
Abstract
Abstract
Background:
Clostridial myonecrosis is an uncommon, highly lethal necrotizing soft tissue infection. The source may be occult at the time of clinical presentation. In cases caused by Clostridium septicum, there is an association with colorectal malignant disease, suggesting that underlying colonic pathology frequently is the source of the infection.
Methods:
Case report and literature review.
Case Report:
A 37-year old man with acquired immunodeficiency syndrome, end-stage renal disease, and C. difficile colitis presented to the Emergency Department (ED) with a primary complaint of abdominal pain and incidental right forearm pain. While undergoing evaluation in the ED, he developed progressive erythema, edema, and emergence of bullae over his right forearm. After rapid imaging of his abdomen, he underwent guillotine amputation of his right upper extremity because of extensive myonecrosis and total abdominal colectomy secondary to right colonic necrosis and C. difficile colitis. Blood cultures were positive for C. septicum. Microscopic examination of both the necrotic colon and the right forearm musculature demonstrated invasion of gram-positive bacilli throughout.
Conclusions:
Myonecrosis caused by C. septicum frequently occurs in the presence of colonic pathology, typically malignant disease. This case report illustrates the development of this pathological process in an immunosuppressed patient who did not have colon cancer, but rather colonic mucosal inflammation produced by C. difficile.
The case detailed here involved simultaneous necrotizing soft tissue infection and colon necrosis caused by C. septicum, which appears to have arisen in the setting of underlying colonic mucosal pathology secondary to C. difficile.
Case Report
Clinical course
A 37-year old man with severe acquired immunodeficiency syndrome (recent absolute CD4+ count 9 cells/mm3), end-stage renal disease, and recent hospitalization for C. difficile colitis presented to the Emergency Department (ED) because of increasing abdominal pain associated with nausea and diarrhea. He incidentally noted right forearm pain, described as aching and burning. His medical history was remarkable for hypertension, gastroesophageal reflux disease, and a myocardial infarction in the past. He also had been hospitalized for three weeks recently with severe C. difficile colitis and had been discharged on a regimen of oral vancomycin and metronidazole. There was no history of abdominal operations. The patient had undergone transurethral prostatic resection six years previously because of bladder neck obstruction and multiple vascular access procedures. He was receiving highly active antiretroviral therapy; however, he had stopped taking vancomycin and metronidazole because he felt better. Of note, the patient had a history of non-compliance with his medications.
On initial examination, the patient appeared moderately ill. His temperature was 39.4°C, his heart rate was 124 beats/min, his blood pressure was 165/79 mm Hg, and his ventilatory rate was 18 breaths/min. His abdomen was scaphoid, but tender to palpation diffusely, more so in the right lower quadrant. His right arm had marked erythema over part of the forearm.
Laboratory studies were requested, and blood was drawn for culture. His hemoglobin concentration was 13.2 g/dL, but the white blood cell count was 1,200 cells/microliter, with an absolute neutrophil count of 700 cells/microliter. The blood glucose concentration was slightly low at 62 mg/dL. The blood urea nitrogen and creatinine concentrations were 36 and 8.2 mg/dL, respectively, but electrolyte values were normal. The lactic acid concentration was 1.6 mmol/L. Initial radiographs of the abdomen were unremarkable; thus, computed tomography (CT) of the abdomen and pelvis was requested. The patient received 2 L of physiologic saline for resuscitation. He was started on intravenous vancomycin for presumed cellulitis of the right upper extremity and on oral metronidazole for presumptive recurrent or ongoing C. difficile colitis.
