
Abstract
Abstract
Background:
Resistance to broad-spectrum antibiotics by gram-negative organisms is increasing. Resistance demands more resource utilization and is associated with patient morbidity and death. We describe the implementation of infection reduction protocols, including antibiotic stewardship, and assess their impact on multi-drug-resistant (MDR) healthcare-acquired gram-negative infections.
Methods:
Combined infection reduction and antibiotic stewardship protocols were implemented in the surgical and trauma intensive care units at Vanderbilt University Hospital beginning in 2002. The components of the program were: (1) Protocol-specific empiric and therapeutic antibiotics for healthcare-acquired infections; (2) surgical antibiotic prophylaxis protocols; and (3) quarterly rotation/limitation of dual antibiotic classes. Continuous healthcare-acquired infection surveillance was conducted by independent practitioners using National Heath Safety Network criteria. Linear regression analysis was used to estimate trends in MDR gram-negative healthcare-acquired infections.
Results:
A total of 1,794 gram-negative pathogens were isolated from healthcare-acquired infections during the eight-year observation period. The proportion of healthcare-acquired infections caused by MDR gram-negative pathogens decreased from 37.4% (2001) to 8.5% (2008), whereas the proportion of healthcare-acquired infections caused by pan-sensitive pathogens increased from 34.1% to 53.2%. The rate of total healthcare-associated infections per 1,000 patient-days that were caused by MDR gram-negative pathogens declined by −0.78 per year (95% confidence interval [CI] −1.28, −0.27). The observed rate of healthcare-acquired infections per 1,000 patient days attributable to specific MDR gram-negative pathogens decreased over time: Pseudomonas −0.14 per year (95% CI −0.20, −0.08), Acinetobacter−0.49 per year (95% CI −0.77, −0.22), and Enterobacteriaceae −0.14 per year (95% CI −0.26, −0.03).
Conclusion:
Implementation of an antibiotic stewardship protocol as a component of an infection reduction campaign was associated with a decrease in resistant gram-negative healthcare-acquired infections in intensive care units. These results further support widespread implementation of such initiatives.
Recognizing that practice habits related to antibiotic use may contribute to pathogen resistance and subsequent infections [7, 12, 14], clinicians at Vanderbilt University Hospital (VUH) implemented an infection reduction program. As a component of the overall campaign, a multidisciplinary trauma/surgical critical care service introduced several evidence-based practice guidelines/protocols beginning in April 2002 that were intended to systematize antibiotic utilization in a surgical intensive care unit (SICU) and trauma intensive care unit (TICU). The objective of this observational study was to examine the effect of the antibiotic stewardship program on the incidence of resistant gram-negative HAIs. The authors hypothesized that the incidence of multi-drug-resistant (MDR) gram-negative HAIs would decrease in association with the implementation of a stewardship program.
Patients and Methods
This study represents a retrospective analysis of prospectively collected infection control data. The study was conducted at VUH, an 800+-bed academic medical center in Nashville, Tennessee, from January 2001 to December 2008. The 21-bed SICU provides comprehensive critical care management for a multiplicity of high-risk surgical patients. The 31-bed trauma unit is an integrated, acute and subacute unit with 14 beds designated as intensive care unit (ICU) beds. All patients admitted to VUH's SICU or TICU during the study period who contracted an HAI with microbiological confirmation of at least one gram-negative pathogen were evaluated in this study.
In April 2002, the multidisciplinary Trauma/Surgical Critical Care service began to create a series of evidence-based protocols/guidelines that directed clinical practices related to the prevention, diagnosis, and treatment of HAIs. Several initiatives designed to reduce healthcare-acquired infections (Table 1) were added to the established management guidelines related to glucose control, sedation management, ventilator weaning, and blood transfusions. As illustrated in Table 2, several components of the guidelines/protocols directed protocol-driven antibiotics for specified indications, including empiric antibiotics for confirmed or suspected infection processes, as well as prophylaxis for commonly performed surgical procedures. To ensure compliance with and consistency of application of protocols, electronic order sets for protocol-based diagnostic laboratory data, radiographic data, and empiric antibiotics were incorporated into VUH's locally developed electronic care provider order entry (CPOE) system. In 2004, clinical pharmacists were recruited to assist with creation of antibiotic protocols, to ensure compliance with and appropriate dosing of prescribed protocol antibiotics, and to participate in daily patient care rounds. In collaboration with VUH's informatics department, an infection control database was created for the prospective capture of infection-related data specific to the SICU and TICU. The HAI surveillance was conducted by independent infection control practitioners in accordance with the U.S. Centers for Disease Control and Prevention (CDC) definitions for HAIs [15, 16]. The database included information on pathogen identification, site of infection, and specific antimicrobial susceptibility for each HAI. Additional pertinent data such as the hospital day of infection diagnosis, antibiotic utilization, and susceptibility to antibiotics not included in the infection control system were extracted manually from electronic patient charts and administrative hospital records.
