
Abstract
Abstract
Background:
Hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) is associated with morbid, invasive infections and has been implicated in nearly every type of nosocomial infection. Our aim was to identify the risk factors for patient conversion from MRSA negativity pre-operatively to MRSA positivity post-operatively.
Methods:
We retrospectively reviewed all patients at the Veterans Affairs–Boston Health Care System who underwent clean or clean-contaminated surgical procedures during the years 2008 and 2009 and had documented pre-operative nasal polymerase chain reaction (PCR) testing for MRSA. We abstracted post-operative MRSA microbiologic testing results, MRSA infections, surgical site infections (SSIs), surgical prophylaxis data, and SSI risk index, as calculated using the Veterans Affairs Surgical Quality Improvement Project (VASQIP) database variables. All patients who had a negative nasal MRSA PCR result in the 31-day pre-operative period and did not have any positive MRSA clinical swab or culture in the 1-year pre-operative period were defined as MRSA-negative. These patients were classified as converters to MRSA positivity if they had at least one documented positive nasal MRSA PCR swab, culture, nosocomial infection, or SSI within 31 days post-operatively.
Results:
Among 4,238 eligible patients, 3,890 (92%) qualified as MRSA-negative pre-operatively. A total of 1,432 (37%) of these patients were assessed in the VASQIP database, of whom 34 (2%) converted to MRSA positivity post-operatively. On multivariable logistic regression analysis of the VASQIP sample, age (odds ratio [OR] 1.049; 95% confidence interval [CI] 1.016, 1.083), SSI risk index (OR 2.863; 95% CI 1.251–6.554), and vancomycin prophylaxis alone or in combination (OR 3.223; 95% CI 1.174–8.845) were significantly associated with conversion to MRSA positivity.
Conclusion:
In pre-operatively MRSA-negative patients, age, SSI risk index, and vancomycin prophylaxis were significant factors for conversion to MRSA positivity post-operatively. Alternatives to vancomycin prophylaxis in non-colonized patients and optimization of patients' SSI risk factors should be considered before elective surgery.
The Veterans Affairs (VA) Healthcare System has led an effort to implement universal MRSA surveillance and a bundled approach to MRSA prevention [7]. However, even with high compliance with infection prevention strategies, acquisition of MRSA in the hospital still occurs. The problem is compounded by evidence that surgical site and other nosocomial infections with MRSA carry greater morbidity, a higher mortality rate, and greater hospital cost than infections with methicillin-sensitive S. aureus (MSSA) [5,8–10].
A better understanding of the mechanisms of spread of MRSA and the implications of in-patient care processes for post-operative MRSA acquisition is essential to MRSA infection control and containment strategies. Factors such as length of hospital stay, intensity and processes of care, surgery, invasive procedures, patient risk factors, and antibiotic use all have been implicated in nosocomial MRSA acquisition [11–15]. It was our goal to identify the factors involved in the conversion of patients from MRSA-negative status pre-operatively to MRSA colonization or infection post-operatively using local data from the VA–Boston Healthcare System (VABHCS) MRSA Prevention Program.
Patients and Methods
Study population and data derivation
The study population was derived from a previous investigation of the association between pre-operative nasal MRSA colonization and post-operative MRSA cultures and infections [16]. In brief, the larger study cohort consisted of all patients who underwent clean or clean-contaminated surgery at the VA–Boston Healthcare System (VABHCS) between January 1, 2008, and December 31, 2009, and also had a documented MRSA nasal polymerase chain reaction (PCR)-based screening result (GeneXpert; Cepheid, Sunnyvale, CA) within 31 days pre-operatively. Dental, ophthalmologic, and all contaminated procedures were excluded. We included in the current study a subset of the larger cohort comprising patients who were negative for MRSA pre-operatively, based on a negative MRSA nasal swab in the 31-day pre-operative period and no MRSA-positive swabs or culture results in the 1-year pre-operative period. Patients who met these criteria were considered at risk for conversion to MRSA positivity post-operatively and made up our study population. Approval for the study was obtained from the VA Boston Institutional Review Board.
