
Abstract
Abstract
Background:
Only 13 cases of pyomyoma related to pregnancy have been described since 1945. Treatment consists of hysterectomy, which exposes critically ill patients to operative risks and induces infertility.
Cases:
Three cases of pyomyoma in the postpartum period are described. Treatment using computed tomography-guided drainage was realized successfully in two cases.
Conclusion:
Therapy via drainage and lavage of pyomyoma is a viable option to preserve patient fertility. In the absence of a proper response to this treatment, total abdominal hysterectomy is the treatment of choice.
Case Reports
Case 1
A 31-year-old, black, gravida 4 para 0 woman presented at the outpatient clinic of our tertiary care center with 14 weeks of amenorrhea. Her clinical history was uncomplicated except for three first-trimester pregnancy terminations by dilatation and curettage (D&C). Physical examination showed uterine enlargement up to the umbilicus. No fetal cardiac activity was detected. A subsequent US showed a 13-week monochorionic, biamniotic twin pregnancy with the demise of both fetuses. Two intramural fibroids were visualized: One anterior (68 × 63 mm) and one posterior (85 × 45 mm). The patient was admitted for termination of the pregnancy by extra-amniotic ripening with prostaglandin E2. After 36 h of treatment, no cervical dilation was observed, so a D&C was performed under local anesthesia and US guidance. The intervention was uncomplicated. Prophylactic IV cefazolin was administered at the time of the procedure, but 18 h later the patient developed fever.
Physical examination was notable only for a tender uterus; there were no signs of peritonitis. White blood cell count was normal (9.3 × 103/mm3 with 86% neutrophils), but the C-reactive protein (CRP) concentration was elevated (153 mg/dL). Additional examinations (microscopic urine examination, chest radiography, and echocardiography) obtained to rule out potential sources of sepsis were normal. The endometrial layer measured 6 mm on the transvaginal US. Aerobic cervical cultures were negative, whereas cultures for Ureaplasma urealyticum were positive. Blood cultures were positive forEscherichia coli, suggestive of sepsis secondary to post-operative endometritis.
Intravenous treatment with netilmycin and amoxicillin–clavulanic acid was started in accordance with the bacterial sensitivity to antibiotics. The fever diminished and neutrophilia improved to 72% after six days of IV antibiotic treatment. The patient was discharged with a CRP concentration of 53 mg/dL. Amoxicillin–clavulanic acid was prescribed for 10 more days. One day after the discontinuation of this treatment, the patient returned to the emergency department complaining of severe lower abdominal pain without fever. Fibroid necrosis was suspected and the patient was admitted for analgesia. During hospitalization, the patient developed fever up to 39.2°C. White blood cell count and differential were normal, but CRP was elevated (75 mg/dL). Blood cultures were negative. Amoxicillin–clavulanic acid and netilmycin were administered IV, and non-steroidal anti-inflammatory drugs were added.
Five days later, spontaneous expulsion of a necrotic fibroid measuring 81 × 40 × 33 mm. Ultrasound after expulsion showed the presence of an anterior fibroid and another image compatible with the retention of placental tissue. As fever persisted, a second D&C under local anesthesia and US supervision was performed. Pus and a small amount of tissue were evacuated. Pathological examination could not confirm the presence of placental tissue. Following expulsion and curettage, neutrophilia diminished and clinical symptoms disappeared. The patient was discharged and received amoxicillin–clavulanic acid for ten more days.
She presented again with abdominal pain after nine days. On examination, the uterus was tender. The anterior fibroid presented as a heterogeneous mass on pelvic US, suggestive of suppurative disease. On CT scan, the diagnosis was confirmed (Fig. 1). Percutaneous drainage of the pyomyoma was undertaken to drain and lavage the pyomyoma (Fig. 2). Cultures were positive for E. coli, and the antibiotic treatment was adjusted according to the antibiogram (ciprofloxacin). After seven days, the pigtail catheter was removed, and the patient left the hospital in good clinical condition five days later.
