
Abstract
Abstract
Background:
Invasive opportunistic fungal infections caused by agents of Mucorales that involve the gastrointestinal tract are uncommon but aggressive. These ubiquitous fungal spores typically are inhaled and can germinate in immunocompromised hosts. Standard therapy for invasive mucormycosis includes parenteral amphotericin B (AMB) in combination with radical debridement of infected tissues. Early diagnosis and treatment are of paramount importance. Unfortunately, long-term survival is poor owing to the prohibitive morbidity and mortality rates associated with the medical and surgical therapies. Posaconazole is a novel, extended-spectrum triazole oral antifungal agent with documented success in the treatment of patients with invasive mucormycosis.
Methods:
Case report and literature review.
Results:
A 50-year-old man presented with invasive mucormycosis of the lower esophagus, stomach, and liver, resulting in gastrointestinal hemorrhage. The infection did not respond to AMB but was treated successfully with a combination of posaconazole and liposomal AMB (LAMB) without surgical debridement.
Conclusions:
To our knowledge, this is the first reported case of extensive gastric and intrahepatic mucormycosis that responded to combination posaconazole and LAMB without surgical debridement. This approach may be an alternative to surgery in patients who are precluded from extensive surgical intervention.
Mucormycosis is associated with extensive angioinvasion of the host, with accompanying thrombosis, tissue infarction, and necrosis, followed by hematogenous dissemination of the organism. Surgical debridement combined with systemic antifungal therapy is the de facto standard of care for invasive gastrointestinal mucormycosis (IGM), especially in patients with symptoms and complications, such as ischemia, perforation, emphysematous gastritis, or refractory bleeding [10–15]. Antifungal therapy with parenteral amphotericin B (AMB) for IGM is supported by isolated case reports of studies in which the drug was combined with surgical intervention [14–17]. However, therapy with systemic AMB has been limited by its side effect profile, which includes nephrotoxicity, electrolyte abnormalities, and infusion-related reactions [6–20]. Radical debridement may be associated with prohibitive perioperative morbidity and mortality rates because of the extent of surgery required, the debilitated state of the patient, and the urgent nature of the intervention [6,8]. Additionally, radical resections may, paradoxically, immunosuppress the host, allowing further dissemination of disease [21–23]. Even with aggressive medical and surgical management, the mortality rate for patients with IGM is reported to approach 90 per cent [5].
Posaconazole is a novel, extended-spectrum triazole antifungal agent with activity against a wide variety of yeasts and molds, and has documented efficacy for infections resistant to standard antifungal drugs [24–27]. Herein, we describe a case of IGM of the lower esophagus, stomach, and liver that was eradicated with posaconazole and liposome AMB (LAMB) without surgical intervention; we also provide an overview of the management of IGM.
Case Report
A 50-year-old man with hepatitis C, hypertension, a history of polysubstance abuse, and end-stage renal disease necessitating hemodialysis presented to our university-based tertiary-care referral center emergency department with generalized peritonitis. Upright abdominal radiography revealed pneumoperitoneum. After appropriate intravenous fluid resuscitation and administration of empiric broad-spectrum antibiotics, the patient underwent exploratory laparotomy. Ischemic perforation of the sigmoid colon was found, and a Hartmann's procedure was performed. Treatment was complicated by sepsis and multiple organ dysfunction syndrome that necessitated vasopressor support with norepinepherine and vasopressin. After surgery, the patient was given empiric therapy consisting of intravenous vancomycin (goal trough concentration 15–20 μg/mL), imipenem-cilastatin (250 mg intravenously every 12 h), and fluconazole (400 mg/d). He also received a steroid bolus and taper for a low serum cortisol concentration. His serum was negative for antibodies to the human immunodeficiency virus (HIV).
