
Abstract
Abstract
Background:
Although cystic echinococcus (CE) is a common disorder worldwide, few cases are treated in the United States and other industrialized countries. Migration and tourism have caused an increase in the incidence of this parasitic infection in industrialized countries, and physicians must be familiar with its management.
Methods:
We report successful therapy of CE in an immigrant from Afghanistan.
Results:
The patient presented with a large epigastric mass that was initially misdiagnosed as gastric gastrointestinal stromal tumor. The mass was removed, together with partial gastrectomy, splenectomy, and resection of the left lateral segments of the liver, and diagnosis of CE was made. The patient recovered from surgery, albendazole was started, and at five months follow up, he is recurrence free.
Conclusions:
Echinococcus granulosus must be considered in immigrants and travelers presenting with a cystic mass.
Case Report
A slender 57-year-old man from Afghanistan presented to his primary care physician with a five-year history of a gradually enlarging upper abdominal mass. He reported mild intermittent heartburn during this time but denied any other symptoms such as abdominal pain or weight loss. His past medical history and family history were unremarkable. The patient had left Afghanistan seven years before, spent two years in Iran and Pakistan, and then moved to Northern Virginia, where he works for a car rental company. He did not speak English, requiring an interpreter during all visits, and was uninsured. Both issues emerged as important factors in the further management and clinical course of this patient. While living in Afghanistan, Iran, and Pakistan, the patient lived in large cities but regularly visited rural areas and raised and slaughtered sheep.
On examination, the patient had normal vital signs and was in no distress. In his left upper quadrant, a giant mass was protruding through the abdominal wall. On palpation it was firm, nontender, and poorly mobile, measuring approximately 20 cm in diameter. Initial investigation included chest x-ray, which showed a large calcified mass below the left hemidiaphragm (Fig. 1). A computed tomography (CT) scan showed a large, mixed, solid and cystic mass in the left upper quadrant. The superior portion of the mass was calcified, measuring 11 × 13 cm, and the inferior portion was multicystic, measuring 14 × 7 cm (Fig. 2). The origin of the mass was uncertain, but it was described as being adjacent to and compressing the gastric fundus, which led to consideration of a primary gastric tumor. The radiographic appearance was thought to be consistent with a gastrointestinal stromal tumor (GIST). All obtained laboratory values, including complete blood count and differential, basic metabolic panel, and liver function tests, were within normal limits. No elevation of the eosinophil count was present.
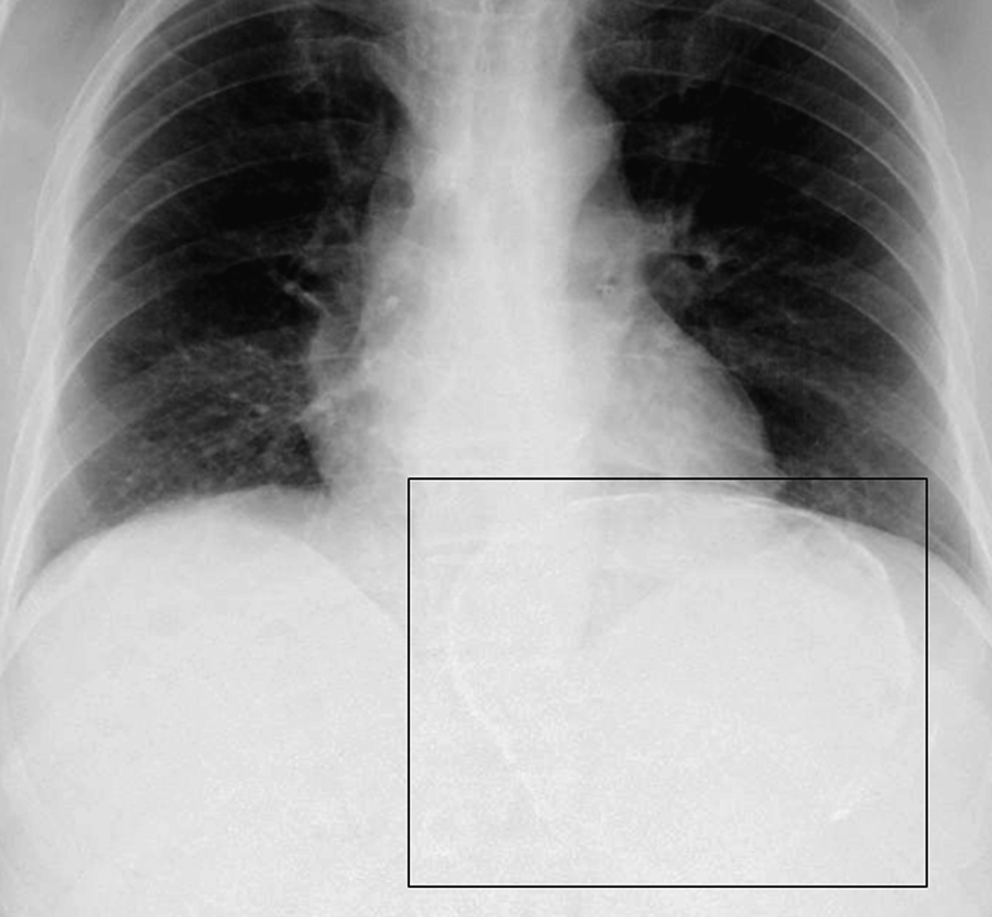
Chest radiograph showing a calcified intraabdominal mass.