Dates represent when procedure was instituted.
Prophylactic antibiotic protocol
In April 2002, guidelines for prophylactic antibiotics were devised for select procedures in the SICU and TICU. On the basis of data from previous experiences in the TICU, prophylaxis for intracranial pressure monitors was converted from broad-spectrum antibiotics (ceftriaxone and ciprofloxacin) to narrow-spectrum antibiotics (cefazolin or vancomycin [if penicillin allergic]) [17]. In the setting of traumatic injuries, 24 h of narrow-spectrum prophylactic antibiotics were instituted with specified drug choices for particular injury types (Table 2) [14, 18]. At VUH, an institution-wide initiative for surgical prophylaxis based on the Surgical Care Improvement Project (SCIP) was implemented in 2005 [19]. Performance measures as directed by SCIP were followed in the SICU and TICU during the observation period.
Therapeutic antibiotic use protocol
In April 2002, the therapeutic antibiotic use protocol was introduced. The goals included the orchestration of rapid administration of broad-spectrum empiric therapy targeted at likely pathogens in the setting of suspected infections. This process involved assuring that appropriate protocol-driven antibiotics were ordered via CPOE order sets, dispensed immediately from the pharmacy or automated cabinets, and administered within 30 min after appropriate culture specimens (quantitative cultures acquired sterilely) were obtained from the suspected sites of infection. Empiric antibiotic selection and therapeutic use included specific emphasis on the avoidance of third-generation cephalosporins and fluoroquinolones for extended courses and the avoidance of clindamycin except for suspected toxin-mediated infections or for perioperative surgical prophylaxis of penicillin-allergic patients. The protocol was categorized by indication. Specifically, regimens were prescribed for pneumonia (early, presumed community-acquired vs. late, presumed healthcare-acquired) and non-pneumonia sites (blood stream, urinary, intra-abdominal, surgical site). Beginning in February 2003, the routine use of bronchoscopy was initiated in the setting of suspected pneumonia to obtain quantitative specimen samples from the lower respiratory tract for the identification of pathogens from microbiological cultures and guidance of appropriate antibiotic therapy [20–22]. When culture and susceptibility data became available, antibiotic therapy was de-escalated to the most active narrow-spectrum single agent within the prescribed drug class when possible with established and defined courses of therapy [23, 24]. The specific antibiotics were selected for the protocol after assessing pathogen frequency and drug sensitivity trends using infection control data specific to each unit.
Antibiotic rotation
In January 2005, antibiotic rotation was incorporated as a component of stewardship (Tables 3 and 4). The goal of this rotation was to direct quarterly antibiotic class heterogeneity in an effort to avoid resistance-selective pressures. This included minimizing select antibiotic class exposure for a single quarter throughout a given year. Dual classes were rotated each quarter according to whether treatment was for pneumonia or a non-pulmonary site (i.e., blood stream, urinary tract, surgical site) [25].
Empiric vancomycin is used for all categories to cover resistant gram-positive pathogens.
BLIC = beta-lactam/beta-lactmase inhibitor combinations; FQ = fluoroquinolones; CARB = carbepenams; 3/4CEPH = 3rd- and 4th-generation cephalosporins.
Empiric gram-negative antibiotic for pneumonia (hospital day 1–3).
Empiric gram-negative antibiotic for pneumonia (hospital day ≥4) = imipenem + tobramycin; antibiotics for definitive therapy rotated as indicated.
Empiric vancomycin was used for pneumonia (hospital day ≥4) to cover resistant gram-positive pathogens.