The patient was eventually weaned from vasopressors, liberated from mechanical ventilation, and transferred from the intensive care unit (ICU). On postoperative day 9, gastrointestinal hemorrhage developed that necessitated 15 units of blood. Colonoscopy showed no active bleeding. Esophagogastroduodenoscopy revealed numerous contiguous necrotic lower esophageal and gastric ulcers (Fig. 1). Biopsy specimens revealed extensive gastritis and tissue infiltration with non-septated hyphae consistent with IGM (Fig. 2). Retrospective review of the resected colon specimen showed no evidence of IGM. A peritoneal fluid culture taken during the patient's initial surgical procedure yielded one colony of Mucor spp. at 30 days of incubation (two weeks after the pathologic specimens from the gastric biopsies were found to be positive for Mucor spp.). The patient's functional status, multiple comorbidities, and malnutrition prohibited surgical management of the acute hemorrhage. In addition, the patient refused to undergo surgery. He was given total parenteral nutrition and intravenous omeprazole.

Esophagogastroduodenoscopy. (
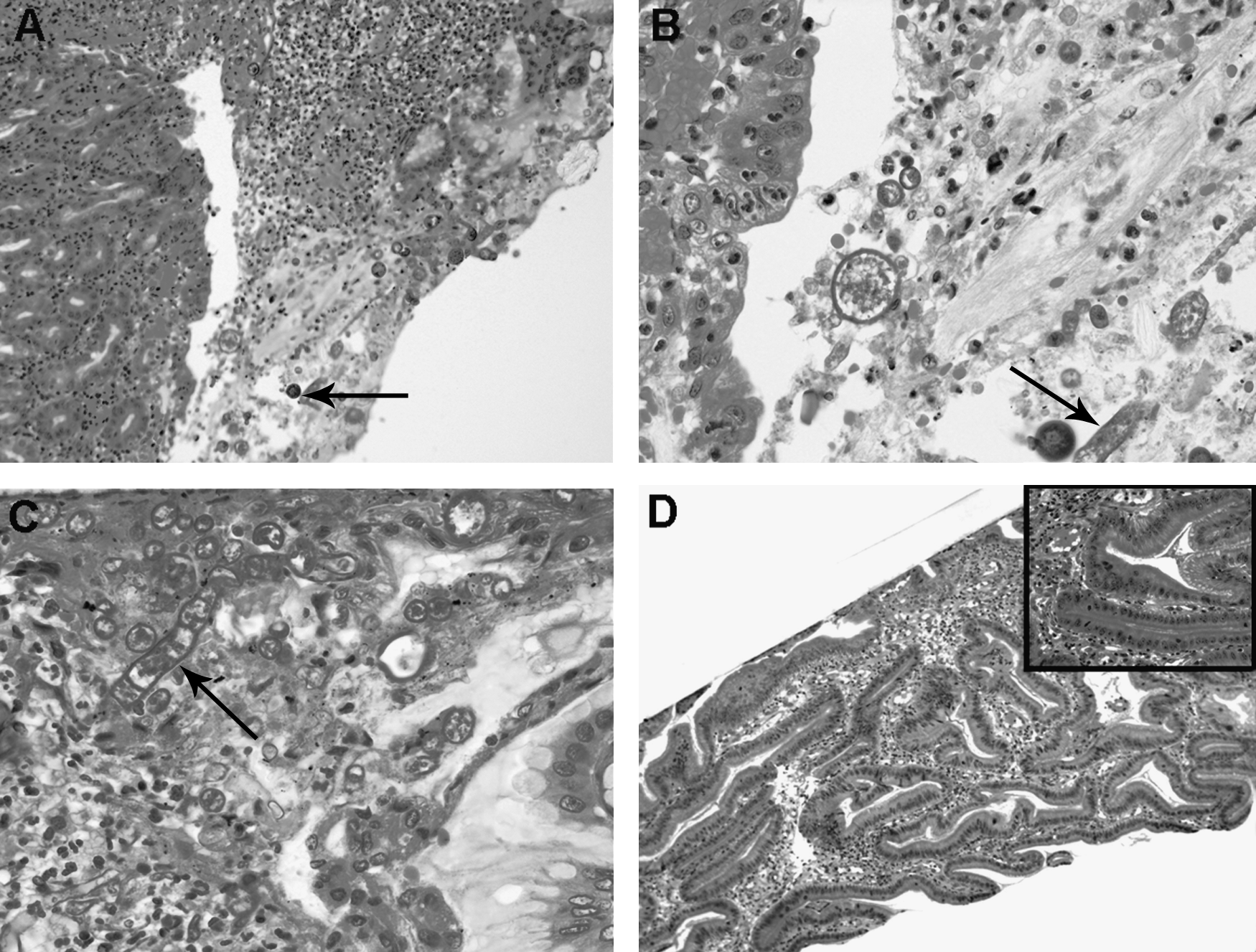
Pathologic analysis of biopsy specimens shows active gastritis with an extensive infiltrate of polymorphonuclear neutrophils. Within the inflamed gastric mucosa are numerous, irregular, ribbon-like, broad, somewhat optically clear fungi with no obvious septae (
Therapy was begun with intravenous LAMB (5 mg/kg/d) and oral AMB (50 mg/d). Infusions of LAMB were complicated by hypotension and rigors. On postoperative day 15, recurrent gastric hemorrhage developed. Angiography revealed no site of active bleeding, and the patient continued to be treated medically. On postoperative day 21, recurrent hematemesis developed. A 99mTc-tagged red blood cell scan revealed an upper gastrointestinal source, and the patient underwent angioembolization of the left gastric artery, resulting in cessation of the hemorrhage. During the resuscitation, the patient received 19 units of blood, fresh frozen plasma, cryoprecipitate, and recombinant coagulation factor VIIa (NovoSeven, 6 mg intravenously; Novo Nordisk, Bagsværd, Denmark).
