
Abstract
To date, more than 565 professional astronauts have flown in space, of whom only 11% have been women. Of these, ∼565 have been NASA astronauts, of whom 86% have been men and 14% have been women. This cohort of professional astronauts has been uniquely fit and exceptionally well trained. The advent of commercial spaceflight will see a wider range of individuals enter space, who lie on a variegated continuum of physical fitness, metabolic fitness, disease complexity, drug therapeutics, and genetics. Yet, there are currently little data on individuals of lesser fitness entering space. In addition, the initial planetary missions to Mars will embark without any data associated with such a mission (e.g., 3 years). Even as we begin to gather such data from the initial Mars missions, the cohorts will be small with uncertain generalizability. While spaceflight medicine has grown in sophistication, we are still faced with clear knowledge gaps. This occurs just as the community of space travelers is about to expand and the complexity of planetary missions is at its most ambitious. Fortunately, the advent of comprehensive molecular profiling, including some in mission, allows us to address some of these unknowns by applying complex molecular analytics to individuals and developing personalized countermeasures derived from those analytics.
Introduction
Personalized medicine is the concept that managing a person's health should be based on the individual's specific characteristics. In spaceflight applications, the definition moves beyond health to also include individual safety and performance under the unique conditions of space. 1
In practice, this has evolved to include the individual's specific molecular characteristics, such as the individual genome, epigenome, transcriptome, proteome, metabolome, and microbiome (Fig. 1). This can include: (1) targeted molecular analysis (preselected, limited number of molecular forms), (2) untargeted analysis (broad number of compounds on an exploratory basis), or (3) a combination of the both.
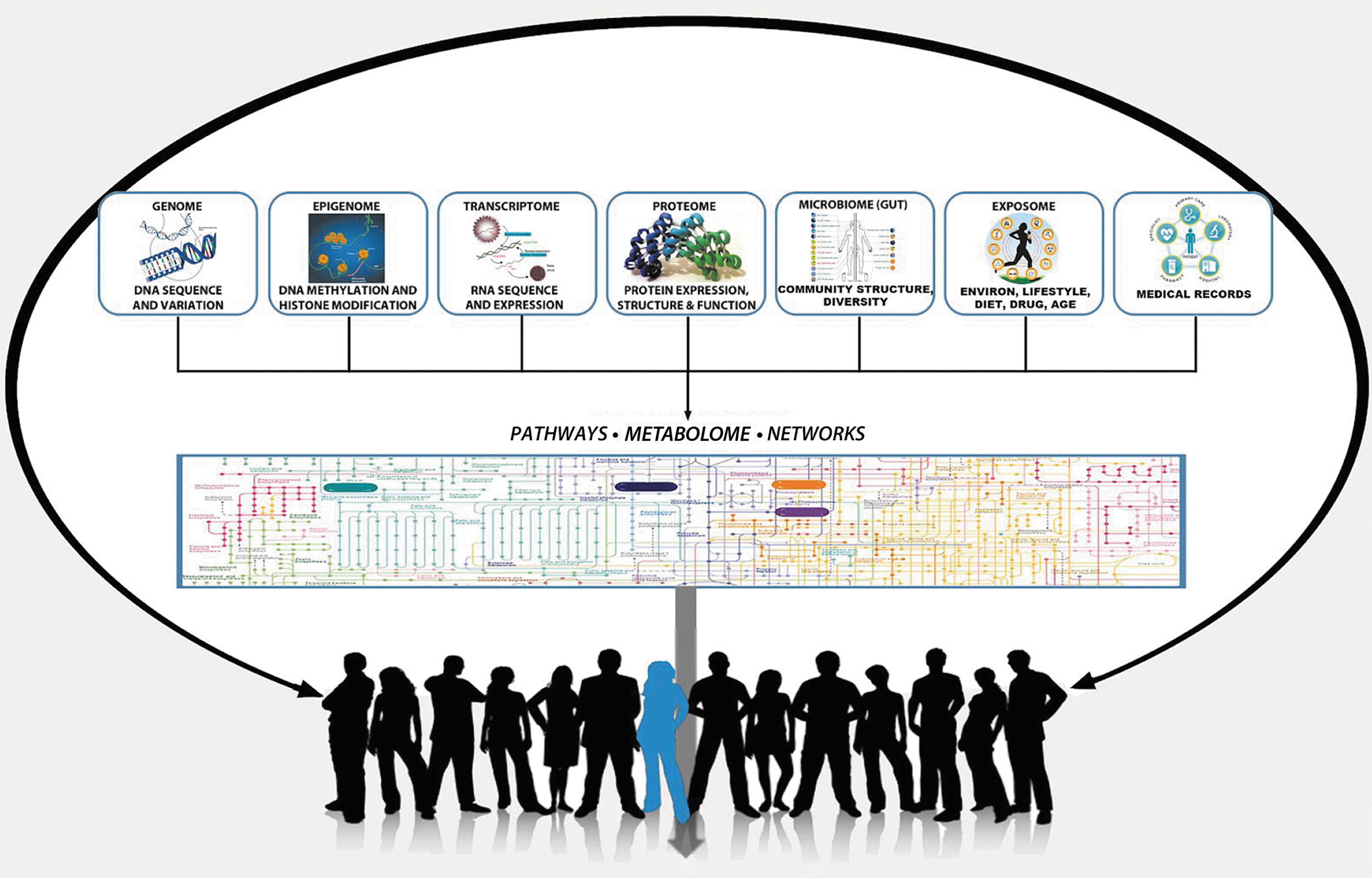
The subdisciplines of multiscale omics. Genome, epigenome, transcriptome, proteome, exposome, and metabolome refer to a continuum of chemical classes that govern all biological processes. Microbiome refers to the sum of individual microbes (and their metabolites) that reside in the gut. Each class consists of thousands of molecular forms. These can now be measured with precision. Following this measurement, a description of the behavior of the biological system can be developed. This can then be used to describe the complexity found within groups (black) or individuals (blue). From the analysis, new hypotheses or countermeasures can be developed. Image credit: Sovaris Aerospace.
The United States National Research Council (NRC) has advanced the term precision medicine, where the focus is on identifying which approaches will be effective for which patients based on genetic, environmental, and lifestyle factors, which is not necessarily focused on individuals. The Council therefore preferred the term “precision medicine” to “personalized medicine.”
In spaceflight applications, the goal truly is personalization, although precision is also sought. Thus, in the present review, the terms personalized medicine and precision medicine are used in a complementary manner. This is done to recognize the fact that the medical approach is necessarily tailored to the person, but that its precision is rooted in the use of molecular profiling to more accurately develop preventive measures, treatments, countermeasures, or training approaches tailored to the individual (Fig. 2). Finally, when the term personalized medicine is used here, its application to human performance is also assumed.
