
Abstract
Abstract
Background:
Extracorporeal membrane oxygenation (ECMO) incorporates surgical techniques as adjuncts in the management of refractory respiratory dysfunction. For many years, its primary application was for support of neonatal infants in cardiorespiratory failure. As the 2009 H1N1 influenza A pandemic developed, more reports came in of severe respiratory dysfunction and even death that seemed to be occurring preferentially in younger adults. Centers with the capability began to use ECMO to salvage these patients.
Results:
The H1N1 virus is a subtype of influenza A. The hemagglutinin receptor binding is similar to that of the seasonal influenza virus, but 2009 H1N1 also binds to α2,3-linked receptors, which are found in the conjunctivae, distal airways, and alveolar pneumocytes. Influenza viruses elude host immune responses through drift and shift in the hemagglutinin (HA) and neuraminidase (NA) proteins. The incubation period ranges from 1–7 days. The majority of patients present with fever and cough, but a broad spectrum of clinical syndromes has been reported, and laboratory testing remains the mainstay of diagnosis. Most patients recover within a week without treatment. The H1N1 virus remains largely sensitive to the NA inhibitors but is resistant to the matrix protein-2 inhibitors. Extracorporeal membrane oxygenation provides continuous pulmonary (and sometimes cardiac) support and minimizes ventilator-induced lung injury. The potential for life-threatening complications is high. In 2009, in the Conventional Ventilation or ECMO for Severe Adult Respiratory Failure (CESAR) randomized trial of ECMO, the overall survival rate was 63% in the ECMO group compared with 47% in the control group (p = 0.03). Similar studies have been reported from Australia and New Zealand, Canada, and France.
Conclusions:
Supportive management is continued along with ECMO. Antiviral drugs and antimicrobial agents should be given as appropriate, as should nutritional support. Volume management should be used. Ventilator settings should be reduced as ECMO support allows, with a goal of reducing airway pressures, ventilator rate, and F
In February 2009, a novel swine-associated (H1N1) influenza virus infection was reported to the U.S. Centers for Disease Control and Prevention (CDC). The child, who was in contact with pigs, recovered uneventfully, and the case was barely mentioned in the April 17, 2009 edition of the Morbidity and Mortality Weekly Report [1]. However, note was made the next week of two cases of influenza A (H1N1) virus infection [2]; both were in children who had no history of contact with pigs. The two viruses were genetically similar and substantially different from prior H1N1 strains. The lack of contact with pigs and the novelty of the strain raised concern about human-to-human transmission of a virus to which there was no large-scale immunity. By the next week, 64 confirmed cases were reported by the CDC [3], and the World Health Organization (WHO) described 26 confirmed cases from Mexico. On April 29, 2009, the WHO upgraded its level of pandemic alert from phase 4 to phase 5, indicating human-to-human spread in at least two countries in one region [4]. By May 5, Mexico had identified almost 12,000 suspected cases with 42 deaths [4]. As the pandemic progressed, more reports came in of severe respiratory failure and even death that seemed to be occurring preferentially in younger adults. Centers with the capability began to use ECMO to salvage these patients. This review discusses the increased use of ECMO in the context of the 2009 H1N1 influenza A pandemic.
H1N1 Virus
The virus at the root of the pandemic, H1N1, is a subtype of influenza A. Influenza A, along with B and C, are in the Orthomyxoviridae family. Influenza A viruses have eight single strands of negative-sense RNA that code for 11 proteins [5]. Influenza A subtyping is based on the antigenicity of the two major cell-surface glycoproteins: hemagglutinin (HA) and neuraminidase (NA) (Fig. 1). There are 16 H antigens and 9 N antigens. The HA protein promotes binding of the virus to receptors on the host cell and subsequent endosomal fusion. Viral release from host cells is facilitated by the NA protein.

Structural diagram of influenza A virus. H = hemagglutinin; M = matrix; N = neuraminidase; NP = nucleoprotein; NS = nonstructural; PA = acidic polymerase; PB = basic polymase. Reprinted with permission from Kaiser J. A one-size-fits-all flu vaccine. Science 2006;312:380–382.
