
Abstract
Abstract
Background:
Timely re-dosing of antibiotic for prolonged surgical cases is an important measure in reducing the risk of surgical site infections. For the anesthesia team, which generally administers the antibiotic re-doses, it is difficult to keep track of and remember the exact timing requirements. We explored the efficacy of two types of electronic reminders to aid the anesthesia team in performing timely antibiotic re-doses.
Methods:
The first electronic reminder was a timer-triggered “blinking button” feature in the Anesthesia Information Management System (AIMS). The second was generated with a real-time decision support system, the Smart Anesthesia Messenger (SAM). The AIMS reminder was applied for the first five months of the study, whereas the SAM reminder was applied for the second five months. A retrospective analysis was performed to evaluate the efficacy of the reminder messages in improving the antibiotic re-dose success rate.
Results:
In a total of 940 cases, the anesthesia team was reminded of the need for antibiotic re-dosing with AIMS, whereas in 922 cases, the SAM system gave the reminder. The AIMS reminders achieved a timely re-dose success rate of 62.5% ± 1.6%, whereas the SAM reminders achieved a significantly higher success rate: 83.9% ± 3.4% (p < 0.001).
Conclusions:
Compared with the simple reminders generated with AIMS, the relevant, informative messages generated with SAM were more effective in improving compliance with timely antibiotic re-doses.
In the operating room, prophylactic antibiotic and any needed subsequent doses are almost always administered by the anesthesia team [12]. In the busy operating room environment, where the anesthesia team multi-tasks several critical care steps, a reminder system can improve antibiotic re-dose success rates. A computerized notification method employed by Zanetti et al. [13] was able to achieve a cefazolin re-dose compliance rate of 68% in cardiac cases. In a later approach by Jacques et al. [14], electronic reminders for the anesthesia team improved antibiotic re-dose compliance from 20% to 58% for non-cardiac surgical cases.
In this study, we report the effect of two types of electronic reminders on antibiotic re-dosing. The first utilized a feature of the Anesthesia Information Management System (AIMS; Docusys Inc., Atlanta, GA) that the anesthesia team uses to document anesthetic care. The second utilized a decision support system, Smart Anesthesia Messenger (SAM), to generate drug-specific electronic alerts.
Materials and Methods
Antibiotic re-dose protocol
At our institution (University of Washington Medical Center, Seattle, WA), specific guidelines (Table 1) for antibiotic re-dosing have been established on the basis of two to three times the half-lifes of commonly administered antibiotics. For an ongoing surgical procedure, an antibiotic is considered due for a re-dose when the time elapsed since its previous dose is nearing the drug's re-dose interval. In such an event, the anesthesia team administers the ordered re-dose amount and documents it in the anesthesia record (AIMS).
Anesthesia Information Management System features
For a variety of reasons, ranging from ease of use, greater safety, and better compliance, our institution has installed an AIMS, a computerized system that can be used by the anesthesia care team to document the anesthetic management of a surgical patient. Antibiotic documentation in AIMS is performed through a two-step process. Step 1 is documentation of the “Antibiotic Management Protocol,” and Step 2 is the documentation of the specific drug, dose, route, and time of administration. The buttons to bring up the screens needed to document the above data are configured on the main AIMS screen (Fig. 1). The users press the “Antibiotic Note” button to document the antibiotic management protocol and the “Bolus Meds” button to document the administration of the specific antibiotic. As shown in Table 2, the “Antibiotic Management Protocol” note template has options to document prophylactic antibiotic management, as well as re-dose management.