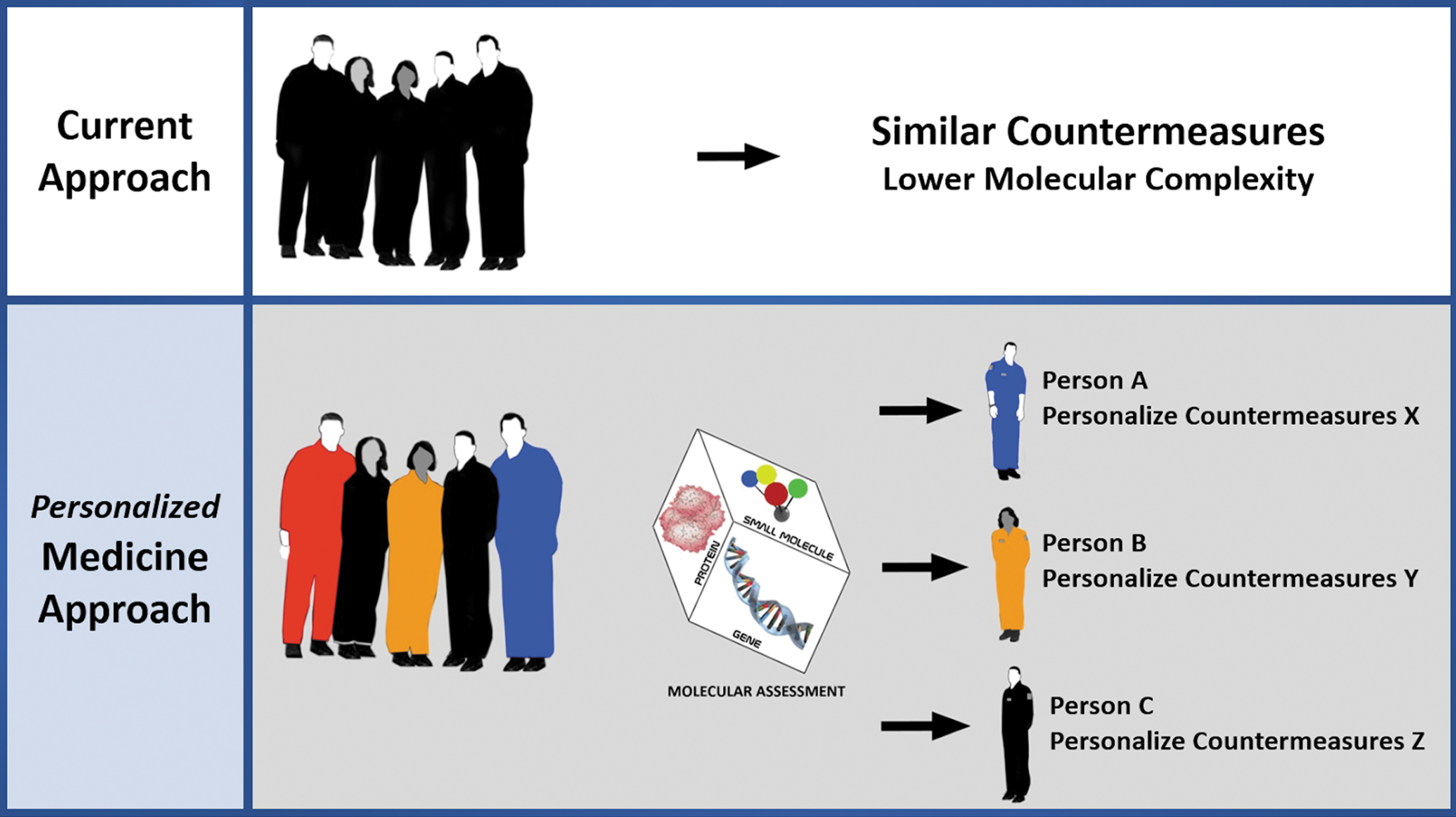
Personalized medicine paradigm for human in space. Modern approaches to space medicine have always incorporated a measure of individualization. However, the concept of personalized medicine is focused on a considerable expansion of the number of molecular features assessed, mapping the feature variance to molecular pathway and network maps, characterization of biological meaning, and derivation of targeted countermeasures. This approach is focused on the principle of incremental gains intended to optimize efficiency of those pathways and networks. The goal is improvement in health, safety, and performance in space. Improved safety of drugs and regulation of metabolism in space are among the early actionable applications. Image credit: Sovaris Aerospace.
A Systems Engineering Model for Personalized Medicine
One can use a systems engineering paradigm as a means to apply a structured approach to the development of personalized medicine for spaceflight participants and crew. In an attempt to better characterize the operating environment, it is important to briefly note the difference between complicated systems and complex adaptive systems. 2 These can be described as follows: (1) Complicated Systems are systems that are hard to define and understand due to scale, coordination, and specialization (e.g., Saturn 5 rocket) and (2) Complex Adaptive Systems are systems that are based on relationships, network effects, connections, and evolution (e.g., the human body).
Complex adaptive systems, such as the human system, cannot be fully decomposed and controlled, due to their complex nature. However, desired outcomes in these systems can be facilitated. To approach, understand, and engineer these outcomes through assessments and countermeasures, different management techniques are required (Table 1).
Differentials in the Systems Engineering Approach to Managing Complex Adaptive Systems a
Reference 2
To facilitate desired outcomes in human systems to the greatest degree possible, it is useful to depart from a highly mechanistic mode of operation toward a methodology that considers the complex and emergent nature of the human system. This table presents one approach to describing these differences and makes general recommendations as to how one can view their management.
Due to the complexity of human systems, it is often noted that the only model that can replicate the relationships, networks, connections, and evolution of the system is the system itself. In place of this type of intractable model (and in an effort to reduce complexity), we propose an input–output rendering to characterize the relationship between (1) inputs, (2) processes (hidden layer), and (3) outputs (Fig. 3). In this model, the output layer generally includes the phenotype consisting of physiology, morphology (form), and behavior (although this can be reduced to any number of specific outputs in practice). Phenotype refers to the observable characteristics or traits.
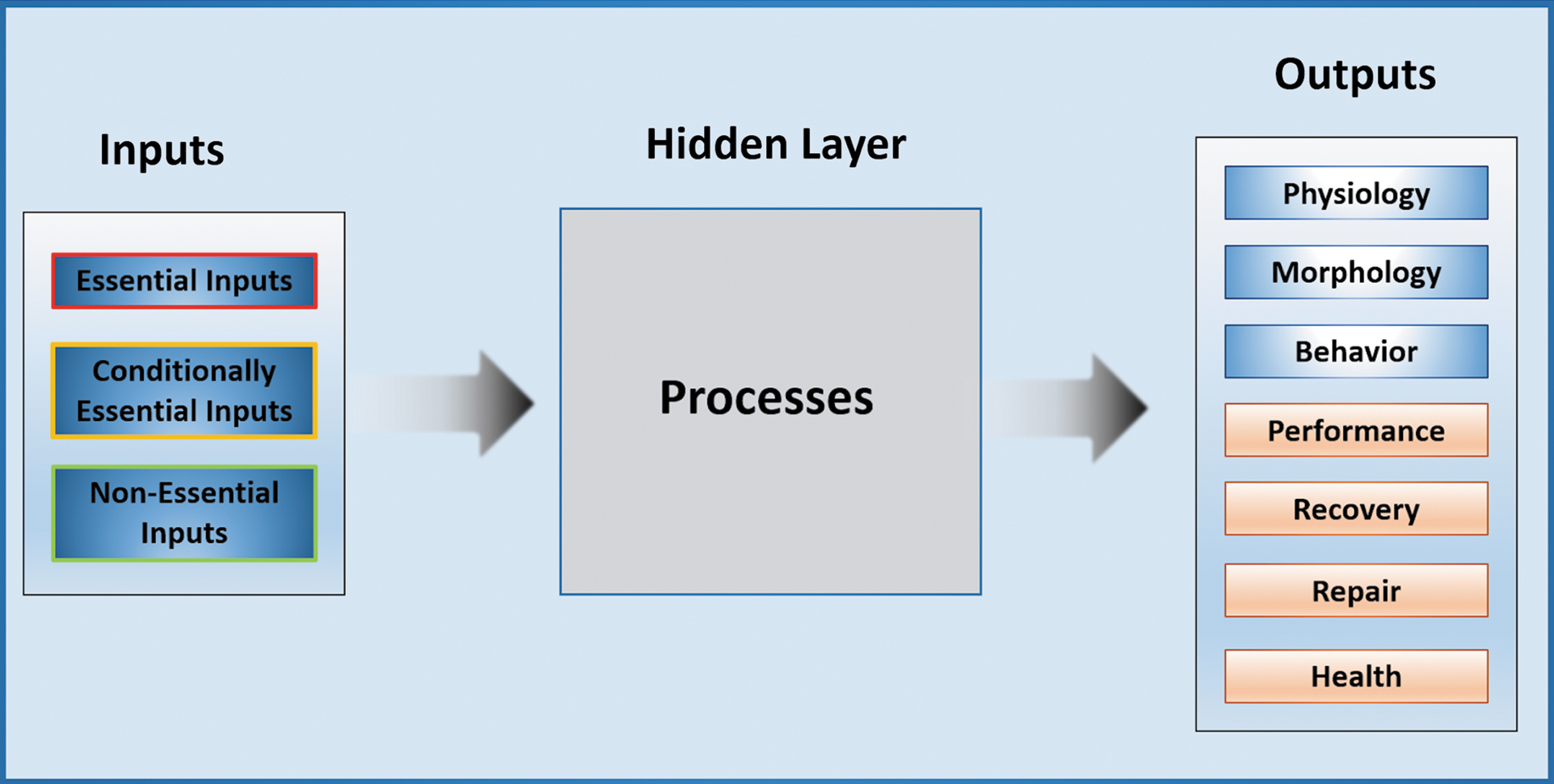
Basic input–output model. Three types of inputs enter the hidden layer (process layer). This layer can be seen as the sum of the biological and chemical processes that govern all human function. Driven by the varied inputs, this process layer is heavily modulated by the genome, epigenome, and feedback from other molecular forms, which influence the adaptive nature of the process. Single elements within the input layer, process layer, and output layer can be increasingly well characterized. This characterization adds precision to the personalized medicine application. Image credit: Sovaris Aerospace.
For the purpose of the specific systems application discussed here, we show an artificial neural network as a schematic representation (rather than as a pattern recognition or predictive modeling tool). In this schematic representation (Fig. 4), we show how (one or more) inputs interact within the hidden layer (process layer), which leads to one or more outputs. The nature of the output is governed by the processes taking place in the hidden layer. This depiction is generally analogous to simple input–output system engineering approaches used in electrical, mechanical, chemical engineering, and other engineering disciplines, as well as machine learning algorithms.
