
Abstract
Abstract
Background:
Abscess incision and drainage (I&D) operations form the bulk of surgical procedures in the emergency department (ED). Nevertheless, epidemiologic, clinical, and bacteriology data are lacking for patients with abscesses presenting at Sudanese hospitals. Information also is unavailable on the magnitude of the problem of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) and its susceptibility to the most commonly used antibiotics. Our objectives were (1) to identify and document the epidemiologic and clinical variables of patients with superficial abscesses; (2) to isolate the causative organism(s) from the pus and determine their antibiotic sensitivity; (3) to determine the prevalence of CA-MRSA and its antibiotic susceptibility; and (4) to audit our practice of I&D of abscesses.
Methods
Results:
A total of 248 patients were included. The majority (84%) were younger than 40 years of age. There were twice as many male as female patients (69% vs. 31%, respectively). The majority of patients did not have a known predisposing factor, but 13% had a history of an abscess. A history of trauma was found in 27% of the patients, whereas diabetes mellitus was found in only 6%. The most common site of the abscess was the upper limb (46%) followed by the lower limb (20%). Most (85%) of the abscesses were drained under local anesthesia. Sensitivity tests were performed on 151 pus isolates. No growth was obtained in 28 (18.5%) of the specimens. Of the 123 specimens yielding growth, S. aureus was the most common organism (90%), followed by Klebsiella spp. (6.5%). The proportion of CA-MRSA was 24%. Many of these S. aureus isolates were resistant to other antibiotics also.
Conclusion:
This study documents some epidemiologic and bacteriological data on one of the most common surgical problems. We found a substantial proportion of the infecting organisms to be CA-MRSA. This reflects the abuse of antibiotics in the community and stresses the importance of health education. Standardized surgical and anesthetic guidelines should be followed for I&D of abscesses to avoid recurrence. Further studies are needed urgently.
Recently, methicillin-resistant Staphylococcus aureus (MRSA), particularly strains acquired in the community (CA-MRSA), has become a major cause of skin and soft tissue infections (SSTIs), particularly abscesses. Unfortunately, knowledge of their proportion in the abscesses and their susceptibility to other antibiotics is completely absent in Sudan.
In this era of evidence-based medicine, obtaining such information is vital to create guidelines for the prevention and treatment of this common surgical problem. This study aimed to reduce this gap in our knowledge. In addition, we sought to audit our practice of abscess drainage.
Patients and Methods
Patients
We conducted a prospective observational descriptive study of a convenience sample of patients who presented to the KNTH casualty department with community-acquired superficial (cutaneous and subcutaneous) abscesses (CA-A). This study was approved by the Ethics and Research Committee at KNTH and by the Research Committee at Alazhari University, Khartoum, Sudan. The study period spanned two years (2009–2010). We defined CA-A as an abscess acquired in the community when the patient had not been in the hospital for at least four weeks before. We included patients presenting on our unit's on-call day, which occurs on the sixth day of every week. Inpatients with hospital-acquired abscesses or a history of hospitalization within the four weeks prior to acquiring the abscess were excluded. A pro-forma was prepared to record the personal, clinical, and operative data of these patients (Fig. 1).
Abscess pro-forma.
There were two operations lists, at 12:00 noon and 5:00
Laboratory techniques
All of the swabs were cultured on several media: Blood agar under aerobic and anaerobic conditions, chocolate blood agar, MacConkey agar (Oxoid, LTD., Basingstoke, Hampshire, United Kingdom), and cooked meat medium. The plates were incubated for 48 h. Growth was studied further to identify the microorganisms using appropriate biochemical tests and serology.
Sensitivity tests against the most commonly used antibiotics were done using the Kirby-Bauer disk diffusion method with HiMedia discs (HiMedia Laboratories Pvt. Ltd., Mumbai, India). For gram-negative bacteria, we tested the following antibiotics: Ciprofloxacin, amoxicillin-clavulanic acid, ceftriaxone, cefuroxime, trimethoprim-sulfamethoxazole, and chloramphenicol. For gram-positive bacteria, we used amoxicillin-clavulanic acid, tetracycline, ceftriaxone, trimethoprim-sulfamethoxazole, oxacillin, and vancomycin. The results were interpreted according to the guidelines of the Clinical and Laboratory Standards Institute [1]. The disk diffusion results for each organism were classified into three categories—sensitive, intermediate sensitive, and resistant—according to the zone size interpretative chart, which is based on results obtained using Mueller-Hinton agar (HiMedia).
