
Abstract
Abstract
Background:
The Study for Monitoring Antimicrobial Resistance Trends (SMART) follows trends in resistance among aerobic and facultative anaerobic gram-negative bacilli (GNB) isolated from complicated intra-abdominal infections (cIAIs) in patients around the world.
Methods:
During 2004–2009, three centralized clinical microbiology laboratories serving 59 private hospitals in three large South African cities collected 1,218 GNB from complicated intra-abdominal infections (cIAIs) and tested them for susceptibility to 12 antibiotics according to the 2011 Clinical Laboratory Standards Institute (CLSI) guidelines.
Results:
Enterobacteriaceae comprised 83.7% of the isolates. Escherichia coli was the species isolated most commonly (46.4%), and 7.6% of these were extended-spectrum β-lactamase (ESBL)-positive. The highest ESBL rate was documented for Klebsiella pneumoniae (41.2%). Overall, ertapenem was the antibiotic most active against susceptible species for which it has breakpoints (94.6%) followed by amikacin (91.9%), piperacillin-tazobactam (89.3%), and imipenem-cilastatin (87.1%), whereas rates of resistance to ceftriaxone, cefotaxime, ciprofloxacin, and levofloxacin were documented to be 29.7%, 28.7%, 22.5%, and 21.1%, respectively. Multi-drug resistance (MDR), defined as resistance to three or more antibiotic classes, was significantly more common in K. pneumoniae (27.9%) than in E. coli (4.9%; p<0.0001) or Proteus mirabilis (4.1%; p<0.05). Applying the new CLSI breakpoints for carbapenems, susceptibility to ertapenem was reduced significantly in ESBL-positive E. coli compared with ESBL-negative isolates (91% vs. 98%; p<0.05), but this did not apply to imipenem-cilastatin (95% vs. 99%; p=0.0928). A large disparity between imipenem-cilastatin and ertapenem susceptibility in P. mirabilis and Morganella morganii was documented (24% vs. 96% and 15% vs. 92%, respectively), as most isolates of these two species had imipenem-cilastatin minimum inhibitory concentrations in the 2–4 mcg/mL range, which is no longer regarded as susceptible.
Conclusions:
This study documented substantial resistance to standard antimicrobial therapy among GNB commonly isolated from cIAIs in South Africa. With the application of the new CLSI carbapenem breakpoints, discrepancies were noted between ertapenem and imipenem-cilastatin with regard to the changes in their individual susceptibilities. Longitudinal surveillance of susceptibility patterns is useful to guide recommendations for empiric antibiotic use in cIAIs.
Country-specific epidemiologic and susceptibility data are important to guide empiric therapy, and such data have not been available for South Africa. This report provides an evaluation of the epidemiology of gram-negative pathogens isolated from cIAIs for the six-year period 2004 to 2009 in South Africa and highlights the prevalence of ESBL production, the comparative susceptibility patterns of ESBL-positive vs. ESBL-negative strains, the rate of MDR pathogens, and the impact of the new lower Clinical Laboratory Standards Institute (CLSI) carbapenem breakpoints on carbapenem susceptibility.
Materials and Methods
Three centralized clinical microbiology laboratories (Ampath National Laboratory Services, Johannesburg; Ampath National Laboratory Services, Pretoria; Pathcare, Cape Town) collected isolates derived (anonymously) from cIAIs in patients at 59 private hospitals in three South African cities: Johannesburg (n=19), Pretoria (n=21), and Cape Town (n=19). Only one isolate per patient was accepted for the study. All organisms were determined to be clinically important by local participants. Inclusion of isolates was independent of prior antimicrobial use, age, or gender. Consecutive isolates of as many as 100 GNB from each microbiological center were collected annually between 2004 and 2009 from specimens derived from intra-abdominal sites (appendix, peritoneum, colon, bile, pelvic cavity, and pancreas). Acceptable specimens included tissue, fluid, or deep site cultures obtained intra-operatively. Isolates from blood or urine of patients with cIAIs and specimens from peri-rectal abscesses were excluded. No data were recorded relating to when the specimen was collected in relation to time after hospital admission.