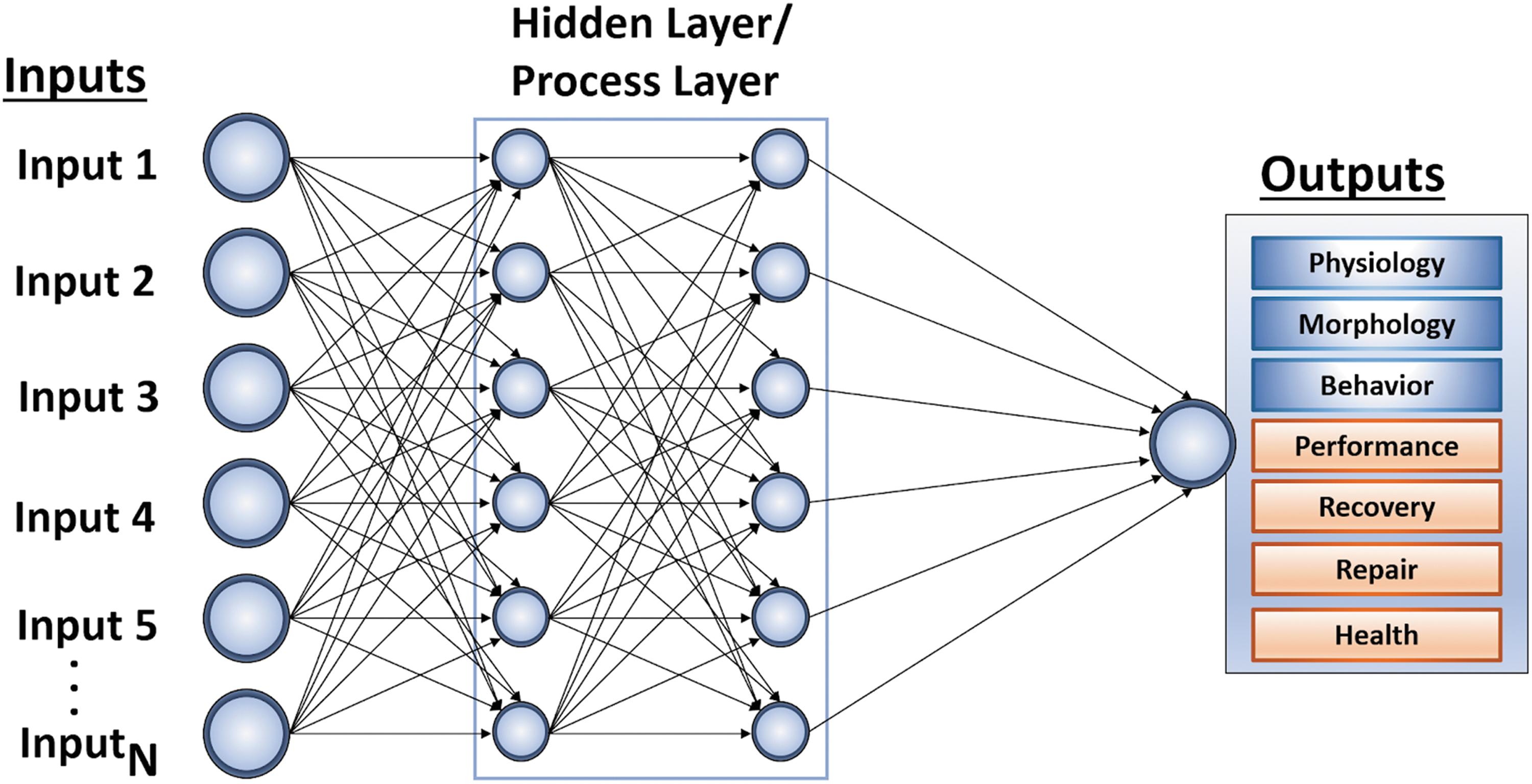
ANN rendering to display the interaction between inputs, processes, and outputs. This feedforward ANN is used here merely to represent a set of relationships, rather than focusing on the traditional use of ANN for modeling, pattern analysis, training, and prediction. It is intended to show how multiple inputs interact across multiple processes to arrive at some output. The goal is to apply precision in characterizing each of the relevant components for the purpose of applying structure to the practice of personalized medicine. ANN, artificial neural network. Image credit: Sovaris Aerospace.
Inputs in the form of essential, conditionally essential, and nonessential elements enter the system (human) and participate in a vast number of molecular networks (hidden layer). This hidden layer contains metabolic pathways and molecular networks spanning a range of processes that vary considerably, based on (1) the status of inputs (deficiency or excess; environmental exposures), (2) the number of converging inputs, and (3) the genetic landscape (genome, epigenome) within this hidden process layer. Each essential input may participate in several hundred distinct metabolic processes.
A personalized medicine approach is rooted in the understanding that the efficiency of these networks strongly impacts health, performance, and safety within a given environment or condition. This represents a novel way of looking at individual spaceflight participant susceptibility, risk, and countermeasure development. In each case of the examples that follow, there are key inputs (coupled with variations in the genetic landscape) that have the potential to significantly modify the human response in space. We can characterize these inputs according to the descriptions of essential, conditionally essential, and nonessential elements shown in Figure 5.
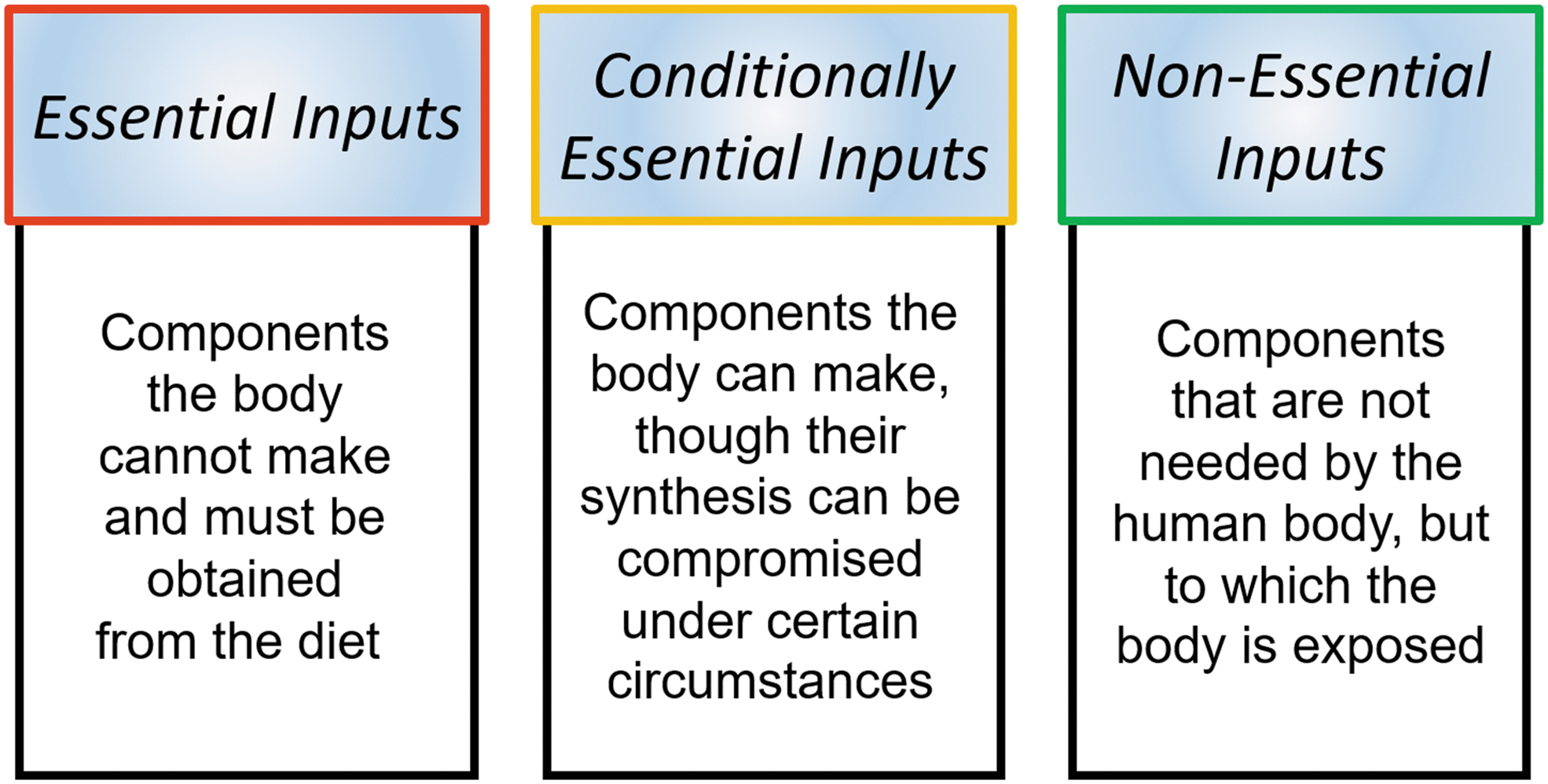
Essential, conditionally essential, and nonessential inputs.