Data were summarized and grouped on a master sheet, computed, and analyzed with Statistical Package for the Social Sciences (SPSS) software program (SAS, Chicago, IL). Frequencies and proportions of the common causative micro-organisms, their antibiotic sensitivities, and the types of abscess were determined.
Results
A total of 171 male (69%) and 77 female (31%) patients were included. Two thirds of the patients (66.4%) were between the ages of 11–30 years of age, and (84.1%) were younger than 40 years of age (Fig. 2). Almost one-half of the patients (46%) were manual workers (Table 1). Students accounted for 17%, followed by office employees and housewives (11% each). Children accounted for 10% of the series, and 5% were unemployed adults.
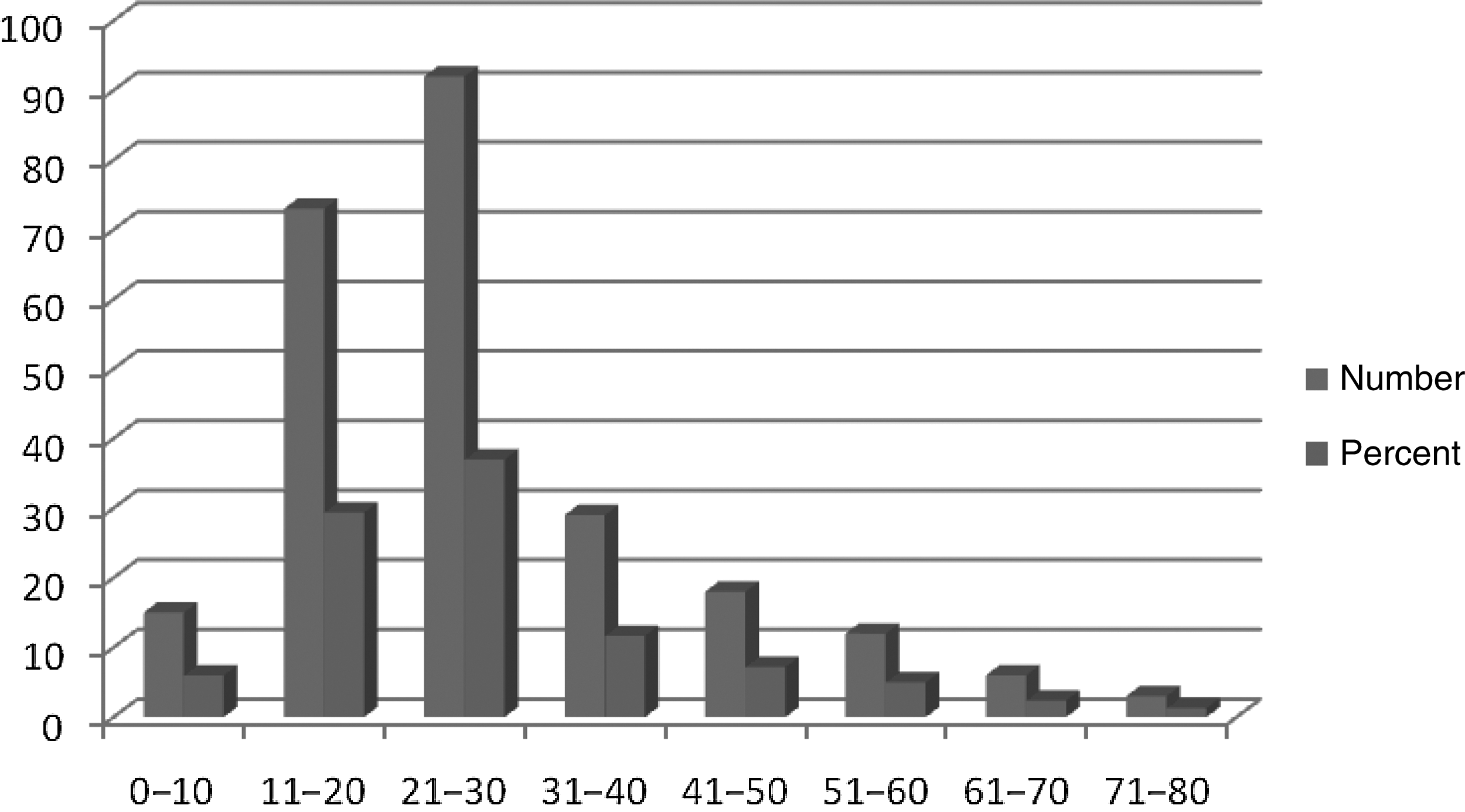
Age distribution of 248 patients with abscesses.