The hemagglutinin receptor binding of H1N1 is similar to that of seasonal influenza in that H1N1 binds to α2,6-linked cellular receptors. However, the 2009 strain of H1N1 also binds to α2,3-linked receptors [6], which are found in the conjunctivae, distal airways, and alveolar pneumocytes. It is this binding that is believed to account in part for H1N1's higher virulence and ability to infect the lower respiratory tract [7]. The 2009 H1N1 virus also shows greater replication in bronchial tissue than does seasonal influenza [8], which may also contribute to its ability to cause severe viral pneumonitis. Animal studies show that inoculation of the respiratory tract can result in viral invasion of the gastrointestinal (GI) tract mucosa [9].
Drift vs. Shift
Influenza viruses elude host immune responses through drift and shift in the HA and NA proteins [10]. “Drift” refers to the frequent minor changes in the antigens. These drifts are associated with annual changes in seasonal influenza. “Shift” refers to the introduction of an influenza A virus subtype to which the population has no immunity. Shifts are believed to be facilitated by the virus' ability to infect a wide variety of hosts [10]. Antigenic shifts in the HA subtypes are associated with pandemics, three of which occurred in the 20th Century [11]. Prior to 1957, H1N1 viruses were the dominant influenza A viruses, until replacement by the H2N2 “Asian” strain. These prior H1N1 strains may have resulted in cross-protective antibodies against 2009 H1N1 for those alive prior to 1957 [12,13].
Illness
Clinical manifestations
The incubation period of the H1N1 virus differs widely [14–18], but in general ranges from 1–7 days, with most symptomatic cases occurring within 1–5 days after exposure. The majority of patients present with fever and cough [19,20], but a broad spectrum of clinical syndromes has been reported, from asymptomatic illness to fulminant viral pneumonia [14]. Gastrointestinal symptoms are more common with 2009 H1N1 than with seasonal influenza [21,22], which may reflect the virus' ability to attack the mucosa of the GI tract [9].
Because of the wide range and non-specificity of the symptoms, laboratory testing remains the mainstay of diagnosis of H1N1. The usual method is by nasopharyngeal swab or aspirate taken early after the onset of symptoms or bronchoscopic aspirates in those requiring intubation. The most accurate test is one that detects viral RNA by conventional or real-time reverse transcriptase polymerase chain reaction (RT-PCR) [23]. Multiple studies demonstrate fewer false-negative results from bronchoscopic specimens [22–25], so these should be used preferentially when available. A study by Blyth et al. showed that almost 20% of patients with a positive bronchoscopic aspirate had a negative result from an upper respiratory sample [25]. Consequently, a single negative upper respiratory sample does not rule out H1N1, and treatment should not be stopped on this basis. Falsely negative lower respiratory samples have also been reported, so repeat bronchoscopic sampling in the setting of clinical suspicion is also appropriate with these patients [14].
Treatment
Most patients will recover within a week even without treatment. Patients with severe illness (Table 1), who deteriorate, or who have risk factors for complicated illness (Table 2) should be treated [26]. The virus remains largely sensitive to the NA inhibitors oseltamivir and zanamivir. However, it is resistant to the matrix protein-2 inhibitors amantadine and rimantadine [21,27]. Clinicians should consider using higher doses of oseltamivir for a longer period for patients who have severe disease or who are deteriorating [28,29].
From Reference 26.
Adapted from Reference 14.
There are reports of isolates of oseltamivir-resistant H1N1, especially in patients with immunosuppression who received prolonged courses [30,31] or who failed post-exposure prophylaxis with oseltamivir [32]. These patients may still recover without complications, but if they require treatment, zanamivir should be used [33]. There have been no reports of zanamivir resistance in 2009 H1N1 influenza A.