Data collection
Demographic data for patients admitted to the SICU ≥18 years of age were collected from administrative hospital records and from an admission registry database (created in February 2005). Demographic data for patients ≥18 years of age who were admitted to the TICU were collected from the Trauma Registry of the American College of Surgery (TRACS) database. Rates of HAIs were collected from the infection control database and defined according to criteria set forth by the National Healthcare Safety Network/National Nosocomial Infection Surveillance (NHSN/NNIS) system for nosocomial infections [15,16]. For culture-positive HAIs, identification and antibiotic susceptibility data were collected for isolated gram-negative pathogens. The antimicrobial classes evaluated were generally regarded as broad-spectrum antibiotics used commonly to treat MDR gram-negative pathogens in institutional settings [1]. The drug classes were beta-lactam/beta-lactamase inhibitor combinations (BLIC), fluoroquinolones (FQ), carbapenems (CARB), aminoglycosides (AMG), and third- and fourth-generation cephalosporins (3/4CEPH).
Prior to the initiation of this study, approval by the Vanderbilt University Institutional Review Board was granted. All study data were maintained in a Health Insurance Portability and Accountability Act-compliant, password-protected database. All patient identifiers were eliminated from the database prior to analysis and reporting.
Outcome measures
The primary study endpoint was to determine if a reduction in MDR gram-negative HAI had occurred as a result of the implementation of infection reduction and antibiotic stewardship protocols. Pathogens were categorized as MDR if they were resistant to three or more of the five drug classes of interest. Pathogens were categorized as pan-sensitive (PS) if they were susceptible to all five classes. All routine microbiological culture and susceptibility testing was performed by the VUH microbiology laboratory using the Kirby-Bauer disk-diffusion method [26]. Alterations in antimicrobial susceptibility were assessed by the following: (1) The proportion of total gram-negative HAIs categorized as PS for each study year-quarter; (2) the proportion of total gram-negative HAIs categorized as MDR for each study year-quarter; (3) the rate of MDR infections per 1,000 patient-days for each study year-quarter; and (4) the rate of HAIs categorized as MDR consequent to Pseudomonas or Acinetobacter, species and Enterobacteriaceae per 1,000 patient-days for each study year-quarter. Broad-spectrum antibiotic use targeting gram-negative pathogens was reported as days of use of antibiotics within each class per 1,000 patient-days.
Statistical analysis
Statistical analysis of study data was performed using SPSS 16.0 (SPSS, Inc., Chicago, IL) and STATA 11 (STATA Corp., College Station, TX). Patient demographics and baseline characteristics were captured using descriptive statistics. Antibiotic sensitivity (MDR) is expressed as the proportions of total HAIs. Continuous variables (antibiotic days) are reported as mean ± standard deviation (SD) and compared using t-tests. To estimate trends and to quantify the rates of change over time in the annual percentage of MDR gram-negative pathogens, total MDR HAI rate per 1,000 patient-days, and specific MDR gram-negative pathogens per 1,000 patient-days, linear regression analysis was conducted. The strength of the association of progressed time (in years) and the observed changes in MDR HAI rates are reported as correlation coefficients. A negative binomial regression model was used to quantify the association of contributive factors to the incidence of MDR HAIs. The model incorporates patient-days in each ICU over time as the exposure variable and Trauma Injury Severity Score (TRISS) as a covariate for patients in the TICU. All p values ≤0.05 were considered statistically significant.
Results
Patient demographics
Patient demographics, baseline characteristics, and clinical outcomes are listed in Table 5. In the SICU, the mean age was 57 ± 16 years, and there was a slight predominance of males. The largest percentage of patients was admitted by the Emergency General Surgery service. The median stay was three days, and the median number of days of mechanical ventilation was three. During the observation period, 8.3% of the patients died.
Data from February 2005 to December 2008.
SD = standard deviation; ISS = Injury Severity Score; TRISS =trauma injury severity score (probability of survival); LOS = length of stay; IQR = interquartile range; ICU = intensive care unit; APACHE II = Acute Physiology and Chronic Health Evaluation.
In the TICU, the mean age was slightly younger, and males accounted for three-fourths of the patients. Blunt trauma was the most common cause of injury. The mean Injury Severity Score (ISS) was 18 ± 12, and the mean TRISS was 0.868 ± 0.243. The median ICU stay was three days, and the median days of mechanical ventilation was two. Only 7.2% of the patients died.
