
Abstract
Abstract
Background:
We report a series of six immunocompetent patients who were believed initially to have primary bone sarcomas, but turned out to have subacute osteomyelitis.
Methods:
Case report and review of relevant literature.
Results:
All our patients were treated with antibiotics and recovered fully from the infection. Only one patient had a recurrence with the same offending microorganism, which resolved after a longer period of intravenous antibiotic.
Conclusions:
Subacute osteomyelitis and bone tumors can be similar in presentation, and the key to proper diagnosis is histopathological and microbiological confirmation in biopsy specimens.
Patients and Methods
All patients referred to the Orthopedic Oncology Unit, University of Malaya Medical Center, from January 1, 2007, to December 31, 2007, for whom there was an initial suspicion of primary bone sarcoma on the basis of the clinical and radiographic findings were reviewed. Only cases with the final diagnosis of osteomyelitis proved by culture are included in this review. We recorded the demographic details, site of infection, clinical presentation, investigations (laboratory, radiologic, and histopathological), duration and route of antibiotic therapy, and complications.
Results
The six patients had clinical or radiographic findings suggesting malignant bone lesions, which later proved to be subacute pyogenic osteomyelitis on histopathological examination and bacteriological confirmation. There were four male and two female patients with a mean age of 19.3 years (range 7–35 years). They consisted of one child, three adolescents, and two adults, as shown in Table 1.
None of the patients had predisposing factors.
R = right; L = left.
Clinical presentation
Pain was a symptom in all the patients. Two patients complained of swelling, and none were febrile at presentation. The delay between the onset of symptoms and diagnosis ranged from one to six mos (average three mos). Two patients had histories of significant weight loss (more than 10 kg within a month) associated with loss of appetite. There were no underlying diseases or history of antibiotic treatment in any patient. None of the patients had a history of trauma or surgical procedure performed on the involved bone. Physical examination revealed normal overlying skin with no dilated veins or discharging sinuses in any patient. Two patients presented with swelling, which was slightly tender, warm, and firm with ill-defined margins. Otherwise, there was no limitation of movement of the adjacent joints and no associated joint effusion.
Microbiology and laboratory investigations
On admission, only one patient had leukocytosis (>11 × 109 /L), and three patients had significant elevation of the erythrocyte sedimentation rate (ESR) (>100 mm/h), as shown in Table 2. Core needle biopsy was performed for all patients, and the samples were sent for histopathological and microbiological diagnosis. Histologically, all biopsies showed a subacute inflammatory reaction with no evidence of malignancy. Staphylococcus aureus (methicillin-sensitive) was cultured from the biopsy specimens in all cases. Cultures for tuberculosis and fungi were negative. Blood cultures were not carried out in these patients, as there was no systemic evidence of sepsis.
WBC = white blood cell count; ESR = erythrocyte sedimentation rate; IV = intravenous; MSSA = methicillin-susceptible Staphylococcus aureus.
Imaging
All the patients had radiographs of the involved bones, which were suggestive of primary bone tumors, as illustrated in Figures 1, 2, and 3. There was distal femoral involvement in two cases and involvement of the proximal femur, proximal tibia, proximal radius, and ilium in one case each. All the cases involved the metaphysis. Radiologically, three cases were consistent with Ewing sarcoma and the other three with osteosarcoma (Tables 1 and 2). A lamelliform (onion skin) appearance was found in two cases, sclerosis in four, Codman triangle in two, and osteolysis in one. Case 5 was the only case that had magnetic resonance imaging (MRI) done (Figure 4). These results, too, were suggestive of primary bone neoplasm, with gross involvement of the distal femoral metaphysis and soft tissue extension. Radiologically, there were no changes to suggest abscess formation or chronic osteomyelitis such as sequestrum or involucrum in any of the cases.

Anteroposterior and lateral radiographs in Case 1. There is gross involvement of proximal end of right femur with disruption of cortex and bowing, along with obliteration of medullary cavity.
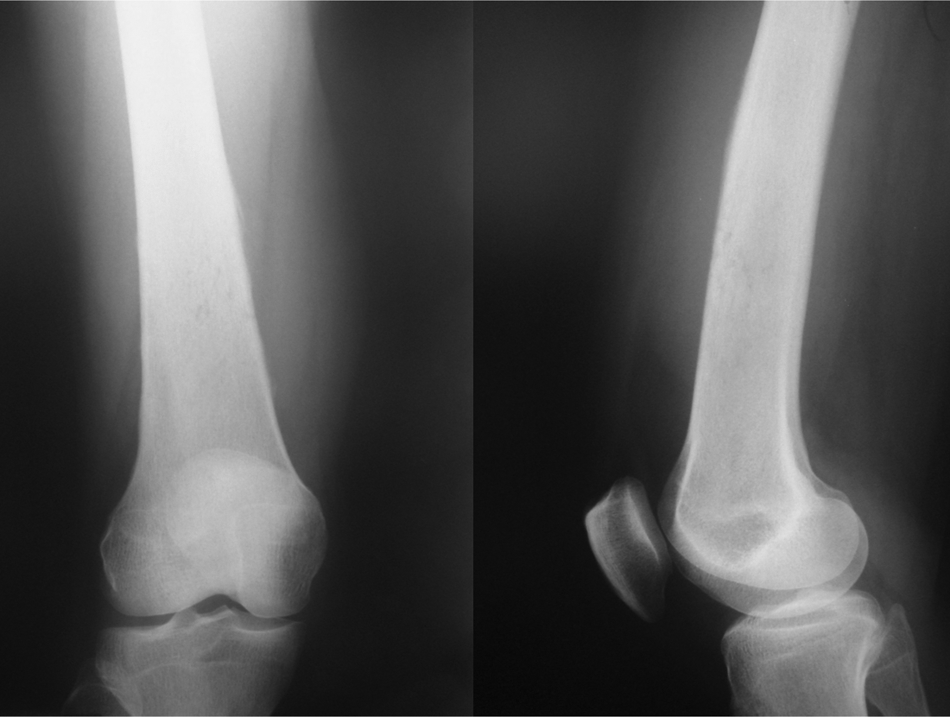
Radiographs in Case 2 demonstrate “sunburst” appearance over lower third of femur.