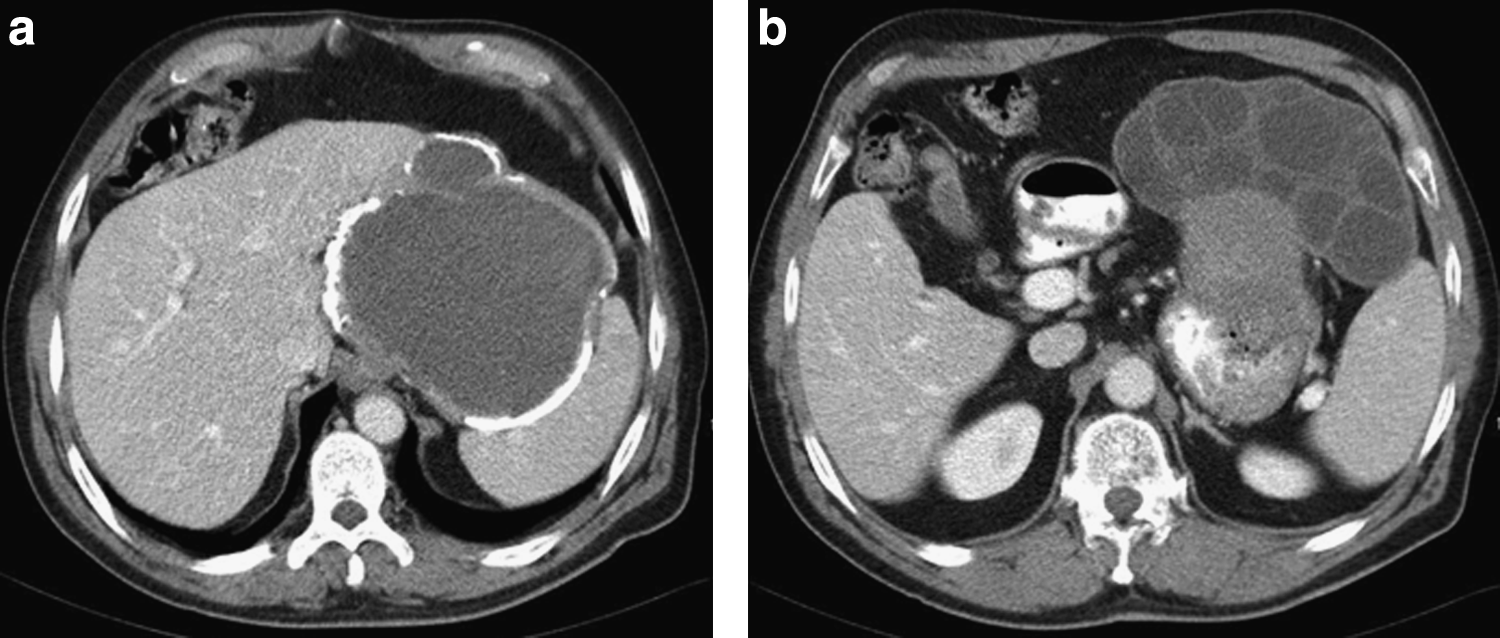
Abdominal computed tomograph scan. (
After substantial delay because of financial screening, a surgical consultation was obtained at our hospital, and the patient was scheduled for excision of the presumed GIST. Intraoperatively, the tumor was found to be more extensive than thought initially, involving the stomach, the left lobe of the liver, the left hemidiaphragm, and the spleen. Left hepatectomy, near-total gastrectomy with Roux-en-y gastrojejunostomy, left hemidiaphragmectomy, and splenectomy were performed. A feeding jejunostomy tube was placed. The patient became hypotensive after blood loss during liver resection, briefly requiring vasopressors and blood transfusion, but was otherwise hemodynamically stable throughout the operation.
Pathologic examination revealed a 20 × 17 × 10 cm mass (Fig. 3). Sectioning through the mass identified two cystic components, one measuring 11 × 10 × 7 cm, which was calcified with a necrotic center. A second smaller cyst, measuring 6 × 6 × 5 cm, was filled with numerous globular cystic structures that produced serous fluid when sectioned. Echinococcus granulosus was suspected, and microscopic examination of cyst aspirate showed Echinococcus hooklets and hydatid sand (Fig. 4).