As expected, pain was the most common presenting symptom. Interestingly, 21% of the patients admitted having a pre-hospital treatment of some sort, which included antibiotics, herbs, or hot soaks (Table 2). There was a history of an abscess in 32 patients (13%). Of those, 20 patients (63.5%) had an abscess recurrence in the same site (commonly perianal). Regarding predisposing factors, we obtained a history of trauma in 27% of the patients, diabetes mellitus in 6%, or drug addiction (volunteered by one patient). We obtained no history of intramuscular injection as a predisposing factor. In the rest of the patients (54%), no cause was apparent (Table 3). Most abscesses were on the upper limbs (46%), followed by the lower limbs (20%), head and neck (16.5%), perineum (mainly perianal) (10%), and 7% trunk (breasts 2% and gluteal region 4%) (Table 4).
Some patients presented with more than one symptom.
The diagnosis of the abscess was made mainly on clinical grounds. Confirmatory aspiration of the pus was done in 4.5% of the patients. No patient was sent for an ultrasound or computed tomography scan. Most of the abscesses (85%) were drained under local anesthesia, and all the patients were discharged home the same day.
Culture and sensitivity tests were done on pus specimens obtained from 151 patients. No growth was obtained in 28 cultures (18.5%). Of the 123 specimens yielding bacteria, S. aureus was isolated from 111 (90.25%) followed by Klebsiella spp. in 8 (6.5%). Pseudomonas aeruginosa, Proteus vulgaris, and Streptococcus pyogenes together accounted for 3.25% of the positive cultures (two, one, and one patient, respectively) (Table 5).
Staphylococcus isolates were subjected to sensitivity tests using standardized bacteriology techniques. The organisms were then categorized into three groups: Sensitive, intermediate sensitivity, or resistant to the particular antibiotic (Fig. 3).
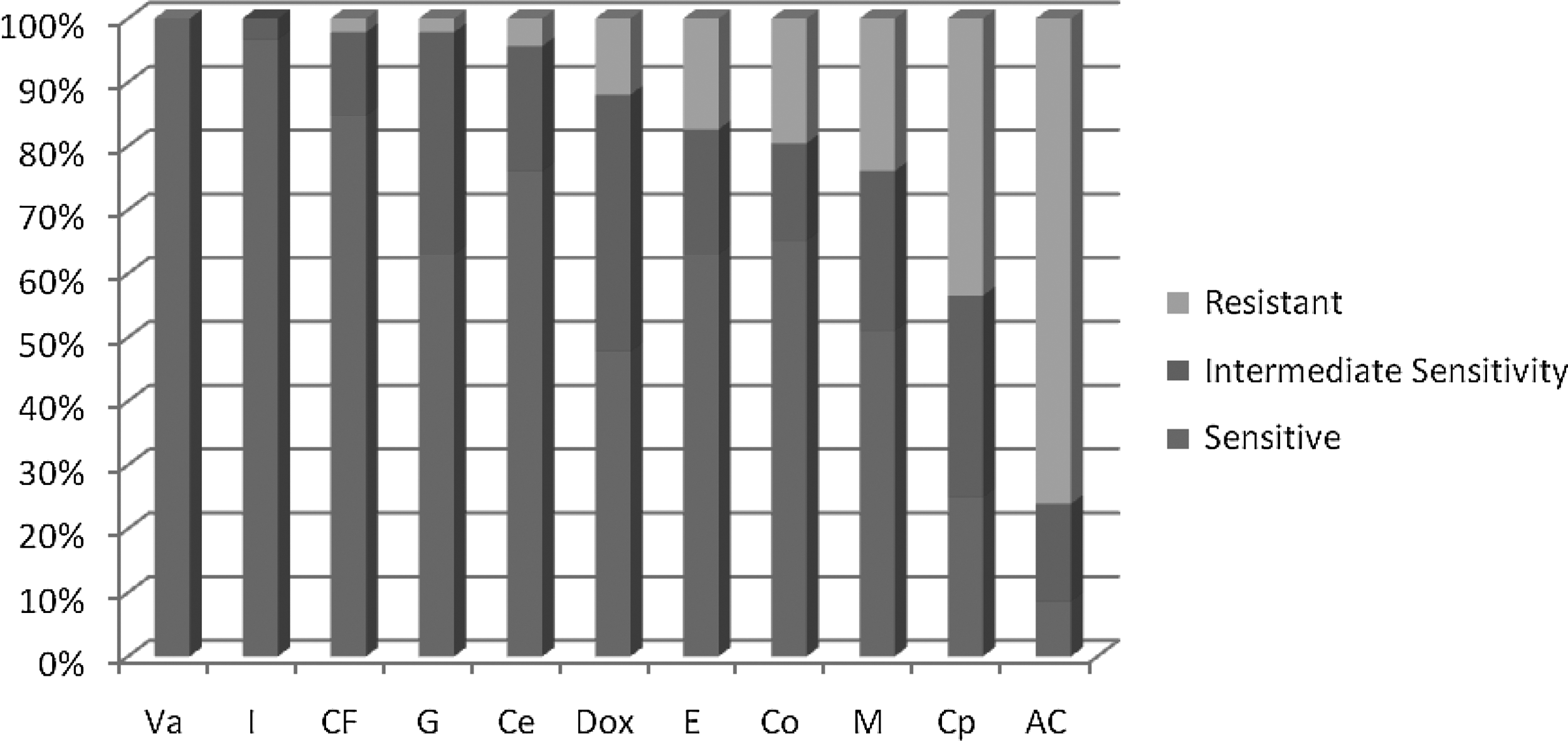
Results of antibiotic sensitivity tests for 111 Staphylococcus aureus isolates. Va=vancomycin; I=imipenem-cilastatin; CF=ciprofloxacin; G=gentamicin; Ce=cefotaxime; Dox=doxycycline; E=erythromycin; CO=trimethoprim/sulfamethoxazole; M=methicillin; Cp=cephalexin; AC=amoxicillin-clavulanic acid. A total of 24% of the isolates were community-acquired methicillin-resistant S. aureus.
A total of 20 (24%) of S. aureus isolates showed resistance to the commonly advocated antibiotics cloxacillin and methicillin. We have strong reason to believe that these organisms were acquired in the community and thus were indeed CA-MRSA.
Six of the eight Klebsiella strains (75%) were isolated from abscesses in the perineum and lower limbs. Sensitivity tests were done and the results categorized as above (Fig. 4).