From 2004 through 2007, isolates were identified to the species level and tested for antimicrobial susceptibility at each site. Beginning in 2008 and 2009, all isolates were sent to a central laboratory (Laboratories International for Microbiology Studies, a subsidiary of International Health Management Associates, Inc., Schaumburg, IL) for confirmation of identification and antimicrobial susceptibility testing. A centralized database of study results also was operated by International Health Management Associates. The isolates were sent to the central laboratory on chocolate agar slants, and representative samples were stored both at the investigator site and the central laboratories in tryptic soy broth containing 2% glycerol at −70°C.
Minimum inhibitory concentrations (MICs) were determined for 12 antimicrobial agents using custom MicroScan dehydrated broth microdilution panels (Siemens Medical Solutions Diagnostics, West Sacramento, CA) according to the Clinical and Laboratory Standards Institute (CLSI) guidelines [13]. The MIC interpretive criteria followed guidelines established by the CLSI, and isolates of E. coli, K. pneumoniae, K. oxytoca, and Proteus mirabilis were classified phenotypically as ESBL producers using CLSI methodology [14]. Quality control (QC) was performed on each day of testing using the CLSI-recommended QC strains: E. coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, and K. pneumoniae ATCC 700603 (positive ESBL control). Results were included in the analysis only when corresponding QC isolates tested within the acceptable range according to the CLSI guidelines [13,14]. The ESBL data for regions outside South Africa were provided by IHMA, Inc., and adapted from the SMART database. Multi-drug resistance was defined as resistance to three or more of the following antibiotic classes: Aminoglycosides (represented by amikacin), cephalosporins (ceftriaxone, ceftazidime, cefotaxime, and cefepime), fluoroquinolones (ciprofloxacin, levofloxacin), β-lactam/β-lactamase inhibitors (ampicillin-sulbactam, piperacillin-tazobactam), and carbapenems (ertapenem, imipenem-cilastatin).
The prevalence of resistance to the aminoglycoside, fluoroquinolone, and carbapenem antibiotics was compared in ESBL-positive and ESBL-negative isolates of E. coli, K. pneumoniae, and P. mirabilis using the Fisher exact (two-tail) test (Graphpad Instat 3 for Windows; Graphpad Software, Inc., La Jolla, CA).
Results
Frequency of pathogen occurrence
The frequency of isolation of various species (n≥10) over the six-year study period is depicted in Table 1. A total of 1,218 aerobic and facultatively anaerobic GNB were isolated. Enterobacteriaceae comprised 83.7% (1,019/1,218) of the total: E. coli 46.4% (n=566), Klebsiella spp. 14% (n=171), Enterobacter spp. 7.5% (n=92), and Proteus spp. 6.7% (n=81) contributing the majority of these isolates, accounting for 89.3% (910/1,019) of the Enterobacteriaceae and 74.7% (n=910) of all isolates. Following E. coli, P. aeruginosa was the most common pathogen cultured, accounting for 12.6% (n=154) of all isolates. K. pneumoniae (n=136) and P. mirabilis (n=71) were the third (11.2%) and fourth (5.9%) most commonly identified species, respectively, and miscellaneous species (n=19) represented 2.9% (31/1,218) of the total isolates.
ESBL=extended spectrum β–lactamase.
Comparative antimicrobial susceptibility
Comparative antimicrobial susceptibility results for the most frequently isolated GNB (n≥10) are shown in Tables 2 and 3. Overall, against species for which it has breakpoints, ertapenem was the most active drug (94.6%), followed by amikacin (91.9%), piperacillin-tazobactam (89.3%), imipenem-cilastatin (87.1%), and cefepime (86.8%). Data on the latter four agents include susceptibility testing results for P. aeruginosa and Acinetobacter baumannii, which lowered the relative activity because of the high number of resistant isolates typically found in these species. Overall, the highest resistance rates were seen for ampicillin-sulbactam (58%), ceftriaxone (29.7%), cefotaxime (28.7%), ciprofloxacin (22.5%), levofloxacin (21.1%), and cefoxitin (18.6%).
