
Abstract
Abstract
Background:
Hydatid disease is endemic in many areas of the world, where it is an important public health problem. The aim of this study was to describe a series of patients with atypically located primary hydatid disease, accompanied by a literature review.
Methods:
Six male and four female patients with atypically located hydatid cysts who presented to the Kars State Hospital between September 2004 and March 2008 were evaluated. The mean age was 42.5 years (range 17–72 years). Hydatid cysts were identified by using a combination of serology tests, ultrasonography, and computed tomography (CT).
Results:
Six of the patients underwent surgical treatment. Three patients (two with pericardial hydatid involvement and one with pancreatic involvement) were sent to a tertiary medical center for surgery, and one patient died from cardiac and renal failure two days after diagnosis.
Conclusions:
Although this disease is seen most often in the liver and lungs, it can be found in any part of the body. Hydatid disease must be considered in the differential diagnosis of cystic lesions, especially in patients who have spent time in endemic areas.
The parasite spreads from animals to humans through the fecal-oral route and is endemic in the Mediterranean, the Middle East, South America, New Zealand, Australia, South Asia, and Turkey [2,3]. A high prevalence of parasitic infection is found in the Middle East as well as North Africa [1].
The cyst can develop in almost any organ or tissue, although the liver accounts for between 60% and 70% of cases and the lungs for 5–20% [4,5]. Hydatid disease also has been described in the spleen, kidneys, heart, brain, bone, and, indeed, almost every other organ or tissue in the body [1,6,7].
The differing prevalence of hydatid disease in various locations in the body arises from the life cycle of the parasite. The liver represents the first filter where organisms enter from the intestine through the portal circulation. Most of the larvae seed the parenchyma of the liver at this stage and continue their life cycle in the form of cysts. However, some travel beyond this first microvascular barrier and reach the lungs. A small percentage of parasites (10–20%) that escape the hepatic–pulmonary filter spread between the preparenchymal and postparenchymal circles to any organ or tissue, probably through precapillary anastomoses [5,8]. In 1965, Grassi published a classification of rare forms of primary echinococcosis based on statistical data that remains valid today: (1) Infrequent: kidney, spleen, bone, muscle; (2) rare: brain, pancreas, diaphragm, thyroid gland, heart, breast, salivary glands, pelvic cavity; and (3) very rare: pituitary gland, prostate gland, adrenal glands, lymphatic ganglia, peripheral nerves, eyes, labia majora, and others [9].
Hydatid cysts cause death and morbidity by their associated complications such as secondary infection; cyst rupture into adjacent structures, which commonly involves intraperitoneal dissemination of the disease from hepatic cysts; anaphylactic reactions; and pressure on adjacent organs leading to signs such as obstructive jaundice as a result of pressure on the biliary tree [10].
In Turkey, the estimated rate of hydatid disease that requires surgery is 0.8–2 cases per 100,000 people [3, 11]. According to these data, the average number of new cases of hydatid disease in Turkey is approximately 2,000–2,500 per year. Rarer locations of primary disease account for between 5% and 30% of cases; these instances are of interest for epidemiologic reasons as well as for the diagnostic problems that sometimes lead to an unclear clinical diagnosis [8,12].
The aim of this retrospective study was to review our experience in a series of patients with unusually located primary hydatid cysts. The clinical presentations, diagnostic work-up, and treatment outcomes of the patients are discussed.
Patients and Methods
Between September 2004 and March 2008, 98 patients with hydatid disease were admitted to the General Surgery Unit at Kars State Hospital, Turkey. The medical records of these patients were reviewed. Patients were evaluated with regard to age, sex, symptomatology, treatment, complications, and length of the hospital stay (LOS).
In all patients, the diagnosis was based on the history, physical examination, laboratory tests, and radiographic examinations. Ultrasonography was performed in six patients, and computed tomography (CT) imaging was performed for all. After the diagnosis of extrahepatic hydatid disease was made, all patients were evaluated for hepatic hydatidosis. Patients who had positive or suggestive radiologic or clinical evidence of hepatic disease were excluded from this series.