It was determined clinically that the IGM had progressed despite standard therapy with AMB. Posaconazole suspension was requested and approved, and the patient was enrolled in a compassionate-use protocol. Posaconazole dosed at 200 mg orally every 6 h was added to the patient's therapy with intravenous LAMB; oral AMB was discontinued. The dosage of posaconazole was mandated by the compassionate-use protocol (200 mg every 6 h for optimal absorption). Eight days after initiation of combination therapy, repeat endoscopy showed interval healing of the gastric ulcerations (Fig. 1C). Tissue biopsy specimens obtained at that time were negative for evidence of continued active infection with Mucor spp. (Fig. 2D). Posaconazole was continued as single-agent maintenance therapy dosed at 400 mg orally every 12 h (protocol specified), and the patient was discharged on postoperative day 35. Repeat endoscopy just before discharge showed normal gastric mucosa (Fig. 1D).
Four weeks after discharge, the patient returned with right upper quadrant abdominal pain. Transabdominal ultrasonography and dynamic computed tomography (CT) of the abdomen identified a 2.3 × 3.6 × 3.2-cm cystic lesion laterally within the right lobe of the liver (Figs. 3A, B). This lesion had been noted six weeks before as a punctuate lesion by CT. Cyst fluid obtained by CT-guided aspiration was positive for non-septated hyphae, consistent with Mucor, by calcofluor staining; however, fungal cultures were negative. Bacterial cultures of the aspirated fluid also were negative.

Computed tomography (CT) scan of the abdomen revealing hepatic abscess (black arrows). Calcofluor stain shows non-septated hyphae on CT-guided aspiration (
Because of the development of the hepatic lesion while the patient was on single-agent therapy, intravenous LAMB was reinitiated in addition to oral posaconazole. After one month of combination therapy, the patient's pain had resolved, and repeat CT of the abdomen showed resolution of the cystic lesion. The LAMB was discontinued again in favor of single-agent posaconazole therapy, with no recurrence of symptoms. The patient completed 1 year of posaconazole maintenance therapy with no reported adverse events. Serial CT scans 1, 2, 7, and 12 mos after initiation of posaconazole and a follow-up CT scan 2 months after completion of posaconazole therapy showed no evidence of recurrent IGM. Serial blood cultures obtained after discontinuation of posaconazole remained negative. The appropriate duration of therapy for IGM is unknown; the time course in our patient was determined by radiographic resolution of the hepatic lesion and absence of clinical recurrence. Eight months after completion of therapy, the patient died of complications related to gram-negative bacteremia arising from an indwelling hemodialysis catheter. Autopsy findings showed no evidence of active Mucor infection.