Attack rates
The attack rate is the cumulative incidence of infection in a population during an epidemic. Reported attack rates for H1N1 have ranged from 100 to 10,000 per 100,000 population [19,34,35]. However, in one residential school, the attack rate for influenza-like illness was 71% and for confirmed H1N1 was 42% [36], showing the dramatic impact that close living quarters can have on transmission of the virus. Estimated rates of hospitalization for those who contract the virus range from 0.3% to 9%, with case fatality rates ranging from 0.02% to 0.5% (Fig. 2) [21,34,37].
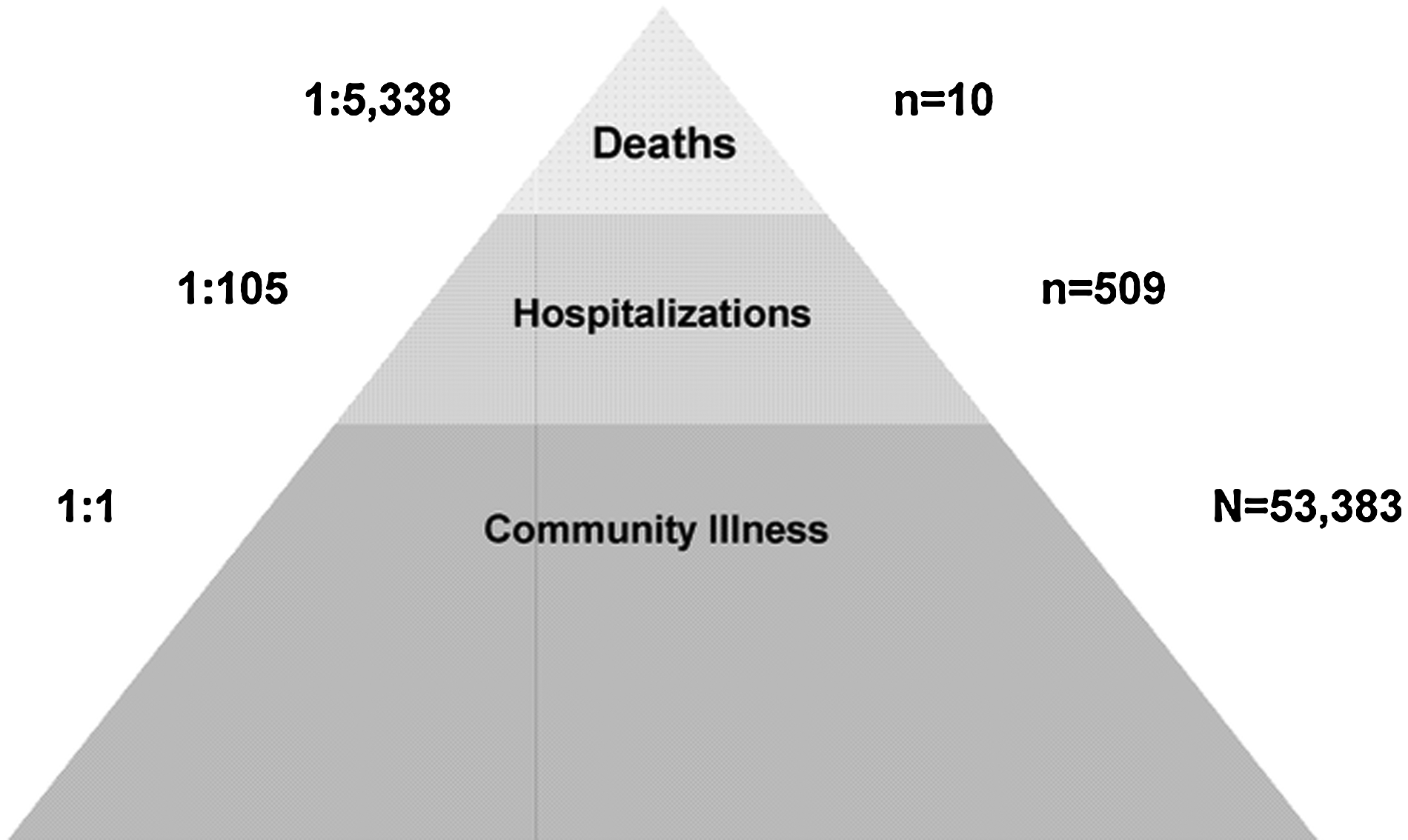
Estimated pandemic disease burden. Reprinted from Dawood FS, Hope KG, Durrheim DN, et al. Estimating the disease burden of pandemic (H1N1) 2009 virus infection in Hunter New England, Northern New South Wales, Australia, 2009. PLoS One 2010;5:e9880.
