
Abstract
Abstract
Background:
Tight glucose control has been advocated as a method to improve outcomes of surgical critical care. However, continuous infusion of insulin has potential morbidity (e.g., neurologic consequences of hypoglycemia), and it remains unclear to what degree the glucose concentration must be controlled. We examined our performance in instituting a protocol for tight glucose control in our surgical intensive care unit (ICU).
Methods:
Prospective study of 220 consecutive patients (February, 2003–March, 2006) who received an infusion of insulin for glucose control for >24 h by protocol. Data collected included age, acuity (Acute Physiology and Chronic Health Evaluation [APACHE] III) score, sex, history of diabetes mellitus, organ dysfunction (Marshall), and death or survival. Infusion-related data included initial glucose concentration, time to glucose <120 mg/dL, h/day of glucose <110 mg/dL and <140 mg/dL, duration of infusion (days), insulin units/day, year of therapy, and complications. Analysis was performed by χ2, analysis of variance, and logistic regression, with p < 0.05 considered significant.
Results:
Insulin drips were required by 10.2% of patients (287/2,804); 29 of these (10.1%) had diabetes mellitus. The mean APACHE III score for the treated patients was 77 ± 2 (standard deviation), and the mortality rate was 24%. Hypoglycemia (<60 mg/dL) occurred in 4.2% of patients. The trigger insulin concentration decreased over time (2003 vs. 2005) from 249 ± 14 to 160 ± 5 mg/dL, and the h/day of glucose <140 increased from 11 ± 1 to 16 ± 1. However, age, acuity, APACHE III, days of insulin, time to achieve glucose <120, h/day of glucose <110, and mortality rate were unchanged. By logistic regression, only the year of treatment (odds ratio [OR] 1.871; 95% confidence interval [CI] 1.177, 2.972; p = 0.008] predicted success in controlling the blood glucose concentration to <140 mg/dL; age, illness severity, diabetes history, and trigger glucose concentration [OR 0.996; 95% CI 0.992, 1.001; p = 0.11] did not.
Conclusions:
Success in implementing tight glucose control was modest, albeit improving, despite a specific protocol for administration. No medical reason could be identified for inability to achieve tight glucose control; therefore, successful implementation must be volitional. Education, particularly regarding hypoglycemia, and possible refinement of our protocol may improve our ability to control blood glucose in our ICU.
Many investigators have described the possible mechanisms of the benefit of intensive insulin therapy [4–14]. The positive effects most likely relate to the direct effect of acute glycemic control rather than the infusion of the insulin hormone [15]. Some authors contend that the therapy minimizes derangements in normal host defense mechanisms, whereas others claim tight glycemic control modulates the release of inflammatory mediators [16–23].
Because a plethora of data suggest that improved glycemic control is beneficial in critically ill surgical patients, our institution undertook an initiative in February 2003 to maintain tighter blood sugar control via insulin infusion in our surgical intensive care unit (ICU). After three years of the program with prospective data collection, we assessed our practice of this technique. In particular, we determined whether our blood glucose control was becoming more stringent over time, and whether our patients having infusions were receiving larger amounts of insulin. An additional goal was to determine whether the mortality rate was changing. We hypothesized that glycemic control would improve over time, as measured by the proportion of time in a 24-h period the blood glucose concentration was <140 mg/dL as well as <110 mg/dL. We also hypothesized that stricter glycemic control would decrease the mortality rate and the number of nosocomial infections in our critically ill patients.
Patients and Methods
Data were collected prospectively on all patients admitted to the surgical ICU of New York–Presbyterian Hospital/Weill Cornell Medical Center from February, 2003–March, 2006. Included were 287 consecutive patients who received an infusion of insulin for glycemic control for at least 24 h according to an institutional protocol (see Appendix). If patients required an insulin infusion, subcutaneous insulin by “sliding scale” was prohibited. Patients who were receiving intravenous insulin admixed with parenteral nutrition solution also were excluded. The insulin infusion protocol was modified by the institution's Formulary and Therapeutics Committee Subcommittee on Critical Care Therapeutics in early January, 2006, in response to observations made during the initial data analysis for the submission of an abstract on December 1, 2005, for presentation at the 2006 Annual Meeting of the Surgical Infection Society. The trigger glucose concentration was decreased from 150 mg/dL to 110 mg/dL for patients with hyperglycemia, and the “hold” parameter for interruption of the insulin infusion for hypoglycemia was liberalized. The protocol changes were accompanied by an educational initiative to inform critical care nurses and surgical house staff of the changes and the importance of adherence to the protocol.