According to Clinical Laboratory Standards Institute M100-S21 breakpoints.
Ertapenem, cefotaxime, ceftriaxone data for P. aeruginosa and A. baumannii not included, as there are no CLSI breakpoints for these agents.
AS=ampicillin-sulbactam; Ak=amikacin; Cax=ceftriaxone; Caz=ceftazidime; Cft=cefotaxime; Cfx=cefoxitin; Cp=ciprofloxacin; Cpe=cefepime; Etp=ertapenem; Imp=imipenem-cilastatin; Lvx=levofloxacin; PT=piperacillin-tazobactam; ESBL=extended spectrum β-lactamase.
Percent susceptibility according to Clinical Laboratory Standards Institute M100-S21 breakpoints.
Ertapenem, cefotaxime, ceftriaxone data for Pseudomonas aeruginosa and Acinetobacter baumannii not included, as there are no CLSI breakpoints for these agents.
For the six-year study period, imipenem-cilastatin (99%), amikacin (98%), and ertapenem (97%) were the most active antibiotics against all E. coli isolates followed by piperacillin-tazobactam (94%). The fluoroquinolones, ciprofloxacin (77%), and levofloxacin (78%), as well as ampicillin-sulbactam (40%), were the least active. Regarding P. aeruginosa, piperacillin-tazobactam (92%) was the most active agent followed by imipenem-cilastatin (75%), ceftazidime (75%), cefepime (74%), and amikacin (73%). For both ESBL-positive and -negative K. pneumoniae and K. oxytoca, imipenem-cilastatin (99%), ertapenem (96%), and amikacin (93%) were the most active agents, whereas 86% and 84% of these species were susceptible to levofloxacin and ciprofloxacin, respectively. Activity against P. mirabilis (inclusive of ESBL-positive isolates) exceeded 90% for all drugs other than ampicillin-cilastatin sulbactam, ceftriaxone, cefotaxime, and imipenem-cilastatin. For the 89 isolates of Enterobacter listed in Table 2 (E. cloacae 67, E. aerogenes 14, and unspecified species 11), amikacin (96%), levofloxacin (93%), cefepime (91%), and ciprofloxacin (90%) were the most active agents, with carbapenem susceptibility documented as 84% for both imipenem and ertapenem.
Production of extended-spectrum β-lactamase
Nine percent (110/1,218) of the Enterobacteriaceae were ESBL producers (see Tables 1 and 2). As depicted in Figure 1, where the combined international ESBL rates (2002–2009) of E. coli and K. pneumoniae were compared by region, a major disparity between these two species was observed. The highest ESBL-positive rate was documented for K. pneumoniae, with 41.2% (56/136) of isolates positive, whereas only 7.6% (43/566) of E. coli were ESBL producers. With regard to P. mirabilis and K. oxytoca, 11.3% (8/71) and 8.6% (3/35), respectively, were ESBL producers. Because the CLSI method for ESBL detection is not validated for Enterobacter spp., these isolates were not categorized as ESBL-positive or -negative using the phenotypic test. No significant differences in ESBL production were observed over the six-year study period for any of the pathogens (data not shown).