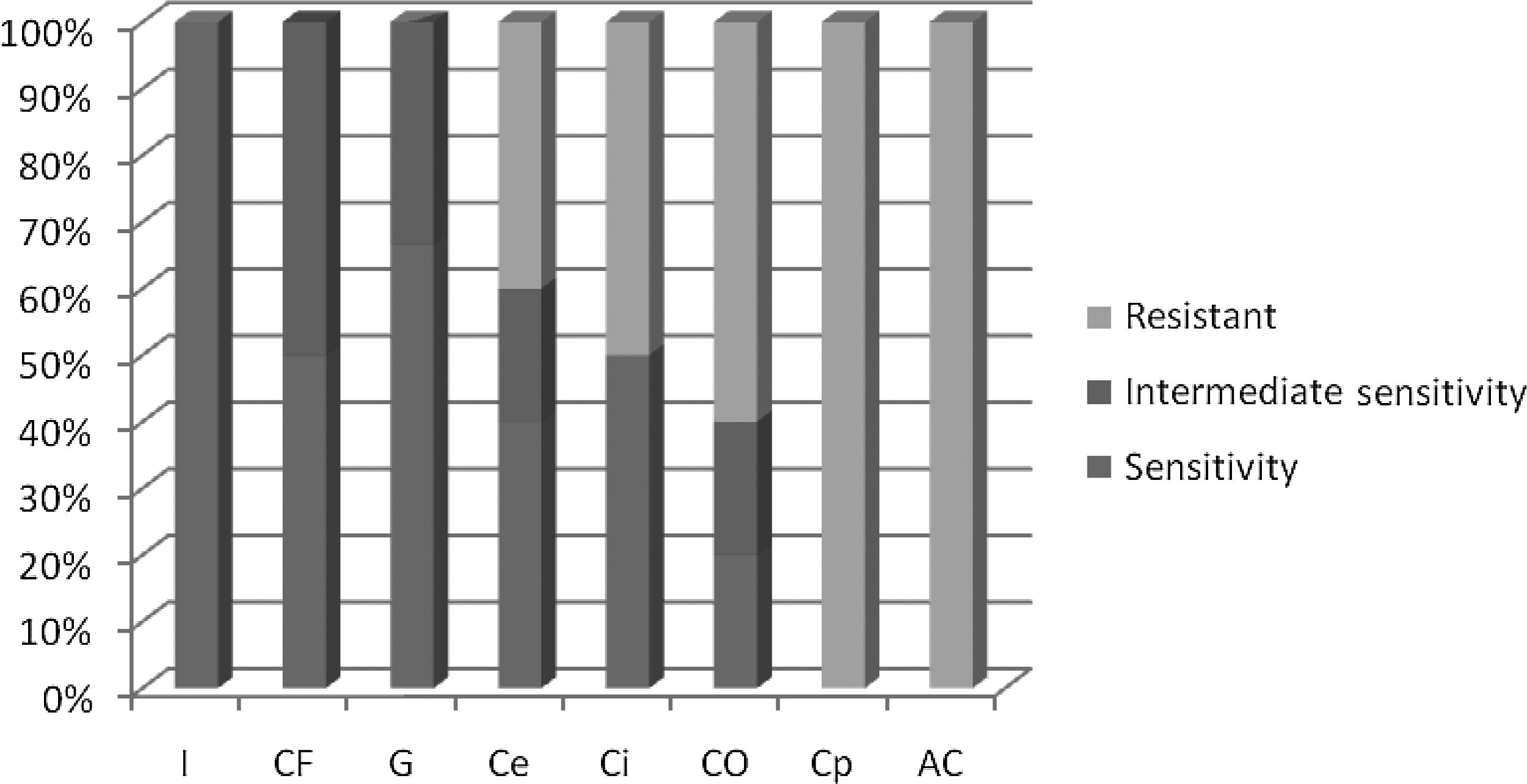
Results of antibiotic sensitivity tests for eight Klebsiella isolates. I=imipenem-cilastatin; CF=ciprofloxacin; G=gentamicin; Ce=cefotaxime; Ci=ceftriaxone; CO=trimethoprim/sulfamethoxazole; Cp=cephalexin; AC=amoxicillin/clavulanic acid.
Discussion
The observation that so many patients with superficial abscesses acquired in the community continued to present to the surgical casualty department in our hospital was the trigger for this study. The workload of the operation of “I&D of an abscess” at KNTH casualty has been estimated at between 20 and 30 operations/day, constituting 70%–80% of all surgical operations performed on one on-call day.
We propose to define CA-A as an abscess acquired in the community where the patient has not been in hospital for at least four weeks before acquiring the abscess. We have, therefore, excluded any patient with a history of hospitalization for abscess within four weeks of presentation.