Risk factors
Risk factors for contracting the disease appear to be younger age, pregnancy, contact with someone with H1N1 infection or influenza-like illness, and belonging to a disadvantaged group [14,19,38]. Pregnant women and obese individuals are over-represented in the population of patients infected with H1N1 who require hospitalization or who succumb to the disease [39–45]. A number of other patient characteristics also are associated with severe disease or complications (Table 2) [28]. A subset of patients become critically ill and develop acute respiratory distress syndrome (ARDS) characterized by severe hypoxemia. In cases of respiratory failure refractory to conventional treatment, high ventilator settings, alternative ventilator modes (such as bilevel ventilation and high-frequency oscillatory ventilation), and other rescue modalities, such as prone positioning, nitric oxide, or ECMO may be used.
Extracorporeal Membrane Oxygenation
Methods of ECMO support
Components of the ECMO circuit are the pump, the oxygenator, and vascular access to the patient's circulatory system. There are two forms of ECMO: Venovenous (VV) and venoarterial (VA). Venovenous ECMO provides only oxygenation, whereas VA ECMO provides circulatory support as well.
In VV ECMO, blood drains out of a large-bore venous cannula, passes through the membrane oxygenator for gas exchange, then is returned to the venous system via a cannula placed close to the right atrium. A multiple cannula system such as this usually drains from one or two cannulas in the femoral veins and returns blood to the vena cava via a cannula in the right internal jugular vein. A dual-lumen cannula is also available. Insertion is into the right internal jugular vein, and the cannula drains from both the superior and the inferior vena cava. The blood is returned to a port that is aimed at the right atrium under ultrasound guidance.
Venoarterial ECMO also drains from the femoral vein but usually returns blood to the femoral artery. The action of the pump in the circuit provides cardiac support. Compared with VV, VA ECMO has more potential complications, including ischemia from arterial cannulation. “North–South syndrome” occurs when some left ventricle function is preserved. The ventricular pumping action directs the relatively deoxygenated blood that has passed through the native lung into the head and upper extremities while preventing retrograde flow into the proximal aorta of well-oxygenated blood from the ECMO circuit. Therefore, the brain, heart, and upper extremities may be hypoxemic, whereas the lower extremities are well oxygenated.
Characteristics of procedure
Extracorporeal membrane oxygenation provides continuous pulmonary (and sometimes cardiac) support on a longer-term basis than the cardiopulmonary bypass machines used in the operating room. This period can last from days to weeks and allows minimization of ventilator-induced lung injury while the lungs heal. Extracorporeal membrane oxygenation is a complex treatment that requires a dedicated team that includes surgical support or supervision. The potential for life-threatening complications is high; therefore, its use is reserved for patients whose hypoxia confers a substantial risk of death.
The efficacy of ECMO for neonatal [46–48] and pediatric [49,50] patients has been well established, with an overall survival rate to discharge of 64% in a large voluntary database (Extracorporeal Membrane Oxygenation Organization; unpublished data]. However, initial trials of ECMO in adults [51,52] had disappointing results, and adult ECMO fell by the wayside except in a few centers. However, the publication of the Conventional Ventilation or ECMO for Severe Adult Respiratory Failure (CESAR) trial [53] and concurrent reports of the use of ECMO for the sickest patients during the 2009 H1N1 pandemic re-ignited interest in adult ECMO for respiratory failure.
