
Abstract
Abstract
Background:
Abscesses are one of many complications of diverticulitis and can be found intra-abdominally or in the pelvis.
Methods:
Case report and review of the pertinent English-language literature.
Results:
We describe an unusual presentation of a diverticular abscess, tracking down the inguinal canal and causing acute scrotum possibly secondary to a hernia.
Conclusion:
A deviation from the usual clinical presentation of diverticulitis should prompt the physician to obtain further radiologic evaluation. Computed tomography scanning is recommended, especially when an abscess is suspected.
Case Report
A 49-year-old man presented in the Emergency Department (ED) with a chief complaint of an intense crampy, left lower-quadrant pain that had started three days earlier. The patient reported fever, diarrhea, and worsening of pain the day before arrival. He denied bloody bowel movements, nausea, or vomiting. The medical history included three diverticulitis attacks treated at other institutions, morbid obesity, and hypertension. Physical examination revealed no peritonitis and a reducible left inguinal hernia. Computed tomography (CT) scanning performed on arrival in the ED showed sigmoid diverticulitis with phlegmon and no free air or abscess (Hinchey I). The most recent colonoscopy, performed six months earlier, revealed diverticulosis and no malignancy.
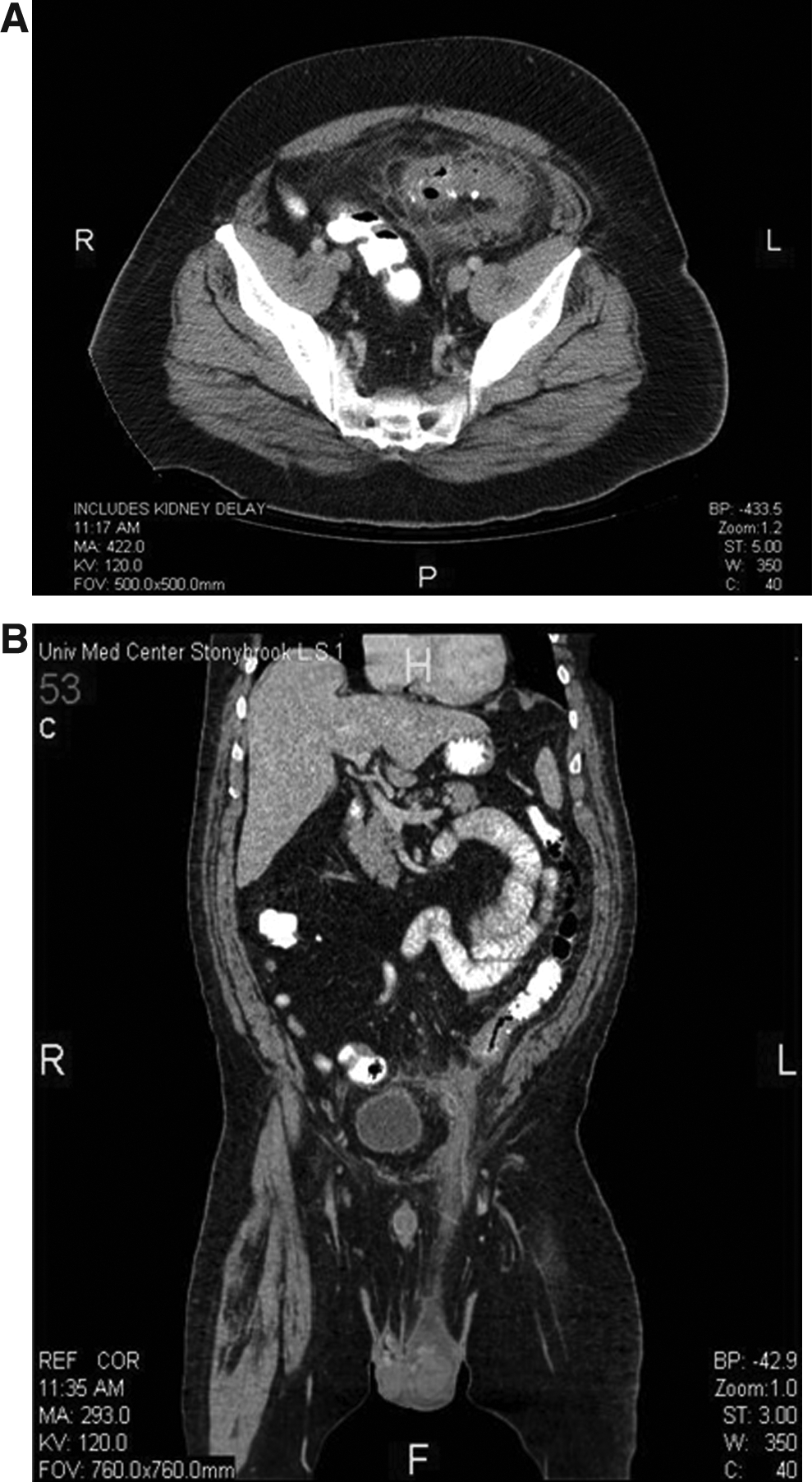
The patient was admitted and started on intravenous antibiotics: Piperacillin-tazobactam, metronidazole, and ciprofloxacin. On hospital day 3, the patient complained of left scrotal pain. On physical examination, the scrotum was swollen, erythematous, and tender. Repeat CT scan revealed interval abdominal worsening, with an abscess (3.2×4.7×2.5 cm) draining through the inguinal canal into the scrotum (Hinchey II). Figure 1A shows a phlegmon from the sigmoid colon diverticulitis. Figure 1B shows extension of inflammatory changes of the sigmoid colon with an abscess extending down the left inguinal canal into the scrotal sac.