Essential Inputs
Essential inputs refer collectively to the class of small molecules, amino acids, vitamins, fatty acids, minerals, and trace elements that must be obtained from the diet. They cannot be synthesized by the human body. These molecules govern vast molecular networks and processes throughout the human body.
They are collectively referred to as inputs because these are external components that enter the system to collectively influence all metabolic activities. It is tempting to view these micronutrient essential inputs only in general ways and to underestimate the impact of relative states of insufficiency or excess. However, if one views the human in terms of integrated molecular networks and gives the requisite attention to the core metabolic steps in which these essential inputs participate, the true magnitude of small deficits in these inputs can be appreciated. Table 2 illustrates common examples of the number of processes in which selected inputs are individually involved.
Common Essential Inputs and Their Process Involvement
Shown is a representative sample of selected essential inputs and the percentage (number) of the body's enzymatic reactions in which the input participates. The convergence of multiple input deficits can aggregate to scale across an increasing number of molecular networks.
The numbers referenced in the table are often referred to as “participation numbers,” referring to the number of fundamental processes dependent on a given input. The aggregation of one, two, three, or more input deficits (and the sum of their participation influence) can begin to scale significantly across molecular networks and human systems, which can have notable implications for health, safety, and performance.
Case One: Essential Inputs, Genetics, and Visual Problems in Space
Spaceflight-associated neuro-ocular syndrome (SANS) is now one of the most pressing clinical problems associated with spaceflight. SANS describes a series of functional and morphological (shape, form) changes in the eyes of astronauts. SANS is clinically defined by the development of optic disc edema (swelling) during prolonged exposure to the weightless (microgravity) environment. There is mounting evidence that such neuro-ocular changes are related, in part, to disordered one-carbon (1C) (–CH3) metabolism involving vitamin B12, folate, homocysteine, and their related genes.
Approximately 20% of the International Space Station (ISS) crew members on spaceflight missions of 4 months or longer have experienced ocular changes and persistent visual problems on return to Earth. An initial ISS study found that these were correlated with significantly elevated levels of homocysteine, methylmalonic acid, and cystathionine, along with reduced levels of folate and vitamin B12 (all signs of 1C network dysregulation). 3 The metabolite data indicate that a significant proportion of crew members may have associated genetic traits that contribute to disturbed 1C metabolism.
A follow-up study examined ocular changes and genetic polymorphisms (variants) in the 1C molecular network in 49 astronauts. Variants in the genes methionine synthase reductase (MTRR) and serine hydroxymethyltransferase (SHMT1) were found to be associated with visual deficits. Specifically, all the astronauts who inherited two variant copies of the gene MTRR 66GG exhibited choroidal folds (depressions in the white outer layer of the eyeball) and cotton wool spots (fluffy white patches on the retina).
In contrast, none of the individuals with the normal MTRR 66AA genotype had evidence of choroidal folds or cotton wool spots after ISS missions. Of further significance, none of the astronauts with the normal (wild type) SHMT1 (1420TT) genotype had evidence of disc edema after flight. 4 Our projection of the spaceflight-derived 1C SANS data to a simplified input–output model can be seen below (Fig. 6).
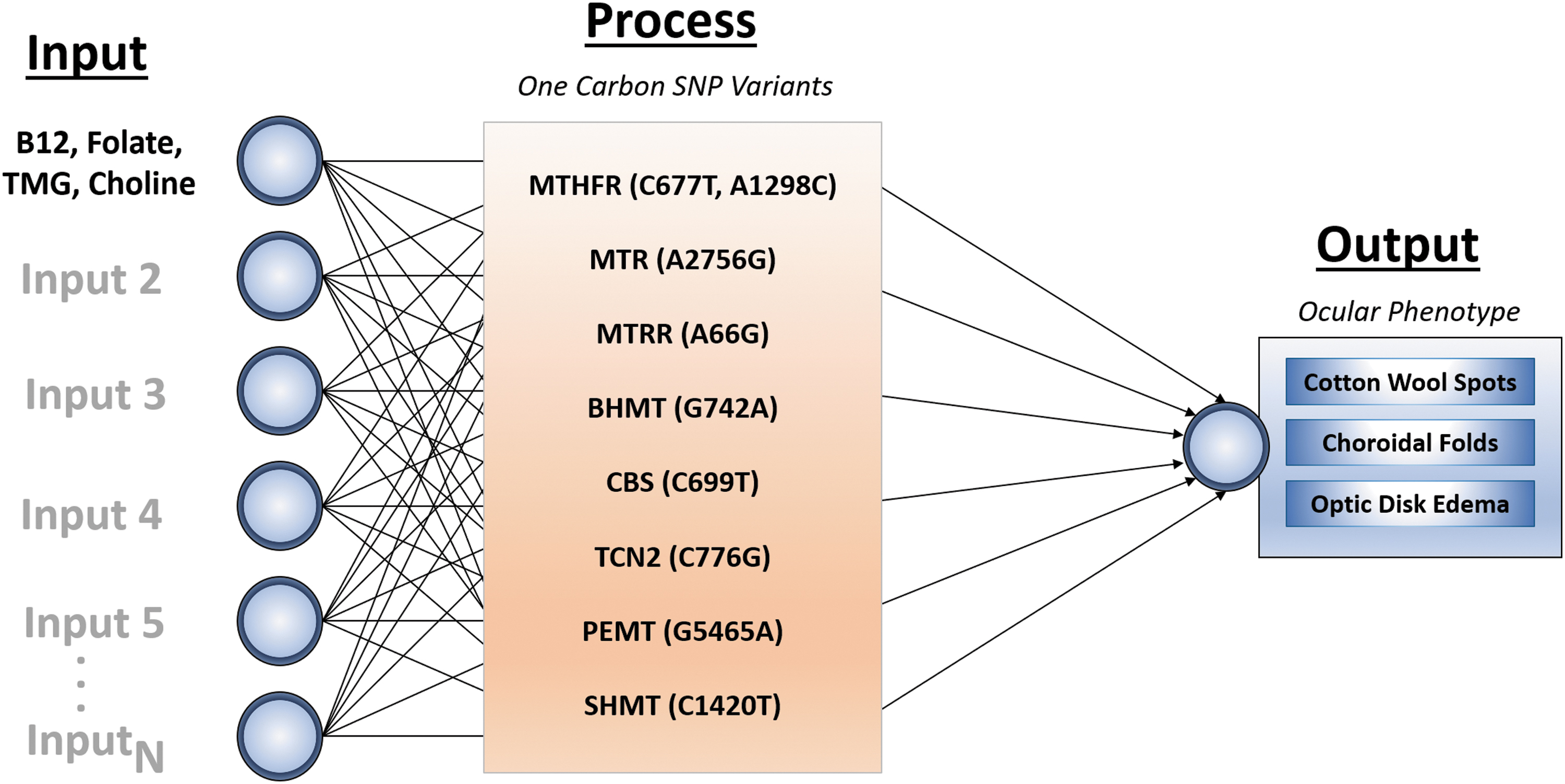
The 1C network in space-associated neuro-ocular syndrome. The primary inputs include vitamin B12, folate, TMG (betaine), and choline. The process layer includes a constrained network of genes affecting 1C metabolism. This layer is built by characterizing genetic variants known as SNPs. An SNP is a substitution on a gene where the “normal” base (letter; ATCG) is replaced by another base. Each gene can be mutated by one or two substitutions (a single variant can be inherited from each parent, leading to a maximum of two variants on a single gene). These substitutions can alter gene function and the function of its resultant protein in notable ways. Alterations (variants) in one or more of these associated genes can have a scaling effect in human systems. (Note: Gene insertions, deletions, and copy number variants can also occur, but these have been left out for simplicity.). 1C, one carbon; SNP, single nucleotide polymorphism; TMG, trimethylglycine. Image credit: Sovaris Aerospace.
These findings represent only one part of the SANS puzzle. But they do provide insight that individual variability can be associated with altered risk and that countermeasure targets can be derived from knowledge of this molecular variability. As a practical matter, we are presently able to measure all the genes in the 1C molecular network. Likewise, the small-molecule inputs and intermediates are easily measured today, using existing clinical chemistry tools.
