
Abstract
Abstract
Background:
Patients receive prophylactic antibiotics against surgical site infections (SSIs) before or during many procedures. Glycopeptide antibiotics are effective against most strains of methicillin-resistant Staphylococcus aureus (MRSA), but their wider use risks increasing resistance. Our objective was to review the evidence for clinical effectiveness that might help to determine whether there is a threshold of MRSA prevalence at which switching from non-glycopeptide to glycopeptide antibiotic prophylaxis might be justified.
Methods:
We performed a systematic review of randomized trials comparing a glycopeptide with an alternative antibiotic regimen for SSI prophylaxis in adults undergoing clean or clean-contaminated surgical procedures. The evidence was used to inform development of a decision-analytic model. We subsequently updated the review to May 2008.
Results:
Fourteen studies were identified that provided evidence concerning clinical effectiveness. The studies were too heterogeneous clinically for meta-analysis. Only one of 12 trials found that glycopeptides reduced SSIs significantly at 30 days compared with non-glycopeptide antibiotics. Of the two trials that reported on MRSA infection, neither found a significant difference between glycopeptide and comparator drugs.
Conclusions:
This systematic review did not find any evidence to support the use of glycopeptides in preference to other antibiotics for the prevention of MRSA infections and SSIs. The limitations of the evidence make it difficult to identify a threshold at which a switch from non-glycopeptide to glycopeptide prophylaxis should be recommended. Given the difficulties of addressing this issue through randomized trials, further research should focus on hospital infection control policies, MRSA screening, and the isolation and treatment of anyone infected with MRSA prior to surgery.
Prophylactic administration of antibiotics can reduce postoperative infection risk by inhibiting bacterial growth and adherence to prosthetic implants. The use of antibiotic prophylaxis before, during, or immediately after surgery is recommended for various procedures [2]. Cephalosporins currently are the antibiotics used most widely for surgical prophylaxis in the U.K., particularly in vascular and orthopedic procedures, where infections can lead to the failure of prosthetic grafts or implants.
The glycopeptide antibiotics vancomycin and teicoplanin are active against gram-positive bacteria, including MRSA and methicillin-resistant S. epidermidis (MRSE). Vancomycin and teicoplanin usually are reserved for treating MRSA infections because of concerns about increasing drug resistance. A survey of U.K. hospitals in 2004 found that 88% of MRSA isolates were resistant to three or more classes of antibiotics, but more than 99% of strains were fully susceptible to vancomycin and teicoplanin [3]. However, vancomycin resistance has been detected in enterococci and S. aureus [4, 5], and MRSA strains with reduced teicoplanin susceptibility have been identified in the U.K. [6] and France [7].
Current guidance on antibiotic prophylaxis in surgery from the Scottish Intercollegiate Guidelines Network (SIGN) recommends against glycopeptide use for prophylaxis because of fear that overuse will increase the prevalence of vancomycin-resistant Enterococcus (VRE) [2]. Recent guidelines from the British Society of Antimicrobial Chemotherapy recommend that glycopeptide prophylaxis be given only to patients with a history of MRSA colonization or infection without documented eradication, admission from a facility with a high prevalence of the organism, or a likelihood that the patient's MRSA carriage recurred after eradication [3].
In 2005, we were commissioned by the U.K. National Health Service Health Technology Assessment (HTA) Programme to investigate whether there is a threshold MRSA prevalence at which switching from non-glycopeptide to glycopeptide prophylaxis is indicated in surgical environments with a high risk of MRSA. To address this question, we undertook a systematic review of the clinical value, cost-effectiveness, and adverse effects of glycopeptide prophylaxis. This evidence was used to develop a decision analytic model to inform decisions about when to use glycopeptide prophylaxis. Further details are available in the HTA report [8] and in a recently published paper [9]. Following publication of the report, we updated the systematic review of clinical effectiveness to determine whether any new evidence is available.
Materials and Methods
The systematic review was undertaken following the guidelines produced by the Centre for Reviews and Dissemination [10]. To identify relevant studies for the initial systematic review, we searched MEDLINE, EMBASE, CINAHL, CENTRAL, Science Citation Index, and BIOSIS from 1990 to September 2005. The year 1990 was chosen as a cut-off date after discussion with clinical experts because MRSA was unlikely to be reported in trials published earlier. The following sources also were searched for ongoing trials and unpublished research: ISI Proceedings; Science & Technology Edition; Inside Conferences; National Research Register; metaRegister of Controlled Trials; and the National Technical Information Service. Reference lists were searched, and no language restrictions were applied. Details of the MEDLINE search strategy, which was adapted for other databases, are available in the full report [8].