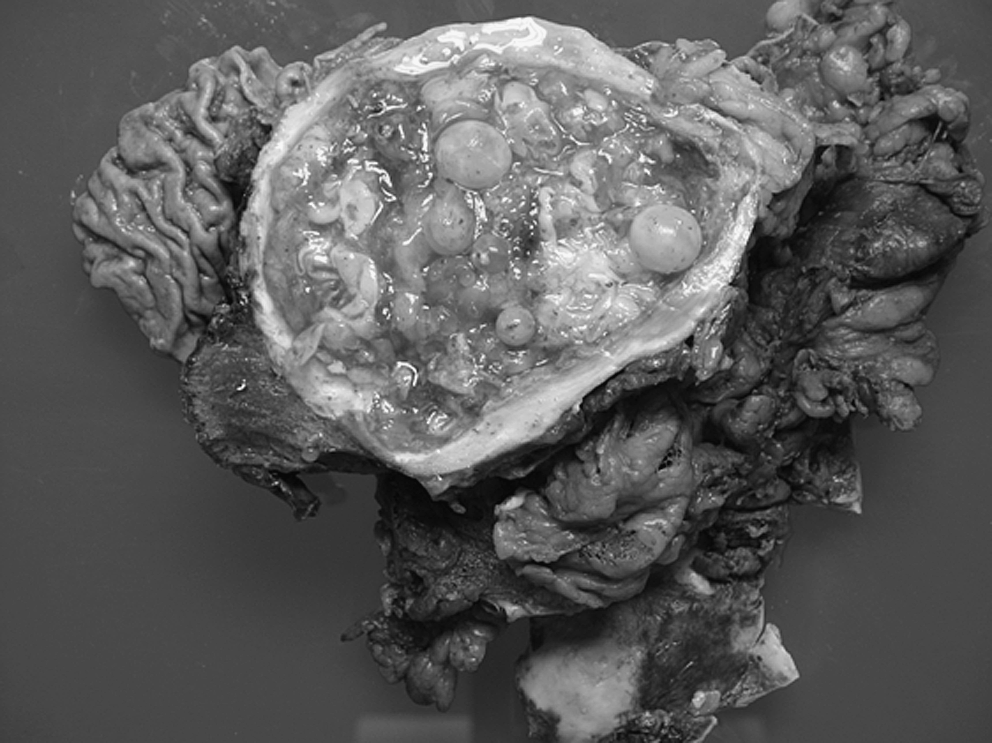
Gross pathological specimen: the mass was excised in toto.
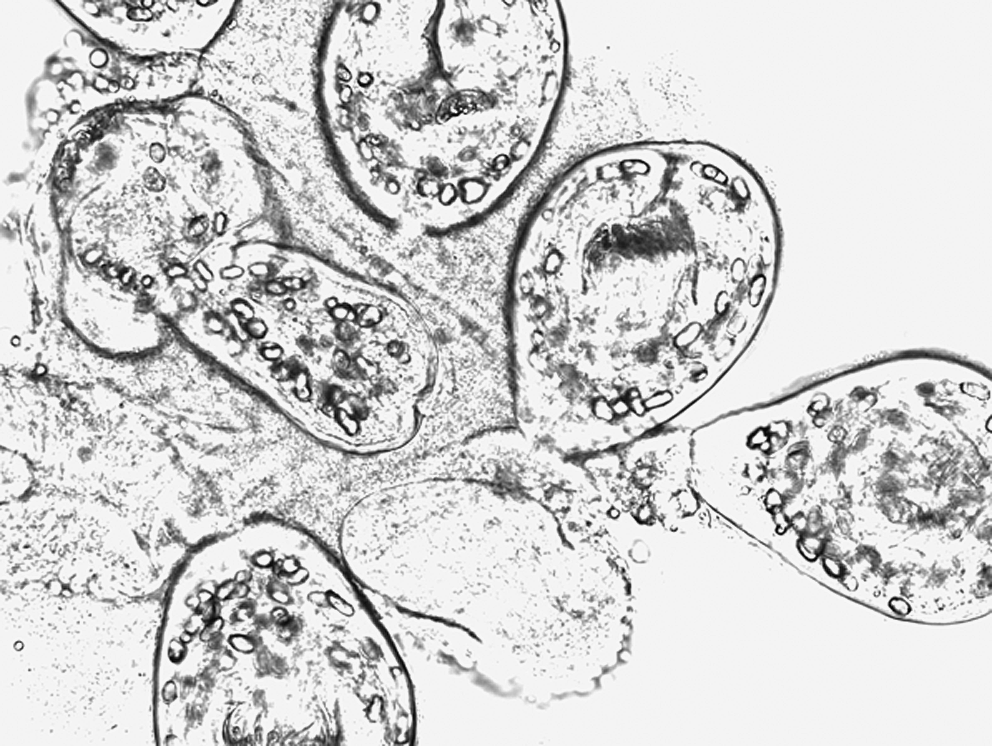
Microscopy of cystic fluid showing Echinococcus hooklets and hydatid sand.