The patient was re-examined within 1–2 h of his initial presentation and appeared to have deteriorated substantially. He was diaphoretic, non-communicative, and in severe distress from pain. He remained febrile, tachycardic, and hypertensive. He had developed tachypnea, with a ventilatory rate of 24–30 breaths/min. There was now involuntary guarding and rebound tenderness on abdominal examination. His right forearm was markedly edematous and warm to the elbow. Large bullae had developed up to the elbow. Erythema extended above the elbow. A radial pulse could not be palpated, although there were strong Doppler signals in the right radial and ulnar arteries. The right upper arm dialysis graft had a good thrill. An arterial blood gas assay revealed metabolic acidosis, with a pH of 7.26 and a calculated bicarbonate concentration of 16 mmol/L. In addition to the vancomycin and metronidazole, intravenous clindamycin was administered. Surgical consultants recommended that the patient undergo emergency exploration of the right upper extremity and abdomen. The patient was informed that there was a high likelihood that he would have to undergo amputation of his right upper extremity and subtotal colectomy with ileostomy formation. The patient consented orally to this, although it was unclear if he fully understood the implications. There was no designated decision-maker available to provide surrogate consent.
While the operating room was being prepared for the procedure, the patient underwent rapid CT imaging of the abdomen and pelvis, with the right arm being included in the field. This demonstrated diffuse thickening of the wall of the entire colon with thumbprinting, consistent with pancolitis (Fig. 1A). The small bowel was hyperemic and slightly thick-walled, suggesting reactive ileus. There was focal loss of definition of the cecal wall with adjacent extraluminal gas, consistent with perforation of the cecum (Fig. 1B). Gas was noted to be tracking within the anterior compartment of the forearm proximally and through the anterolateral aspect of the right upper arm (Fig. 1A and 1B).
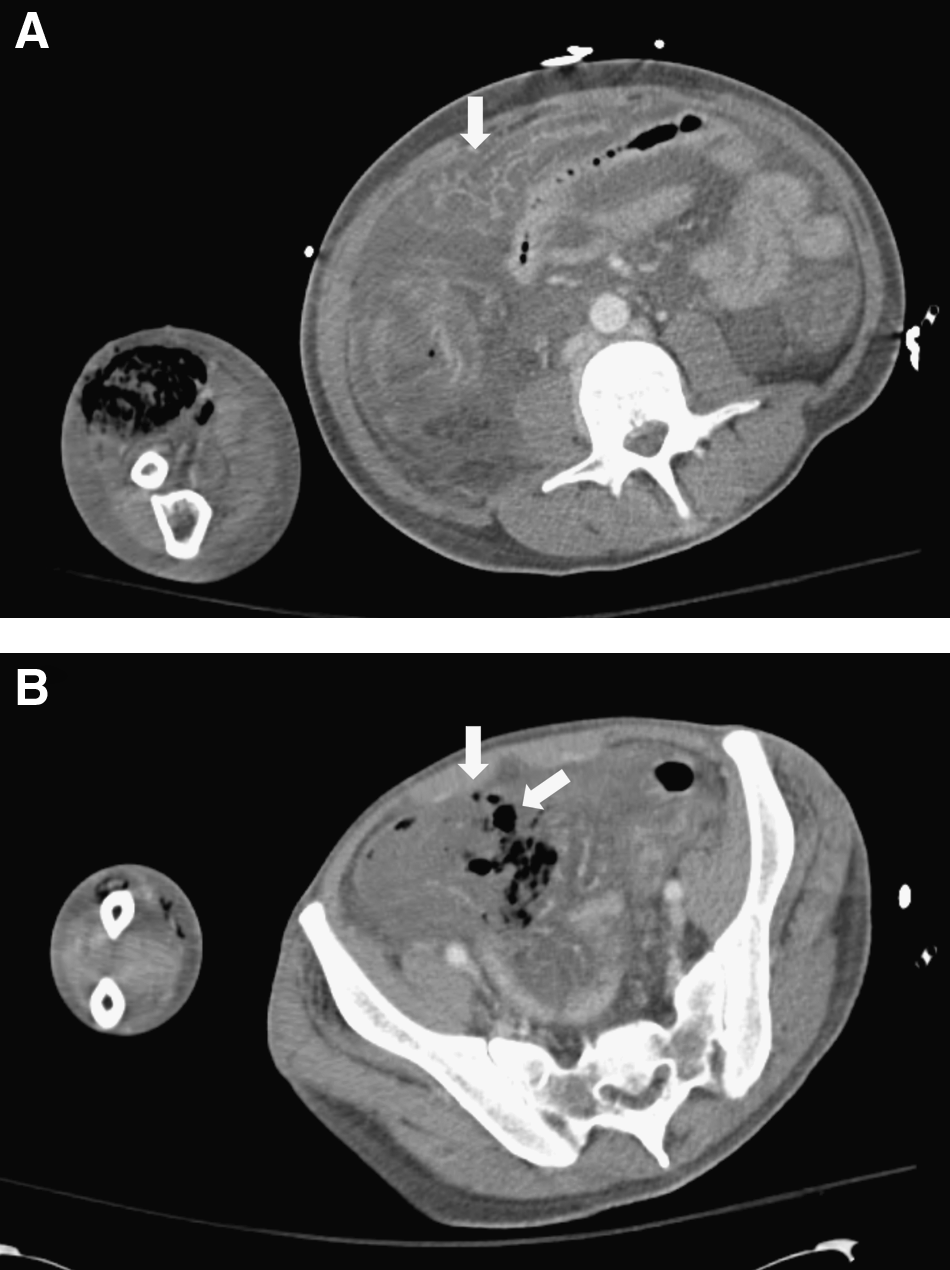
Computed tomography of abdomen showing (
After this imaging study, the patient was transported to the operating room, where he underwent exploration of the right arm. All of the musculature of the forearm was pale and non-contractile; fine bubbles of gas exuded from the muscle wherever the fascia was opened. Myonecrosis extended above the elbow and involved most of the musculature of the anterior and posterior compartments nearly to the level of the shoulder. There was sparing of muscle located within a few centimeters of the patent dialysis graft. A high right above-the-elbow guillotine amputation was performed with ligation of the dialysis