
Abstract
Abstract
Background:
Pseudomembranous colitis (PMC) usually is caused by antibiotic-related changes in colonic anaerobic microflora, leading to Clostridium difficile overgrowth and overproduction of toxins. We present the first reported case of PMC affecting the intrathoracic, interposed colon of an esophagectomy patient in the absence of inflammation of the in situ colon.
Methods:
Case report and review of pertinent English-language literature.
Case report:
A 47 year-old male developed Clostridium difficile-related colitis after in Ivor-Lewis esophagectomy for carcinoma of the esophagus, and rendered asymptomatic after 10 days of therapy with oral vancomycin. Postoperatively, the patient developed a broncho-esophageal fistula, and was reconstructed with a two-stage colonic esophageal colonic interposition three months after the fistula was closed surgically. On postoperative day nine, the patient developed symptomatic PMC of the interposed colon segment, whereas the in situ colon was spared. Therapy with oral vancomycin for three weeks eradicated the infection.
Conclusions:
Pseudomembranous colitismay develop in the interposed colon after a esophageal colonic interposition, even absent inflammation of the in situ colon. Previous infection with C. difficile may have increased the risk in this patient.
Case Report
After receiving neoadjuvant chemoradiation, an otherwise healthy 47-year-old man underwent a robot-assisted Ivor-Lewis esophagogastrectomy for localized esophageal cancer. Postoperatively, the patient developed symptomatic tachycardia and diarrhea secondary to Clostridium difficile. Given the severity of the patient's diarrhea and tachycardia, the decision was made to start him on oral vancomycin instead of the less-efficacious metronidazole. The diarrhea and tachycardia resolved soon after the start of therapy. The vancomycin was continued for 10 days. As the patient was asymptomatic on completion of therapy, no repeat cultures were obtained.
At the two-week outpatient follow-up, the patient complained of persistent cough and dysphagia. Bronchoscopy and esophagogastroduodenoscopy (EGD) confirmed a broncho-esophageal fistula, and the patient underwent a re-do thoracotomy, resection of the intrathoracic stomach, creation of a cervical esophagostomy, and closure of the fistula with a muscle flap. Postoperatively, the patient received intravenous piperacillin-tazobactam and vancomycin until discharge.
About three months later, with a normal preoperative diagnostic mesenteric angiogram, the patient underwent colonic esophageal interposition and re-establishment of gastrointestinal continuity. The right side of the colon was used as a substernal, isoperistaltic interposition graft. Preoperatively, the patient had normal bowel movements. Polyethylene glycol-3350 (with no antibiotics) was used for preoperative bowel preparation. Intraoperatively, the interposed colon was noted to be well vascularized throughout its length. Postoperatively, the patient was given cefuroxime, aztreonam, and metronidazole per our protocol. We routinely administer broad-spectrum antibiotics to our esophagectomy patients until a swallow study confirms the absence of an occult anastomotic leak. After his swallow study confirmed as much on day five postoperatively, the patient was started on an oral diet, and antibiotics were discontinued.
On postoperative day nine, the patient developed symptomatic tachypnea, tachycardia, and leukocytosis without abdominal tenderness, distention, or diarrhea. A repeat contrast swallow study was negative for a leak. Computed axial tomography (CT) of the chest, abdomen, and pelvis showed only a small left pleural effusion and pericardial effusion with no evidence of pulmonary embolus, air space disease, ischemic bowel, or collections. The patient was started on broad-spectrum antibiotics (piperacillin-tazobactam and linezolid), and oral intake was withheld. However, the tachycardia and leukocytosis persisted after five days of treatment. Therefore, the patient underwent left video-assisted thoracoscopy, pleural and pericardial fluid sampling, bronchoscopy, and EGD. The EGD confirmed an intact anastomosis, but pseudomembranes were noted in the distal portion of the interposed colon (Fig. 1). The friable mucosa was not biopsied because of concern about perforating the thoracic colon. Unfortunately, given the patient's prolonged fasting status, the lumen of the interposed colon was clean, with no mucus, fluid, or debris available for culture. No attempt was made to obtain intraluminal washings, as the yield was believed likely to be low. The patient was started on oral vancomycin. The tachycardia and leukocytosis resolved soon after. All cultures from the pericardium, pleura, blood, stool, and urine were negative. The vancomycin was continued for three weeks. A mild anastomotic stricture but no pseudomembranes were noted on repeat EGD at that time.