Conditionally Essential Inputs
Conditionally essential inputs are those molecules that the body can make under optimum conditions, but which it cannot make in sufficient amounts in the absence of a critical precursor or cofactor. The presence of a genetic variant can also alter synthesis of the input, rendering it conditionally essential. Exposure to environmental chemicals or drugs is another influence on conditional essentiality. In all these cases, it may be necessary to provide the preformed end product to attain the desired output. Examples of conditionally essential inputs include:
Glutathione: Glutathione (GSH) is critical to drug detoxification, chemical exposure, and exposure to harsh environments, such as space. Although the body can make it, GSH requires three amino acids in its formation (cysteine, glycine, and glutamic acid).
9
Cysteine is the most limiting of the amino acids and its deficiency (from poor dietary protein quantity or quality) can increase the need for preformed GSH as a countermeasure. Eicosapentaenoic acid and docosahexaenoic acid: These long-chain fatty acids (commonly found in cold water fish) are critical for proper cell membrane architecture, cardiovascular resiliency, brain function, and regulation of inflammatory networks. Humans can synthesize these from the fatty acids found in flax seeds, walnuts, pumpkin seeds, and chia seeds (i.e., alpha-linolenic acid). However, genetic variants of the enzyme (FADS1) required for the synthesis of eicosapentaenoic acid and docosahexaenoic acid (EPA/DHA) from essential precursors can make it necessary that an astronaut receive preformed EPA and DHA (which are not ordinarily essential). We recently reported on the effect of 1 year in space (the NASA Twins Study) on the genes that regulate fatty acid synthesis.
10
Case Two: Converging Variables: Acetaminophen and GSH (Nonessential and Conditionally Essential Inputs)
The analgesic acetaminophen represents an example of the convergence of a nonessential input (acetaminophen), coupled with dependence upon a conditionally essential (and potentially limiting) nutrient involved in drug detoxification (GSH; sulfur groups). Under normal conditions, acetaminophen is partially (15%) metabolized via the enzyme CYP450 2E1. This process leads to the formation of the hepatotoxin (liver toxin) NAPQI (N-acetyl-p-benzoquinone imine). 11 The next critical step in removal of NAPQI is the molecular binding with the conditionally essential nutrient GSH to form an NAPQI-GSH complex. This process normally renders the toxic NAPQI water soluble for safe excretion in the urine (Fig. 7).
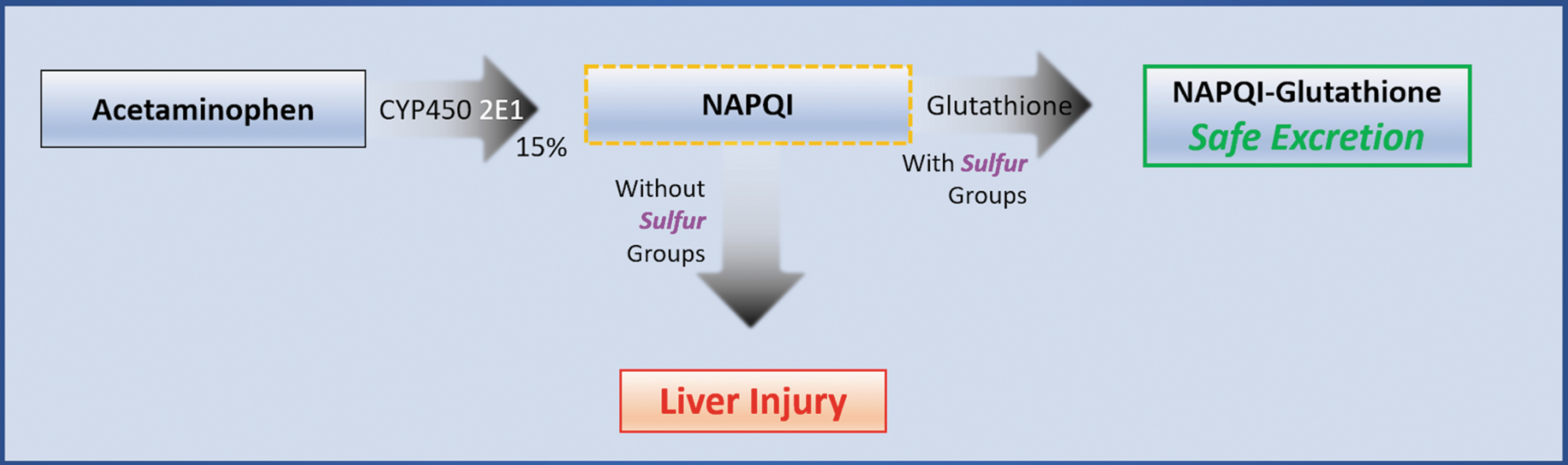
Acetaminophen conversion to NAPQI and removal by glutathione. NAPQI, N-acetyl-p-benzoquinone imine.
It is important to recognize that there must be sufficient GSH to execute this conjugation (binding) with acetaminophen. This step is limited by (dependency upon) the crucial dietary precursors needed to synthesize GSH (cysteine). If cysteine or GSH is in limited supply, the resultant NAPQI can accumulate, exerting highly toxic effects by covalent (strong chemical bonding) reactions with the body's structural and functional proteins. This can lead to liver damage typically associated with acetaminophen use. 12
If GSH depletion is identified through pre-mission blood chemistry (low GSH or low GSH:GSSG ratio), pre-formed GSH or GSH precursors (N-acetylcysteine) can be provided at the dosage needed to assure optimum mission safety and performance. Pre-formed GSH or GSH precursors, such as N-acetylcysteine, can also be provided for long-duration missions. Alternately, those with the genetic variant (CYP450 2E1) can have their mission drug list personalized by using an alternative drug to acetaminophen.
Nonessential Inputs
The term nonessential input refers to those external components (molecules, xenobiotics, radiation) that enter the human body, which have no known essential function, yet they exert a biological effect. This might also be referred to as the “exposome.” Many of these nonessential inputs, such as those in the ambient environment, are beyond our control. Others, such as drugs, clearly fall within our control. Whether controllable or not, these inputs can significantly perturb molecular networks. They can also have significant adverse effects on the essential and conditionally essential inputs. The control or, at minimum, annotation (characterization) of nonessential inputs can be vital to optimum personalization. These inputs can include: (1) drugs, vaccines, biologics; (2) environmental chemicals (xenobiotics); (3) nonessential food components (flavonoids, alkaloids, vasoactive amines, microbiome); (4) radiation; (5) water; (6) air (O2, CO2); and (7) heavy metals (arsenic, cadmium, chromium, lead, mercury, etc.).
Since the refinement of drug therapeutics in space is among the most amenable to the personalized medicine approach, we will explore its application using pharmacogenomics.
Application of Pharmacogenomics in Spaceflight
Pharmacogenomics is the study of gene variants that influence the regulation of drug metabolism. From a practical standpoint, pharmacogenomics is a tool that enables the physician to more precisely tailor a drug to the individual's specific genotype for the purpose of optimizing benefit and minimizing adverse events.
Contemporary pharmacogenomics is used to classify individuals into four subgroups (phenotypes), based on their ability to metabolize a given drug or class of drugs. These include: (1) poor metabolizer (PM), (2) intermediate metabolizer (IM), (3) extensive metabolizer (EM) (now referred to as normal metabolizer [NM]), and (4) ultra-rapid metabolizer (UM).
The clinical profile associated with drug metabolism is strongly dependent on the number of variations on one or more genes in an individual astronaut. For example, possessing two variant alleles in a CYP450 enzyme results in loss-of-function. This is the PM type. Conversely, possessing multiple copies of the same DNA strand containing the wild-type CYP450 gene can result in gain-of-function. This is the UM type. Possessing a single variant allele would yield an intermediate type.
In general, gain-of-function variants lead to increased drug clearance and lower drug concentrations. Loss-of-function variants lead to reduced drug clearance and increased drug concentrations. If the drug is a pro-drug (meaning the administered drug must be metabolically converted to its active form), the converse is true. 13 UMs experience rapid metabolism of an active drug, little or no drug effect, and poor clinical outcomes. Conversely, PMs will experience slow (or no) drug conversion, high plasma levels of the drug, and increased adverse events.
As a practical matter, the PM and UM phenotypes would deserve first-order attention among space medicine physicians. These are less common phenotypes, but the likelihood of poor outcomes is greater in these cases without an adjustment to the drug's recommended usage. These are also the circumstances where the pursuit of alternate drugs addressing the same clinical endpoint can be useful.
We can use codeine as an example of a drug where understanding the personal genotype is essential to making the proper drug selection for spaceflight.
Case Three: Codeine to Morphine Conversion in Personalized Drug Therapy
One can regulate the impact of a nonessential input (drug) by characterizing the genetic features of the input's metabolism and refining the selection of that input accordingly. Codeine is among the opioid analgesics that are used to relieve mild-to-moderate severe pain. The enzyme CYP450 2D6 converts codeine to the active metabolite morphine, which is responsible for the analgesic effects of codeine (Fig. 8).