Sixty-five discrete data elements were collected daily for the first seven days (midnight to 11:59
Insulin infusion-related data collected were the initial plasma glucose concentration (trigger), time to achieve a glucose concentration <120 mg/dL, h/day that the blood glucose concentration was maintained <140 mg/dL and <110 mg/dL, the time of day of the start of the infusion, the duration of infusion (days), insulin units/day, and the year of therapy. Hypoglycemia (blood glucose <60 mg/dL) and any complications related thereto were recorded. The development of nosocomial infections, the source of infection, and the specific pathogen(s) isolated were noted as well. Nosocomial infections were defined according to the criteria of the U.S. Centers for Disease Control and Prevention [25] except for hospital-acquired/ventilator-associated pneumonia, the diagnosis of which required the identification of >104 colony-forming units (cfu)/mL of a predominant pathogen by quantitative culture of sputum collected by bronchoscopic bronchoalveolar lavage [26].
Univariable analysis of coordinate variables was performed by contingency table analysis with the Fisher exact test, and univariable analysis of continuous variables was performed using the Mann-Whitney U test. Another non-parametric test (Kolmogorov-Smirnov) was used to examine differences in data that were not normally distributed according to determination of skewness and kurtosis. Changes in continuous variables with respect to time were analyzed by repeated measures analysis of variance (ANOVA) with Bonferroni correction, and correlations were made by the Pearson method. Differences in survival were assessed by Kaplan-Meier analysis. Statistical significance was defined as p = 0.05. Univariable results of possible significance (p < 0.15) were tested in multivariable models for independence of effect on death; the dependent variable under study after auto-correlation was excluded by matrix correlations and the Durbin-Watson statistic. For binary logistic regression analysis, the durations of blood glucose concentrations <140 mg/dL and 110 mg/dL were dichotomized on the basis of the mean values of 15 h/day and 9 h/day, respectively. This time was determined by a post-hoc analysis based on the initial results. Odds ratios (ORs) and the 95% confidence interval (CI) were determined; and the sensitivity, specificity, and goodness of fit (model χ2; Hosmer-Lemeshow test) were determined for each logistic regression model. Data are expressed as mean values ± standard error.
Results
Two thousand eight hundred four patients were admitted into the surgical ICU during the study period, of whom 287 (10.2%) required a continuous infusion of insulin for >24 h. Twenty-nine of the subjects (10.1%) had known diabetes mellitus. The mean APACHE III score for treated hyperglycemic patients was 77.4 ± 1.5 points, and the hospital mortality rate was 24.4%. The mean MOD score was 7.8 ± 0.3 points, and nosocomial infections developed in 55.1% of the study patients.
Episodes of hyperglycemia were recorded. Hypoglycemia occurred in 4.2% of patients. Although acute neurologic changes were not captured, no long-term sequelae attributable to hypoglycemia were noted during the study period.
Demographic data overall and as a function of the year of therapy are shown in Table 2. Neither age, severity of illness, organ dysfunction, the incidence of nosocomial infection, nor the mortality rate fluctuated over the study period. The mean ICU day of initiation of the insulin infusion was 3.32 ± 0.27, and the median day of initiation was 2.
APACHE = Acute Physiologic and Chronic Health Evaluation; MOD = multiple organ dysfunction; SD = standard deviation.
The mean trigger blood glucose concentration decreased over time, from 249.5 ± 13.8 mg/dL in 2003 to 160.1 ± 5.1mg/dL in 2006 (p < 0.001), with a substantial incremental decrease achieved in 2006 after the protocol was modified and reinforced (Table 3). During this same time, the duration of insulin infusion increased significantly, from 8.8 ± 0.8 to 14.8 ± 2.5 days (p < 0.05), increasing by a full five days from 2005 to 2006. Between 2003 and 2006, the lower trigger glucose concentration resulted in a significant reduction in the elapsed time to achieve a glucose concentration <120 mg/dL, with essentially all of the decrease occurring in 2006 compared with 2005. Similarly, the mean h/day of glucose <140 mg dL and <110 mg/dL increased significantly over time, with a dramatic increase in 2006 (Table 3; Fig. 1). The relation between the time of day the insulin infusion was started and the duration of insulin therapy on day one is shown in Figure 2. The insulin dose (units/day) decreased significantly (p < 0.01) with respect to time (Fig. 3), even as control of blood glucose improved.