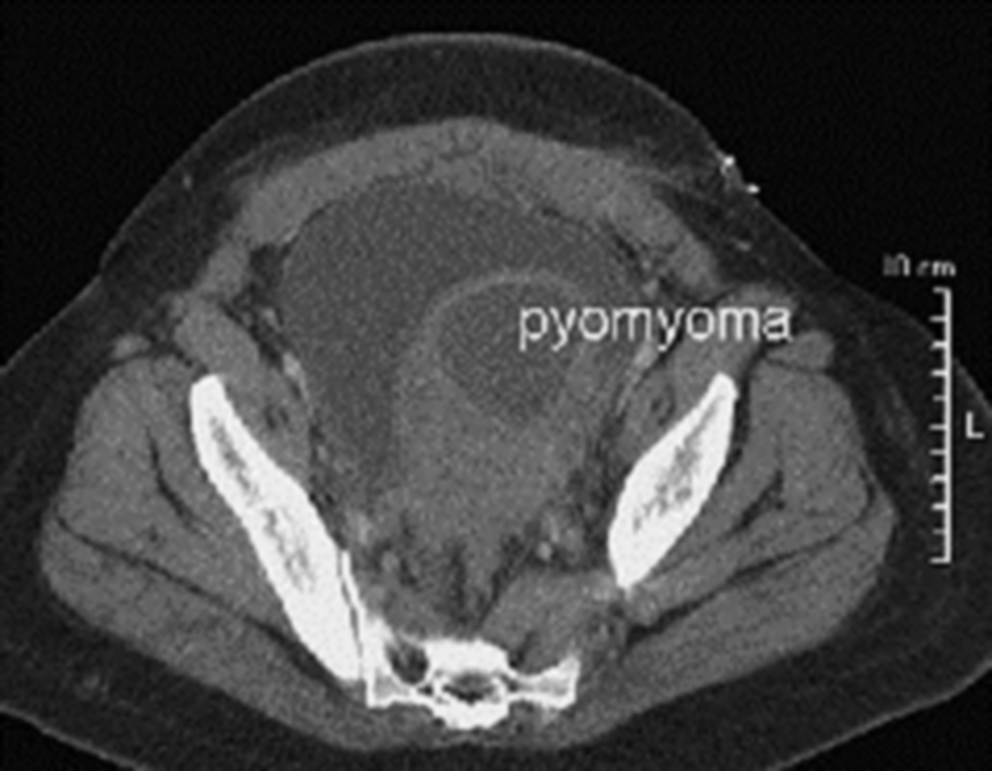
Anterior pyomyoma (case 1).
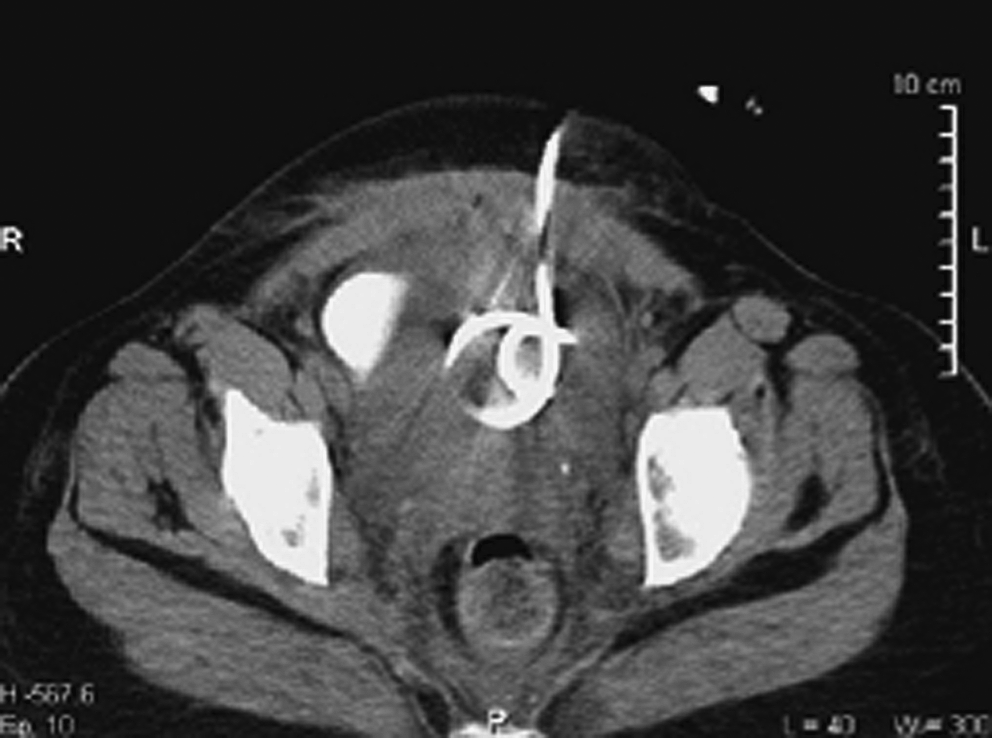
Pigtail catheter inserted into pyomyoma (case 1).