History
Heart–lung machines were used in surgery many years before ECMO became practical. The problem was that the oxygenators of the time involved direct contact of air with the bloodstream, and resulting cell damage limited use to 4 h or less. Longer use required the development of a membrane oxygenator [54]. Once that device was available, ECMO was successful in 1971 on an adult trauma patient in California who developed ARDS [55]. However, a multicenter randomized controlled trial in 1979 showed no benefit to ECMO vs. conventional ventilation for adult ARDS [51]. Problems identified with the study included selection bias that excluded both the least ill and the sickest patients; failure to use “rest settings” on the ventilator for some patients in the ECMO arm; absence of prior ECMO experience in some centers; and a biased patient pool attributable to the influenza epidemic of 1976 [56].
Two subsequent studies looked at extracorporeal CO2 removal only. In 1986, Gattinoni et al. reported a series of 43 patients who had low-flow extracorporeal CO2 removal combined with low-frequency “rest ventilation” [57]. Survival in this cohort was 48.8%, which was impressive for this era. However, in 1994, Morris et al. reported a randomized controlled trial of CO2 removal compared with inverse ratio ventilation, which was popular at the time [52]. This was a small trial (n = 40), and no difference was found in survival (42% for the control group and 33% for the extracorporeal group). This study has been criticized for its small size, failure to achieve lung rest in the extracorporeal group, and the high blood loss in the extracorporeal group [58]. Both studies have been criticized for focusing on CO2 removal, as hypercarbia generally is well-tolerated in ARDS.
With these studies, interest in ECMO for respiratory disease in adults waned in the 1980s and 1990s, whereas research continued in pediatric and cardiac populations. In contrast to the original studies, newer data reflect advances in intensive care unit (ICU) support, ventilator management strategies, non-ventilatory ARDS care, and ECMO technology that have occurred over the past 20 years.
A retrospective review of the Extracorporeal Life Support Organization (ELSO) data from 1986–2006 examined the results for 1,473 adult patients who received ECMO for severe respiratory dysfunction [59]. The overall survival rate to discharge was 50%; however, patient treatment was not randomized, and there was no control group. The study authors found that increasing age, pre-ECMO arterial blood pH < 7.18, longer duration of pre-ECMO mechanical ventilation, lower patient weight, Asian background, and complications of ECMO were associated with a poorer survival rate. Venovenous ECMO was associated with better survival than VA ECMO. As noted, this technique provides cardiac support in addition to pulmonary support, so differences in underlying disease in the patients placed on VA and those given VV ECMO may account for this finding. Acute respiratory dysfunction and asthma conferred a survival benefit compared with patients whose diagnosis was listed as ARDS. Approximately 9% of patients sustained radiographic evidence of cerebral infarction, hemorrhage, or brain death.
In 2009, the results of the CESAR trial were published [53]. This was a multicenter, randomized, controlled trial conducted in the United Kingdom from 2001 through 2006. Patients with severe (Murray score ≥3 (Table 3) or pH < 7.20), but potentially reversible, ARDS were randomized to either conventional care at one of the participating 68 tertiary care centers or transfer to a single center that is the sole provider of adult ECMO in the U.K. Whereas patients at the ECMO center were treated according to a strict protocol, the “pragmatic” nature of the trial meant that care at the other 68 centers was not standardized. Patients were excluded if they had been on high ventilatory pressures or high inspired oxygen concentrations for more than seven days prior to trial entry, had signs of intracranial bleeding, or had contraindications to the heparinization necessary for ECMO or continuation of treatment.
PEEP, positive end-expiratory pressure.
From Murray JF, Matthay MA, Luce JM, Flick MR. An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis 1988;138:720–723.