graft. The patient then underwent exploratory laparotomy, which revealed necrosis of the right side of the colon and severe edema of the remaining portion of the colon. A right hemicolectomy was performed. Opening of the specimen revealed marked pseudomembrane formation beyond the area of transmural necrosis, consistent with severe C. difficile colitis. The left side of the colon was therefore resected to complete a total abdominal colectomy. During the procedure, the patient became progressively hypotensive, for which he was started on a norepinephrine infusion, and developed worsening acidosis and coagulopathy, with an international normalized ratio of 2.65. Therefore, the procedure was truncated, and the patient did not have an ileostomy created. Abdominal packs were placed for hemostasis and a temporary vacuum-type abdominal closure was utilized. The plan was to return the patient to the operating room in 24–48 h for a second-look laparotomy, as well as re-exploration of the right upper-extremity stump, once the patient was more stable.
Postoperatively, the patient was admitted to the surgical intensive care unit. He was treated with intravenous vancomycin, clindamycin, and meropenem; the latter was switched subsequently to cefepime. Blood cultures obtained in the ED returned C. septicum, but tissue cultures obtained at the time of amputation failed to yield any organisms. He remained on vasopressor therapy because of hypotension and on mechanical ventilation for respiratory failure. After 24 h, his condition had stabilized somewhat. Continuous veno-venous hemodialysis (CVVHD) was initiated using temporary venous access. The patient's arm wound appeared clean at the time of dressing changes.
He was returned to the operating room within 48 h for re-exploration of his right arm stump and abdomen. Only a minor amount of additional necrotic muscle was found in his arm, and there was no evidence of bowel ischemia or hemorrhage in his abdomen. Abdominal packing was removed, and an ileostomy was created, but definitive fascial closure was not performed because of severe visceral edema. Subsequently, his condition continued to stabilize; vasopressor use was discontinued, and the patient had more aggressive removal of fluid using CVVHD. He was returned to the operating room again 48 h later, at which time, no necrosis of the remaining musculature of the right arm was noted. The patient had a gastrostomy tube placed, and his abdominal fascia was closed. The patient was able to be taken off mechanical ventilation the following day. Antibiotic therapy was continued using intravenous vancomycin, cefepime, and metronidazole. He remained stable hemodynamically for the next three days. He also became somewhat more alert and complained of substantial postoperative pain.