Discussion
In 1885, Paltauf first described life-threatening systemic infection by fungi in the class of Phytomycetes (Mucor or Rhizopus spp.) [4,28]. In an immunocompetent host, these pleonastic spores usually are phagocytosed and cleared. Mucormycosis presents most commonly as rhinocerebral or pulmonary disease, or both; IGM is an uncommon presentation. Patients most at risk for IGM include those who are extremely malnourished (especially infants and children) and those in whom the infection arises from ingestion of fungal spores. Other risk factors for IGM include necrotizing enterocolitis, seen in premature infants; profound neutropenia; and other immunocompromising conditions, such as acquired immunodeficiency syndrome (AIDS), systemic lupus erythematosus, and organ transplantation [1,4,5].
Gastrointestinal involvement has been described in the literature since the early 1960s, mainly through case reports [29,30], and occurs most commonly in the stomach, colon, and ileum. The survival rate is lower for IGM than for infection at other sites [5,7,10–12,14,16,19,30]. The spores of Mucor spp. adhere to endothelial matrix proteins, where tissue injury results, followed by infarction, necrosis, and ultimately the dissemination of the organism [31]. Because this infection is uncommon, acute, and rapidly fatal, the diagnosis often is made by postmortem examination.
The optimal systemic antifungal therapy for IGM is ill-defined because of the paucity of clinical trial data. Although efficacious historically in combination with radical debridement, AMB use is limited by infusion-related adverse events and systemic toxicity [4,17,20]. Posaconazole is an orally administered triazole with activity against mucormycosis and a toxicity profile similar to that of fluconazole [24–26]. It has been an effective prophylactic agent against IFIs in patients with graft-vs.-host disease [32] and patients with neutropenia associated with induction chemotherapy for the management of high-risk hematologic malignant disease [33]. Posaconazole also has proved to be effective in patients with infections caused by Mucor spp. who have been intolerant of or have failed treatment with other antifungal agents, primarily AMB-based regimens [24].
As with all azole antifungal agents, posaconazole disrupts fungal cell membrane synthesis through the inhibition of cytochrome P450-dependent 14α-sterol demethylase, an enzyme crucial for the biosynthesis of ergosterol. The extended side chain of the posaconazole molecule may result in a higher binding affinity to CYP51 than is obtained with fluconazole or voriconazole, which lack this substituent, and therefore may make posaconazole less susceptible than other azoles to the development of resistance as a consequence of mutations in this enzyme [24,33,34]. A recent clinical trial evaluated posaconazole in patients for whom treatment failed, or who did not tolerate traditional antifungal therapy [24]. Objective responses were recorded in 79% of patients in whom prior therapy failed and 80% of patients intolerant of traditional therapy. Interestingly, long-term survival was associated with surgical debridement of infected tissue, emphasizing again the fact that radical surgical debridement remains the standard of care for this aggressive disease.
Our patient received posaconazole on a compassionate-use basis for the treatment of IGM. At the time this manuscript was written, the U.S. Food and Drug Administration had approved posaconazole only for the prophylaxis of invasive Aspergillus and Candida infections in high-risk, severely immunocompromised patients undergoing chemotherapy for acute leukemia and in hematopoietic stem-cell transplant recipients with graft-vs.-host disease. The adverse events reported most commonly for this drug are nausea, vomiting, diarrhea, rash, hypokalemia, thrombocytopenia, and aberrations in liver enzymes.
Our case illustrates the complexity of treating patients who have IGM, who often have substantial barriers to recovery. To our knowledge, this is the first case of extensive gastric and intrahepatic mucormycosis to respond to combination posaconazole and AMB therapy without surgical debridement. Medical management with combination antifungal therapy offered cure in this patient, whose functional status precluded ideal surgical debridement of the infection. This approach may be an alternative to surgery for patients in whom the preoperative risk of surgical intervention portends a poor outcome.
Footnotes
Acknowledgment
This case was presented in abstract form at Focus on Fungal Infections 17; March 7–9, 2006; San Diego, CA.
No competing financial interests exist.
Author Disclosure Statement
No conflicting financial interests exist.