Of the 90 patients randomized to the ECMO arm, 75% ultimately received ECMO. Of these, 63% survived. Of the patients who did not receive ECMO, three died prior to transfer, two died during transfer, and one developed a contraindication to heparin. The other 16 patients improved with conventional management at the ECMO center, and 82% of these survived to hospital discharge. The overall survival rate was 63% in the ECMO group compared with 50% in the control group. This difference approached statistical significance (p = 0.07). When the endpoint of death or severe disability was used, ECMO conferred a benefit (63% vs. 47%; relative risk [RR], 0.69; 95% confidence interval [CI] 0.05–0.97). The mean time of ventilation prior to entry into the study was similar: 35 h for the ECMO arm and 37 h for the control arm. Mean Murray scores were high at 3.5 and 3.4, respectively. Median hospital days and critical care days were longer in the ECMO arm. Economic analysis showed that patients referred to the ECMO center gained 0.03 quality-adjusted life-years (QALYs) at six-month follow up at a cost of about $32,000 per QALY.
The study authors acknowledge in their discussion that the benefit may come from referral to a center with extensive experience treating ARDS rather than from ECMO itself. However, three quarters of the patients referred to the center ultimately required ECMO despite presumably optimal management. This suggests that ECMO may still have a role in severe ARDS not responsive to optimal management.
Extracorporeal membrane oxygenation and the 2009 H1N1 Influenza A pandemic
At the same time the CESAR trial was published, the 2009 H1N1 influenza pandemic was raging. Two months after CESAR's publication, 15 centers that provide ECMO in Australia and New Zealand published an observational study of the use of the technique for patients with H1N1-associated pulmonary failure [60]. Of the patients with 2009 H1N1 in the 15 centers who required mechanical ventilation, 68 (34%) were placed on ECMO. Only the 61 patients on ECMO who had confirmed influenza A respiratory failure were included in the analysis. The most common co-morbidities in the group requiring ECMO were obesity (body mass index >30 kg/m2) (50%), asthma (28%), and diabetes (15%). However, the rates of these co-morbidities were not statistically different from those in the group that did not receive ECMO. The overall incidence of pregnant patients was 15%. The ECMO group had a lower median age (36 years vs. 44 years), were more likely to have required vasopressor therapy on admission to the ICU, and had longer durations of mechanical ventilation and ICU stays, but not hospital stays. The mortality rate in the ECMO group was an impressively low 21% (all deaths occurred in the ICU), with an ICU mortality rate of 9% in the comparison group and an overall mortality rate of 13%. The ICU death rate was significantly lower in the comparison group, but the overall mortality rate approached statistical significance difference (p = 0.06). Unlike the U.K. study, the investigators in Australia and New Zealand had the capacity to place patients on ECMO at a referring hospital and transport patients on ECMO. More than one–half (38) of the 68 ECMO patients were placed on ECMO for transport.
Because the 15 centers are the only ones in Australia and New Zealand that provide ECMO, the authors were able to calculate a population-based ECMO use rate of 2.6 per million population during this time. By comparison, the previous influenza season had resulted in only four patients requiring ECMO, for a rate of 0.15/1,000,000. Clearly, ECMO played a more important significant role in the treatment of pandemic H1N1 influenza than in seasonal influenza.
Canadian researchers reported on the experience of 34 ICUs across the country [61]. The centers admitted 168 patients with confirmed H1N1 influenza infection. Of these, 6 (4%) required ECMO. These patients were younger (22 vs. 32 years of age) and were more likely to have received therapies such as high-frequency ventilation (three patients), inhaled nitric oxide (six patients), prone ventilation (two patients), and neuromuscular blockade (six patients). They were less likely to have received corticosteroids (33% vs. 51%). Two patients were placed on VA ECMO, the rest on VV. The mortality rate was 33%, compared with 14% in the non-ECMO group. Both patients died while on ECMO. As in the CESAR trial, patients who survived to decannulation also survived to hospital discharge.
More recently, researchers in Marseille, France presented their single-center experience [62] with 22 institutional criteria for ECMO. One patient died before ECMO could be instituted. Six patients were placed on VV ECMO and the other three on VA ECMO. Six patients required cannulation at the referring facility and transport on ECMO. Five patients (56%) died in both the ECMO and non-ECMO ARDS groups. Other investigators have reported single cases and case series of their experiences with ECMO for H1N1 severe ARDS [63–71].