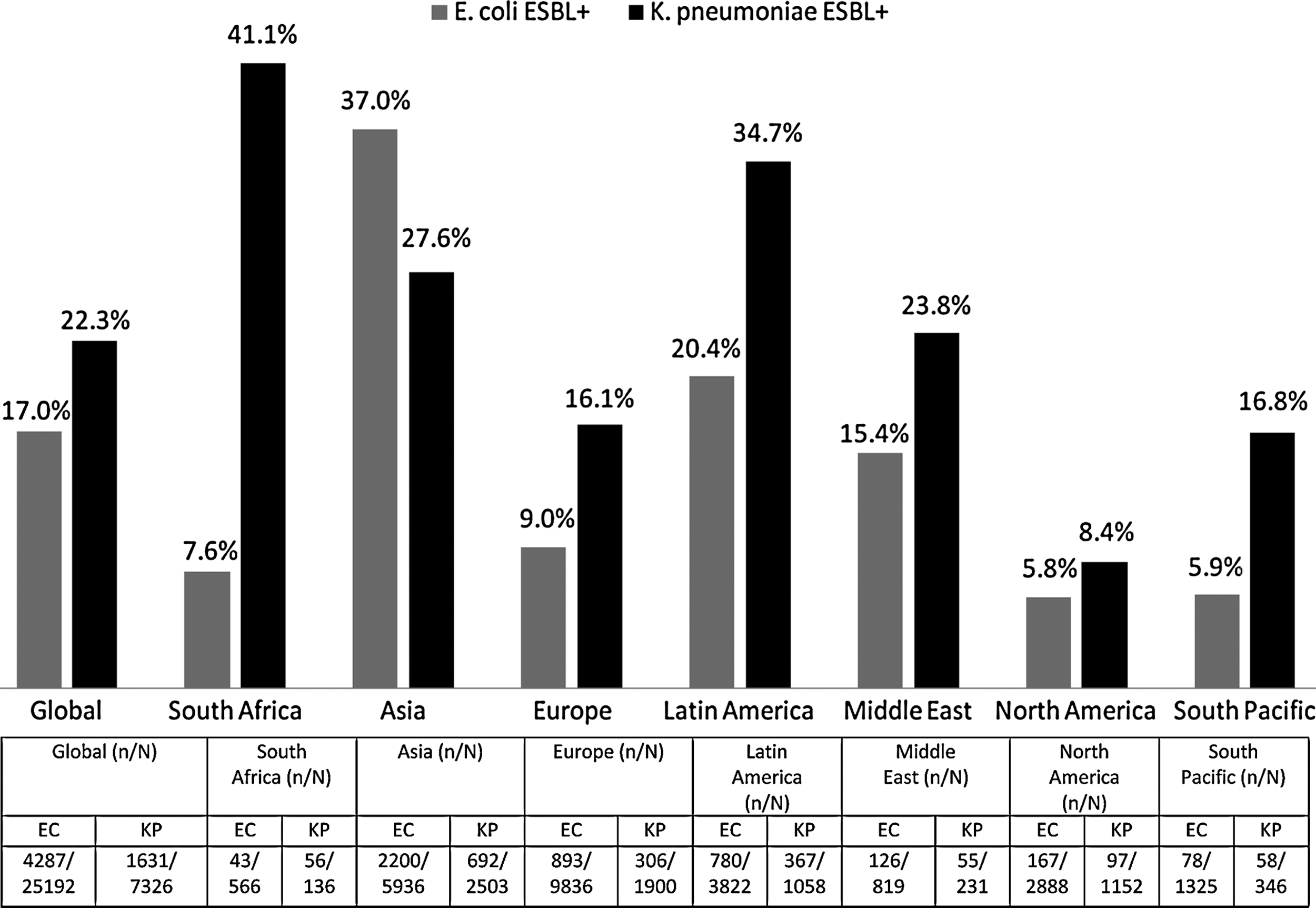
Comparative extended-spectrum β-lactamase production by Escherichia coli vs. Klebsiella pneumoniae by region: Combined SMART data 2002–2009.