Mean duration of time per day that glucose concentration was kept below 140 mg/dL (light bars) (overall mean 15.0 ± 0.5 hours) or 110 mg/dL dark bars (overall mean 9.4 ± 0.4) hours. Both relationships are statistically significant (p < 0.01) with respect to time.
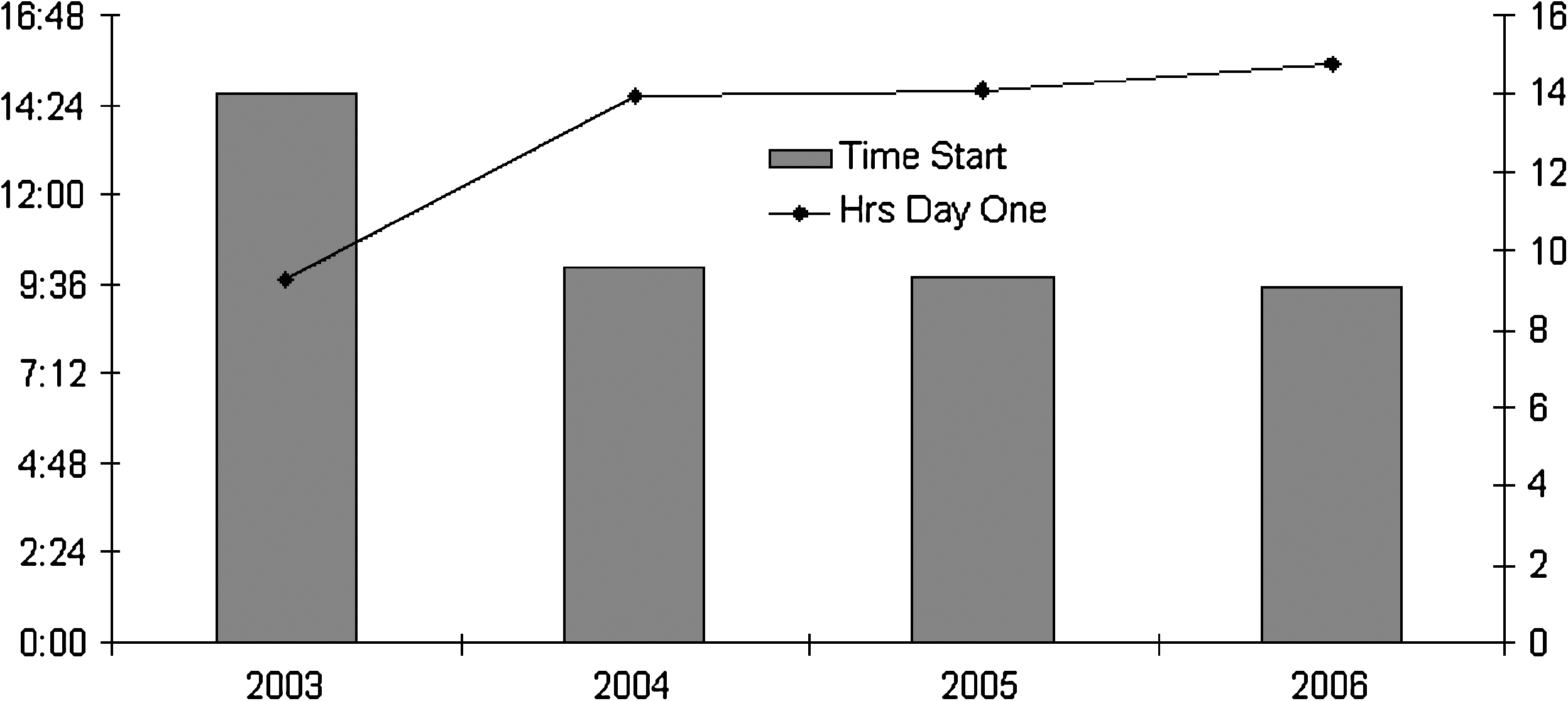
The hour of starting a continuous insulin infusion is shown, stratified by year of therapy. Shown together is the total duration of insulin infusion therapy on day one of the infusion. Earlier start times (p < 0.05) were associated with longer duration of therapy (p < 0.05).