Radiographs in Case 6 reveal involvement of distal end of right radius with expansion of bone and break in medial cortex.
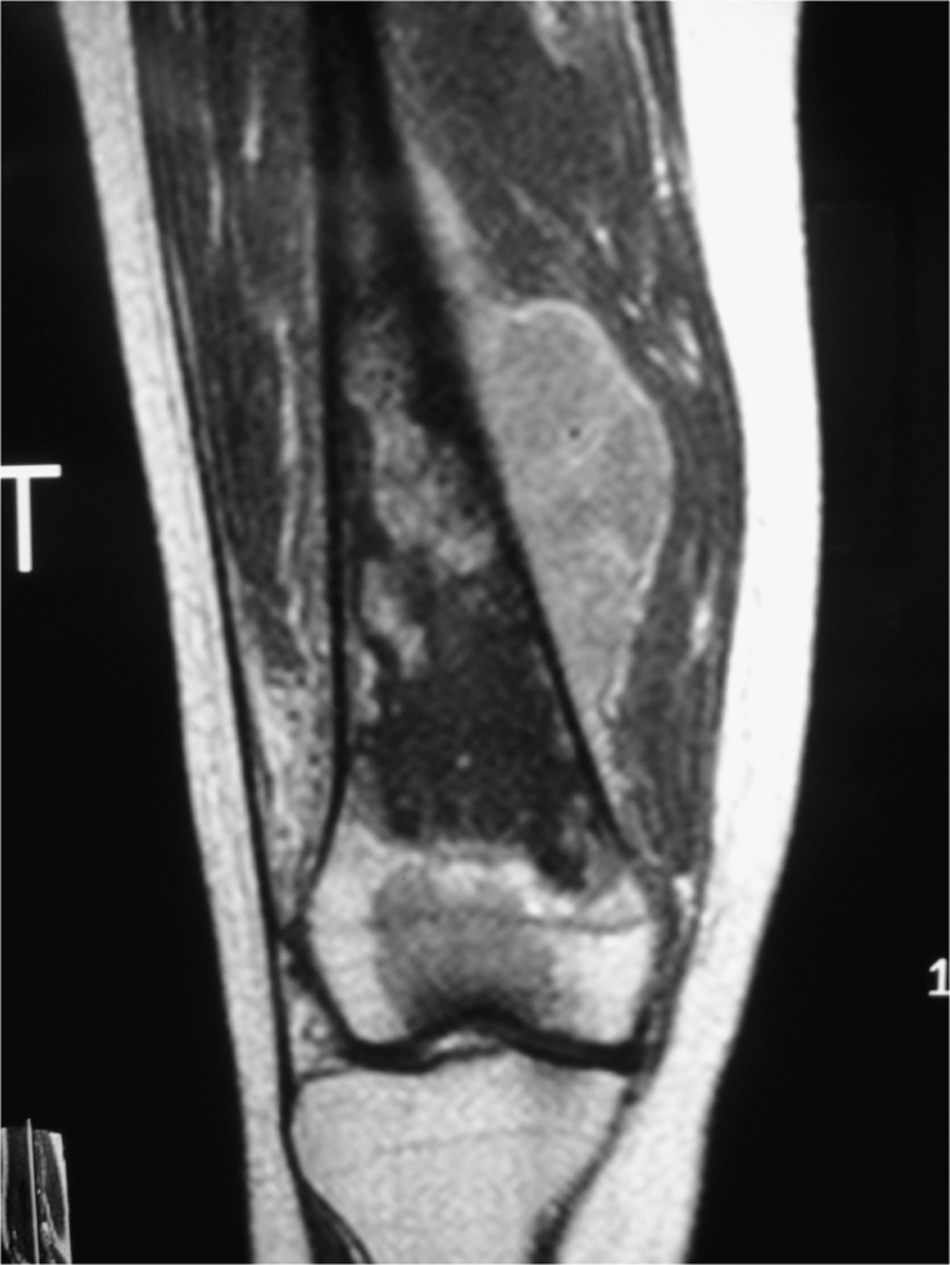
Sagittal view of magnetic resonance image of Case 5 showing gross involvement of distal femur with break in cortex and soft tissue extension of lesion.