The impact of ESBL production on susceptibility rates to antibiotic classes were as follows: Amikacin susceptibility was significantly lower in ESBL-producing phenotypes for both E. coli (38/43 [88%] vs. 518/523 [99%]; p<0.05) and K. pneumoniae (44/56 [79%] vs. 77/80 [96%]; p<0.05). Production of ESBL in E. coli impacted dramatically on levofloxacin resistance (22/43 [51%] vs. 99/523 [19%]; p<0.0001) and ciprofloxacin (25/43 [58%] vs. 105/523 [20%]; p<0.0001) compared with ESBL non-producers. This was similar for ESBL-positive phenotypes of K. pneumoniae for levofloxacin (30/56 [54%] vs. 9/80 [11%]; p<0.0001) and ciprofloxacin (22/56 [61%] vs. 70/80 [12%]; p<0.0001), respectively. Activity of all the cephalosporins also was considerably compromised in ESBL producers among E. coli compared with non-ESBL isolates (64.5% vs. 2.5% resistance; p<0.0001). Resistance rates for the specific agents in ESBL-positive isolates were 83%, 70%, 63%, and 42% for cefotaxime, ceftriaxone, ceftazidime, and cefepime, respectively. This was similar for the cephalosporins overall with regard to K. pneumoniae (89.5 vs. 5.5%; p<0.0001) and for cefotaxime, ceftriaxone, ceftazidime, and cefepime, for which resistance rates were 98%, 95%, 91%, and 75%, respectively. In comparison with ESBL-positive E. coli, ESBL-positive K. pneumoniae were not less susceptible to ertapenem (49/56 [88%] vs. 39/43 [91%]) and amikacin (44/56 [79%] vs. 38/43 [88%]), a difference that was not statistically significant. Similarly, ciprofloxacin and levofloxacin susceptibility was not significantly different in these species (22/58 [39%] vs. 18/43 [42%] and 26/58 [46%] vs. 21/43 [49%], respectively). However, the impact of ESBL production on cephalosporin resistance was significantly greater in K. pneumoniae (p<0.05) than in E. coli (see above).
Impact of the new carbapenem breakpoints
When the new CLSI carbapenem breakpoints were applied, imipenem-cilastatin susceptibility, in contrast to ertapenem susceptibility, was substantially decreased for P. mirabilis (24% vs. 96%, respectively) and Morganella morganii (15% vs. 92%, respectively), as most of the isolates had imipenem-cilastatin MICs in the 2–4 mcg/mL range (P. mirabilis 73.2% [52/71] and M. morganii 84.6% [11/13]). This is in accordance with SMART data globally. The SMART database for P. mirabilis and M. morganii from 2004–2009 excluding South Africa revealed that 58.5% (889/1,519) of M. morganii isolates had imipenem-cilastatin MICs of 2 or 4 mcg/mL, which was defined as susceptible with the old imipenem-cilastatin breakpoint, whereas only 2% (15/750) of isolates that had been susceptible to ertapenem with the old breakpoint became non-susceptible. Similarly, 58.5% (889/1,519) of P. mirabilis isolates had imipenem-cilastatin MICs of 2 or 4 mcg/mL, representing resistance, whereas only 1% (15/1,519) had their ertapenem susceptibility reclassified as non-susceptible by the new breakpoints. However, ertapenem susceptibility was significantly reduced in ESBL-positive E. coli compared with ESBL-negative isolates (39/43 [91%] vs. 513/523 [98%]; p<0.05), although this did not apply to imipenem-cilastatin (41/43 [95%] vs. 517/523 [99%]; p=0.0928). Among the small number of isolates, the activity of ertapenem decreased in ESBL-positive P. mirabilis compared with ESBL-negative isolates (6/8 [75%] vs. 62/63 [98%]; p<0.05). Of note, the difference in susceptibility to ertapenem in ESBL-producing K. pneumoniae vs. non-producing isolates was not significant (49/56 [88%] vs. 75/80 [94%]; p=0.2317).
Multi-drug resistance
Multi-drug resistance (Table 4) was significantly more prevalent in K. pneumoniae overall (38/136 [27.9%]) than in E. coli (28/566 [4.9%]; p<0.0001) and P. mirabilis (3/71 [4.1%]; p<0.05). The highest MDR rate was recorded for A. baumannii (26/34 [76.4%]) followed by ESBL-producing K. pneumoniae and E. coli, with 60.7% (34/56) and 41.7% (18/43) of isolates, respectively, being resistant to three or more classes of drugs. Only 5.0% (4/80) and 1.9% (10/523) of ESBL non-producing K. pneumoniae and E. coli, respectively, were MDR, indicating the presence of resistance mechanisms other than ESBL production alone. There was a trend toward more MDR in K. pneumoniae than E. coli ESBL producers (p=0.0710). Also, 22.7% (35/154) of P. aeruginosa strains and 14.8% (12/81) of the E. cloacae and E. aerogenes isolates (assessed together) were MDR, which did not differ significantly from K. pneumoniae. None of the isolates of K. oxytoca (n=35) or Serratia marcescens (n=20) was resistant to three or more antibiotic classes.