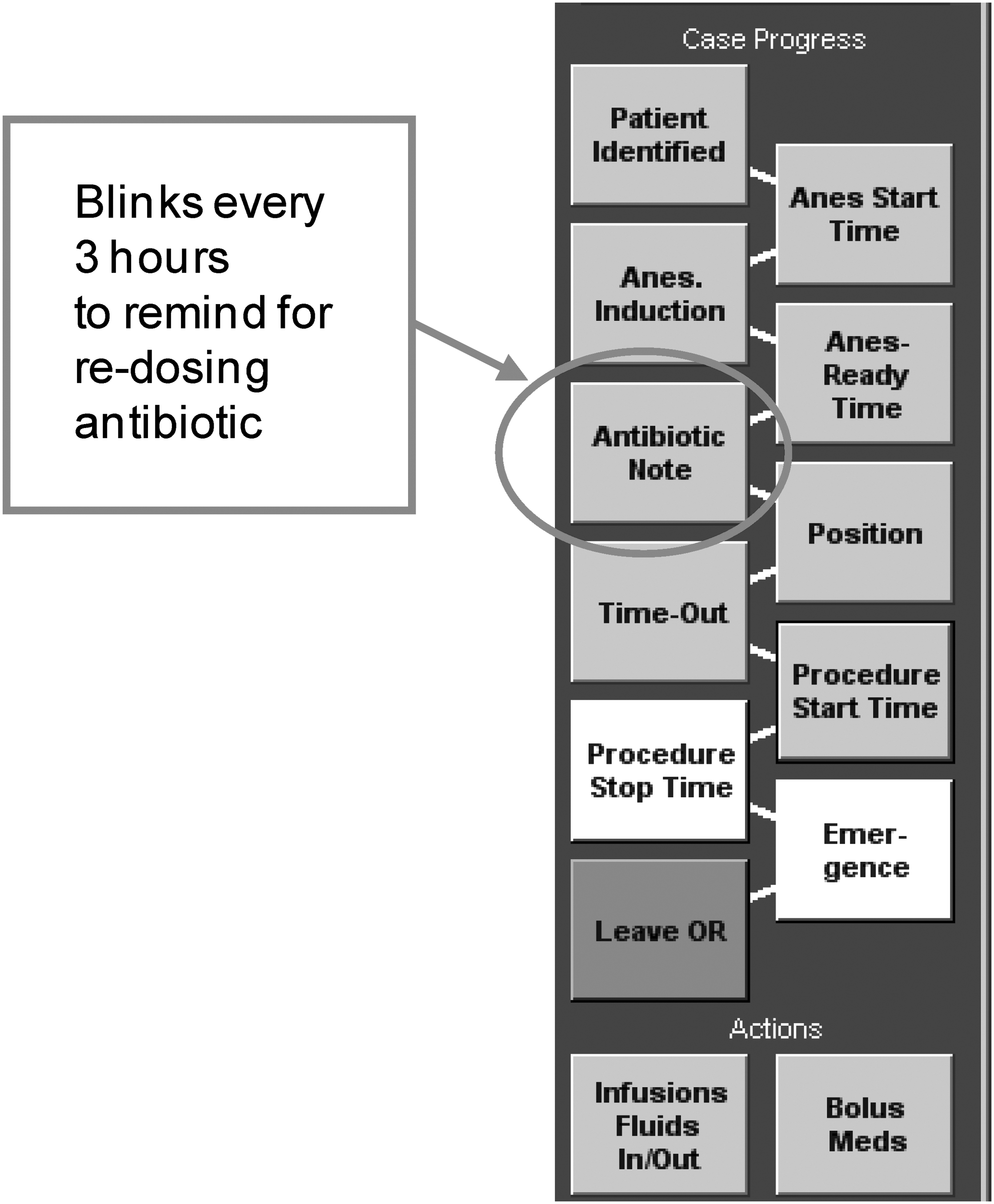
Anesthesia Information Management System screen showing “Antibiotic Note” button that blinks every 3 h.
Options related to antibiotic re-dose are in boldface.
The AIMS program has a feature to remind users if an antibiotic is due for a re-dose. Specifically, the “Antibiotic Note” button has a built-in timer that initiates blinking at a previously defined interval. Because the interval is a static parameter in AIMS, and because the shortest re-dose interval in our guideline was 3 h, we configured the timer to trigger blinking every 3 h. The timer is set off starting from the time the anesthesia team last pressed the “Antibiotic Note” button. Thus, the timer is reset when the user documents prophylactic antibiotic management through the “Antibiotic Note” button and triggers blinking of the button 3 h later. If the antibiotic is re-dosed, this is documented using the “Antibiotic Note” button, which in turn resets the timer to start blinking another 3 h later.
Smart Anesthesia Messenger features
The blinking button feature of the AIMS has limitations. The blinking is triggered irrespective of whether a prophylactic antibiotic is administered. Moreover, this feature does not accommodate the different re-dose intervals appropriate for various antibiotics. Additionally, the timer can be reset easily if the user accidentally presses the “Antibiotic Note” button.
To have a better reminder for antibiotic re-dose, we utilize a real-time decision support system: Smart Anesthesia Messenger (SAM). This is a server-based application that analyzes AIMS data in near real-time at a sampling interval of 6 min. On the basis of the analysis, messages related to patient care and wrong or missing documentation are transmitted to the individual AIMS workstations documenting the surgical case. Each AIMS workstation also runs a client component of SAM. The SAM client receives messages from the server and displays them on a pop-up screen overlaid on the AIMS screens (Fig. 2). The SAM was developed internally using University of Washington resources.