After diagnosis, all patients were treated immediately with a anthelminthic drug (albendazole 800 mg/day) for one week before surgery and for at least four weeks postoperatively.
Results
The mean age of the 98 patients with hydatid disease was 37.1 years (range 10–72 years), and the male-female ratio was 59:39. Hepatic and pulmonary disease was diagnosed in 88 patients in our hospital.
We found six male and four female patients with primary hydatid disease in an unusual location. Their mean age was 42.5 years (range 17–72 years). Nine patients were examined with the echinococcal immune hemagglutination test, and the results were positive in all. Demographic features, along with radiologic and serologic findings, are summarized in Table 1.
F = female, IHA = indirect hemagglutination; M = male; NA = not available.
Two patients with pericardial hydatidosis were referred to the tertiary cardiac surgery center for operative management of their disease, and one patient with pancreatic hydatid disease was referred to a tertiary hospital having a specialized hepatopancreaticobiliary surgery unit. Six patients underwent operations by the general surgeons in our hospital.
Two male patients, who were 32 and 38 years old, presented with thoracic pain and dyspnea. Chest radiographs and a thoracic CT scan revealed cystic disease in the right mediastinum (Fig. 1A) and left pleural space (Fig. 1B), respectively. Both patients were treated successfully by extirpation of the cysts with decortication.
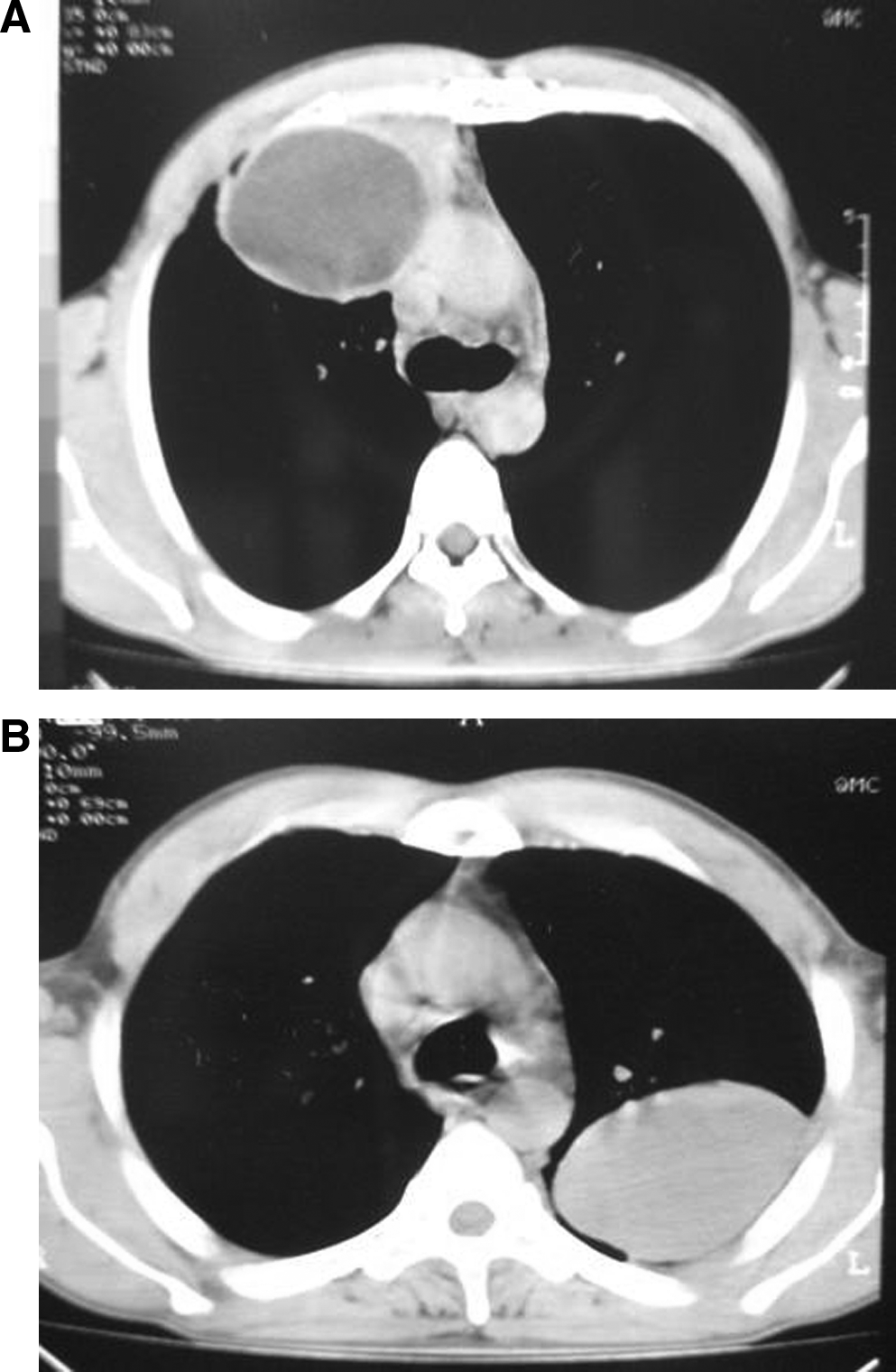
Hydatid cysts in the chest. (