It was striking, although not surprising, that the majority of patients (84%) were younger than 40 years of age. This is similar to the findings of Mahdi et al. at Khartoum Teaching Hospital [2]. Two thirds of the patients were in the active age group (11–30 years), and there was a peak of cases in the 21–30 years group (see Fig. 3). This reflects the fact that abscesses afflict young and economically active persons.
Manual workers constituted almost one-half of the patients (46%). This could explain the finding that almost half of the abscesses occurred on the upper limbs. Those manual workers and office workers accounted for 57% of the patients. This reflects the huge economic impact of abscesses, not only on the individual patient, but also on the community in the form of lost working hours. The unemployed constituted only 5% of the patients, whereas housewives and children together accounted for 21%. Health education, particularly regarding hand washing with soap and water after work, play, and household activity, may reduce hand contamination and hence decrease the likelihood of acquiring an abscess.
The majority of abscesses (81%), including those in patients with a history of trauma, occurred in previously healthy patients without a known predisposing factor or immunocompromise. This situation also was observed by Gorak et al. from the United States [3]. Persons with diabetes mellitus constituted only 6% of our patients, which may be attributable to the fact that 84% of our patients were young.
In contrast to the findings of Frazee et al., injection of illicit drugs was admitted by only one patient [4]. A history of some sort of trauma was found in 27% of the patients, whereas none had a history of intra-muscular injection of drugs such as chloroquine, which was observed in the past. This may be secondary to the fact that chloroquine is no longer used for the treatment of malaria in Khartoum state because of the emergence of resistant Plasmodium strains.
Only four patients (1.5%) admitted using antibiotics before presentation to the hospital for the specific reason of preventing or treating the abscess. No specific question was asked about whether the patients had used antibiotics for any other infections such as those of the respiratory or urinary tract. We should take this possibility into account in our future studies. The finding suggests that the 24% CA-MRSA prevalence could not be attributable to antibiotic use by the patients and might indicate antibiotic abuse in the community. The real prevalence of antibiotic use in the population served is not known. However, the general impression of antibiotic abuse stems from the following observations: (1) Physicians prescribe antibiotics empirically without bacteriology susceptibility tests in many cases; (2) antibiotics can be obtained in many pharmacies without a medical prescription; (3) physician fees are high, so patients go directly to a pharmacy for medical advice; and (4) patient-to-patient consultations occur freely.
As stated above, antibiotic abuse may occur at the level of patients, physicians, and pharmacists. It is to be noted that this has become a worldwide problem. Health education and several approaches have been suggested to reduce antibiotic resistance in the community [5]. We can only add our voice and recommend health education for all: Physicians, pharmacists, and the general public. Actions should include reducing unnecessary antibiotic prescriptions; using an optimal dosage and duration of antibiotic regimens, as inappropriately low doses and long treatment could promote resistance; and adherence to laws preventing the dispensing of antibiotics without a prescription.
Although the majority of patients did not have a predisposing factor for abscess, there was a history of abscess in 13%. These lesions occurred mostly in the same site as the present abscess (63.5%), especially perianal abscesses. Further studies are required to explore the cause(s) of this observation. However, the finding that 85% of the abscesses were drained using local anesthesia may explain the high recurrence rate in part as indicating inadequate drainage.
Clinically, about two thirds of the abscesses were on the limbs: 46% on the upper and 20% on the lower limbs. This is different from the study at Khartoum, where the head and neck had the highest percentage of lesions. Auditing our practice revealed that the diagnosis was made mainly on clinical grounds. Confirmatory aspiration of pus was done in only 4.5% of patients, and no patient underwent an imaging scan. We also found out that 85% of the abscesses were operated on under local anesthesia. This may be attributable to the lack of resources
Bacteriology (culture and susceptibility) tests on pus specimens showed that S. aureus was the causative organism in the majority (90%) of cases in which micro-organisms could be grown. This finding conforms to the results of most previous studies.