Antibiotic use and protocol compliance
Surgical intensive care unit
The utilization in the SICU of broad-spectrum antibiotics targeting gram-negative pathogens (BLIC, CARB, FQ, 3/4CEPH) is shown in Figure 1. After the implementation of quarterly antibiotic class rotation and limitation protocols in the first quarter of 2005, antibiotic heterogeneity was maintained, as demonstrated by quarterly fluctuations in antibiotic days per 1,000 patient-days for each drug class. Antibiotic classes targeted for “indicated” use each quarter according to protocol were used at a significantly higher rate than the classes targeted for “limited” use (mean days per 1,000 patient-days = 227.6 ± 37.9 vs. 49.3 ± 28.8; p < 0.001). Antibiotic classes targeted for limited use each quarter were the least used of the classes for nine of 16 quarters (56%). There was a significant decrease in the utilization of total broad-spectrum antibiotics (BLIC, CARB, FQ, 3/4CEPH) targeting gram-negative pathogens over the observation period (antibiotic days per 1,000 patients declined by −0.09 per quarter; p < 0.001) (Fig. 2).
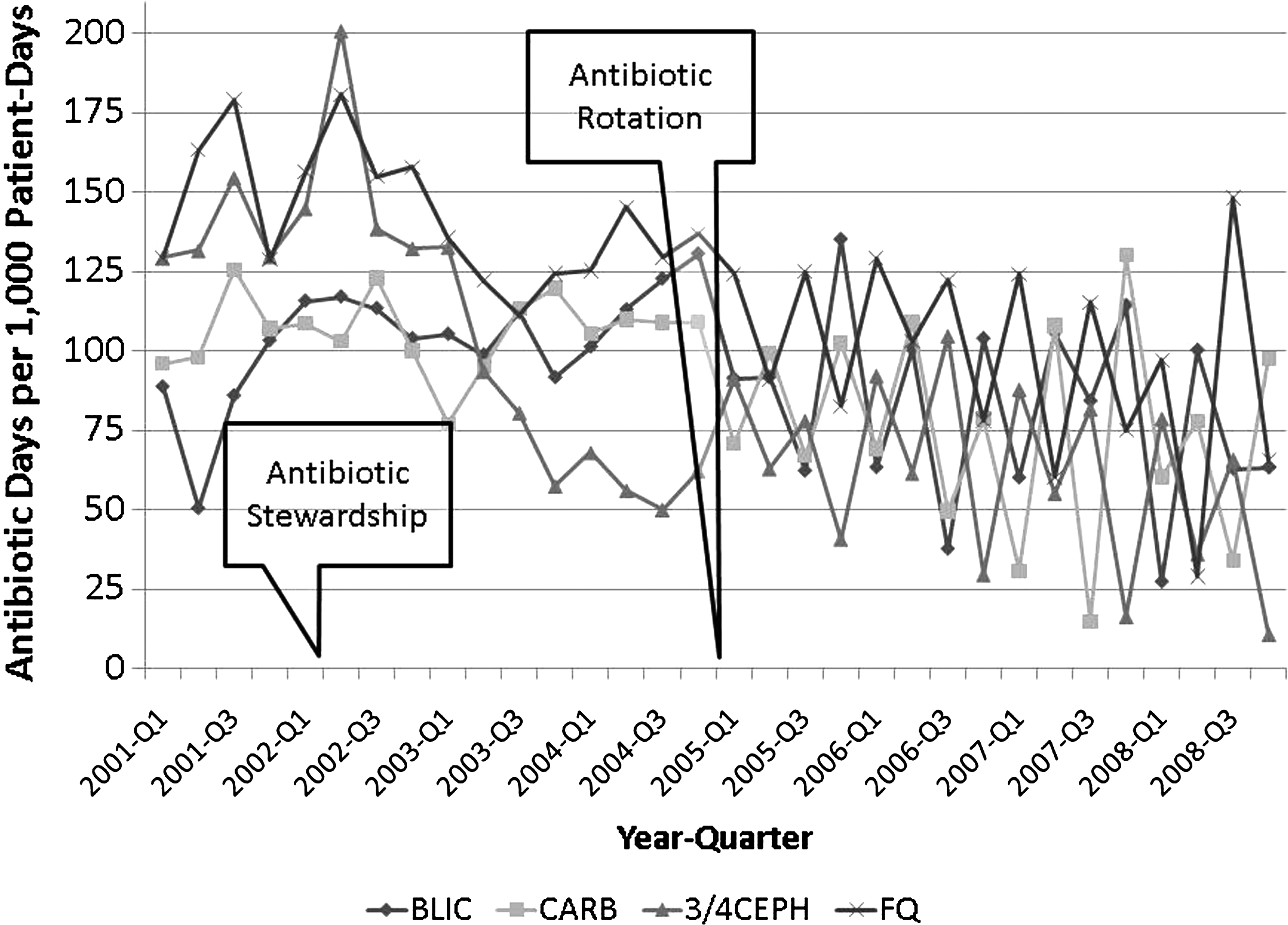
Quarterly broad-spectrum antibiotic use in surgical intensive care unit.