A subcutaneous cyst had previously been diagnosed in the right infrascapular region in a 35-year-old woman. The patient presented with pain and swelling over the right dorsal side of her torso. Ultrasonography and a CT scan (Fig. 2) revealed a cystic mass before the diagnosis was confirmed by the immune hemagglutination test. This mass was removed surgically.
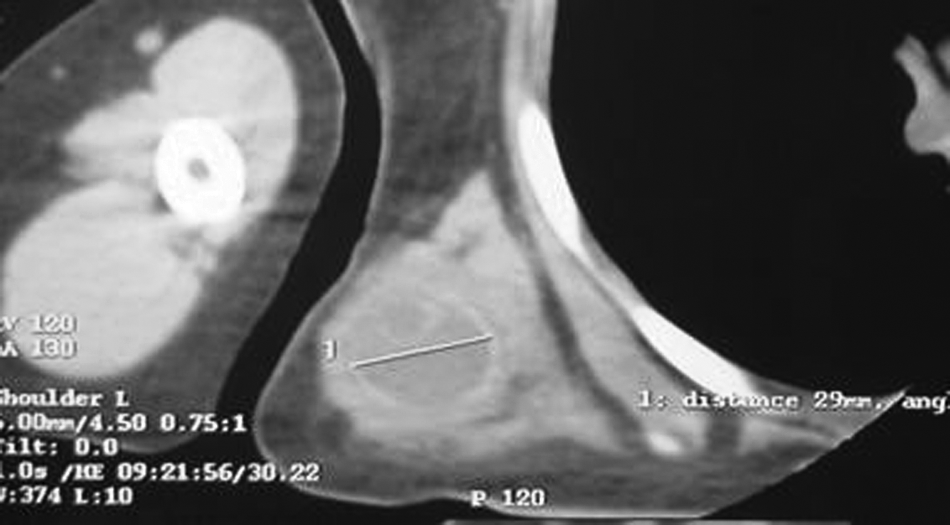
Hydatid cyst in right infrascapular region.
Another female patient who likewise was 35 years old complained of a painful neck swelling, which was located within the thyroid gland. An ultrasound examination revealed a swelling with a cystic nodular formation, and a hypoechoic halo was found in the right lobe of the thyroid gland. The nature of the disease was confirmed by a combination of CT (Fig. 3), which revealed a hypodense mass, and serology. This patient was treated with a right lobectomy and isthmectomy of the thyroid.

Hydatid cyst in right lobe of thyroid.
Splenic hydatid disease was diagnosed in a 72-year old woman who complained of abdominal discomfort. The diagnosis was made with a combination of ultrasonography, CT scan, and serology. A laparotomy was performed through a midline incision in order to explore the whole abdominal cavity, and a splenectomy was performed to remove all of the hydatid disease with vaccination before surgery.
One patient, who was 22 years old, was admitted to the emergency department with symptoms of an acute abdomen. He also had pelvic pain with guarding and rebound tenderness. Ultrasonography and CT revealed a cyst in the rectovesical space. The immune hemagglutination test was not performed in this patient, as an emergency laparotomy was necessary, and the cyst was removed intact.