Searches to update the review were performed in May 2008 in MEDLINE, EMBASE, and CINAHL only. Search filters for randomized controlled trials (RCTs) were used to restrict the number of records retrieved and increase the specificity of the search.
Inclusion criteria
Participants
Studies involving adult patients undergoing clean or clean-contaminated surgical procedures were eligible for inclusion. Studies of contaminated procedures, infectious surgical indications (appendicitis, cholecystitis, diverticulitis, salpingitis), or further surgery resulting from an SSI were excluded.
Intervention and comparators
Randomized or quasi-randomized controlled clinical trials (CCTs) of preoperative or intra-operative administration of any glycopeptide antibiotic by any route, compared with an alternative antibiotic regimen, were eligible for inclusion. Studies restricted to postoperative administration were excluded.
Outcomes
Surgical site infections, infections caused by MRSA or other methicillin-resistant organisms, and deaths resulting from an infection were the primary outcomes. Surgical site infections were defined using the original study classifications. The primary time period was infection within 30 days of surgery. Other outcomes, including adverse events, were assessed; full details are available elsewhere [8].
Data extraction and analysis
Two reviewers independently screened the abstracts retrieved by the literature searches and study selection. Disagreements were resolved by discussion, with referral to a third reviewer if necessary. Data extraction was performed by one reviewer and checked by a second. Relative risks (RRs) and 95% confidence intervals (95% CIs) were calculated for dichotomous outcomes on an intention-to-treat (ITT) basis where possible, using Review Manager 4.2 (Cochrane Collaboration, Oxford, United Kingdom). Because of differences in surgical procedures, antibiotic regimens, and doses and timing of prophylaxis in the various studies, no meta-analysis was undertaken. Results are presented in a narrative synthesis grouped by outcome and surgical specialty.
Quality assessment
Controlled clinical trials were assessed for methodological quality according to the following study characteristics: Randomization, allocation concealment, similarity of treatment groups at baseline, specification of eligibility criteria, blinding (of outcome assessors and patients), ITT analysis, sample size calculation, and reporting of withdrawals. Quality assessment was performed by one reviewer and checked by a second.
Results
Search results
Sixteen studies were included in the original review of clinical effectiveness; an additional three studies were included for adverse event outcomes only and are not discussed further in this paper. Three other studies included in the original review compared different glycopeptide drugs or regimens [11–13]; these studies likewise are not discussed in this paper, which focuses on comparing glycopeptide and non-glycopeptide regimens for the primary outcomes of SSI and SSI-related death. Further details of all these studies can be found in the HTA report [8]. Following the update searches in May 2008, a further 1,674 references were screened, of which two were retrieved for further evaluation. One of these was excluded because no glycopeptide regimen was included [14], and one met the inclusion criteria for the review [15], giving a total of 14 included studies (Fig. 1). Details are presented in Table 1.

Flow chart of studies through review process. Figures in brackets refer to 2008 update searches. CCT = controlled clinical trial.
Quality criteria: 1 = randomization; 2 = allocation concealment; 3 = baseline comparability; 4 = eligibility criteria; 5 = outcome assessor blinding; 6 = patient blinding; 7 = ITT analysis; 8 = sample size calculation; 9 = withdrawals reported.
CABG = coronary artery bypass graft; VR = valve repair.
All studies were described as RCTs, although they differed in quality. Only six reported using suitable methods of randomization; and of these, only one trial, in cardiac surgery [16], provided details of adequate allocation concealment. Most trials had clearly specified patient eligibility criteria, treatment groups that were comparable at baseline, and reports of how many patients withdrew. Only one-half of the trials reported that the outcome assessors were blind to treatment. Details of sample size calculations were particularly poorly reported, with only four trials reporting an a priori sample size calculation. It is therefore unclear whether the trials were powered to detect differences in SSI rates, and especially MRSA infection rates, which are likely to be low. Details of the quality criteria satisfied by each trial are presented in Table 1.
Prevention of SSI
The number of SSIs within 30 days of surgery was reported for 12 trials (Fig. 2). For the newly included study by Dhadwal et al., data on infections at 30 days were collected by the institutional infection control team rather than as part of the trial [15]. Reported infection rates at 30 days were 4.2% (4/95) in the glycopeptide group and 11.3% (12/106) in the comparator group (p = 0.06). Only one trial [17] reported a statistically significant benefit of glycopeptide prophylaxis, with infection rates of 3.7% for vancomycin and 12.8% for cefazolin or cefamandole in patients undergoing cardiac or vascular procedures (RR 0.29; 95% CI 0.11, 0.81). No statistically significant benefits of glycopeptide prophylaxis for SSI prevention were found in the other trials.