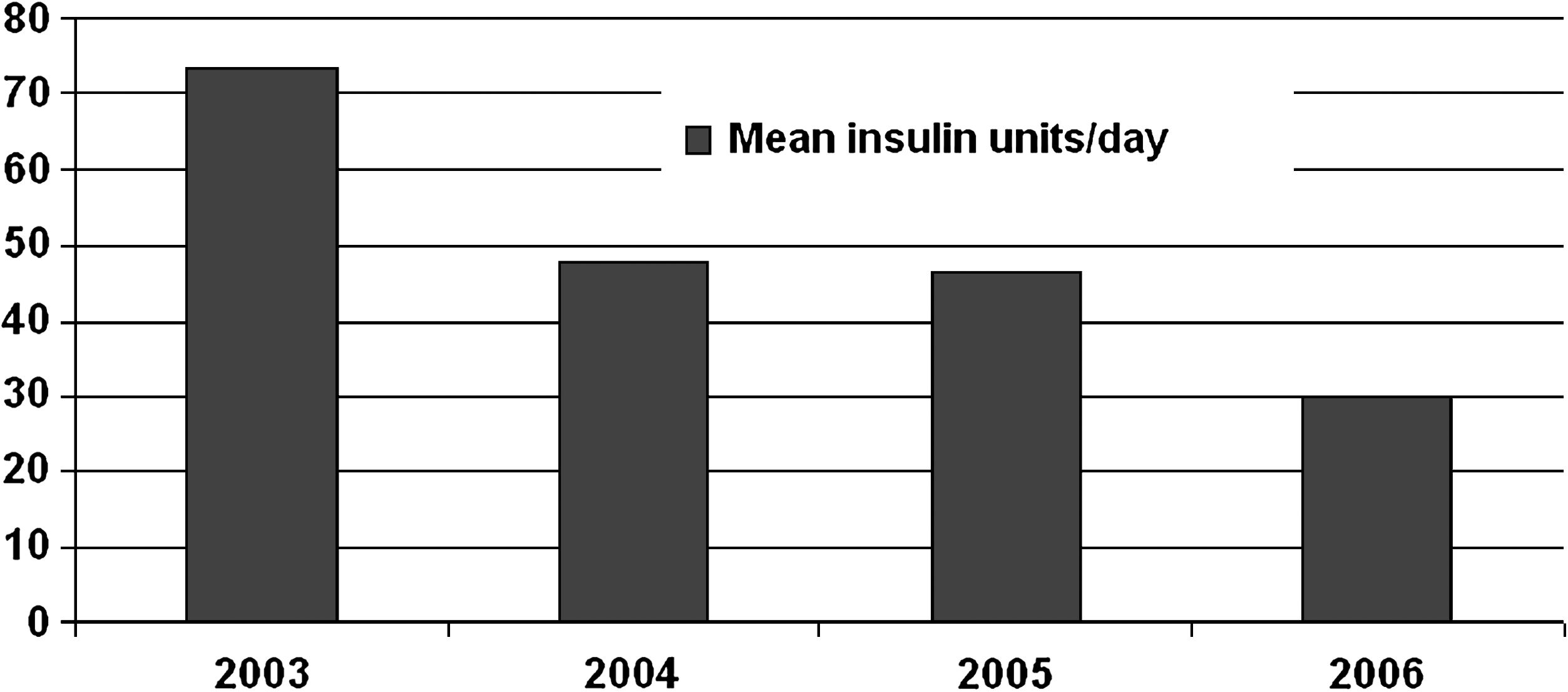
The mean daily dose of insulin (units/day) is shown, stratified by year of therapy. The amount of insulin required daily to maintain control of blood glucose concentration decreased significantly (p < 0.01), despite tighter control over time.
Mean ± standard deviation.
Glucose concentration at which insulin infusion was initiated.