Combined broad-spectrum antibiotic use in surgical intensive care unit.
Trauma intensive care unit
Figure 3 demonstrates antibiotic utilization within the TICU over time. The quarterly fluctuations are not as dramatic as those observed in the SICU. In the TICU, the ability to impose quarterly antibiotic class limitation was hindered by the long-standing high incidence of resistant Acinetobacter HAIs. Historical antibiotic sensitivity data for these pathogens necessitated combined therapy with a carbapenem and aminoglycoside as primary empiric therapy to ensure adequate pathogen coverage. When culture and sensitivity data were available, the selection of protocol-prescribed antibiotics for de-escalated therapy was rotated each quarter; antibiotics were discontinued if cultures were negative. In the first quarter of 2008, the incidence of resistant Acinetobacter HAIs had declined enough to allow the institution of antibiotic class limitation and rotation. Antibiotic classes specifically targeted for “indicated” use as definitive therapy each quarter according to protocol had a significantly higher utilization rate than classes targeted for “limited” use (mean antibiotic days per 1,000 patient-days = 78.8 ± 22.0 vs. 46.9 ± 15.6; p < 0.001). Although carbapenems were used as primary empiric therapy each quarter, their overall utilization was significantly less than that of drug classes targeted specifically for use as definitive therapy (mean antibiotic days per 1,000 patient-days = 78.8 ± 22.0 vs. 37.4 ± 13.8; p < 0.001). There was also an observed significant decrease in the utilization of total broad-spectrum antibiotics (BLIC, CARB, FQ, 3/4CEPH) targeting gram-negative pathogens over the observation period (antibiotic days per 1,000 patients −0.11 per quarter; p < 0.001)(Fig. 4).
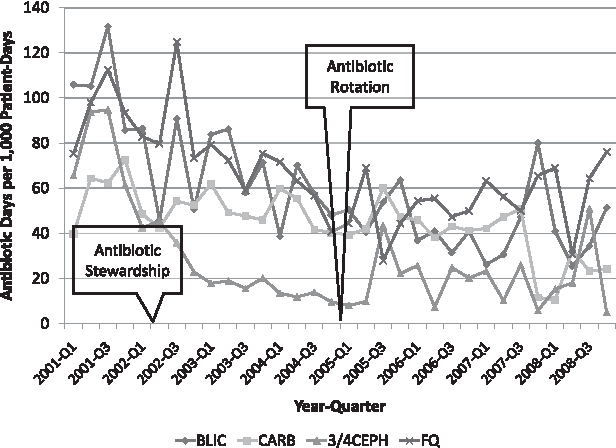
Quarterly broad-spectrum antibiotic use in trauma intensive care unit.

Combined broad-spectrum antibiotic use in trauma intensive care unit.