The patient underwent surgery the same day. Findings at laparotomy included an infected and indurated sigmoid colon with transmural involvement, covered by extensive pseudomembranes and adherent to the left pelvic side wall with purulent exudate. A sigmoid resection with primary anastomosis and loop ileostomy was performed. A left transverse scrotal incision was made, continuing to the parietal tunica vaginalis and proximally along the spermatic cord. Extensive loculated collections of purulent material were lysed digitally and drained. Copious irrigation with saline, peroxide, and bacitracin solution followed. The incision was packed and left open with scrotal support. Cultures revealed Enterococcus raffinosus, Bacteroides fragilis, and Eggerthella lenta. Postoperatively, the patient recovered well, tolerating a low-residue diet. He was discharged home on postoperative day six.
Discussion
A large population-based study found a 7.4% incidence rate of abscess in patients with diverticulitis [1]. Abscesses can be found intra-abdominally, in the pelvis, and in various unexpected locations. Several unusual manifestations of perforated diverticulitis have been reported, such as spread through the abdominal wall and multiple abscesses in the thigh [2]. Other authors have described manifestations in the buttock, hip, and joints [3]. This case is an addition to the collection of unusual presentations of perforated diverticulitis—abscess tracking down the inguinal canal causing acute scrotum. It is important to recognize that in this case, the inguinal hernia discovered during physical examination predisposed the patient's abscess to track along the inguinal canal. Without the hernia, the patient's abscess might have remained confined to the abdominal cavity.
This unusual clinical presentation of diverticulitis rendered the diagnosis difficult. The acute scrotum suggested several possible diagnoses, such as incarcerated inguinal hernia, testicular torsion, and epididymitis. By clinical presentation alone, it would have been difficult to identify an inguinal abscess as the cause of the acute scrotum. A deviation from the usual clinical presentation in diverticulitis should prompt the physician to obtain further radiologic evaluation. Computed tomography scanning is recommended, especially when an abscess is suspected [4], because of its high sensitivity and specificity [5]. It was only after the repeat CT scan was performed that a correct diagnosis was obtained in this case leading to definitive surgical source control [6] and appropriate antibiotic therapy [7].
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.