Our study sample was identified by merging the surgery and infection control databases available within the VABHCS. The medical records of the patients were then abstracted using the Veterans Health Information Systems and Technology Architecture (VistA) to obtain additional variables such as patient age at the time of surgery, patient sex, MRSA culture results within one year pre-operatively and 31 days post-operatively, antibiotic prophylaxis data, type of skin preparation, and type of surgery. A previously validated variable [17], the SSI risk index, was extracted from a subset of the sample population, which consisted of patients selected randomly for inclusion in the VA National Surgical Quality Improvement Program (VASQIP) database. Variables comprising the SSI risk index are collected prospectively by a dedicated nurse reviewer as part of the VASQIP and are age, presence of diabetes mellitus or dyspnea, use of corticosteroids, alcoholism, smoking, recent radiotherapy, American Society of Anesthesiologists (ASA) class, albumin, total bilirubin, priority of the surgery, complexity of the surgery, type of operation according to Current Procedural Terminology (CPT) code, and incision classification. Surgical procedures were classified into tier 1 and tier 2 types according to the likelihood that the surgery would involve prosthesis implantation and be the target of a decolonization program; tier 1 operations, including cardiac, thoracic, vascular, and orthopedic procedures, were more likely to be targeted for active decolonization. Tier 2 operations included general, genito-urinary, neurosurgery, otorhinolaryngology, plastic, podiatry, and ambulatory orthopedics procedures.
Conversion to MRSA positivity was defined as at least one documented positive MRSA result from a nasal surveillance swab, a culture, a standard National Healthcare Safety Network (NHSN)-defined infection, or an SSI within 31 post-operative days. The NHSN infection criteria are based on the U.S. Centers for Disease Control and Prevention definitions of healthcare-associated infections. The MRSA cultures were defined as those taken from any body site for clinical purposes (not surveillance).
Statistical analyses
In the VASQIP patient sample, bivariable analysis was performed to compare the SSI risk index variables between converters and non-converters to MRSA positivity. The student t-test was conducted for comparing the means of continuous variables, and the chi-square or Fisher exact test was performed for comparing the proportions of categorical variables.
A multivariable logistic regression analysis modeling the odds of conversion to MRSA positivity was conducted for VASQIP-assessed MRSA-negative patients. The variables tested were age, SSI risk index, time between MRSA screening and surgery, vancomycin prophylaxis, chlorhexidine–alcohol skin preparation, and surgery tier. For sensitivity analysis, a multivariable regression analysis modeling the odds of conversion to MRSA positivity was conducted for the entire sample of MRSA-screened surgical patients (including non-VASQIP patients). The SSI risk index variable was excluded, as it was not assessed in non-VASQIP patients. Confidence intervals (CIs) of 95% were used in the regression analyses, and a p value of <0.05 was considered significant.
A survival analysis was performed for time to conversion to an MRSA-positive swab and to an MRSA-positive culture for both the total patient sample and the VASQIP subset. All analyses were conducted using SAS version 9.1 (SAS Institute, Inc., Cary, NC).
Results
In the two-year study period, a total of 4,238 unique patients underwent an eligible surgical procedure and were swabbed nasally within 31 days pre-operatively (Fig. 1). The swabs were collected a mean of five days, a median of one day, and a range of 0–31 days prior to surgery. The pre-operative swab was negative for MRSA in 3,956 of these patients (93%). Any MRSA-positive swab or culture within the one-year pre-operative timeframe led to further exclusion of 66 patients, resulting in a final sample of 3,890 patients (92%), who constituted the study population at risk for conversion. Post-operative conversion to MRSA positivity occurred in 69 of these patients (2%). Of the 3,890 patients, 1,432 (37%) were assessed in the VASQIP database, of whom 34 (2%) converted to MRSA positivity post-operatively (Fig. 1).
