteo Core Plasty technique is a safe and effective minimally invasive treatment option for symptomatic BMLs in the knee at 1-year follow-up with no reported complications regardless of age and BMI. There is still a need for high-quality RCTs studies and systematic reviews in the future to enhance further treatment strategies in preventing or treating BMLs of the knee.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest. The authors did not receive supplies for the study. No conflict of interest between the authors and the manufacturers.
Data Availability Statement
The underlying data supporting the results of this study can be found are securely maintained in the OASI Bioresearch Foundation, Milan, Italy.
Funding Information
This study was funded by the OASI Bioresearch Foundation, Milan, Italy, and did not receive any external funding. A.M. has received grants, non-financial support and other from Merck KGaA; grants, non-financial support and other from Kolon TissueGene; grants, non-financial support and other from Merck KGaA; grants from Pfizer; grants from European Commission-Innovative Medicines Initiative; grants from European Union Structural Funds administered by the Research Council of Lithuania (Lietuvos mokslo taryba); grants from European Union Structural Funds administered by the Research Council of Lithuania (Lietuvos mokslo taryba); grants from European Commission-Framework 7 (FP7-HEALTH); grants from European Commission-Framework 7 (FP7-PEOPLE) Marie Skłodowska-Curie Program; personal fees from Galapagos-Servier; personal fees from Image Analysis Group; personal fees, non-financial support and other from Artialis SA; personal fees and other from Achē (Achē Laboratrios Farmaceuticos); personal fees and other from Abbvie; personal fees from Guidepoint Global; personal fees from Alphasights; personal fees from Science Branding Communications; personal fees and non-financial support from Pfizer Consumer Healthcare; non-financial support from GlaxoSmithKline (GSK) Consumer Healthcare; personal fees and other from Flexion Therapeutics; personal fees from Pacira Biosciences; other from Genacol; personal fees, non-financial support and other from Sterifarma; other from Henry Stewart Talks; non-financial support from GSK; grants from Versus Arthritis (Arthritis Research UK); personal fees and other from Korean Society for Osteoarthritis and Cartilage Repair; personal fees from American College of Rheumatology; personal fees and other from Spanish Society of Rheumatology; personal fees and other from Heilongjiang Rheumatology Association; personal fees and other from Zhujiang Hospital of Southern Medical University; non-financial support and other from International Cartilage Regeneration and Joint Preservation Society; non-financial support and other from Osteoarthritis Research Society International; non-financial support from AxDev International; other from Gordian Biotechnology; other from UNITY Biotechnology; personal fees and other from Bioiberica; other from The Dutch Arthritis Society (ReumaNederland); other from Kolon Life Science; personal fees from SANOFI; personal fees from European Commission; other from BRASIT/BRASOS, Brazil; other from GEOS, Brazil; other from European Orthopaedic Research Society; other from Brazilian Society of Rheumatology; other from Society for Osteoarthritis Research, India; other from MCI Group, Geneva outside the submitted work.