Three binary logistic regression models were created for the dependent variables duration of blood glucose < 140 mg/dL (Table 4), development of a nosocomial infection (Table 5), and death (Table 6). By logistic regression, the year of treatment (OR 1.871; 95% CI 1.192, 2.717; p = 0.005), trigger glucose concentration (OR 0.994; 95% CI 0.988, 0.999; p = 0.025), the start time of insulin infusion (OR 0.929; 95% CI 0.887, 0.972; p = 0.001), and the ICU day of start of insulin infusion (OR 1.145; 95% CI 1.009, 1.299; p = 0.036) predicted success in controlling blood glucose <140 mg/dL (dichotomized at the mean value of ±15 h/day). Therefore, requiring insulin later in the ICU stay rather than nearer to admission, and starting insulin as soon as possible after the trigger blood glucose criterion is met, are associated with better glucose control. Also, by logistic regression, the development of a nosocomial infection was independently associated with insulin therapy later in the ICU stay (OR 1.223; 95% CI 0.987, 0.998; p = 0.007), a larger insulin dose requirement (units/day)(OR 1.015; 95% CI 1.005, 1.025; p = 0.004), but paradoxically a lower trigger glucose concentration (OR 0.993; 95% CI 0.987, 0.998; p = 0.029).
Model χ2 49.220, p value 0.0001; Nagelkerke R2 0.284; Hosmer-Lemeshow test χ2 11.051, p value 0.199.
ICU = intensive care unit; PMH = positive medical history; Trigger = glucose concentration at which insulin infusion was initiated.
Model χ2 39.366, p value 0.0001; Nagelkerke R2 0.276; Hosmer-Lemeshow test χ2 6.565, p value 0.584.
Trigger = glucose concentration at which insulin infusion was initiated.
Model χ2 118.490, p value 0.0001; Nagelkerke R2 0.664; Hosmer-Lemeshow test χ2 7.464, p value 0.488.
APACHE = Acute Physiology and Chronic Health Evaluation; MOD = multiple organ dysfunction.
The binary logistic regression for death is shown in Table 6. The Kaplan-Meier survival curve is shown in Figure 4. The mortality rate was decreased significantly by a mean duration of glucose concentration <140 mg/dL of more than 15 h/day (OR 0.78; 95% CI 0.623, 0.831; p < 0.0001).
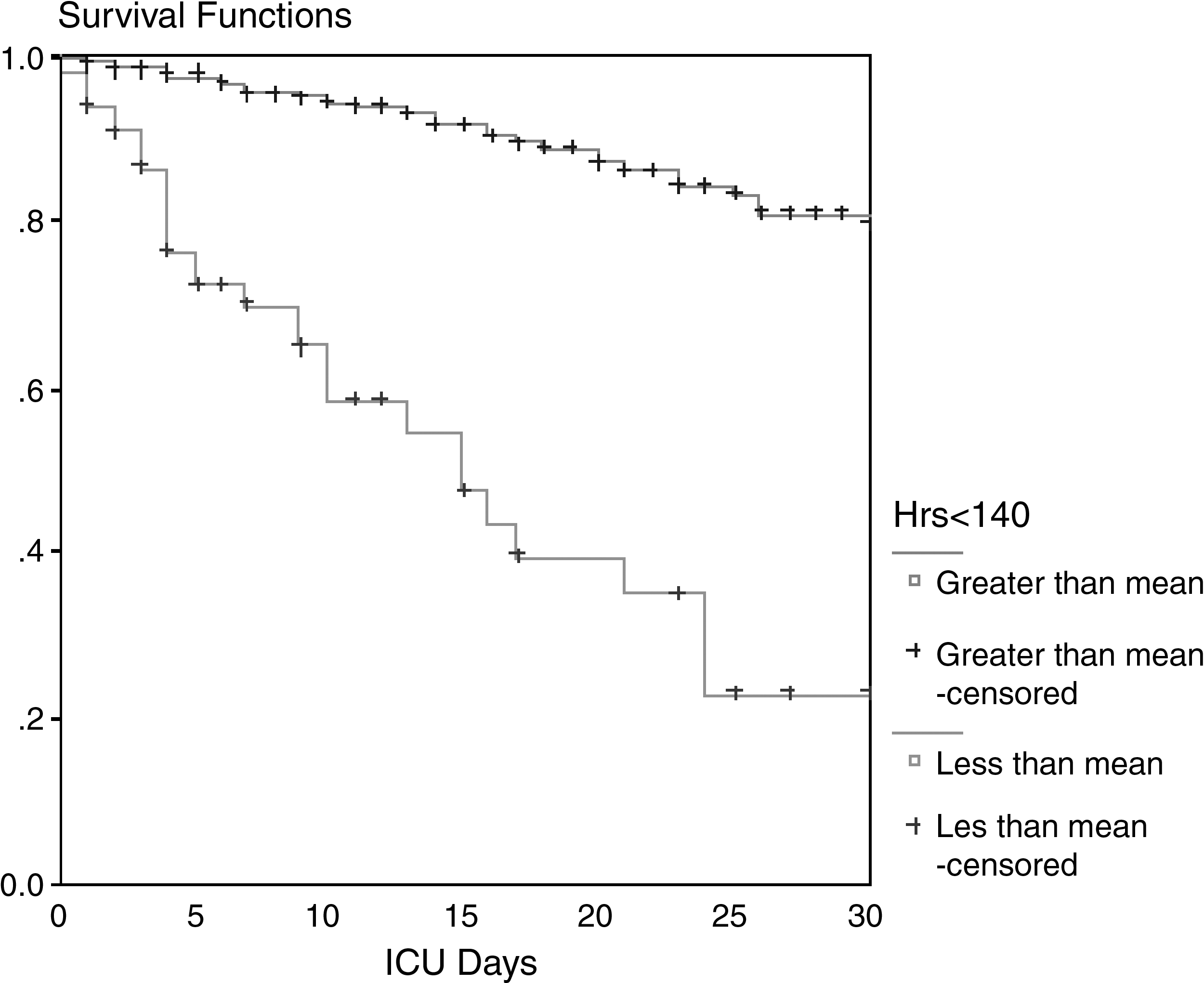
Kaplan Meier survival plot of glucose concentration times day <140 mg/dL. Time was dichotomized at the mean value of 15 hours/day. The curves are significantly different (p < 0.01).
Discussion
Multiple mechanisms can contribute to the potential benefits of insulin infusion in critically ill patients [27–30]. Most of the benefits appear to be related to prevention of hyperglycemia, which affects outcomes adversely. In the trauma population, Yendamuri et al. have found that hyperglycemia independently predicts longer ICU and hospital LOS as well as the mortality rate. These authors substantiated greater infectious morbidity for both mild (glucose concentration >135 mg/dL) and moderate (glucose concentration >200 mg/dL) hyperglycemia [31]. Other investigators have observed trauma patients to fare worse when the initial glucose concentration is elevated [32]. Importantly, glycemic variability also appears to predict death in critically ill patients [33].