Twenty-four percent of these S. aureus isolates were methicillin/cloxacillin resistant. Because those abscesses were acquired in the community, mostly by young patients without any predisposing factors for infection and without a history of hospitalization for four weeks prior to presentation, we can assume that the organisms were CA-MRSA. The antibiotic susceptibility tests provided additional evidence for this view. The limitation of this study was the unavailability of genetic typing of the CA-MRSA strains. This should be addressed in future studies.
Our study showed, for the first time in Sudan, that CA-MRSA constituted almost one-quarter (24%) of the organisms isolated in casualty department-drained abscesses. Some studies from abroad revealed a higher incidence of CA-MRSA in the ED, amounting in one study to 51% of the total [4]. Even our lower tally is alarming, however, as these abscesses were acquired in the community, not in hospitals. We would expect the prevalence of hospital-acquired (HA)-MRSA to be much higher. Further studies are needed to explore this problem in inpatients also and to compare the antibiotic susceptibilities of HA- and CA-MRSA.
Because CA-MRSA is known to infect young, otherwise-healthy individuals, the high proportion of CA-MRSA may be the reason behind the high numbers of patients presenting with abscess, not only at KNTH, but also at all the major hospitals in the capital, Khartoum. It may also explain the fact that in most of our patients, there was no predisposing factor, such as diabetes mellitus or other cause of immunocompromise.
Antibiotic susceptibility tests of Staphylococcus showed high sensitivity to vancomycin (100%), clindamycin (100%), imipenem-cilastatin (97%), ciprofloxacin (85%), and cefotaxime (76.5%). It is to be noted that a drug such as gentamicin has shown a lower sensitivity percentage (63%) than cefotaxime. However, it has a much lower resistance rate (2%) than does cefotaxime (4%). Hence, we propose the use of the sensitivity:resistance ratio (SSR) as a mathematical tool to compare the efficiency of drugs. This ratio is calculated by dividing the sensitivity percentage by the resistance percentage of the micro-organism under question for each drug. We believe that the SSR is a better description than pure resistance percentages, as it allows the prescribing physician to compare the efficiency of antibiotics and choose the most appropriate one for a given organism. In the comparison mentioned above, gentamicin had a higher SRR of 32:1 (% sensitivity [63]/% resistance [2]) than cefotaxime (19:1). On the other hand, cefotaxime was more efficient than cephalexin (SRR=1:2). The latter drug shows “reversal” of the ratio, meaning there are more isolates resistant to this drug than sensitive to it.
Interestingly, this study also showed high resistance of S. aureus and low SRR to the following commonly used antibiotics: Trimethoprim/sulfamethoxazole (20%; SRR 3:1) and methicillin/cloxacillin (24%; SRR 2:1). A total of 76% of isolates were resistant to amoxicillin-clavulanic acid, producing a reversed SRR (1:8). These findings mean that these three drugs can no longer be recommended for prophylaxis and treatment of staphylococcal infections in Sudan despite the fact that trimethoprim/sulfamethoxazole is used extensively in some other countries such as the United States to treat MRSA [6]. In our study 65% of the Staphylococcus isolates were sensitive to this drug combination, whereas 20% were resistant (SRR=3.2:1). We generally would not recommend an antibiotic with an SRR<5, as this would mean its inefficiency in one of four patients, too low a probability of success to depend on. The resistance of staphylococci isolated from these CA-As to many of the commonly used antibiotics strengthens the suspicion of antibiotic abuse in the community.
Klebsiella spp. (gram-negative bacilli) were isolated from eight of the specimens of pus (5.3%). In these cases, the infected pus usually (75% of cases) was drained from perianal and lower limb abscesses. This is not surprising, as Klebsiella is part of the natural flora of the bowel and can contaminate the perianal area. Tests showed high sensitivity to imipenem-cilastatin, ciprofloxacin, tetracycline, gentamicin, and amikacin. The organism showed a high level of resistance to the rest of antibiotics tested, notably the third-generation cephalosporins cefotaxime (40%; SRR 1:1) and ceftriaxone (50%; SRR 1:1). Klebsiella also showed high resistance to trimethoprim-sulfamethoxazole (60%) with a reversed SRR (0.33:1). Notably, all isolates were resistant to cephalexin, ceftazidime, and amoxicillin-clavulanic acid (SRR=0). Care must be taken in interpreting these results, however, as the number of isolates was small.