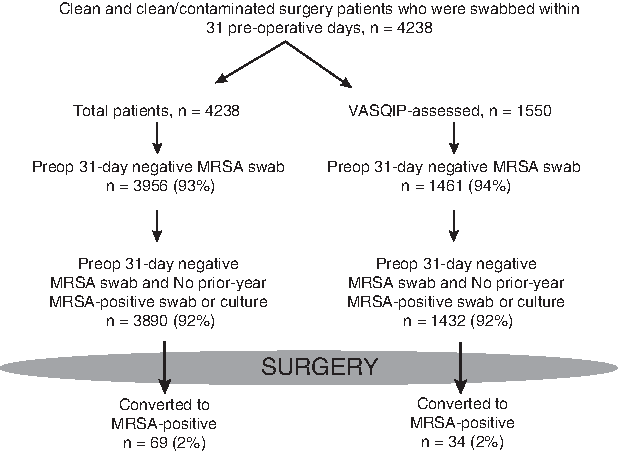
Flow diagram of patients who converted to methicillin-resistant Staphylococcus aureus positivity post-operatively.
Demographic and SSI risk index variables for the VASQIP-assessed patients are displayed in Table 1. A significantly higher proportion of converting patients had an SSI risk index >8 points (p=0.0017), were older (p=0.0014), were in ASA class 3–5 (p=0.0248), had a serum albumin concentration ≤3.5 g/dL (p<0.001), and underwent emergency surgery (p=0.0122) than those who remained MRSA negative post-operatively. Differences between converters and non-converters were non-significant for sex, diabetes mellitus, dyspnea, steroid intake, significant alcohol consumption, smoking, radiotherapy, bilirubin concentration >1 mg/dL, all surgical procedure types by CPT code, complexity of surgery, and incision status.
ASA=American Society of Anesthesiologists; NS=not significant; RVU=relative value unit; VASQIP=Veterans Affairs Surgical Quality Improvement Program.
On multivariable analysis modeling, VASQIP patients were significantly more likely to convert to MRSA positivity when older, having a high SSI risk index, and after receiving vancomycin prophylaxis alone or in combination (Table 2),. Chlorhexidine–alcohol skin preparation, number of days elapsed from MRSA swabbing to surgery, and surgery tier 1 vs. 2 were not significantly associated with conversion to MRSA positivity in the VASQIP cohort of patients.
NA=not available; SD=standard deviation; SSI=surgical site infection; VASQIP=Veterans Affairs Surgical Quality Improvement Program.
A sensitivity analysis was performed by repeating the multivariable analysis on all MRSA swab-negative patients (including non-VASQIP patients) (Table 2). In the absence of the SSI risk factor variable, surgery tier 1 became significantly associated with conversion. Age and vancomycin prophylaxis continued to be significant risk factors. Chlorhexidine–alcohol skin preparation and number of days elapsed from MRSA swabbing to surgery remained non-significant.
Table 3 demonstrates the numbers and percentages of patients who converted to MRSA positivity by nasal swab, culture, NHSN infection, or SSI. The majority of the patients converted to a MRSA-positive nasal swab result in both the total (89.9%) and VASQIP (88.2%) patient samples. Conversion to a positive culture occurred in a lower percentage of patients in the total (31.9%) and VASQIP (29.4%) groups; NHSN infections and SSI occurred in even lower percentages of patients in both groups. The four conversion categories are not mutually exclusive, and all patients with an NHSN infection or SSI were found to be so by a positive culture.
NHSN=National Healthcare Safety Network; VASQIP=Veterans Affairs Surgical Quality Improvement Program.
The survival analysis for time to conversion to MRSA positivity, plotted in Figures 2 and 3, showed few conversion events. Nasal swab conversions occurred gradually for both the total patient population (Fig. 2A) and the VASQIP subset (Fig. 3A); in contrast, a clustering of conversions to a positive culture was observed after day 29 for the total patient population (Fig. 2B) and after day 26 for the VASQIP subgroup (Fig. 3B).