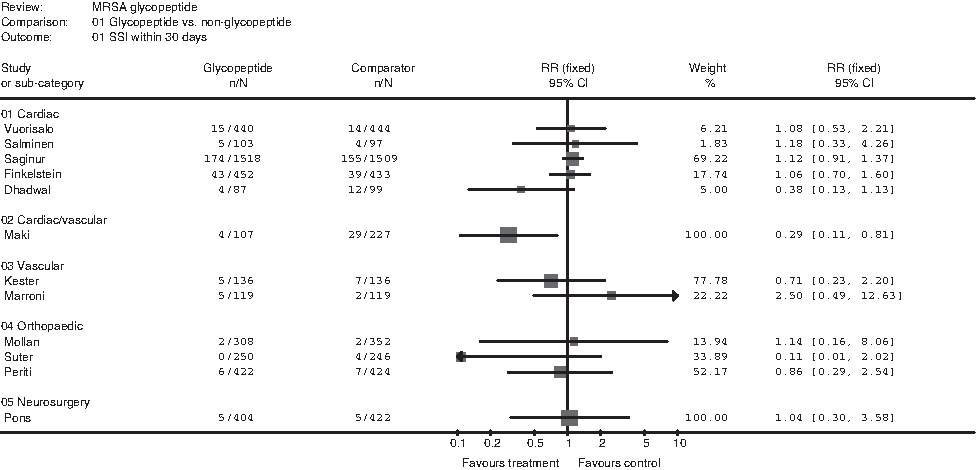
Summary of results for surgical site infections within 30 days.
The primary endpoint of the study by Dhadwal et al. was SSI within 90 days of surgery. According to the ITT analysis, infection rates were 8.4% (8/95) in the glycopeptide-treated group and 23.6% (25/106) in the comparator group [15] (p = 0.004). The per-protocol analysis gave a similar result.
Although details of the causative organisms were reported in most trials, few reported testing for MRSA. Two trials, one in cardiac surgery [18] and one in vascular surgery [19], provided results for infections caused by MRSA, but neither found a statistically significant difference between glycopeptide and non-glycopeptide prophylaxis (Fig. 3). The trial in cardiac procedures was conducted in a unit with a high prevalence of MRSA (incidence of new cases or colonization of 3% and 2.6% in the two years prior to the trial), and 0.4% of vancomycin and 1.6% of cefazolin patients developed a MRSA infection (RR 0.27; 95% CI 0.06, 1.31). The vascular trial reported no cases of MRSA in the vancomycin group and 3.8% in the cefamandole group.

Summary of results for surgical site infections caused by methicillin-resistant bacteria.
Results for infections caused by any methicillin-resistant bacteria, including MRSE and CNS, are presented in Figure 3. One patient undergoing vascular surgery who received cefamandole had a prosthetic graft infection caused by MRSE, but no MRSE infections occurred in the vancomycin group [17]. Of the three studies that reported testing for resistance to glycopeptides, two reported that no teicoplanin resistance was detected [16, 17], whereas one found no vancomycin resistance in gram-positive organisms isolated from sternal incision sites [15].
Death resulting from an infection
Five trials reported deaths caused by or related to an infection (Fig. 4). No statistically significant differences between glycopeptide and non-glycopeptide prophylaxis were observed. Infection-related deaths generally were few (less than 1.5% of patients). In one vascular surgery trial, one teicoplanin-treated patient died from a prosthesis-related infection and one cefazolin-treated patient from a blood stream infection [20]. In one cardiac trial, 0.9% of teicoplanin- and 0.8% of cefazolin-treated patients still had infections at the time of death [16]. In another cardiac trial, one cefuroxime-treated patient died from mediastinitis caused by MR-CNS.
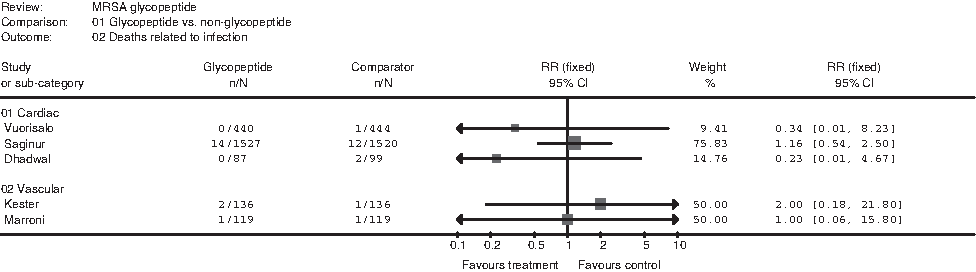
Summary of results for death related to infection.