On postoperative day 8, the patient developed recurrent hypotension, with his hemoglobin concentration decreasing from 9.5 to 6.3 g/dL. He was therefore returned to the operating room for abdominal re-exploration. Bloody fluid and clot were evacuated from the abdomen, but no discrete source of bleeding was identified. The patient was returned to the surgical intensive care unit. He remained stable hemodynamically over the next four days but continued on mechanical ventilation because of continuing respiratory failure. He also remained obtunded and unable to participate in decision-making.
By this point, the patient's family had been located. Considering his new disabilities, as well as his chronic health problems, they questioned his desire for continued aggressive medical therapy. Discussions were held with the patient's family, who requested a change in the emphasis of medical care to comfort care only. Accordingly, mechanical ventilation and hemodialysis were discontinued, and the patient died approximately 24 h later.
Pathologic findings
Surgical pathology specimens from the initial operations exhibited extensive necrosis of both the right upper extremity and the colon. Microscopic examination confirmed pseudomembraneous colitis of the entire colon and transmural necrosis of the right colon (Figs. 2A, B). Gram-positive bacilli were observed in the seromuscular layers of the non-viable colon (Fig. 2C), but not in similar layers of viable colon. Microscopic examination of the muscle tissue of the arm confirmed necrosis (Fig. 3A). Gram-positive bacilli were demonstrated throughout the non-viable muscle (Fig. 3B). There was extensive vascular occlusion in both tissues. Only minimal inflammatory infiltrates were encountered in the necrotic areas of both the colon and the arm musculature.

Colon pathology. (
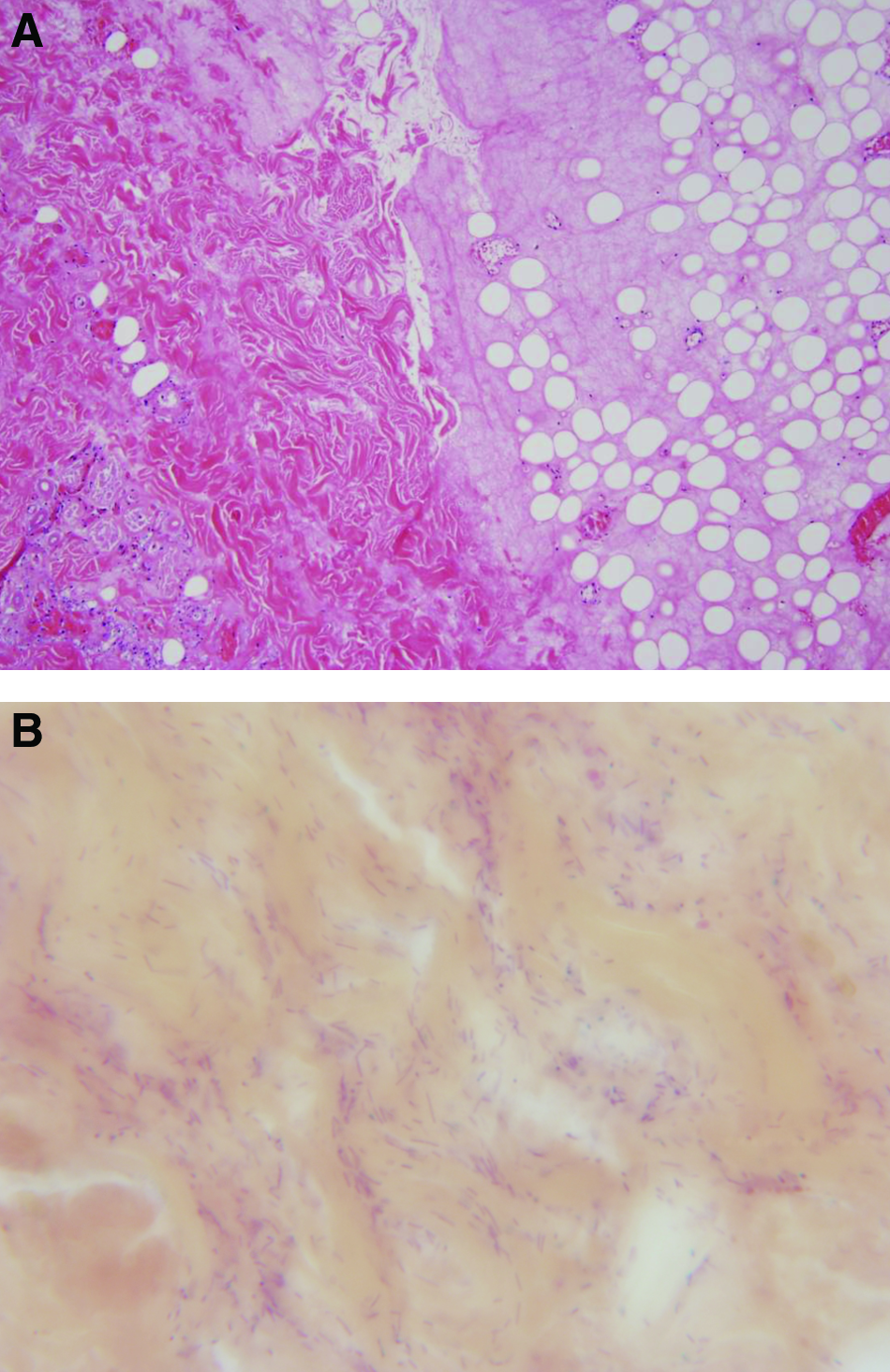
Right arm pathology. (
Discussion
The clinical history and pathological findings of this patient were interpreted as showing simultaneous myonecrosis and colonic necrosis caused by C. septicum. Presumably, an invasive infection attributable to this organism developed in the right side of the colon in the setting of immunosuppression by human immunodeficiency virus (HIV) infection and an inflammatory process of the colonic mucosa caused by C. difficile. Once an invasive C. septicum infection of the colon was established, it spread hematogenously to the right forearm, resulting in non-traumatic clostridial myonecrosis.