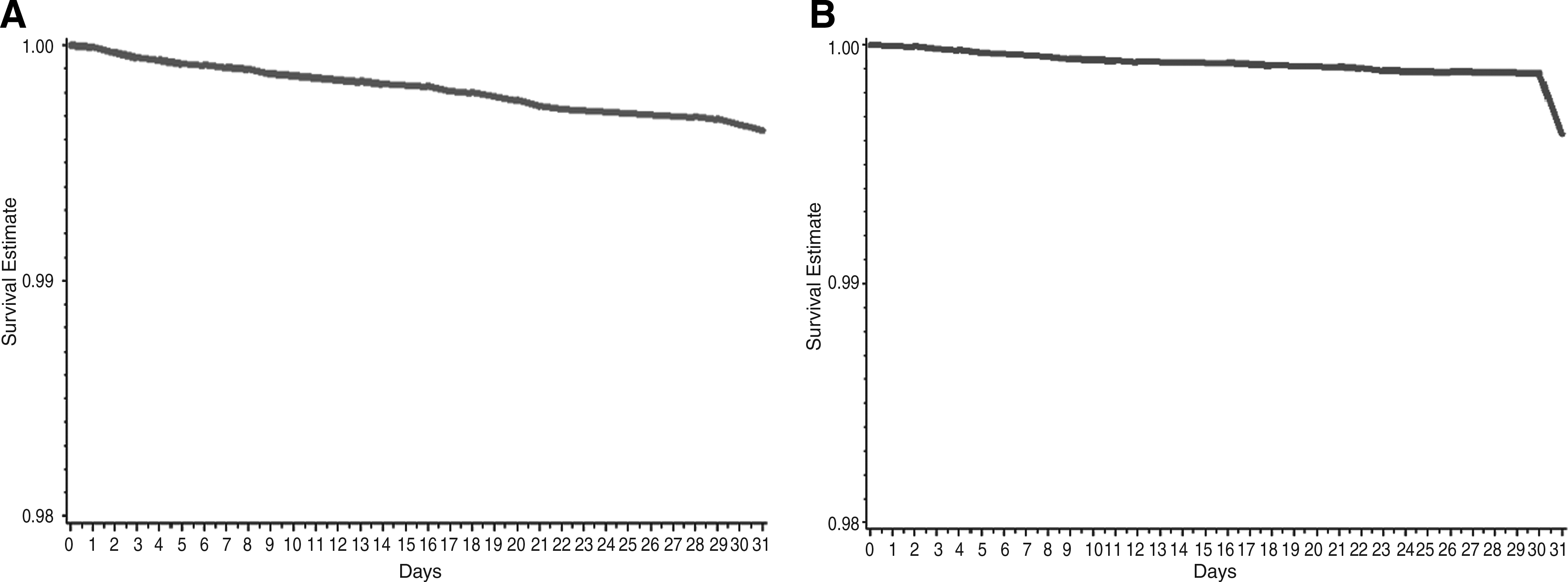
Multivariable survival analysis of time to conversion to methicillin-resistant Staphylococcus aureus positivity in total population of 3,890 initially MRSA-negative patients. Conversion to swab-positive status occurs gradually (

Multivariable survival analysis of time to conversion to methicillin-resistant Staphylococcus aureus positivity in 1,432 initially MRSA-negative patients in Veterans Affairs Surgical Quality Improvement Project population. Conversion to swab-positive status occurs gradually (
Discussion
We evaluated the rates and risk factors for MRSA acquisition in the 31-day post-operative period. We had a strictly defined risk group that was known to be negative for MRSA nasal colonization within a month prior to surgery and with no positive MRSA results in the year prior. In addition, post-operative acquisition of MRSA was assessed by a variety of methods, including nasal swabs for colonization, culture, and SSIs. Our results demonstrated that the overall rate of conversion to MRSA positivity after surgery is low, being 2% in at-risk patients. The majority of these conversions were clinically silent, being detected primarily because of our active surveillance program. Our findings add substantially to the current literature on MRSA conversion, which is limited largely to studies in critical care settings (intensive care units, trauma and burn units), none of which looked at prior-year MRSA status in defining baseline MRSA negativity [18–23]. Moreover, no study to date has examined the rates of post-operative MRSA colonization or infection in patients who tested MRSA-negative prior to surgery, as performed in this study.