Discussion
Principal findings
This review did not find any evidence to support the use of glycopeptides in preference to other antibiotics as prophylaxis for the prevention of MRSA infections and SSIs in patients undergoing surgical procedures. Only two trials reported MRSA infection rates [18, 19], and one of these was the only trial designed to evaluate MRSA and the only trial to report both MRSA prevalence and MRSA as an outcome [18]. The 2008 update found a large number of new studies for possible inclusion in the review, but only one new trial met the inclusion criteria, and this did not report on MRSA infection [15].
The results of the review were used to inform a decision-analytic model. However, on the basis of such limited evidence, it would be difficult to define a threshold prevalence of MRSA that would justify changing the antibiotic prophylaxis policy in a particular hospital. In the light of the lack of evidence and the risk of increasing the development of glycopeptide-resistant organisms, decisions should be based on an individual patient's risk of infection. As reported elsewhere [9], it is difficult to model the cost-effectiveness of different antibiotic regimens for prophylaxis of MRSA infection, although an indicative model has been developed that provides a framework for further evaluation [8].
Strengths and weaknesses of the review
Standard and robust systematic review methods were used to identify and screen potentially relevant studies using explicit inclusion and exclusion criteria. Our search was thorough and covered a wide range of bibliographic databases and other Internet sources. We searched for both published and ongoing or unpublished trials. An update search was performed in May 2008 to incorporate any recent evidence. We also used recognized methods to reduce the risk of bias and errors in study selection (independent decision-making) and data extraction (checking of all data). Some of the included studies were published in abstract form only, which increases the comprehensiveness of the review but has limitations in terms of results and quality assessment.
The limitations of the review reflect the limitations of the available evidence. Many studies were poorly reported or had methodological weaknesses. The only trial that reported MRSA prevalence and was designed to address MRSA prevention did not use an appropriate method of randomization, which meant that clinicians could have advance knowledge of treatment allocations. Only five trials reported a sample size calculation, and most trials were likely to have been too small to detect differences in MRSA rates. Follow-up beyond 12 mos was reported only rarely, which affects conclusions for orthopedic surgery, where deep infections that occur some time postoperatively and can result in revision surgery are a major concern. In addition, the studies in this review were of clean surgical procedures only, and there was little information on whether the infections were superficial, deep incisional, or organ space. There was no evidence relating to MRSA prophylaxis for clean-contaminated surgery.
A potentially relevant study by Tacconelli et al. [21] was published after the completion of our update search. This quasi-randomized trial (treatment allocated by patient's last name) compared vancomycin and cefazolin for prophylaxis in patients undergoing surgery for cerebrospinal shunt placement. The prevalence of MRSA in the hospital was reported to be high (one new case per 100 admissions in 2001). The primary outcome of shunt infection was significantly lower in the vancomycin group (RR 0.27; 95% CI 0.04, 0.44). The omission of this trial is a limitation of our review, but its inclusion would be unlikely to alter the conclusion that there is a lack of high-quality evidence to guide decisions about antibiotic prophylaxis policy.
Relation to other studies
We are aware of one earlier systematic review that investigated the effectiveness of switching from non-glycopeptide to glycopeptide antibiotics for prophylaxis; this was published by Bolon et al. [22]. However, this review concentrated on cardiac surgery, whereas our review covered all specialties. All the studies included in the review by Bolon et al. were included in our review with the exception of two published before our earliest inclusion date of 1990. Despite including all surgical specialties, our review found only ten additional trials, many of which were small, of poor quality, or both. Our findings agree with the conclusion of Bolon et al. that there is no evidence that glycopeptides are more effective than beta-lactams for prophylaxis of SSIs.
Our update searches identified a study by Muralidhar et al. that did not meet the inclusion criteria for the systematic review but which did attempt to establish a threshold for switching from non-glycopeptide to glycopeptide prophylaxis [23]. Muralidhar et al. used data from an audit of patients admitted to a vascular surgery unit to establish the prevalence of MRSA carriage at admission in both elective and emergency/transfer patients. They then used a simple decision analysis model to calculate the number of MRSA SSIs expected at a given prevalence of MRSA in the two groups after surgery. The costs and effectiveness of three prophylactic regimens (cefuroxime + vancomycin, cefuroxime + gentamicin, and vancomycin + gentamicin) for the prevention of SSIs caused by MRSA were examined. The authors concluded that gentamicin should be used when the prevalence of MRSA reaches 10% and vancomycin when the prevalence reaches 50% [23].