Consideration for referral to an ECMO center
If ECMO is to be used for an adult with severe ARDS as a result of H1N1, referral to an ECMO center should be considered if the patient is not responding to conventional management and has a mortality risk estimated to exceed 50%. Adult respiratory distress syndrome in patients with H1N1 infection can progress rapidly, and transportation on ECMO is available in only a few places in the world. Therefore, a balance must be struck between referring too early and overwhelming the ECMO center with patients who will not require ECMO vs. referring too late, when the patient is too sick to survive transport. As the pandemic wanes, the first consideration becomes less important than the second. Referral criteria derived from the CESAR trial [53] are patients 65 years of age or younger and a Murray score of ≥3 (see Table 3) or uncompensated hypercarbia with pH < 7.20. Contraindications to ECMO include irreversible pulmonary disease, terminal disease, contraindication to full anticoagulation, and refusal to receive blood products. Individual ECMO centers may have additional criteria such as a maximum acceptable body mass index because of inability to achieve sufficient oxygen delivery for the body size. Relative contraindications to ECMO (because of historically poor survival rates) include mechanical ventilation for more than 10 days or high-pressure mechanical ventilation for more than seven days. Early telephone contact with the ECMO center can help identify appropriate candidates for transfer.
Management on ECMO
Supportive management is continued after initiation of ECMO. Antiviral drugs [72] and antimicrobial agents should be instituted or continued as appropriate. Nutritional support, preferably by enteral means, should be continued. Volume management, which may require hemofiltration, should be used to achieve the patient's appropriate dry weight. Ventilator settings should be reduced as ECMO support allows, with a goal of reducing airway pressures, ventilator rate, and percentage of inspired oxygen (FiO2). Oxymetric measurement of the venous limb of the circuit can be used to monitor the adequacy of support. Systemic anticoagulation, usually with heparin, is administered to prevent circuit clotting. Heparinization is monitored by bedside measurement of activated clotting time or partial thromboplastin time. Continuous renal replacement therapy commonly is needed. It is preferable to run this via separate venous access, but some circuits can accommodate a filter if separate access is impossible.
Complications
Complications of ECMO are common and prevent its wider use for less moribund patients. Bleeding is the most common complication and can result in death, especially if it occurs intracranially. Avoidance of bleeding is of primary importance. Invasive procedures should be limited, bronchoscopy performed atraumatically, and cautery used extensively for any procedure that must be performed. If bleeding does occur, it can be managed by decreasing or temporarily stopping heparin (with the attendant risks) and infusing platelets and clotting factors. Pulmonary hemorrhage may necessitate frequent bronchoscopy to clear the airways. Intracerebral hemorrhage or infarction occurs in 10–15% of ARDS patients on ECMO [49]. In Australia and New Zealand, 43% of the deaths on ECMO were related to intracranial hemorrhage [60]. Because of the critical condition of these patients and the inability to stop anticoagulation for any significant period of time, intracranial hemorrhage usually is fatal.
During cannulation, fatal vascular perforation can occur because of the size and stiffness of the cannulas. For this reason, if a surgeon is not personally performing the cannulation, one with vascular repair capabilities should be at hand. Hemolysis generally does not occur with modern ECMO circuits unless there is a problem in the circuit or the patient. The plasma free hemoglobin concentration should be monitored daily. Values > 10 mg/dL should prompt an investigation into the cause and correction thereof. Thromboembolic disease has been reported after decannulation after ECMO for H1N1-associated respiratory failure [71]. For this reason, consideration should be given to continuation of full anticoagulation after cannula removal. If the patient had a femoral venous cannula in place, consideration should be given to placement of an inferior vena cava filter at the time of cannula removal.
The 2009 H1N1 influenza A pandemic has produced a surprising number of relatively young patients with severe respiratory dysfunction. Because these patients are young, seldom have life-limiting co-morbidities, and have a reversible disease, they can be considered for salvage therapy with ECMO when conventional therapies fail. Because of the intensive knowledge, personnel, and equipment needs, an ECMO program is not to be undertaken lightly.
Author Disclosure Statement
No conflicting financial interests exist.