The conversion of codeine to morphine. The conversion of codeine to morphine is a single step process. This is governed by an enzyme called CYP540 2D6. This enzyme is regulated by the CYP540 2D6 gene. Gene variants in individuals can be characterized with genetic sequencing methods readily available to the clinician today.
In those who carry two inactive copies of the CYP450 2D6 gene (PMs; ∼10% conversion to morphine), there may be inadequate pain relief, due to inadequate morphine formation. Conversely, those who carry more than two functional CYP450 2D6 copies more rapidly and completely convert codeine to morphine. These are the UMs (40%–50% conversion to morphine). In this case, even normal doses of codeine may lead to symptoms of morphine overdose: shallow breathing, sleepiness, confusion, sweating, nausea, vomiting, constipation, dizziness, drowsiness, laryngospasm, and others. 14 These symptoms would be obvious threats to mission performance and human safety.
In the space medicine environment, we can readily determine the genotype of an individual regarding codeine to morphine metabolism (Fig. 9). Once the individual's genotype is determined, we would immediately remove codeine from the mission drug list of the PMs (5%–10%) and UMs (2%). We would be less concerned about the IM and NM of codeine.
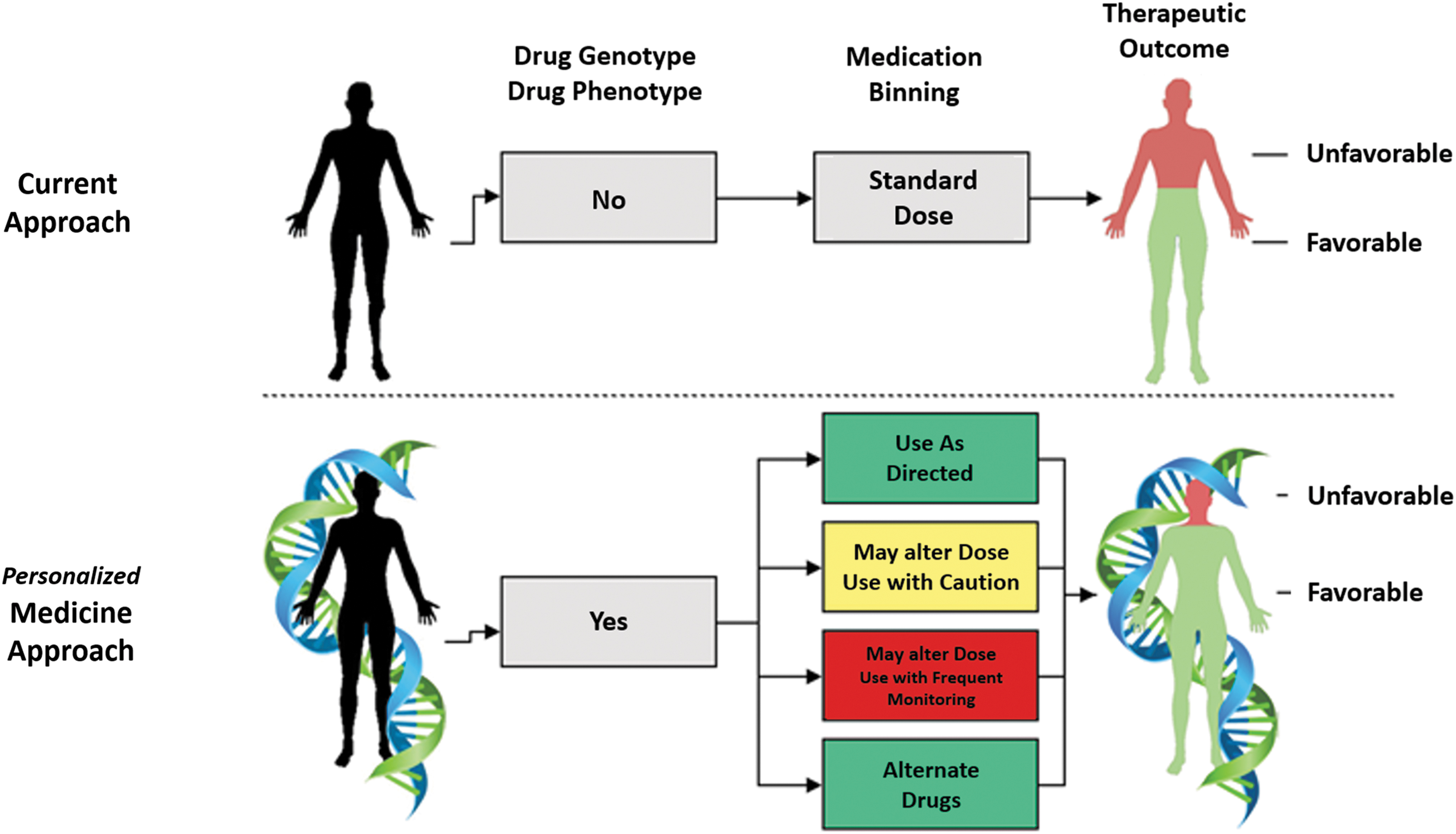
How pharmacogenomics may guide precision medicine in space. In the near future, drug prescribing for astronauts in space will rely upon pharmacogenomics. Each astronaut will be provided a drug-metabolizing enzyme profile, based on genotyping. The drug-metabolizing phenotype will guide the selection of drugs from each application area (analgesic, antibiotic, etc.), which will be tailored (personalized) to the astronaut. Phenotyping can guide when to use drugs as directed, when to use with caution, when to monitor closely, and when to select a drug with similar action that is metabolized via a different enzyme. Precision selection would be expected to optimize for favorable outcomes in the astronaut. This advent of personalized (precision) medicine must also consider a range of dynamics beyond genotype. Image credit: Sovaris Aerospace.
This aligns with the Food and Drug Administration drug label for codeine, which states that even at labeled dosage regimens, individuals who are UMs may have life-threatening or fatal respiratory depression, or experience signs of overdose. The Clinical Pharmacogenetics Implementation Consortium (CPIC) recommends that codeine be avoided in UMs because of toxicity. In PMs, codeine should be avoided, due to lack of efficacy. 14
Case Four: Converging Variables: Impact of the Gut Microbiome on Drug Metabolism in Space
Acetaminophen can also be used to illustrate the potential impact of the gut microbiome on drug metabolism in space. Clayton et al. administered 1 g of acetaminophen to humans, while assessing urinary levels of p-cresol sulfate, acetaminophen sulfate, and acetaminophen glucuronide to humans. 15 Individuals who had high predose urinary levels of p-cresol sulfate were found to have lower post-dose urinary acetaminophen sulfate.
To understand this study, it is important to note that p-cresol is produced by certain gut bacteria that transform the dietary amino acid tyrosine into p-cresol. After p-cresol is produced by gut bacteria, it is absorbed into the bloodstream for processing in the liver. The liver requires a rich pool of sulfur molecules to detoxify the p-cresol. However, when acetaminophen is delivered to those in whom p-cresol is being produced by gut bacteria (e.g., by certain clostridial species), there is competition for the liver's sulfur groups between the two molecules. In short, the gut-derived p-cresol can reduce the amount of sulfur available to properly metabolize acetaminophen (and other drugs), rendering the drug more toxic.
How might this be relevant to spaceflight? We have recently reported on the trajectory of p-cresol in the plasma of Scott Kelly, during the NASA Twins Study of 1 year in space. Both p-cresol sulfate and p-cresol glucuronide were elevated in space when compared with his own baseline and endpoint ground measurements. In addition, p-cresol sulfate and p-cresol glucuronide were elevated in comparison to his monozygotic twin (control) on the ground. 16
To further explore the implications of p-cresol, it is important to recall Case Two (above), regarding the metabolism of acetaminophen in the absence of adequate sulfur groups (e.g., GSH), wherein the toxic intermediate NAPQI is produced and liver impairment can ensue. In the present case (Case Four), the additional burden of elevated gut microbial p-cresol can further compromise the liver in its ability to metabolize the drug by placing additional demands on the sulfur pool. This case is an example of the convergence of five variables that are identifiable through the molecular analytics of personalized medicine and actionable through specific countermeasures: (1) drug input (acetaminophen), (2) dietary input (tyrosine), (3) nutrient input (GSH), (4) gut microbes (process layer; clostridial species), or (5) gut microbial metabolites (output layer; p-cresol).
Case Five: Converging Nonessential Inputs: Drug–Drug Interactions
Many drugs that would be found on a spaceflight mission formulary can interact at the process level (governed by genes and enzymes) to produce undesired effects. Conceptually, drug A may inhibit (or induce) a drug-metabolizing enzyme (CYP450) needed for the metabolism of drug B that is concurrently being used by the astronaut.