A history of MRSA in the year prior is considered an important risk factor for MRSA colonization or infection in patients admitted to the hospital. Although our patient sample was MRSA-negative by prior-year history, the use of a 31-day pre-operative MRSA history alone resulted in similar conversion rates (data not shown), and the resultant risk factor profile for conversion did not change. Thus, a 31-day history was sufficient to predict conversion risk in our population.
The multivariable survival analysis for time to conversion to MRSA-positive swab and MRSA-positive culture yielded the curves in Figures 2 (total patient population) and 3 (VASQIP subset). Few events were seen in any of the four curves; this is indicative of the low conversion rates of 2% encountered in our medical center. Conversion to positive swabs was gradual over time, as seen in Figures 2A and 2B, and reflect the continuity of our center's MRSA surveillance program, which involves nasal swabbing throughout hospitalization, at unit transfers, and on discharge. Conversely, rates of conversion to positive cultures were clustered after day 29 for the total population (Fig. 2B) and after day 26 for the VASQIP sample (Fig. 3B), indicating that MRSA cultures were obtained because of clinical suspicion of MRSA infections, which occurred later in the post-operative period.
Vancomycin effect on conversion
Our data suggest that vancomycin use is associated with a higher risk of post-operative conversion to MRSA colonization or infection. The main clinical use of vancomycin prophylaxis is for prevention of post-operative infection in patients known to be MRSA colonized or to have a history of MRSA at the time of surgery [24]. Vancomycin is not recommended for routine use in all patients, especially MRSA-negative patients, as it is considered to be an inferior surgical prophylaxis agent compared with standard beta-lactam regimens for non-MRSA infections [24–30]. The use of vancomycin prophylaxis in 186 patients in our cohort was attributable mostly to a beta-lactam allergy or the surgeon's particular preference; this practice should be discouraged in favor of other, more effective, antibiotic regimens, especially when the SSI risk index is high.
The positive association of vancomycin surgical prophylaxis with MRSA conversion in our cohort may reflect underlying processes of care or patient characteristics that might lead to conversion. Post-operative processes of care are a key factor influencing MRSA acquisition by surgical patients, as they play a role in cross-transmission by MRSA among patients in healthcare settings [31,32]. Transiently colonized healthcare workers and contaminated hands have been postulated to transmit MRSA from patient to patient [33,34], and infection control guidelines have emphasized the importance of contact precautions in limiting the nosocomial spread of MRSA [35]. Although we did not account for post-operative variables in our multivariable regression analysis, processes of care effects after surgery may explain why vancomycin prophylaxis was not protective against MRSA acquisition in our sample population. Several case reports of sternal incision infections after cardiothoracic surgery have suggested post-operative seeding of the surgical site as a cause of SSI [36,37]. In a retrospective study of the risk factors for MRSA vs. MSSA SSI, no pre-operative or intra-operative variables were found to be associated independently with MRSA SSI [38]. Instead, only discharge to a long-term care facility, post-operative stay exceeding three days, post-operative antibiotic treatment exceeding 24 h, and leaving a surgical drain in place for more than 24 h were independent predictors of MRSA SSI. The study, among others [39–41], suggested contamination of the surgical site through manipulation by caregivers and via surgical drains as a likely mechanism by which post-operative variables predict MRSA SSI development.