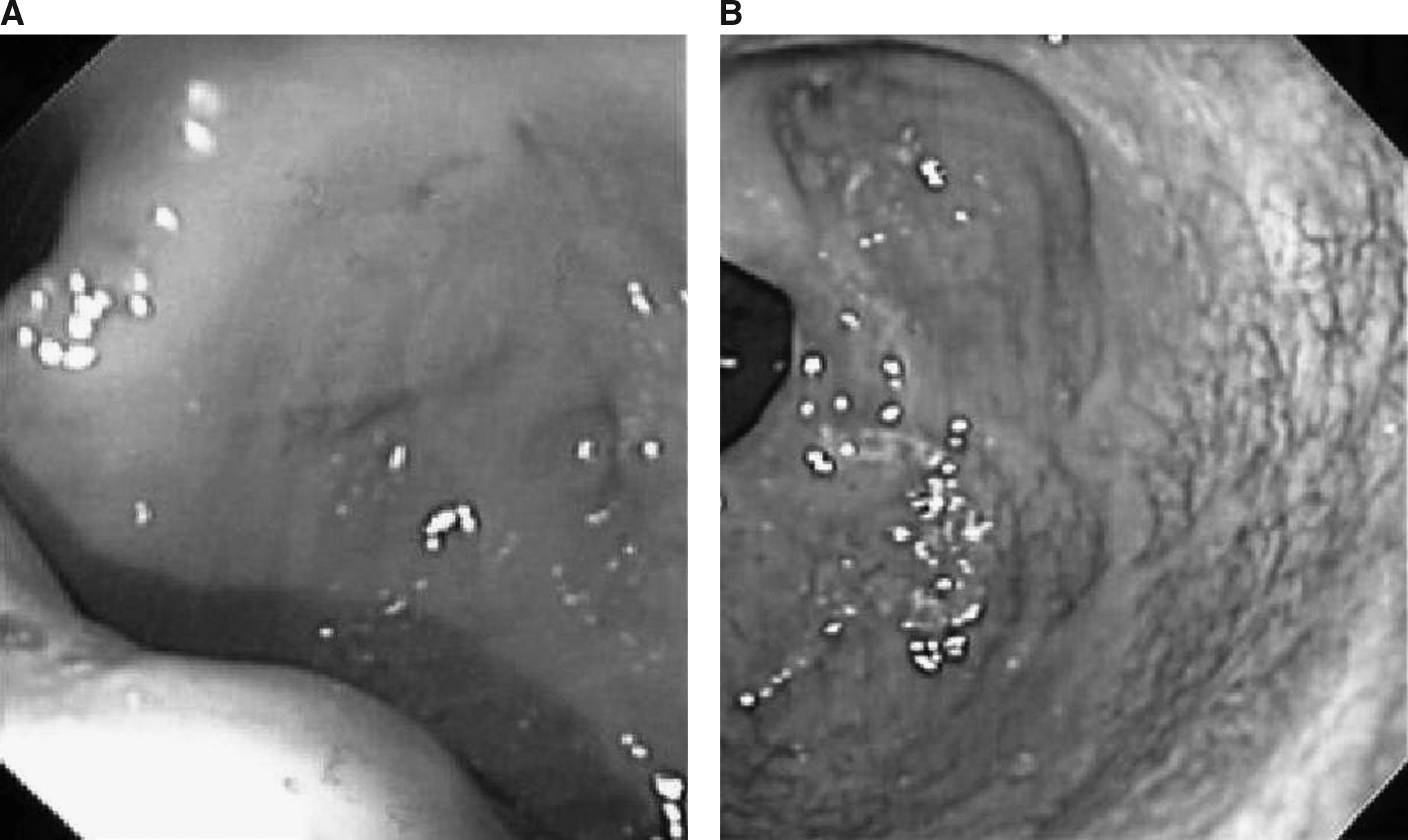
Views of esophagogastroduodenoscopy. (
Discussion
This is the first reported case of PMC affecting the intrathoracic, interposed colon of an esophagectomy patient. This case of symptomatic intrathoracic PMC occurred (with reactive pleural/pericardial effusions) in the absence of symptomatic inflammation of the in-situ colon (i.e., abdominal pain, distention, or diarrhea) or radiologic evidence of such (i.e., bowel thickening, stranding). The diagnosis of C. difficile colitis of the conduit was made because of the presence of pseudomembranes, the response to oral vancomycin, and the exclusion of other sources of sepsis. It is unfortunate that we were unable to obtain a confirmatory biopsy or culture during the EGD. However, in clinical practice, the presence of pseudomembranes on endoscopy and a positive response to therapy are usually sufficient to make the diagnosis of C. difficile infection without the need for confirmatory cultures or biopsies. The overgrowth of C. difficile and the subsequent development of PMC in the conduit were likely due to the absence of an anaerobe-rich fecal stream in the interposed colon. Our overuse of antibiotics after the interposition procedure could have been a contributing factor. Previous case reports of fulminant postoperative PMC affecting the in-situ colon but not the transplanted, interposed colonic segment of esophagectomy patients have suggested that C. difficile-associated PMC requires exposure to enterically excreted antibiotics in the fecal stream and thus could not affect the intrathoracic colon [1]. This case suggests that PMC of the transposed colon can occur if the colon is colonized with C. difficile that overgrows in the absence of an anaerobe-rich fecal medium.