For example, CYP450 3A4 is the enzyme required for the metabolism of Ambien (zolpidem), a drug widely used for sleep in spaceflight. In this case, Ambien is the substrate (the substance on which an enzyme acts). If circumstances also require the co-administration of Biaxin for an infection (clarithromycin, an inhibitor of CYP450), the administration of Biaxin will slow down Ambien metabolism and prolong Ambien's effect. 17
The combination of the two drugs, then, may result in Ambien's prolonged symptoms of drowsiness, dizziness, fatigue, weakness, loss of coordination, and others, during a period of critical operations in spaceflight, extravehicular activity, or on a planetary surface. In the traditional clinical setting, these “side effects” might be characterized as “unexpected.” In the personalized medicine setting, these responses would be considered predictable and repeatable.
Fortunately, the substrate, inhibitor, and inducer profile for prescription and nonprescription drugs is generally well characterized. Thus, we have the capability today to model a wide range of drug–drug interaction profiles for any human entering space. For a detailed review of drug–drug interactions involving CYP450 enzymes, the reader is referred to Bahar et al. 17
The Space Environment: Using the Model for Personalization of Radiation Countermeasures
The systems model can also be used to explore inputs that influence the human response to one of the primary environmental risks of traveling in space: radiation. Data from the Radiation Assessment Detector (RAD) experiment on the Mars Science Laboratory 18 revealed that, during a 360-day Mars transit mission, an astronaut would receive a dose of about 600 millisieverts (mSv). This is just short of international space agencies career exposure limits of 1,000 mSv. 19 If we assume that a crew would spend 18 months on the surface (while they wait for the planets to realign so they can make the journey back to Earth), they will be exposed to an additional 400 mSv (total of 1,000 mSv).
Levels of exposure for sensitive neural tissue like the brain's hippocampus (memory center) are independently set by NASA at 1,000 mSv for a year and 1,500 mSv for a career. 20 In the preclinical work of Acharya et al., chronic (6 months) low-dose (18 cGy) and dose rate (mGy/day) exposures of mice to a mixed field of neutrons and photons resulted in diminished hippocampal neuronal excitability and disrupted hippocampal long-term potentiation. This was accompanied by severe impairments in learning. 21 As a corollary, Scott Kelly displayed decreased cognitive speed and accuracy for almost all 10 cognitive tests given, even 6 months after his return to Earth following 1 year in space (NASA Twins Study). 22
In these space radiation conditions, maintenance of DNA repair capability is crucial to maintaining function and preventing injury. The importance of this was further emphasized when the NASA Twins Study revealed that the majority of the pathways for DNA repair and DNA maintenance were significantly activated during prolonged spaceflight. 22 As part of human radiation countermeasure development, it seems prudent, at a minimum, to assure that the essential inputs that govern DNA repair are optimized before, during, and after spaceflight.
Case Six: Magnesium and DNA Repair
One example serves to illustrate this point. Magnesium (Mg; Mg+2) is an essential cofactor in almost all enzymatic systems involved in DNA processing. In general, magnesium is a cofactor for the following enzyme systems involving DNA repair23,24: (1) mismatch repair, (2) base excision repair, (3) nucleotide excision repair, and (4) double-strand break repair.
This is based on three fundamental roles of magnesium in DNA repair, including: (1) a catalytic center of numerous DNA repair enzymes, (2) a key trace element that stabilizes all adenosine triphosphate (ATP) molecules (ATP being required for DNA repair), and (3) a core element in the enzyme ATP synthase.
Studies from the ISS have previously shown that urinary Mg+2 levels were 44% lower after landing than before launch (P < 0.001). Specifically, 55% of the ISS crew members had Mg concentrations lower than the low end of the clinical range (3.0 mmol/day). Moreover, after 6 months in space, there is a loss of Mg reservoirs, with a 35% loss in some leg muscles. This is noteworthy, as muscle and bone are the principal reservoirs for Mg in the human body, accounting for 27% and 53% of total body Mg, respectively.25,26
In our own analysis of elite collegiate athletes (a fitness analog to astronauts) on Earth (N = 30), we found that red blood cell magnesium levels were below the standard reference range (4.5–6.5 mg/dL) in 86% of participants. Several cohort members had levels as low as 3.1 mg/dL.
Collectively, these findings would support attention to Mg status (as an essential input) as one means to assure that the DNA repair system has sufficient levels of this catalytic element to remain fully operational in space. This represents one step toward potentially mitigating some of the effects of a nonessential input (radiation).
Jugular Vein Thrombosis: Application of the Model to Emergent Problems in Space
In 2019, a newly discovered risk associated with spaceflight was reported. 27 It has been previously well established that, during prolonged weightlessness, body fluids shift headward resulting in facial puffiness, decreased leg volume, increased cardiac stroke volume, and decreased plasma (blood) volume. Until now, there had been no examination of the hydrodynamics of the major venous system that is responsible for draining blood from the brain, namely the jugular veins.
This knowledge gap led to the initiation of a prospective study that included 11 ISS crew members (mean [SD] age, 46.9 [6.3] years, 9 [82%] men) participating in long-duration spaceflight missions (mean 210 days). The primary research question addressed whether long-duration exposure to weightlessness is associated with impaired cerebral venous outflow and increased risk of jugular venous thrombosis (clotting within the blood vessel).
During this study, internal jugular vein measurements from before launch and ∼40 days after landing were acquired in three positions: seated, supine, and 15° head-down tilt. In-flight internal jugular vein measurements were acquired at roughly 50 days and 150 days into spaceflight, during normal spaceflight conditions. Lower body negative pressure was applied where indicated.
Stagnant or reverse flow in the internal jugular vein was observed in six crew members (55%) on approximate flight day 50. Importantly, one crew member was found to have an occlusive internal jugular vein thrombus, whereas a potential partial internal jugular vein thrombus was identified in another crew member retrospectively. Lower body negative pressure was associated with improved blood flow in 10 of 17 sessions (59%), during spaceflight.
These findings led to the conclusion that weightlessness is associated with blood flow stasis in the internal jugular vein, which may in turn lead to thrombosis in otherwise healthy astronauts. This has been deemed a newly discovered risk of spaceflight with potentially serious implications.
Case Seven: Conditionally Essential Inputs and Jugular Vein Occlusion
In emergent problems such as this, two approaches to the systems model can be explored. The first is the use of untargeted multiscale omics (genomics, epigenomics, transcriptomics, metabolomics, metagenomics, gut metagenomics, etc.) in an effort to detect patterns of molecular variance associated with those who do and do not develop vascular or clotting changes. In the untargeted approach, one does not predetermine the molecular species being measured, but rather analyzes as many molecular features as possible. Thus, it is a nonhypothesis-driven approach, where the data are used to identify features (signals) of potential significance.
Second, one can use the input–output model to formally examine essential, conditionally essential, and nonessential inputs in an effort to identify those inputs that might characterize potential contributors to elevated risk and, also, inform development of potential countermeasures.
For the purpose of illustration, it is useful to explore specific conditionally essential inputs discussed previously, the omega-3 fatty acids EPA and DHA. There are presently well-established biochemical mechanisms linking EPA, DHA, and their anticoagulant properties to modulating platelet activation, vascular tissue factor activity, and levels of plasma tissue factor, which are associated with lowered risk to thrombus formation. In addition, the omega-6 fatty acid arachidonic acid (AA; via its downstream signaling cascade) is mechanistically associated with greater platelet stickiness and increased risk to thrombus formation. 28
From this mechanistic vantage point, a brief review of clinical evidence can be used to explore the role of fatty acids as relevant inputs in spaceflight-associated venous thrombus. In one of the largest studies of its kind, Isaksen et al. recruited 29,648 participants from the fourth and sixth survey of the Tromsø Study. They examined the link between omega-3 fatty acid intake and venous thromboembolism (VTE). Overall, individuals with an omega-3 fatty acid intake above the reference (≥4.7 g/week) had a significant 22%–26% lower risk of VTE. 29
Hiki et al. enrolled 45 patients with acute VTE and compared them with healthy controls (control: age 55 ± 11 years; VTE: age 57 ± 17 years). Those with VTE showed significantly higher AA levels and lower EPA levels in serum, which is consistent with their known mechanisms. The younger patients with VTE showed significantly lower EPA/AA ratio than their age-matched controls, also consistent with the known mechanism. 30
Omega-3 fatty acids were also assessed in 826 patients aged ≥65 years, as part of the Swiss Cohort of Elderly Patients with VTE. At 6 months, patients with higher omega-3 fatty acid levels had a risk reduction of more than 60% for developing recurrent VTE or total mortality. The individual secondary endpoints, recurrent VTE and total mortality, occurred significantly less frequently in patients with medium and high compared with low omega-3 FA levels. 31
There is a significant contribution of microgravity and fluid shifts to the spaceflight-associated impairment of cerebral venous outflow. However, these hydrodynamic forces also exert their effects in the context of an astronaut's complex molecular networks, which have notable interindividual variability. EPA, DHA, and AA can be viewed as single inputs (Input1, Input2, Input3) among many possible inputs (Input…N) that influence this dynamic. In practice, they serve to illustrate the potential value of formally evaluating known inputs in a stepwise manner for the purpose of identifying the incremental features that may aggregate across systems to influence vascular health and safety in space (Input1 + Input2 + Input3 + InputN = Summation of Effect).