In terms of clinical effectiveness, this study is particularly important for including gentamicin, an antibiotic not compared with a glycopeptide in any of the trials included in our review. The study also suggests that the use of center-specific data combined with a relatively simple decision model may be a good alternative to attempting to model cost-effectiveness on the basis of global estimates of effectiveness derived from a systematic review. Given the shortage of trial evidence and the complexity of the issues surrounding antibiotic prophylaxis for surgery, any model or algorithm used to guide practice would need to be updated constantly and to be valid in the conditions of the specific unit where it was being applied. Further work is needed to validate the assumptions of the model developed by Muralidhar et al., and, as noted by the authors, there is scope to refine the model. However, the existing model has been useful for guiding antibiotic prophylaxis policy in the authors' hospital [23].
Implications for clinicians and policy makers
Glycopeptides are not recommended for prophylaxis because of concern about the emergence of new resistant strains, but they are used to treat MRSA infections. On the basis of this review, there is no evidence to justify a change in overall policy. This conclusion is based on the lack of clear evidence for the superior effectiveness of glycopeptides over other antibiotics and an unquantifiable but definite risk of more resistance if glycopeptides use increases.
Although this was not the focus of our review, the uncertainty surrounding antibiotic prophylaxis suggests that policies for protection of surgical patients against infection should focus on fundamental issues such as screening and eradication of MRSA on admission and maintenance of good hygiene practices throughout the hospital.
Healthcare-associated infections, including SSIs, are of great concern to the public, media, and policy makers, as well as to healthcare workers. This may lead to pressure to be seen to be addressing the issue, whether by new policy initiatives (for example, “deep cleaning”) or by commissioning research. Commissioners of research involving evidence synthesis and economic modeling should be certain that the question of interest can be answered by the methods proposed. If this is unclear, scoping work or other preliminary research may be useful to ensure that the proposed research actually will add to the evidence base for decision making.
Unanswered questions and further research
Our clinical effectiveness review does not answer the question whether a threshold exists for switching from non-glycopeptide to glycopeptide prophylaxis in relation to the risk of MRSA infection. None of the included trials was designed to address this question, and only one provided details of MRSA prevalence and the effectiveness of vancomycin prophylaxis.
As there is a lack of evidence on the clinical value and cost-effectiveness of glycopeptide prophylaxis for MRSA and other infections caused by methicillin-resistant organisms, a large multi-center RCT could provide results across surgical centers with various MRSA prevalences. However, such a trial may be difficult to conduct in the light of current guidance recommending against glycopeptide prophylaxis in general. In addition, by the time the trial was completed, the results could be superseded by new treatments for MRSA currently in development, such as daptomycin.
Given the complexities of decision making relating to infection control and particularly the prevention of MRSA, it is unclear how generalizable the findings of any trial would be because so much depends on the situation in the individual hospital. Further research should address the complete picture, including hospital infection control policies, MRSA screening, and the isolation and treatment of anyone infected with MRSA prior to surgery. Screening and eradication of MRSA colonization or infection for an individual patient should remain the primary concern, rather than basing decisions about glycopeptide prophylaxis on the background MRSA rate at a particular hospital, which will change over time.
Footnotes
Acknowledgments
We are grateful to Peter Campbell (Consultant Orthopedic Surgeon), Professor Peter Gilbert (Clinical Microbiologist), Doctor Ian Gould (Consultant Microbiologist), Peter Kay (Consultant Orthopedic Surgeon), Steve Leveson (General Surgeon), and Jonathan Michaels (Professor of Vascular Surgery) for clinical advice; Eimear NicLochlainn, John Edmunds, Jenny Roberts, and Richard Smith, who advised on modelling methods; and our colleagues at the University of York, Professor Martin Bland, Professor Eve Roman, and Professor David Torgerson, for providing advice on potential study designs for future research.
This research was commissioned and funded by the HTA Programme as project number 05/36/01. The views expressed in this paper are those of the authors and not necessarily those of the NHS, NIHR, or the Department of Health. The funding body did not have a decision-making role in this research. None of the authors has declared any conflict of interest.
Author Disclosure Statement
No conflicting financial interests exist.