Clostridial myonecrosis is caused most commonly by C. perfringens or C. septicum, although other pathogenic clostridial species also can produce this disease process. Clostridia are gram-positive, anaerobic, spore-forming bacilli that produce multiple exotoxins. Of the 20 or more known exotoxins, α-toxin is considered to be the most virulent. Its phospholipase C activity leads to aggregation of platelets and leukocytes within blood vessels. This vessel occlusion leads to ischemic necrosis of the tissues and rapid spread of the infection [2,3].
There are approximately 1,000 cases of clostridial myonecrosis reported per year in the U.S., with a mortality rate ranging from 15%–70% [3–5]. Half of these cases are secondary to trauma, including motor vehicle collisions and industrial accidents, and 35% of cases are attributed to surgical complications [6]. Clostridium perfringens is responsible for approximately 80% of these traumatic cases [7]. However, clostridial myonecrosis also can occur in the absence of a direct injury. This is much less common, accounting for only about 10% of cases. For non-traumatic clostridial myonecrosis, 60% of the cases are caused by C. perfringens, and 30% are attributable to C. septicum. Co-infection with both organisms may occur [8].
Non-traumatic clostridial myonecrosis usually is an acute illness associated with certain chronic diseases. Patients with diabetes mellitus or peripheral vascular disease are at higher risk, presumably because the decreased oxygen tension in the tissues provides a better environment for proliferation of the anaerobes. Altered immune function in diabetic patients also may play a role. Other risk factors associated with non-traumatic clostridial myonecrosis include injection drug use, alcohol abuse, malnutrition, visceral or hematologic malignant disease, and immunosuppression secondary to HIV infection, chemotherapy, or glucocorticoids [9]. Common presenting symptoms are similar to those of traumatic myonecrosis: Severe pain out of proportion to findings on physical examination, fever, tachycardia, and hypotension. The skin has a brawny discoloration, and there is rapid development of bullae and crepitus. A foul-smelling discharge may be present. With progression, pain may diminish, and numbness may develop secondary to destruction of cutaneous nerves. The skin may change in color to blue or black secondary to thrombosis of nutrient vessels. As the infection progresses quickly, organ dysfunction develops, including acute kidney injury, mental status changes, and cardiovascular deterioration [3,10].