The patient remained in the intensive care unit for five days. After diagnosis of echinococcal disease, screening for additional manifestations was performed. Computed tomography scans of the head, chest, abdomen, and pelvis revealed no further cystic disease. Albendazole at a dose of 400 mg twice daily was administered for 4 weeks, followed by 2 weeks without medication and then another 3 weeks of albendazole at the same dose. He was discharged on postoperative day 15 and was readmitted 2 weeks later with a subphrenic abscess, which was treated using CT-guided drainage. Streptococcus milleri was cultured, and ampicillin and sulbactam (3 g three times daily) was initiated. At the 5-month follow up visit, the patient had recovered well from surgery, with no evidence of recurrent hydatid disease. He was tolerating a regular oral diet and resuming his normal activities.
Discussion
The above report describes a case in which advanced CE was misdiagnosed as a GIST. Although the diagnosis of CE may be more straightforward in endemic areas, the presentation and radiographic appearance can be nonspecific, and misdiagnosis as solid tumors has been reported [3,4]. Because of the prevalence of CE in immigrants from certain areas, it is important for physicians in nonendemic countries to be familiar with the presentation, diagnosis, and treatment of CE. Patients with CE are usually asymptomatic for many years. When symptoms occur, they vary depending on the site of infection. Because the liver is the most commonly affected organ, symptoms are often due to mass effect and include dyspepsia and abdominal discomfort, as seen in our case. Cysts may also rupture, leading to pain, secondary infection, and even anaphylaxis due to leakage of immunogenic cyst fluid [5].
Cystic echinococcosis should be suspected in any patient from an endemic area who presents with a cyst-like mass. Imaging is the primary mode of diagnosing CE. Ultrasound is most commonly used because of its availability and low cost and has a sensitivity of 93% to 98% and a specificity of 88% to 90% [6]. Computed tomography scan and magnetic resonance imaging may also be used. Serologic studies are performed commonly to confirm presumed diagnoses. Enzyme-linked immunosorbent assay tests for antibody to echinococcal antigens are 60% to 90% sensitive but can be falsely positive with other helminthic infections and malignancies [1]. They are thus often followed with the more-specific immunodiffusion or immunoblot assays for echinococcal antigens [1]. In a recent study of 287 patients with CE of the liver, liver function tests were abnormal in only 43%, and eosinophilia was seen in only 35% [7].
Surgical intervention remains a mainstay of treatment for CE and is indicated for cysts that are large, are exerting mass effect, involve vital organs, or are likely to rupture [5]. Surgical options include pericystectomy, capitonnage, simple drainage, and resection of the involved organ, which can be performed using an open or minimally invasive procedure. A newer treatment option is called Puncture, Aspiration, Injection, Reaspiration (PAIR). In this treatment, the cyst is aspirated percutaneously under ultrasound guidance, injected with hypertonic saline or absolute alcohol, and reaspirated. A recent systematic review of the literature shows PAIR plus albendazole to have efficacy similar to that of surgery but fewer adverse events and shorter hospitalization [8], although the authors note that their conclusions are based on two small studies and that more evidence is needed before a firm recommendation can be made.
Medical therapy alone also has been suggested. Up to 30% of patients can be cured with albendazole alone, and an additional 40% to 50% show shrinking of cysts [9]. This option is reserved for patients who cannot tolerate surgery or suffer from disseminated disease, although albendazole is more commonly used as an adjunctive treatment to surgery or PAIR and may be more effective in combination with praziquantel [10].
In summary, we report on a patient from Afghanistan who presented with a complex cystic and solid abdominal mass that was misdiagnosed as a GIST. Although imaging was not pathognomonic for CE in our patient, CE must be considered in any patient from an endemic area presenting with a cystic mass. In retrospect, serologic studies in addition to reimaging before surgery might have helped to diagnose CE. Surgery was indicated in this patient, given the size of the mass and the extent of organ involvement, but establishing a diagnosis of CE preoperatively would have allowed preoperative treatment with albendazole and praziquantel and appropriate preparation for intraoperative complications such as anaphylaxis. As mentioned, the patient had hypotension requiring vasopressors and transfusion intraoperatively, which may have been an anaphylactic reaction.
Cystic echinococcosis is a common disease worldwide. Although uncommon in the United States and other industrialized countries, it must be considered in immigrants and travelers presenting with cystic mass.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.