The other bacteria isolated were two Pseudomonas spp., one hemolytic Streptococcus, and a Proteus vulgaris. Notably, Pseudomonas was isolated from head and neck abscesses. It was sensitive to imipenem-cilastatin, gentamicin, ciprofloxacin, and cefotaxime. Streptococci showed sensitivity to cefotaxime, vancomycin, tetracycline, and gentamicin; intermediate sensitivity to amikacin; and resistance to trimethoprim/sulfamethoxazole. Proteus was sensitive to imipenem-cilastatin, ciprofloxacin, ceftazidime, ceftriaxone, and trimethoprim-sulfamethoxazole. It was resistant to cefotaxime and had intermediate sensitivity to amikacin, cefalexin, and amoxicillin-clavulanic acid.
This and similar studies on antibiotic sensitivity are useful, as the findings give the treating physician information on antibiotic susceptibility in cases when the empirical use of antibiotics is important or urgent before the results of culture arrive. These tests and susceptibility tables have to be updated from time to time and from place to place to cope with changing antibiotic resistance patterns.
It is to be stressed that the definitive treatment of an abscess is I&D. Antibiotics should not be given to patients with a formed abscess, as they will not help as well and can create an “antibioma.” Antibiotics can be used during the early cellulitis or inflammatory phase, to tip the balance in favor of body defenses and abort the formation of an abscess. This is particularly helpful in persons with diabetes mellitus and immunocompromised patients. The value of antibiotics after I&D of an abscess is controversial. Some randomized studies indicate that it may reduce the likelihood of recurrence or formation of another abscess [6].
We had to deal with certain difficulties during the conduct of this study. Sampling was interrupted several times by the lack of financial support, which was needed mainly to cover the cost of culture and sensitivity tests. At the time, the price of a single test was 15 Sudanese pounds (USD7–8). Many patients could not afford the cost and never returned. We found no financial support from the government or private companies. Hence, we financed the study ourselves. We eventually got a reduced rate from the director of KNTH, to whom we are grateful. This financial problem was the main reason for interrupting the study several times.
We must emphasize that this study reveals different antibiotic susceptibilities of Staphylococcus (MRSA) than is known in the developed world. Such information may be life saving in the era of easy transcontinental travel. Medical authorities should therefore be alert to the development of resistant strains.
Conclusions
Abscess drainage forms the bulk of surgical emergency operations in our hospital. Most community-acquired abscesses occur in the young and previously healthy with no known predisposing factors. The significance of this study is the finding of a high prevalence of CA-MRSA in the pus drained from these patients. This could explain the observed high numbers of patients with superficial abscesses presenting to hospital casualty departments in the Khartoum area. The high proportion of CA-MRSA also may indicate abuse of antibiotics in the community. Health education is needed urgently to prevent abscesses and reduce antibiotic resistance.
Further studies on CA-MRSA are needed, particularly genetic typing, epidemiology, and antibiotic sensitivities. We strongly recommend adherence to the practice of performing culture and susceptibility testing of the pus obtained from abscesses in this era of emerging and changing resistance. Policy makers must provide this service in public hospitals free or at a reasonably subsidized fee. Surgical and anesthetic guidelines of I&D of abscesses must be established and followed in all hospitals to prevent recurrences.
Financial support is lacking in Sudanese medical practice. Governmental institutes, such as universities and the Ministries of Health and High Education, as well as private institutions such as pharmaceutical companies and international organizations are invited to encourage further studies and clinical research in order to forward science and improve health service. Information on antibiotic sensitivities of MRSA in developing countries can be of great importance to the developed world in this era of easy transcontinental travel.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Acknowledgments
We are most grateful for the collaboration of the central laboratory staff at Khartoum North Teaching Hospital, led by Mrs. Naimat I. Mohammed. We are indebted to all the surgical team who worked with us during the study and helped in the treatment of patients, collection of data, and carrying the specimens to the laboratory.