Infections outcomes and antibiotic resistance
Among HAIs consequent to gram-negative pathogens present in the SICU, pneumonia (n = 315; 61%) was the most common, followed by blood stream (n = 80; 16%), urinary tract (n = 68; 13%), and surgical site (n = 22; 4%) infections. A total of 513 gram-negative pathogens were isolated and identified. Enterobacteriaceae (n = 261; 51%), Pseudomonas (n = 129; 25%), Acinetobacter (n = 64; 12%), and Stenotrophomonas (n = 39; 8%) were the most common. The proportion of total HAIs attributable to pan-sensitive gram-negative pathogens increased by 0.4% per quarter over the study period (p = 0.315), whereas the proportion considered MDR decreased significantly, by −0.99% per quarter (p = 0.001) (Fig. 5). The HAI rate per 1,000 patient-days for gram-negative pathogens considered MDR declined significantly over the study period (-0.131 per quarter [CI −0.28, −0.06; p = 0.001]). During the third quarter of 2007, an increase in total MDR HAIs occurred in the SICU as a result of a hospital-wide outbreak of MDR Acinetobacter. This outbreak was consistent with national trends [27,28]. There was a significant decline in the rate of HAIs in which MDR Pseudomonas and Enterobacteriaceae were isolated (Pseudomonas −0.04 per quarter [CI −0.07, −0.01; p = 0.007; Enterobacteriaceae −0.05 per quarter [CI −0.10, −0.008, p = 0.023]). There also was a downward trend in the rate of MDR Acinetobacter HAIs, but this decline did not reach statistical significance (−0.03 per quarter [CI −0.08, 0.02; p = 0.190]).
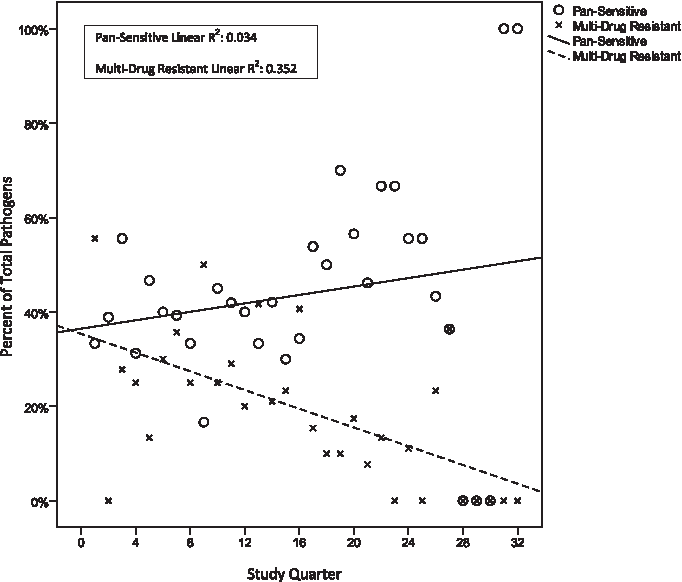
Percentage of pan-sensitive and multi-drug-resistant pathogens isolated in surgical intensive care unit.
Among HAIs consequent to gram-negative pathogens in the TICU, pneumonia (n = 812; 63%) was the most common infection followed by urinary tract (n = 186; 15%), blood stream (n = 124; 10%), and surgical site (n = 87; 7%) infections. From the HAIs, 1,280 gram-negative pathogens were isolated and identified. Enterobacteriaceae (n = 680; 53%), Acinetobacter (n = 259; 20%), Pseudomonas (n = 154; 12%), and Haemophilus influenzae (n = 125; 10%) were the most commonly isolated species. The proportion of total HAIs attributable to gram-negative pathogens considered pan-sensitive increased by 0.2% per quarter over the study period (CI −0.9, 1.3%; p = 0.677), whereas the proportion of those considered MDR decreased significantly, by −1.1% per quarter (CI −1.7, −0.4%; p = 0.003) (Fig. 6). The HAI rate for gram-negative pathogens considered MDR decreased significantly over the study period (−0.23 per quarter [CI −0.33, −0.12; p < 0.0001]). The third-quarter 2007 hospital-wide outbreak of MDR Acinetobacter also affected the TICU. Despite this occurrence, there was a significant decline in the rate of HAIs from which MDR Acinetobacter and Pseudomonas were isolated (Acinetobacter −0.17 per quarter [CI −0.24, −0.10; p < 0.0001]); Pseudomonas −0.03 per quarter [CI −0.05, −0.01; p = 0.001]). There also was a downward trend in the rate of MDR Enterobacteriaceae HAIs, but this did not reach statistical significance (−0.02 per quarter [CI −0.06, 0.03; p = 0.388]).

Percentage of pan-sensitive and multi-drug-resistant pathogens isolated in trauma intensive care unit.