Optimal treatment of clostridial myonecrosis, as with all necrotizing soft tissue infections, requires that the diagnosis be considered. Although fulminant disease usually is recognized easily, the diagnosis may be much less apparent at earlier time points, when it is more amenable to therapy. Many patients present with only non-specific complaints of soft tissue pain and swelling. In addition, a source of infection may not be obvious, the patient's physical signs may not suggest an aggressive soft tissue infection, and laboratory values may not be markedly deranged. All these factors can lead to a major delay in diagnosis, which is associated with increased patient morbidity and mortality. Diagnostic testing may be inconclusive and delay diagnosis further, so prompt surgical exploration may be the most expeditious manner to determine whether a severe soft tissue infection, such as clostridial myonecrosis, is present.
Once diagnosed or strongly suspected, management of clostridial myonecrosis includes prompt antibiotic therapy and aggressive surgical debridement, in addition to restoration of intravascular volume deficits and other ancillary treatments for sepsis. Antibiotic or surgical therapy should not be delayed for further testing or while waiting for the results of gram stains. Septic patients should receive early (i.e., within 1 h) empiric broad-spectrum antibiotics and aggressive fluid resuscitation, as outlined in the Surviving Sepsis 2008 guidelines [11]. Inadequate early broad-spectrum antibiotic coverage is associated with a high mortality rate in septic patients. Thus, systemic antibiotic coverage should be started as soon as the diagnosis of a necrotizing soft tissue infection is entertained. Antibiotic coverage needs to be broad because only a minority of necrotizing soft tissue infections are monomicrobial clostridial infections. Antibiotics should cover gram-positive, gram-negative, and anaerobic microorganisms until definitive culture results are available. There are no randomized studies to direct therapy for necrotizing skin and soft tissue infections, but guidelines exist from retrospective studies. The 2009 Surgical Infection Society Guidelines suggest many single-agent, broad-spectrum regimens, including imipenem-cilastatin, meropenem, ertapenem, piperacillin-tazobactam, ticarcillin-clavulanic acid, and tigecycline [12]. For rapidly progressive infections caused by Streptococcus pyogenes, Clostridium spp., or staphylococci (toxic shock syndrome), the guidelines also advocate the use of a protein synthesis inhibitor, such as clindamycin, erythromycin, or linezolid [12]. This combination therapy may inhibit toxin production, whereas the use of a β-lactam antibiotic alone may lead to a large release of toxin when bacteria lyse, and thus to treatment failure. With the reported rapid rise in community-acquired methicillin-resistant Staphylococcus aureus in skin and soft tissue infections, coverage for this organism should be initiated with either vancomycin or linezolid until it has been ruled out [12]. Not to be discounted, high-dose parenteral penicillin remains a good choice for known Group A streptococcal or clostridial infections [12].
The extent of the necrotizing soft tissue infection is best determined in the operating room. Wide surgical debridement of the infected area should be performed as soon as feasible. One useful maneuver to determine the extent of infection is to test whether the attachments of the skin and subcutaneous tissues to the underlying fascia have lysed, which is recognized when a finger can separate easily the skin/subcutaneous tissue layer from the fascia. It is common for the patient to undergo subsequent surgical debridements, but the initial debridement should be sufficiently extensive to include all grossly necrotic tissue. When myonecrosis is on an extremity, amputation may be the most expeditious form of debridement, as was the case with this patient.