Treatment of patients who have already been started on an oral diet is straightforward, involving oral administration of metronidazole or vancomycin to achieve high intraluminal concentrations. Although equally effective in mild disease, oral vancomycin is superior to oral metronidazole in treating fulminant disease [2]. Emerging oral therapies for C. difficile infection include teicoplanin, fusidic acid, nitazoxanide, tolevamer, tinidazole, and rifaxamin [3]. The management of such a case would have been much more complex if the PMC had occurred early in the postoperative period, before the anastomosis had healed and with the patient still fasting. The intravenous administration of metronidazole is not effective in such a circumstance, as biliary excretion of the drug occurs distal to the interposed colonic segment, likewise, intravenous vancomycin is not an option as it is excreted renally. The risk of colitis-associated complications must be weighed against the risks of early postoperative administration of oral medications. Intravenous immunoglobulin (IVIG) may be an option in such a situation [4], but data on the utility of IVIG are still lacking, and the cost is high.
Preventing PMC in the interposed colonic segment in a patient with a history of C. difficile infection may be a challenge. Judicious use of antibiotics reduces the incidence of PMC [5]; however, this effect may not be as significant for interposed colonic segments that are not exposed to bile and enterically excreted antibiotics. The use of oral vancomycin in asymptomatic carriers decreases short-term colonization by 90%, but recurrent colonization appears in 80% of patients as early as 12–28 days after treatment. These data suggest that treating patient with oral vancomycin 10 days prior to surgery may decrease the incidence of C. difficile colonization in the transplanted colonic segment at time of surgery [6]. The prophylactic use of intravenous metronidazole perioperatively is illogical, as the antibiotic does not reach the interposed colon, and with regard to the in-situ colon, in the absence of diarrhea, most of the antibiotic is absorbed by the small bowel before reaching the colon. Evidence also suggests that using metronidazole for prophylaxis only increases the likelihood of relapse and promotes the development of antibiotic resistance [5]. Intraoperatively, intraluminal washout of the transplanted colonic segment with vancomycin enemas may be considered as a form of PMC prophylaxis as long as care is taken to control contamination of the operative field by the intraluminal contents. In the light of the low risk of fulminant intrathoracic colitis, a patient's history of PMC should not be an indication for jejunal interposition, given the technical complexity, the higher morbidity, and the worse quality of life associated with that procedure.
In conclusion, C. difficile-associated pseudomembranous inflammation of the interposed colon can occur in esophagectomy patients. This rare complication is probably more likely in patients with a history of C. difficile infection, as they have a greater risk of being colonized by the organism [6]. In our opinion, however, colonic interposition in such patients should not be abandoned because of concerns about this rare complication. Although there are no studies addressing the prevention of this rare complication, after review of the literature on C. difficile infection prevention, we believe that prophylactic oral vancomycin 10 days prior to surgery, intraoperative vancomycin washout of the colonic segment, and judicious use of perioperative antibiotics may help reduce the risk. Oral vancomycin (or IVIG if the patient is not ready for oral intake) may be used to treat established pseudomembranous inflammation of the interposed colon.
Footnotes
Author Disclosure Statement
No competing financial interests exist.