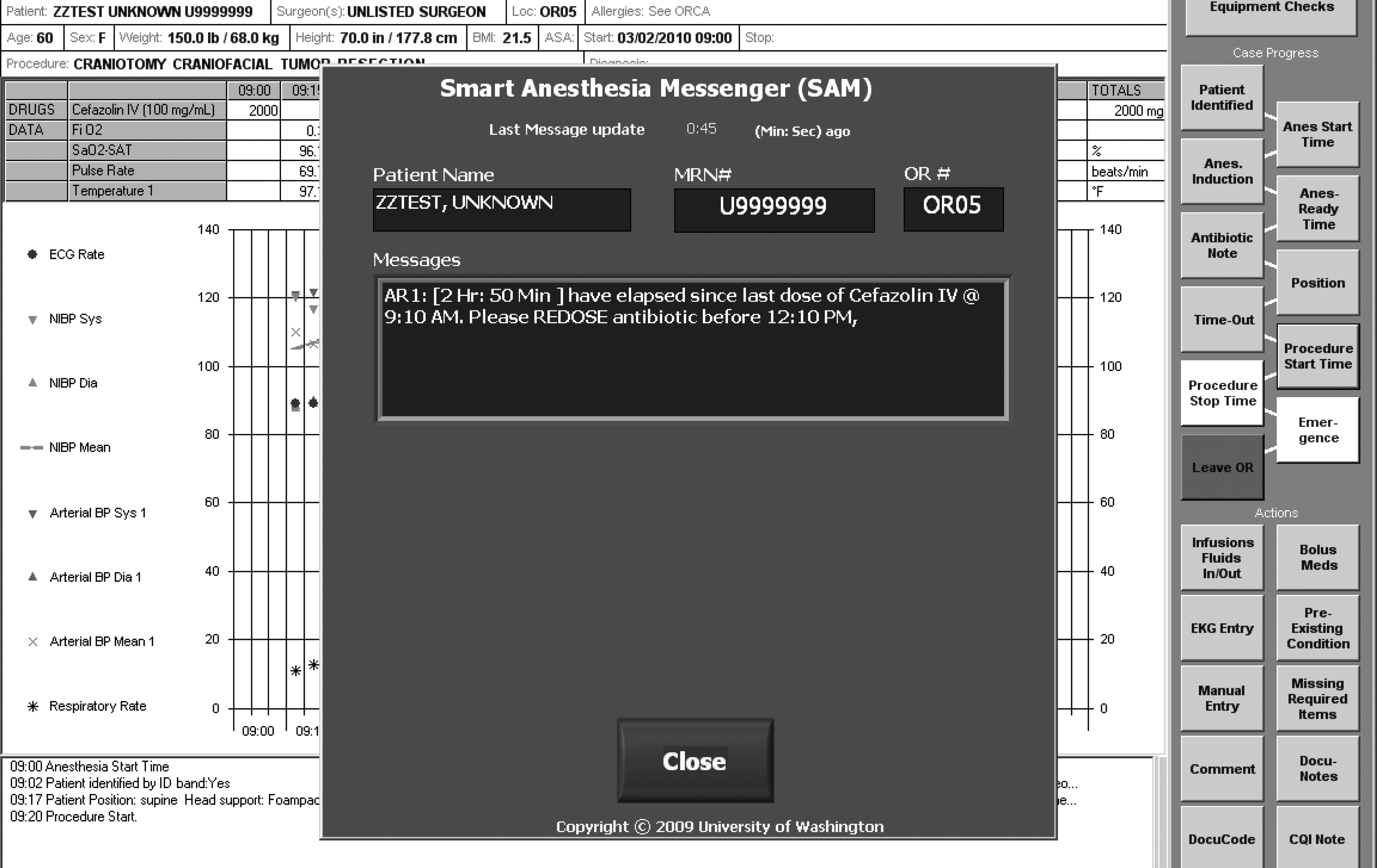
Smart Anesthesia Messenger antibiotic re-dose message overlaid on Anesthesia Information Management screen.