Association of antibiotic rotation with reduction in antibiotic resistance
Antibiotic rotation, as a component of stewardship, appears to have a significant association with a reduction of MDR HAIs, as indicated by our negative binomial regression model (Table 6). In the SICU, the incidence rate ratio (IRR) of MDR HAIs diagnosed during the period before antibiotic rotation (2001–2004) was significantly lower than in the period after the implementation of drug rotation (2005–2008). Total HAIs caused by MDR HAIs, MDR Acinetobacter, MDR Enterobacteriaceae, and MDR Pseudomonas were reduced by 76% (IRR 0.24; p < 0.0001), 67% (IRR 0.33; p = 0.014), 90% (IRR 0.10; p = 0.001, and 72% (IRR 0.28; p = 0.012), respectively.
Negative binomial regression model: multidrug-resistant Infection rate = count variable; patient-days = exposure variable; antibiotic rotation = predictor variable; trauma injury severity score (probability of survival) = predictor variable (covariate for TICU).
IRR = incidence rate ratio; CI = confidence interval; TICU = trauma intensive care unit; SICU = surgical intensive care unit.
In the TICU, the IRR of MDR HAIs also was reduced after the implementation of antibiotic rotation. Total MDR HAIs, MDR Acinetobacter, and MDR Pseudomonas HAIs were reduced by 68% (IRR 0.32; p = 0.005), 78% (IRR 0.22; p < 0.0001), and 83% (IRR 0.17; p = 0.025), respectively. The MDR Enterobacteriaceae HAIs increased by 5%, but this was not statistically significant (IRR 1.05; p = 0.942). Higher TRISS scores as a covariate appeared to have a statistically insignificant association with the observed MDR HAI rate (IRR 1.08; p = 0.21).
Discussion
In this observational study, we describe the implementation in a TICU and SICU of several multifaceted interventions collectively constituting an infection reduction and antibiotic stewardship program. After the initiation of this program, significant reductions in the number of HAIs attributable to MDR gram-negative pathogens were observed. This is represented by a relative reduction of 77% in the proportion of isolated MDR gram-negative pathogens and 93% in the MDR HAI rate per 1,000 patient-days.
The reduction of resistant gram-negative HAIs has important implications for clinical practice in that such infections are associated with increases in patient morbidity and death [4, 6, 9–11, 29]. The global increase in the resistance of gram-negative pathogens to current antibiotic regimens complicates care and may contribute to poor outcomes in nosocomial infections caused by these pathogens. Resistance may increase the likelihood of inadequate empiric therapy, which was associated with an excess infection-related mortality rate (42.0% vs. 17.7%; p < 0.001) and all-cause mortality rate (52.1% vs. 12.2%; p < 0.001) [7] in one large study. Resistant gram-negative infections also have major economic consequences. Costs associated with infections caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae have been noted to be 1.57 to 2.9 times higher than in control patients [30]. In a cohort of critically ill surgical patients, the median hospital costs for those with resistant gram-negative infections were almost triple those for patients with drug-sensitive gram-negative infections ($80,500 vs. $29,604; p < 0.0001) [5].
The data presented here suggest that gram-negative resistance may not be inevitable if clinicians utilize antibiotics in an evidence-based fashion. Multiple studies document that antibiotic exposure is the risk factor most strongly associated with the development of resistant infections in a variety of settings [12,14,31], may increase the risk of inadequate empiric antibiotic therapy for such infections [7], and may increase the risk of development of all subsequent nosocomial infections (both resistant and non-resistant) [17,18,32–34]. Components of this antibiotic stewardship program are designed to limit antibiotic utilization to clearly established indications with the narrowest spectrum and shortest course. The literature has demonstrated efficacy while simultaneously assuring adequate empiric therapy for infections. The use of diagnostic algorithms and quantitative cultures to establish the diagnosis of pneumonia was introduced to target empiric therapeutic regimens for established infections, thus limiting empiric therapy in those patients without identified infections.