A few adjunctive therapies, including hyperbaric oxygen, gpIIb/IIIa inhibitors, and intravenous immunoglobulin, have been used for necrotizing soft tissue infections, but their efficacy remains unproved. The value of hyperbaric oxygen remains controversial. There are no randomized controlled trials that demonstrate a benefit. Some less rigorous studies suggest a lower mortality rate, greater limb salvage, and decreased antibiotic utilization [13,14], whereas others do not show any benefit [15]. In any case, hyperbaric oxygen should never be used as a primary treatment, only as an adjunct, after surgical debridement. It has been hypothesized that antiplatelet therapy with gpIIb/IIIa inhibitors may be beneficial. Because tissue damage with clostridial myonecrosis is attributable to platelet aggregation and vascular obstruction caused by the phospholipase C activity of the α-toxin [16], treating the patient with anti-platelet inhibitors may reduce vessel and blood flow occlusion and slow the massive tissue destruction. Potentially, this could reduce the amount of debridement necessary and improve limb salvage. Finally, intravenous immunoglobulin (IVIg) has been proposed as an adjunctive therapy for streptococcal and staphylococcal toxic shock syndromes. The immunoglobulin neutralizes the “superantigens” produced by these organisms and thus can reduce the inflammatory cytokine response, which leads to leaky capillaries, shock, and multiple organ dysfunction syndrome [12]. Again, there are no randomized clinical trials to support the efficacy of IVIg or recognize its adverse effects. Thus, all of these adjunctive therapies should be used with caution and only after aggressive fluid resuscitation, broad-spectrum antibiotics, and surgical treatment have been employed.
Clostridium septicum is a common causative agent of clostridial myonecrosis in the setting of malignant disease. Unlike C. perfringens, which is part of the normal bowel flora, C. septicum is an opportunistic pathogen and proliferates in the presence of bowel pathology. An association between C. septicum and colon cancer has been reported frequently [17–20]. Additionally, there are reports describing an association with ovarian cancer or hematologic malignant disease [21–23]. It is theorized that in the setting of colonic mucosal injury, potentially secondary to vascular compromise by the tumor, hematogenous seeding of the organism can occur leading to distant sites of myonecrosis. Metastatic spread also can account for an association of neutropenic enterocolitis (attributable to hematologic cancer) and distant clostridial myonecrosis [19]. A review of 231 cases of C. septicum infection by Hermsen et al. showed that 72% of the infections were associated with cancer (gastrointestinal or hematologic), and the most common location for infection was the skin and soft tissue, which was found in 52% of cases [24]. Operative intervention was the only treatment that improved survival [24]. A notable example is a recent case report that detailed a 61-year old woman who presented with C. septicum necrotizing infection of her right foot and was found to have a colon tumor on workup after her foot wound was stable [25]. These studies highlight the importance of looking for an occult cancer when a patient presents with a rapidly progressive skin and soft tissue infection and no known trauma.
Despite the common association with malignant disease, not all C. septicum necrotizing infections are attributable to cancer. A 2003 report described a 75-year old man with myonecrosis of the right shoulder [6]; the patient had radiation colitis secondary to treatment of prostate cancer six months before. Presumably, this patient's underlying inflammatory colonic pathology led to his necrotizing soft tissue infection, even though he did not have a colon cancer. This case seems similar to the present case. However, in that previous case, there was no description of simultaneous colonic necrosis attributable to the clostridial infection. Ultimately, it is likely that any process, malignant or non-malignant, leading to colonic mucosal damage places the patient at risk for development of myonecrosis secondary to C. septicum.
Conclusions
Necrotizing soft tissue infections caused by Clostridium spp. are particularly virulent mono-microbial varieties of this disease. This case report describes a patient with simultaneous myonecrosis and right colon necrosis attributable to C. septicum. It is likely that this disease arose in the colon in a setting of underlying mucosal pathology caused by ongoing C. difficile colitis and immunosuppression by HIV disease and chronic renal failure.
This case report demonstrates the rapidity with which necrotizing soft tissue infections caused by clostridia can develop. It also highlights the importance of prompt clinical diagnosis, early aggressive sepsis management, immediate surgical debridement, and intensive care in the postoperative period. In addition, this case illustrates some of the pitfalls encountered in making the diagnosis, especially when the patient presents with confounding symptoms. Finally, this report underscores the association of necrotizing soft tissue infections caused by C. septicum with colonic pathology, in this case, C. difficile colitis, and reveals the invasive potential of this organism even when there is no underlying colon tumor.
Footnotes
Acknowledgments
The authors thank Nicole Franco for her help with the graphics.
The authors have no relevant conflicts of interest to disclose.