A 62-year old man complained of abdominal pain, and ultrasonography and CT scanning revealed a hypodense cystic mass between the spleen and the left kidney. The immune hemagglutination test was positive. Unfortunately, this patient died of cardiac and renal failure on the second day after diagnosis.
Postoperative complications were seen in two patients. One patient developed unilateral atelectasis, and the other had a surgical site infection. Both of these complications were treated conservatively with antibiotics and mucolytics (Table 2). The mean LOS of the patients undergoing surgery at our center was 4.8 days (range 2–7 days).
NA = not available.
Discussion
Hydatid disease is an infection caused predominantly by E. granulosus and has been well known since the time of Hippocrates [1, 2,13]. House pets are the primary host for the organism, with cows, sheep, horses, and sometimes human beings being intermediate hosts [3,7]. The hydatid organism spreads to humans via other intermediate hosts either directly or through ingestion of water and vegetables that have been contaminated with infected fecal material. Infection occurs mainly during childhood, but is asymptomatic until adulthood [5,6].
Infection with E. granulosus usually is asymptomatic until the size of the cysts increases sufficiently to have an effect. Between 38% and 60% of infected patients are asymptomatic [6,14]. Hydatid disease usually is found in the liver (75%), lungs (5.8–15%), spleen, kidneys, and other intra-abdominal and retroperitoneal organs, but cysts can be present in any part of the body [1,15,16]. The disease generally is diagnosed incidentally by radiologic examinations in patients without relevant clinical symptoms, and patients usually are middle aged at diagnosis [1,5]. Hydatid disease is rarely seen within soft tissues, and this condition causes difficulties for accurate and timely diagnosis [1, 16]. When the disease is diagnosed, the patient must be evaluated systemically [5, 7].
Hydatid disease has no specific symptoms or signs and varies according to the location of the cysts and the organ involved [1,6,14]. When cysts are found in the liver, a hepatic mass, biliary obstruction, and abdominal pain are most often seen. Pulmonary disease can present as dyspnea, chest pain, cough, and hemoptysis. If the cyst ruptures, it can result in fever, urticaria, eosinophilia, or anaphylactic shock [6].
The indirect hemagglutination test is positive in approximately 85% of patients. The Casoni test is positive in >90% of patients but can yield false-positive results after surgery or cyst degeneration [1]. The sensitivity and specificity of all the serologic tests are low, but these tests remain useful in screening for the disease [1,7].
The basis of the management of hydatid disease is surgery [6,7,16]. There are three layers within the cyst, and scolices are produced from the membrane of the germinative layer. The gold standard of surgery is the removal of the germinative membrane of the cyst and closure or reduction in the size of the pericystic cavity [10,13]. The surgeon must be careful to prevent seeding of the surrounding organ and tissues by scolices during removal of the germinative membrane [6,7].
For scolex inactivation, various agents such as hypertonic saline, hydrogen peroxide, polyvinyl iodine, and silver nitrate are used preoperatively [14]. To use these agents, the cystic cavity must first be aspirated and left for 15 min before the scolecidal agent is injected [14]. In our study, 20% hypertonic saline was used as a scolecidal agent.
The operations performed in this series are described in Table 2. To decrease the recurrence rate and prevention of contamination, chemotherapeutic agents were used during both the preoperative and the postoperative period [7,13,14,17]. In our cases, albendazole 800 mg/day was given preoperatively and postoperatively. Also, it has been reported that medical therapy can be used in cases that are inoperable or in patients who cannot withstand the insult of surgery [7,18].
In conclusion, we emphasize that hydatid disease can occur in any organ or tissue and should be considered in the diagnosis of a cystic space-occupying lesion in patients from countries where hydatid disease is endemic [19]. The optimal treatment is a total cystectomy regardless of the location of the disease. When this is impossible because of the location of the cyst or other factors, a partial cystectomy, irrigation with scolecidal agents, and tube drainage of the cyst may be carried out as necessary suboptimal treatments.
Footnotes
Author Disclosure Statement
None of the authors has any financial conflict of interest.