Treatment
All patients were started on intravenous cloxacillin on the basis of antibiotic susceptibility results. Two patients were treated with six weeks of intravenous antibiotic, whereas the other four patients were given two weeks of intravenous followed by oral antibiotic. The total duration of treatment was three months (Table 2).
Follow-up and outcome
The follow-up period ranged from 13 to 36 months (Table 2). Other than the biopsy, no surgical intervention was carried out. One patient had recurrence of osteomyelitis with the same organism within six months of completing her treatment. She presented with similar pain over her right buttock and was started on four weeks of high-dose intravenous cloxacillin followed by eight weeks of oral antibiotic, and her symptoms subsided. Case 1 was a 14-year old student with right proximal femoral involvement who demonstrated a 4-cm shortening of the involved limb at the last review. The infection had caused weakening of the bone, which led to bowing of the proximal femur, giving rise to the shortening. He is scheduled for bone lengthening. All the other patients had a good outcome eventually.
Discussion
These six cases illustrate the common clinical diagnostic challenges, as subacute osteomyelitis may mimic various bone tumors, resulting in delay in diagnosis and treatment [2,3,5]. The cases were referred to us with an initial clinical and radiologic suspicion of primary bone sarcoma but turned out to be subacute osteomyelitis on further investigation.
All our patients presented with pain and other non-specific symptoms. There were no overt symptoms to suggest infection such as prolonged fever or inflammation of the involved site. The clinical course in subacute osteomyelitis is insidious, with symptoms being present for more than two weeks [2,3]. Patients often are afebrile with a paucity of systemic reaction to the infection. On the other hand, pain of moderate intensity is a constant feature and may suggest the diagnosis [1–3]; it was the presenting complaint in all our patients.
All the patients in our series were otherwise healthy with no underlying co-morbidities. The presumed cause for the indolent nature of subacute osteomyelitis, which differentiates it from other forms of osteomyelitis, is increased host resistance combined with low virulence of the infecting organism [1–3].
Laboratory investigations apart from raised ESR in three patients were not especially helpful in establishing the diagnosis. King and Mayo [2] demonstrated a raised ESR in 75% of their patients, whilst only 22% showed elevated white blood cell counts. In subacute osteomyelitis, the total white blood cell counts usually are normal, and an elevated ESR is a more reliable finding [1].
Radiologic findings in subacute osteomyelitis may be non-specific and suggest a benign or malignant neoplasm [4]. There was a high suspicion of primary bone sarcoma in all of our patients, with classical features such as cortical destruction, a sunburst pattern, Codman triangle, and lamelliform periosteal reaction. Multilamellar periosteal reaction (onion skin appearance) and Codman triangle can be seen in osteosarcoma, osteomyelitis, and Ewing sarcoma [4]. King and Mayo [2] described lesions with considerable amounts of layered periosteal reaction. The characteristic feature of subacute osteomyelitis noted on MRI, known as the penumbra sign, which may help distinguish subacute osteomyelitis from tumor [6], was not present in the image of Case 5, the only patient to undergo MRI.
A bone biopsy is mandatory to establish the diagnosis. The samples should always be sent for both histopathological and microbiological evaluation. The histopathological findings in subacute osteomyelitis are the presence of lymphocytes, plasma cells, and granulation tissue [3]. It is of the utmost importance to rule out malignancy, as the cultures need not always be positive in cases of subacute osteomyelitis: The positive culture rate ranges from 29% to 77% [2,3]. Staphylococcus aureus is by far the most common pathogen [1–3]. Cottias et al. reported a similar series of 21 cases. In their series, there were positive cultures in only 12 cases, and four patients were treated with surgical debridement without antibiotics. Those authors, too, had a good outcome in all cases [7].
The role of surgery in subacute osteomyelitis is questionable. Ross and Cole [8] suggested that antibiotics alone may be adequate and that surgery should be reserved for lesions with subperiosteal and joint abscesses. Other authors likewise have reported that subacute osteomyelitis could be treated successfully with antibiotics alone, and recommended that surgery be reserved for cases not responding to antibiotic therapy or those showing aggressive radiologic features [9,10]. In our series, cloxacillin was the antibiotic, as S. aureus was the only pathogen cultured. We had only one recurrence, six months after the initial treatment, and the patient was given a high dose of the same antibiotic intravenously for a longer duration. None of our patients needed surgical debridement. We recommend treating such patients with antibiotics first and reserve surgical debridement for cases that do not respond to medical treatment or in which case where there is clear evidence of abscess formation on imaging studies.
Our series confirms that differentiating subacute osteomyelitis from primary bone sarcomas remains a diagnostic challenge if we depend primarily on clinical and plain radiographic evaluation. Tissue biopsy is essential for both histopathological and microbiological evaluation. Prolonged treatment with antibiotic usually is sufficient, surgical treatment being necessary only when there is evidence of abscess formation or if patients do not respond to medical treatment alone.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.