A hysterosalpingography performed after six months showed a normal endometrial cavity and no additional fibroids. The patient was authorized to attempt pregnancy again.
Sixteen months later, the patient gave birth to a healthy boy by secondary cesarean section because of fetal distress. During surgery, no fibroid was noted on the anterior wall of the uterus, no signs of uterine dehiscence were noted, and no adhesions were present. The clinical condition of both the patient and neonate progressed favorably, and both were discharged in perfect condition.
Case 2
A 35-year-old, black, gravida 2 para 0 woman was admitted for preterm labor at 33 weeks of pregnancy, with the fetus presenting in footling breech. The patient's clinical history was complicated by a myomectomy with opening of the uterine cavity several years prior to the pregnancy. Spontaneous rupture of the membranes occurred, and a secondary cesarean section was performed. During this intervention, multiple uterine fibroids were observed. Pathological diagnosis of the placenta showed signs of chorioamnionitis. Despite perioperative antibiotic prophylaxis with cefazolin, the postpartum period was complicated by fever and abdominal tenderness. The patient's white blood cell count was 12.6 × 103/mm3 with normal differential, and CRP was elevated (108 mg/dL). Blood cultures remained negative. Clinically, endometritis was suspected and IV amoxicillin–clavulanic acid and gentamicin were initiated.
Because of persistent fever and uterine tenderness, a CT scan was performed, which showed an abscess in an anterior fibroid (105 × 95 mm). A pigtail catheter was introduced into the pyomyoma, and the pus was drained. Cultures were positive for E. coli and Candida albicans and C. dubliniensis, and consequently, fluconazole was added. The patient's clinical and laboratory status improved, and the pigtail catheter was removed after three days. Antibiotic treatment was discontinued five days later. The white blood cell count and CRP normalized. The patient left the hospital 17 days after delivery in good clinical condition and was able to become pregnant again.
Case 3
A 31-year-old, black, gravida 3 para 0 woman presented with preterm, premature rupture of membranes at 29 weeks’ gestation. Her medical history was uncomplicated except for a myomectomy without opening of the uterine cavity. The present pregnancy was complicated by two episodes of necrosis of an anterior fibroid at 15 and 24 weeks. Treatment with non-steroidal anti-inflammatory drugs was successful each time. At admission, the patient had a temperature of 38.2°C but was in good clinical condition. As signs of fetal distress were discovered on the cardiotocogram and the fetus presented in footling breech, an emergency cesarean section was performed. During this intervention, a large anterior fibroid measuring 80 × 75 mm was observed close to the uterine incision. Amoxicillin–clavulanic acid was started immediately after the umbilical cord was clamped, but fever persisted and blood inflammatory parameters increased after delivery. Blood cultures and microscopic urine examination were negative. The patient developed a surgical site infection with Enterococcus faecalis and a Streptococcus species. The scar was opened for drainage on postoperative day five, but fever and inflammation persisted. A CT scan showed an abscess of the anterior fibroid and a communication with the infected skin incision. The patient refused a hysterectomy, and thus drainage of the pyomyoma by pigtail catheter insertion (as described in the two previous cases) was attempted. Cultures performed on the drained pus were positive for the same bacteria as the surgical site. Fever persistence for more than 48 h and the persistence of all inflammatory parameters despite therapy with amoxicillin–clavulanic acid and netilmycin indicated the failure of non-operative management. Thus, a subtotal interindexical hysterectomy was performed. The initial surgical site was left open to heal spontaneously. The patient left the hospital in good clinical condition ten days after hysterectomy.