During the study period, an antibiotic rotation protocol designed on the basis of the results published by Raymond et al. [25] and Barie et al. [35] was introduced. The goal was to limit the use of a specific antibiotic class during a given quarter while maintaining antibiotic heterogeneity. The method of drug rotation incorporates the rotation of dual antibiotic classes dictated by the suspected site of infection. Using this strategy, Barie et al. observed improvements in appropriate pathogen coverage with prescribed antibiotics, and Raymond et al. saw reductions in MDR HAIs in addition to a significant reduction in the crude mortality rate. Our analysis suggests that this specific type of antibiotic rotation is significantly associated with the observed reduction in MDR HAIs, as indicated by negative binomial regression modeling, and adds support to the findings of the earlier articles. Nonetheless, the routine practice of antibiotic rotation is a subject of controversy. Numerous researchers have examined different strategies of rotating an assortment of antibiotic classes, ultimately yielding divergent results [25,36–44]. Further well-designed prospective studies of antibiotic rotation strategies are warranted to justify its role in routine clinical practice. Because of the lack of adequate randomized studies to support its use, the Infection Diseases Society of America and Healthcare Epidemiology of America currently do not recommend antibiotic rotation as a method of antimicrobial stewardship [45].
Limitations of the current study's methodology merit discussion. In order to identify causal relations of individual protocol components and decreased antibiotic resistance, a longitudinal or interrupted time series analysis would be ideal. With the exception of antibiotic rotation, other individual components of the stewardship program described in this study were implemented indiscriminately over an indefinite portion of the observation period. As a consequence, the impact of individual components of the infection reduction campaign could not be separated accurately, and adherence to all specific protocols could not be assessed. The current study did not track the number of procedures during the observation period that necessitated the use of prophylactic antibiotics; therefore, compliance with the antibiotic prophylaxis protocol cannot be assessed. Other evidence-based protocols/guidelines unrelated to the diagnosis and treatment of infections also were implemented during the study period (see Table 2). In May 2000, VUH instituted policies for isolation precautions according to the CDC recommendation for persons with suspected or confirmed infection or colonization with MDR gram-negative HAIs [46,47]. In February 2003, VUH instituted policies consistent with the CDC recommendations for hand hygiene measures aimed at preventing the spread of HAIs. Other protocols/guidelines include a nurse-driven skin breakdown risk assessment and intervention protocol, a training module on central venous catheter insertion and management for resident physicians, and conservative transfusion of blood products. Any role these non-antibiotic stewardship protocols played in the observed reduction in infections cannot be identified by the current study. The admissions registry database for the SICU was not established until February 2005; therefore, patient demographics and clinical outcomes were not available prior to this time. In addition, other covariates such as APACHE II score as an indicator of severity of illness could not be used in the negative binomial regression model for the SICU, as they were not available.
The study was devised with the primary endpoint focused specifically on observing the incidence of MDR gram-negative HAIs over time. The current study design was not powered to assess the association of reduced gram-negative resistance and its impact on other clinical outcomes. Despite significant reductions in gram-negative resistance over the eight-year observation period, the impact of the antibiotic stewardship program on patient morbidity and mortality rates is unknown.
Conclusions
In this study, reductions in antibiotic-resistant gram-negative infections were observed in a TICU and SICU after the implementation of an infection reduction and antibiotic stewardship program. Essential components of a successful program must include multiple strategized, collaborative, and multifaceted interventions. The creation and implementation of such efforts requires contributions from multiple healthcare disciplines. The findings of this study provide further justification for the widespread implementation of such initiatives.
Footnotes
Acknowledgments
The authors thank the Department of Informatics for assistance with the development and maintenance of the infection control database; the Department of Infection Control and Prevention for their diligence in infection surveillance; and members of the multidisciplinary critical care teams (nursing, pharmacy, respiratory therapy, and medical) involved in the creation, implementation, and day-to-day practice of infection reduction and antibiotic stewardship. Data from the current manuscript were presented as an oral abstract by MJD at the 29th Annual Surgical Infection Society Meeting (Hilton Head, SC, February 2008).
Financial Support
RMK is supported by National Institutes of Health training grant 5T32DK007061-35. No commercial financial support was provided for the completion of this study.
Author Disclosure Statement
MJD has served on an advisory board at Ortho-McNeil and has received a speaker honorarium from Merck. AKM was a member of The Surgery Advisory Board at Schering-Plough and has received research funding from Pfizer. TRT has received research funding from Sanofi-Pasteur.
Presented at the Twenty-Eighth Annual Meeting of the Surgical Infection Society, Hilton Head Island, South Carolina, May 7–9, 2008.