Insight From the Nasa Twins Study: the Role of Multiscale Omics
We have been involved in the conception, design, implementation, and analysis of the NASA Twins Study of 1 year in space.22,32 This study brought together genomics, epigenomics, transcriptomics, metabolomics, metagenomics (gut microbiome), and other phenotypic measures for the first time in space. We extensively apply “untargeted analysis,” wherein the analytes being measured are not predetermined. Omics studies of this kind generate high-dimensional data sets, which can be challenging in conditions of low subject numbers. We address this to some degree by longitudinal analysis (serial measures) and statistical methods.
Thus, by its nature, such studies are exploratory. They are useful for identifying patterns of variance, which can later be used to generate new hypotheses. Such multiscale omics studies can reduce the iterative process of spaceflight experimentation because vast numbers of analytes can now be measured in one experiment. The identification of patterns leading to new hypotheses is precisely what we need to accelerate the development of personalized medicine, as both a clinical and a research discipline.
As a research discipline, we invite the scientific community to consider (to the extent possible) the following path forward for all future spaceflight experiments involving humans. First, we recommend designing all experiments in such a way that appropriate specimens for omics investigations can be captured. 33 The design of such experiments could be done in collaboration with the omics community to minimize preanalytical variance, optimize detection of true biological variance, and avoid false discoveries. Second, we suggest investigators biobank these specimens according to current best practices, either for immediate analysis or as archival specimens for future analysis. 34
Such an approach would be expected to provide more robust data sets, valuable in refining ideal mission parameters. This approach may also yield unanticipated countermeasure targets, leading to adjunct solutions that could be used to augment general or specific solutions. In our view, this represents a unique opportunity to significantly advance one of the key elements supporting the sustained presence of humans in space.
Optimizing Safety and Performance Versus Treating Disease
Personalized medicine applied to spaceflight differs from Earth-based clinical practice in two notable ways. First, a great deal of Earth-based medicine has a primary focus on managing disease. For instance, extensive work in oncology has shown the promise of combination therapies for improved outcomes, both epigenetic 35 and genetic, 36 although this is the most efficacious when tailored to the clonal state of the cancer 37 and the molecular profile of the patient. In contrast, spaceflight personalized medicine has a substantial focus on safety and performance. As such, personalized medicine applied to space medicine is not primarily focused on biomarkers of disease, but on molecular patterns of variance in health (although application to disease is relevant).
Second, the unique operating environment of space requires that molecular patterns that might affect an individual's response to the selected environmental exposures of space be more fully characterized. These metrics can be assessed on Earth for the purpose of developing mission-centric countermeasures. We also possess a growing capacity to monitor such metrics in real time with instruments that have been recently established to enable molecular diagnostics in zero gravity 38 and on the ISS. 39 Such tools and methods can enable the development of environment-specific countermeasures.
Converging Variables and Incremental Gains
Addressing molecular network dynamics through molecular profiling allows us to take advantage of the principle of incremental gains. While alteration of a single pathway or network may have a mild impact on health and performance, the aggregation (convergence) of multiple variants (deficiency, excess, genetic variants) across multiple networks (and pathways) can amplify beyond single variants in a manner that scales. This effect can further scale with time.
Countermeasures directed at a single pathway or network may have a modest clinical or performance impact, depending on the pathway/network. In our experience, incremental gains accrue when multiple inputs and pathways are targeted with individualized countermeasures, which can aggregate toward an amplified impact on an individual.
Lessons From Operational Analogs
We have extensive experience in the application of molecular profiling and personalized medicine across a wide range of operating environments, including military Special Forces, S.W.A.T., NASA (ISS), high-altitude ascent, wilderness medicine, wilderness expeditions, space analogs, Olympic athletes, NFL (football), NBA (basketball), NHL (hockey), professional racing (Le Mans, NASCAR), and others. This has allowed us to identify patterns of variance in molecular networks common across the spectrum of elite performers, who can be viewed as fit analogs to individuals entering space. It has also allowed us to acutely observe the response to personalized countermeasures, since those operating in these environments are uniquely sensitive to gains or losses in performance. It has also enhanced our ability to refine the molecular profiling methods and the approach to countermeasure development.
Assessing the Need for Personalization
The question of when to apply personalized medicine to individuals entering space is worthy of consideration. While opinions will likely vary, we propose the following. For a spaceflight participant who embarks on a 2-h suborbital flight and is exposed to only 4 min of microgravity, extensive clinical workups beyond the standard requirements may not be routinely indicated. Conversely, there may be instances where the specific medical concerns of an individual would benefit from molecular profiling and individualized countermeasures, even for single short-duration flights. This might be for the purpose of enhancing safety, mission comfort, or simply optimizing the experience.
For a passenger who flies monthly on orbital or suborbital flights from New York to Hong Kong, the argument for personalization would appear to grow stronger. For a pilot who flies regularly into the space environment, there is an occupational and performance component that would benefit from routine personalization. A passenger, scientist, or astronaut entering an orbital habitat would benefit from routine personalization. Lunar and Martian missions of any duration would be among the most relevant missions in need of personalization.
Missions to the Moon and Mars
Lunar settlement, Mars transit, and Mars surface operations will require considerable advances in engineering. This necessarily involves advancing sophistication in astronautical engineering, including subdisciplines such as aerodynamics, structures, propulsion, mechanics, sensors, stability, and control. Fundamental to this is an understanding of pathways, networks, and system integration. All these systems must be designed and tested, so that function and efficiency is optimized across all domains for a given environmental (or mission) condition.
In many respects, these astronautical systems share features with the human system, although a human would be considered a complex adaptive system. It can be argued that the ability to now generate greater precision in the characterization of human molecular pathways and networks gives us the capacity to move in the direction of an astronautical systems engineering approach to space medicine and human performance.
One challenge in sending humans on these types of missions will be that we do not yet have human data from these environments. Analog environments will be useful, but limitations will remain.
This leads us to a question? To what extent do we rely upon a systems approach to robust analysis of diverse molecular features in a human on Earth, as a basis for tailoring our countermeasures to that single individual heading into space? The question can also be posed somewhat in the converse. That is, will there be missed opportunities for positive influence if we do not rely upon such analyses and their derived countermeasures, given that critical aspects of this science are actionable today?
Personalized Medicine in the Context of Current Practice
The standard medical approach to spaceflight medicine remains the foundation of the care for humans entering and returning from the space environment. Most certainly, there has always been a measure of individualized care applied in this historical practice. However, we advocate an expanded, evolutionary, and adaptive approach where a much more detailed analysis of genotype and molecular phenotype is gathered from each spaceflight participant and astronaut. This addresses greater complexity and adds additional precision to the tailored intervention.
In this review, we have outlined our perspective on how personalized (precision) medicine may be envisioned and applied in human spaceflight. While this is only one perspective, it respects the complexity of the rapidly developing fields of Omics, how the molecular landscape elucidated by omics influences the clinical phenotype, and provides a means to reduce the complexity of these networks by attention to the concept of inputs.
We make the case that attention to essential inputs, conditionally essential inputs, and nonessential inputs represents an actionable strategy that can be applied today. We further suggest that countermeasures derived from molecular profiling have the capacity to raise the efficiency of metabolic networks in a manner that is tailored to the needs of any individual. These are expected to positively impact the health, safety, and performance of those entering the space environment. Beyond the surveillance of inputs for the purpose of clinical action, the expanded use of multiscale omics profiling of spaceflight participants should improve our understanding of the biological response of humans in space, which will contribute to the advancement of new spaceflight countermeasure development.
Footnotes
Acknowledgments
We extend a special thanks to the Federal Aviation Administration Center of Excellence for Commercial Space Transportation. We also thank the University of Colorado Aerospace Engineering Sciences, College of Engineering & Applied Science. We offer our sincere thanks to Dr. David Klaus, Associate Chair, Undergraduate Program, Aerospace Engineering Sciences, University of Colorado. Finally, we thank Julian C. Schmidt, MS of Sovaris Aerospace, for manuscript support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for this article. However, for the NASA Twins Study data cited herein, funding was provided by NASA: NNX14AH51G (All Twins PIs); TRISH: NNX16AO69A: 0107 and NNX16AO69A:0061 (Mason); the Bert L and N Kuggie Vallee Foundation, the WorldQuant Foundation, The Pershing Square Sohn Cancer Research Alliance, and the Bill and Melinda Gates Foundation (OPP1151054) for funding (Mason).