SAM was programmed to generate antibiotic re-dose reminders. Specifically, SAM first detects whether a prophylactic antibiotic was administered by the anesthesia team. If so, it triggers an internal timer specific to that antibiotic. The internal timer is based on the re-dose intervals outlined in protocol guidelines. The SAM starts generating reminder messages 15 min prior to the time an antibiotic is due for re-dose. The message describes how much time has elapsed since the last dose of the antibiotic and the time remaining until it should be re-dosed (Fig. 3A). The re-dose message is repeated every 6 min until either the antibiotic is re-dosed and documented, or the re-dose is past due. If the re-dose is past due, a second message is generated repeatedly notifying the anesthesia team that the antibiotic should have been re-dosed (Fig. 3B). The second message also requests the users to document the re-dosed antibiotic if one was administered or that the antibiotic was not re-dosed for a medical reason. The re-dose reminders are not generated if either the end of the surgical procedure is documented or there is documentation that the antibiotic has not been re-dosed for a medical reason.

Smart Anesthesia Messenger messages for antibiotic re-dose. (
The SAM reminders for Docusys were placed in production starting September 1, 2009. At the same time, the blinking button feature of the AIMS system was inactivated.
Data Collection and Statistical Analysis
After obtaining Institutional Review Board approval, data concerning the antibiotic dose and the antibiotic management note were extracted from the AIMS database. Ten contiguous months worth of data, with five months of AIMS reminders and five months of SAM reminders, were analyzed retrospectively. Cases included for analysis were chosen according to the criteria outlined in Table 3 and included those that required at least one re-dose of the antibiotic. Antibiotic re-dosing was considered failed if one of three scenarios occurred: (1) Antibiotic re-dosing was never performed, and there was no documentation that it was not performed for a medical reason; (2) the antibiotic was re-dosed more than 15 min before the recommended time (early); or (3) the antibiotic was re-dosed more than 15 min after the recommended time (late). The recommended re-dose time was computed according to specific guidelines. The 15-min grace periods before and after the recommended time provided the anesthesia care giver sufficient time to view the notification and order and administer the antibiotic.
Monthly success rates of antibiotic re-doses were computed for the two five-month periods when AIMS and SAM notifications were used. To compare the results for the two groups, the Student t-test was performed using GraphPad Software (GraphPad Sofware, Inc., La Jolla, CA). Results were considered statistically significant if the p value was below 0.05.
In addition to antibiotic information, data on the age of the patients, American Society of Anesthesiologists (ASA) stratification code, and procedure duration were extracted from the AIMS database to make sure that the groups of cases with AIMS and SAM reminders were evenly matched with respect to these variables.
Results
Analysis of data was aimed primarily at comparing the antibiotic re-dose success rates with AIMS and SAM reminders. A total of 940 and 922 patients, respectively, required antibiotic re-doses. Among these, 188 in the first group (with AIMS reminder) and 187 in the second group (with SAM reminder) required multiple re-doses. The number of instances when antibiotic needed to be re-dosed was 1,205 for group 1 and 1,156 for group 2. For each group, data corresponding to the patient age, procedure length, ASA class, and type of antibiotic are shown in Table 4. In general, the two groups were evenly matched for most features. However, the mean duration of the procedure was somewhat longer for cases for which the AIMS reminder was used, and there was a slightly higher fraction of cefazolin uses for the group with SAM reminders.
American Society of Anesthesiologists.
To assess the difference in antibiotic re-dose as a result of SAM messages, monthly success rates with AIMS and SAM reminders were plotted (Fig. 4). With AIMS reminders, the re-dose success rate averaged 62.5% ± 1.6%. However, after SAM installation, the success rate rose to 83.9% ± 3.4% (p < 0.001). As is evident from Figure 4, the change in the success rate was dramatic, with the improvement seen immediately after initiating SAM reminders on September 1, 2009. The month-to-month variability in success rates was small within each group, with a standard deviation close to 3%.

Trends in antibiotic re-dose success rate before and after institution of Smart Anesthesia Messenger.
In addition to the overall success rate shown in Figure 4, we computed the success rates for the first re-dose and any subsequent re-doses. The success rates for the first re-dose were 60.6% ± 1.7% with AIMS and 83.2% ± 2.8% with SAM reminders. For subsequent re-doses, the success rates were higher at 69.4% ± 4.5% and 86.6% ± 6.9% for the two groups, although the improvement achieved with SAM messages was slightly less.
As described earlier, we classified the re-dose failures into three categories. The failure rates in each are shown in Table 5. For all three categories, the failure rates were reduced after SAM installation, with the greatest decrease noted for the “late” and “no re-dose” categories.