Severity of illness is an established risk factor for nosocomial MRSA acquisition. Vancomycin, among other antibiotics, is utilized more frequently in severely ill patients; this may account in part for its association with conversion to MRSA positivity [33,42]. Likewise, age and patient co-morbidities are indicators of severity of illness among our sample patients, leading to the significant association of age and SSI risk index with conversion to MRSA positivity in our multivariable analysis. A systematic review of 74 studies of multiresistant organisms also found that on multivariable analysis, advanced age (OR 1.2–1.4); severity of illness according to the Acute Physiology and Chronic Health Evaluation (APACHE) II scoring system (OR 1.9); exposure to invasive medical devices, especially central venous catheters (OR 2.7–4.7); exposure to cephalosporins (OR 3.1) and other broad-spectrum antibiotics (OR 1.7–11.3); and gastrointestinal surgery (OR not quantified) were risk factors for nosocomial acquisition of MRSA [43]. A more recent prospective study using active MRSA surveillance cultures in a surgical intensive care unit found that tracheostomy (OR 2.18; 95% CI 1.13, 4.20), decubitus ulcer (OR 1.72; 95% CI 0.97, 3.06), and enteral nutrition (OR 3.33; 95% CI 1.13, 9.77) were independent risk factors for MRSA acquisition [44]. Undoubtedly, breaks in the skin and the need for invasive procedures are indicators of severity of illness in hospitalized patients and are a well-established conduit for MRSA in the critically ill [45]. In another prospective study of surgical patients, receipt of immunosuppressive therapy (OR 2.7; 95% CI 1.2, 6.5), the presence of at least one co-morbidity (OR 2.3; 95% CI 1.2, 4.7), emergency surgery (OR 2.2; 95% CI 1.2, 4.0), “contaminated” incision status (OR 1.7; 95% CI 1.3, 2.2), and duration of surgery longer than the 75th percentile (OR 3.0; 95% CI 1.7, 5.1) were independent risk factors for post-operative MRSA SSI [46].
Chlorhexidine–alcohol effect on conversion
Skin antisepsis is another process of SSI prevention that is less likely than antibiotic prophylaxis to contribute to multi-drug resistance, as it has a broader spectrum of activity and multiple targets of action [47]. Our results have shown that surgical site antisepsis with chlorhexidine–alcohol was not associated significantly with conversion to MRSA positivity. This may well be attributable to the fact that most of our conversion events were detected by nasal swabbing for MRSA, and nasal colonization occurs independently of skin preparation. Chlorhexidine–alcohol has been shown in recent trials and a meta-analysis to be superior to providone–iodine skin preparation in preventing SSI [48,49], yet its role in preventing post-operative MRSA acquisition is not supported by this study.
Surgery tier effect on conversion
Tier 1 (cardiac, thoracic, vascular, and orthopedic) operations are more likely to be targeted for a decolonization program because of the high rates of prosthesis implantation and the severe consequences of a potential procedure-related infection. Tier 1 operations were associated significantly with MRSA conversion in our total patient sample. In our VASQIP-assessed sample, however, surgery tier became non-significant, possibly because of the routine exclusion of cardiac operations from the VASQIP database and the inclusion of SSI risk index factors such as the type and complexity of operations. On the basis of these results, a procedure-specific decolonization program can be considered in MRSA-colonized patients.
Study limitations
The limitations of this work include the fact that it was conducted in a single institution on a predominantly male veteran population with a higher prevalence and severity of co-morbidities. Additionally, although greater than 95% compliance with Surgical Care Improvement Project (SCIP) guidelines has been reported at the VABHCS with regard to the timing and type of antimicrobial prophylaxis, we were able to capture only the first prophylactic agent administered; antibiotic treatment between the time of surgery and conversion to MRSA positivity was not abstracted. We also did not have data related to length of stay, additional post-operative procedures, and type of disposition at the time of discharge.
Conclusion
In our population of non-colonized patients with no history of MRSA exposure, the risk of conversion to MRSA positivity was small, at 2%. Possible associations with conversion included antibiotic prophylaxis with vancomycin, a high SSI risk index, and higher-risk operations. Post-operative risk factors and exposure to healthcare-associated MRSA in these patients were not measured and could also play a role in conversion. Alternatives to vancomycin prophylaxis should be considered in non-colonized patients and the patients' medical condition optimized to reduce the SSI risk index.
Footnotes
Author Disclosure Statement
Dr. Itani has received research support from Merck Pharmaceuticals and from Sanofi-Aventis Pharmaceuticals.