The anti-inflammatory effects of insulin infusion may contribute to its benefits in critically ill patients. Several cellular mechanisms may be beneficial. Part of the improvement may be related to protection of mitochondrial respiration and prevention of excessive inflammation. Hyperglycemia without antagonism may reduce neutrophil activity and alter specific concentrations of early pro-inflammatory cytokines, including tumor necrosis factor-alpha and interleukin-6 [34].
Intensive insulin therapy may work at the endothelial level by suppressing inducible nitric oxide synthase (iNOS) expression in liver and skeletal muscle, possibly in part via reduced nuclear factor-κB activation. Other actions of insulin may include lowering circulating NO concentrations in both survivors and non-survivors [35]. The metabolic actions of insulin may also benefit other aspects of the physiology of critically ill patients [36]. For example, insulin may contribute to a partial correction of the abnormal serum lipid profile that characterizes critical illness and counteract the associated catabolism [37,38]. Nonetheless, other authors found that increased insulin administration was positively associated with death in critically ill patients regardless of the prevailing blood glucose concentration [39].
In particular, surgical patients may have a better response to tight glycemic control than do medical patients [40]. Whereas insulin infusion was beneficial in an 800-patient study in a combined medical and surgical ICU [41], a meta-analysis examining 35 trials employing insulin infusion in critically ill patients found contrary results. In this meta-analysis, Pittas et al. showed that insulin therapy decreased the mortality rate significantly in the surgical ICU when the aim of therapy was glucose control regardless of whether the patient had diabetes mellitus [42]. These authors also observed a near-significant trend toward fewer deaths in critically ill surgical patients with acute myocardial infarction who did not receive reperfusion therapy. In this meta-analysis, the authors found no randomized trials of insulin in the medical ICU setting. More recently, a large randomized, controlled trial demonstrated that intensive insulin therapy significantly reduced morbidity, but not the mortality rate, among medical ICU patients [43].