AIMS = Anesthesia Information Management System; SAM =Smart Anesthesia Messenger.
To evaluate the timing of the antibiotic re-dose more closely, we prepared a distribution graph of the actual re-dose time relative to the recommended time (Fig. 5). Relative re-dose time is the difference between the actual and the recommended times. The relative re-dose time is negative if the antibiotic is given earlier than recommended, whereas it is positive if the drug is given after the recommended time. Each point in the distribution graph shows the percentage of time antibiotics were re-dosed for each relative time. Figure 5 shows the re-dose timing distribution with AIMS and SAM reminders. The distribution curve is much tighter for SAM messages, with 30% of the re-doses occurring 10 min before the recommended time.
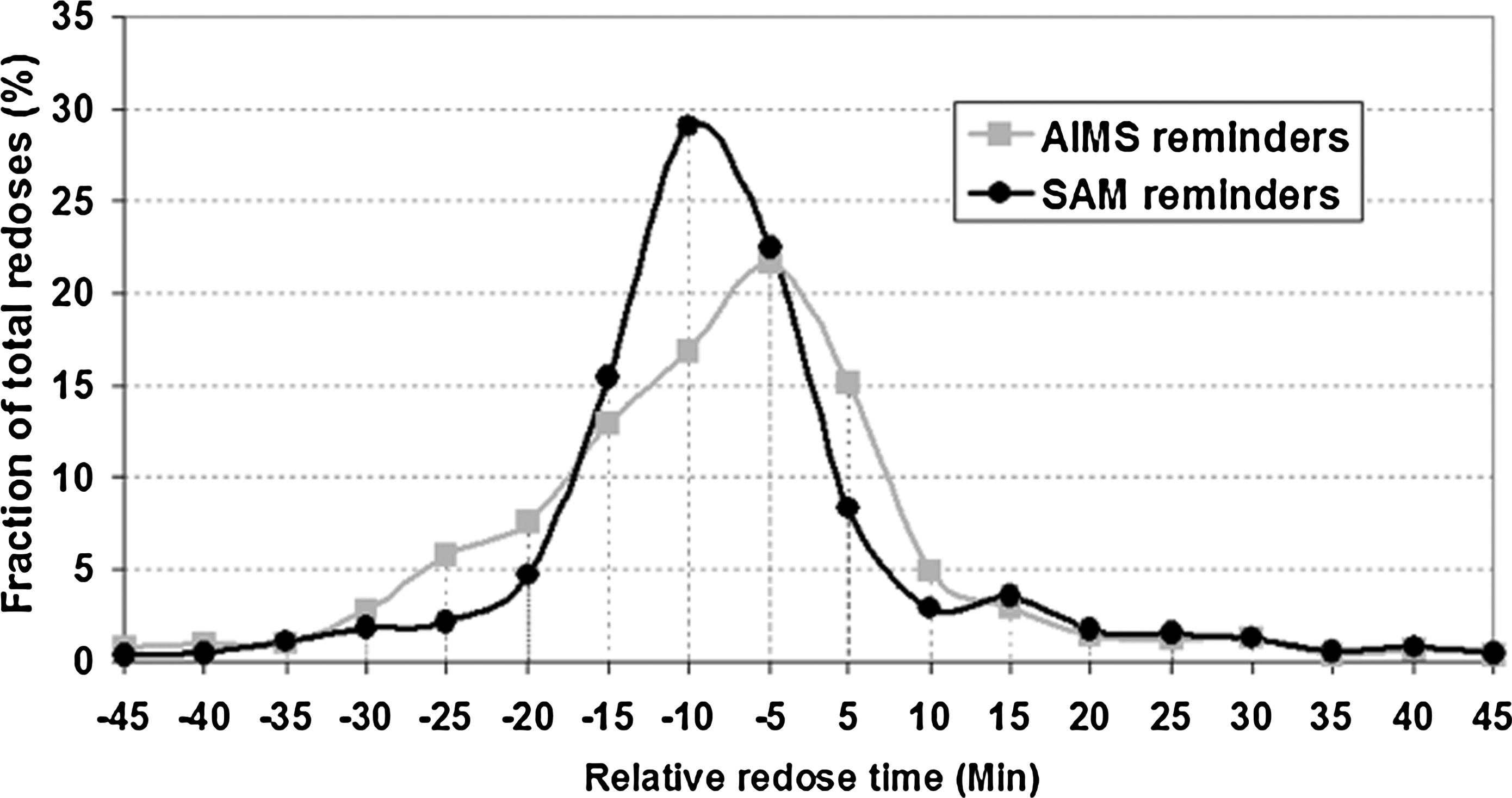
Distribution of antibiotic re-doses in relation to recommended time. AIMS = Anesthesia Information Management System; SAM = Smart Anesthesia Messenger.