Discussion
Herein we describe three cases of pyomyoma, an exceptional complication of fibroids in pregnancy, with an incidence of approximately 0.5% before the introduction of antibiotics in 1945 [1–3]. In the historic review by Miller [1], the mortality rate was found to exceed 50%.
Since 1945, 13 cases of pyomyoma related to pregnancy [4–13] including ours have been described in the literature (Table 1). In six of 13 patients, pyomyoma occurred after preterm rupture of membranes or a second trimester miscarriage. Recent work on preterm labor and delivery emphasizes the importance of subclinical infection in the pathogenesis of these conditions [14]. In the presence of a uterine fibroma, ascending infections may lead to the colonization of necrotie tissue. Four other cases [5,6,12,13] and those reported herein developed after uterine manipulation, such as cesarean section or elective abortion, suggesting the possibility of a perioperative infection. Our cases reflect a combination of two risk factors: Two patients presented with premature rupture of membranes and delivered by cesarean section, and the third patient had a curettage followed by an ascending infection.
Note: TAH + BSO, total abdominal hysterectomy and bilateral salpingoophorectomy; AB, intravenous antibiotic therapy; PPROM, pre-term premature rupture of membranes.
The clinical symptoms and signs of this condition are misleading (Table 2). Even though the presence of a fibroma related to pregnancy was known in all cases, the diagnosis was not suspected immediately. Fever and a tender uterus were described initially in all cases. Persistent fever after antibiotic treatment for suspected endometritis leads to the search for other possible origins of sepsis. After a review of the described cases, we agree with Greenspoon et al. [15], who postulated that the combination of known uterine fibroids with sepsis in the absence of an apparent etiology for bacteremia should raise the suspicion of pyomyoma. Diagnosis of this type of intraabdominal abscess is made easily by CT scan [3,16]. The radiological image, showing a combination of fluid and air inside an existing uterine fibroid, is highly suggestive of pyomyoma [13].
Treatment with IV antibiotics and total hysterectomy or myomectomy is the primary approach to pyomyoma (Table 1), as described in all cases prior to ours [4–13]. This surgical approach cures all patients but is associated with major morbidity. Uterine surgery in the immediate postpartum period is known to involve additional complications such as excessive blood loss and surgical site infections. Total abdominal hysterectomy leads to irreversible sterility and induces premature menopause if combined with bilateral salpingoophorectomy. Therefore, the need for a less invasive but curative intervention exists, especially for nulli- and primiparous women or critically ill patients.
Transabdominal drainage of intraabdominal, ovarian, and tubal abcedations under US or CT guidance has been described previously [16]. In more than 80% of the cases, this technique results in resolution of the clinical symptoms of infection and cures the patient [17]. Our cases illustrate that the drainage of pyomyomas under CT guidance can be successful. Broad-spectrum antibiotic treatment is always indicated. In the third case, the combination of a pyomyoma with surgical site infection might have been a compromising factor and the cause for the failure of the drainage procedure. The success of this approach is illustrated by an uncomplicated pregnancy with delivery of a healthy term baby at 1 year after drainage in one case and an ongoing pregnancy in another case.
We conclude that drainage and lavage of pyomyoma is a therapeutic, fertility-preserving option. In the absence of an appropriate response to this treatment, total abdominal hysterectomy remains the treatment of choice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.