The analysis of our initial experience with intensive insulin infusions yielded notable results from a process improvement standpoint. First, our glucose trigger decreased substantially over the study period. This decrease was accompanied by better control of blood glucose to <140 mg/dL, as measured during a 24-h period. Concurrently, we noted that the hours of infusion required to achieve a blood glucose concentration <120 mg/dL decreased. Although outcomes appeared to be more favorable if a lower glucose threshold initiated the insulin therapy, we do not have data regarding any delay definitively causing an adverse outcome. These results were demonstrated most prominently after the revision of our protocol in early 2006, and were accompanied by reinforcement to the house staff and nursing teams by the surgical intensivists at our institution. Successful protocol implementation required intensive teaching for the ordering and treating personnel. Directed feedback also may be necessary to evoke a beneficial effect of this therapy because interventions such as insulin infusion may yield only subtle benefits while being notably labor intensive.
Our results also demonstrated that an essential feature of successful euglycemia is early recognition and treatment of “borderline” hyperglycemia before sustained and difficult-to-treat hyperglycemia can ensue. We noted that in our more recent study period, patients were receiving lower cumulative insulin doses to control their glucose concentration even though the duration of their drips was longer. This observation may also convey that our personnel may have been attempting to wean patients from insulin infusions prematurely during the earlier portion of the study period. Another finding was that the mean start time of infusion changed to earlier in the day during the study (Fig. 2). This may have occurred because nurses and residents may have felt more independent in the later phases of the study, and the de facto trigger was not the presence of the attending physician during morning ICU rounds. Later in the study, we found that despite tighter control, the total insulin dose was less. This result suggests that earlier glucose control may decrease subsequent insulin resistance.
Perhaps the most important feature of our study centers on the difficulty inherent in creating an insulin infusion protocol in a locale where the physicians and nurses are not familiar with the initiative. In the beginning phases of this protocol, the trigger was a mean of about 250 mg/dL despite aggressive education of all staff on the merits of the protocol. We would have thought that because the protocol-specified trigger was 120 mg/dL for two consecutive values, a much lower mean trigger would have been observed. We did see this in the later phases of the study but not initially.
Several theories may explain why our study failed to show a stronger discernible benefit in terms of mortality rate or nosocomial infections in patients treated with intensive insulin infusion. Notably, a major meta-analysis by Weiner et al. in 2008 had findings that paralleled ours in that a mortality difference was not observed in patients receiving insulin infusions [44]. A type II error may have been present, or perhaps the effectiveness of our infection diagnoses and treatment protocols masked an effect. Perhaps our study population differed from prior studies with this modality owing to a higher severity of illness in our patients prior to the initiation of insulin therapy. Consequently, our patients may already have developed substantial organ dysfunction, and aggressive maintenance of euglycemia has never been shown to be superior to conventional therapy at reversing organ dysfunction.
Another explanation is that the insulin infusions were not employed frequently or aggressively enough in our entire group of critically ill surgical patients; our incidence of insulin infusions was only 10.3%. Other authors likewise have also that the implementation of insulin infusion protocols may not always be associated with initial complete compliance [45]. The theory that a lack of proper glucose control masked more beneficial results is supported by the Kaplan-Meier analysis, which showed a significantly higher survival rate in patients who were controlled <140 mg/dL. Only in 2006 did we finally improve our insulin infusion process such that patients are controlled <140 mg/dL for the majority of the day. Perhaps if we had been more aggressive with blood sugar control with more patients, we would have seen an unequivocal mortality benefit. On the other hand, a practice targeting blood glucose control <140 mg/dL may be sufficient to prevent the ill consequences of hyperglycemia and mitigate the potential damage of hypoglycemia.
We concluded that insulin therapy in the ICU setting is difficult to implement successfully. The practice requires persistence and vigilance to maintain constant euglycemia in critically ill patients. However, we also demonstrated superior survival for patients who were properly controlled for the majority of the 24-h period, with a blood glucose concentration <140 mg/dL. Further studies will demonstrate whether we can maintain stringency in our protocol and whether the provision of successful intensive insulin therapy to a larger cohort of patients will produce demonstrably decreased mortality and nosocomial infection rates.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Appendix
Presented in part at the 26th Annual Meeting of the Surgical Infection Society, San Diego, California, April 2005.