Discussion
Timely administration of prophylactic antibiotics is an important measure to minimize the risk of SSI. The use of electronic reminders to improve compliance with prophylactic antibiotics has been tried previously [9–11]. Similar attempts to improve antibiotic re-dosing have produced only moderate success [13,14]. In this study, we compared the effects of two types of reminders in improving re-dose success. The first reminder system used an existing feature in AIMS software, whereas the second one used a real-time decision support system to generate electronic alerts. Most commercial AIMS programs provide functions to remind the anesthesia team of clinical care items such as antibiotic management. However, they tend to be simple features, often generating non-relevant reminders that usually are ignored. In spite of this disadvantage, the simple AIMS reminders were able to achieve a re-dose success rate (63%) similar to those reported by previous studies, such as the 58% achieved by Jacques et al. [14]. Noting the limitations of the AIMS reminder, we established an alternate notification scheme using an internally developed real-time decision support system called SAM. Unlike previous attempts, automated alerts with SAM focus on generating frequent reminders that present information on how much time has elapsed since the last antibiotic dose and at what time a re-dose is due. Re-dose reminders are not generated if there is documentation that a prophylactic antibiotic was not administered or if the antibiotic was not re-dosed for a medical reason. By generating timely and relevant messages, we could maximize users' attention and minimize information overload. Additionally, we generated messages to remind users to document the antibiotic re-dose, ensuring that if the antibiotic was indeed re-dosed, this was documented in the anesthetic record. With this approach, we were able to achieve a significantly higher re-dose success rate (∼84%).
We could not evaluate the improvement in re-dose success rate attributable to the AIMS itself because prior to AIMS installation, paper anesthesia records were used, and antibiotic re-dose data were not available in an electronic format. This made it difficult to compare re-dose success rates with and without any reminders.
The results achieved with the SAM system show that the majority of the re-dose failures are attributable to early antibiotic administration. If there is an early re-dose, notification messages are not generated with the existing messaging logic. Early re-dosing is difficult to prevent; however, a one-time notification stating that the antibiotic was administered early may teach users to wait for SAM reminders to initiate an antibiotic re-dose. This is planned as a future enhancement to SAM. Because the main goal of antimicrobial re-dosing is to maintain tissue and serum concentrations of antibiotics above the target organism's minimal inhibitory concentration during the entire operative period, it can be argued that early re-doses of antibiotic may not be detrimental. Interestingly, if you expand the grace period for “early failure” from 15 min to 30 min prior to the recommended re-dose time, the success rate with SAM would be close to 95%. In comparison, AIMS achieved a success rate of nearly 80%.
Although late or missed administration of antibiotic re-doses with SAM reminders was rare, the reasons for such failures are not clear. One possible reason is that the anesthesia team underestimated the length of the surgical procedure and ignored the reminder messages when in reality the procedure ended later than expected. Another reason could be that the antibiotic was re-dosed in a timely fashion, but the anesthesia team documented the re-dose retrospectively without editing the administration time to the correct value. On rare occasions, it could be that the SAM system did not generate a message because of a software failure.
The SAM system proved to be an efficient and cost-effective way to ensure a high success rate of antibiotic re-dosing. The development cost and time were around $40,000 and six months, respectively. The maintenance cost of this system is low, at around $10,000 per year. The SAM works reliably alongside AIMS without compromising AIMS functionality.
Timely re-dosing of antibiotic is critical in minimizing the probability of SSI. Compared with the simple reminders that AIMS provides, the relevant, informative reminders automatically generated by SAM achieved high success rates of timely antibiotic re-doses.
Author Disclosure Statement
Support for the development of the Smart Anesthesia Messenger (SAM) was provided entirely by the University of Washington Department of Anesthesiology and Pain Medicine, University of Washington Medicine IT Services, and the University of Washington Medical Center Patient Care Services. None of the authors has any commercial associations that might create a conflict of interest in connection with this manuscript.
Footnotes
Acknowledgment
We thank Rafael Vergara, Patient Care Services, University of Washington Medical Center, for helping with SAM installation and support.