Defined as resistant to at least three of the following antibiotic classes: aminoglycosides (amikacin), cephalosporins (ceftriaxone, ceftazidime, cefotaxime, cefepime), fluoroquinolones (ciprofloxacin, levofloxacin), β-lactam/β-lactam inhibitor (ampicillin-sulbactam, piperacillin-tazobactam), or carbapenems (ertapenem, imipenem-cilastatin).
ESBL=extended-spectrum β-lactamase.
Discussion
Considerable resistance to one, or in many cases, multiple antibiotics that are prescribed commonly for IAIs in South Africa was documented in this six-year surveillance study. Notably, ESBL production in E. coli, the species isolated most commonly, was 7.6% vs. 41.2% in K. pneumoniae. In both instances, this feature compromised susceptibility significantly. The exception was ertapenem, which was the most active antibiotic despite reduced activity against ESBL-positive E. coli and P. mirabilis when using the new CLSI carbapenem breakpoints. In contrast, there was no significant difference in ertapenem resistance between ESBL-positive and -negative K. pneumoniae strains. The large disparity in susceptibility between ertapenem and imipenem-cilastatin in P. mirabilis and M. morganii was attributable to the CLSI breakpoint changes, as most of these species have imipenem-cilastatin MICs in the 2–4 mcg/mL range, which is now regarded as resistant. Even though the breakpoint for ertapenem was lowered even more drastically, to 0.25 mcg/mL, most isolates had MICs much lower than that and therefore remained in the susceptible range. In most studies, P. mirabilis accounts for <5% of all GNB isolated in cIAIs, and data on the ESBL rates and associated resistance are limited. The only previous reports are from Hawser et al. (Europe) [5] and Yang et al. (China) [12], where 5.4% and 19.5% of isolates, respectively, were ESBL-positive and did not impact ertapenem resistance data. In our study, P. mirabilis was the fourth most common GNB, with 11.3% being ESBL producers and 4.1% MDR. Whereas amikacin was the second most active antibiotic overall, susceptibility to this drug was negatively affected by ESBL production in Enterobacteriaceae. Ampicillin-sulbactam, which is not available in South Africa, was the least active agent in vitro. Although the data presented here are consistent with previous reports linking ESBL-producing phenotypes to decreased therapeutic options for IAIs, the differences in susceptibility between ESBL producers and non-producers were relatively small for the carbapenems compared with most other agents [5,7,8,15].
According to the results of this study, K. pneumoniae is substantially more problematic from an antibiotic management point of view in South Africa than is E. coli, which tends to feature more prominently in the international surgical literature on cIAIs, as well as in the other SMART studies [3,4,7–9,15]. Not only did K. pneumoniae have the highest ESBL rate, but it also had the highest MDR rate among the Enterobacteriaceae, which overall was second only to A. baumannii and exceeded the MDR rate of P. aeruginosa isolates. This result affected significantly the susceptibility to the cephalosporins but had no impact on susceptibility to aminoglycosides and fluoroquinolones compared with ESBL phenotypes of E. coli. The CTX-M ESBLs, in conjunction with porin loss, in K. pneumoniae influences carbapenem susceptibility in South Africa, but paradoxically, the impact on ertapenem (and imipenem) was not significant in K. pneumoniae as opposed to E. coli and P. mirabilis [16,17]. Klebsiella pneumoniae has always had a unique role as an etiologic agent of infections in South Africa, particularly in community-acquired pneumonia [18–20]. In addition, during a recent six-month blood culture survey in the same hospitals involved in the present study, K. pneumoniae (n=548) was isolated more frequently than E. coli with 50% of bacteremic isolates producing an ESBL as opposed to only 5% of E. coli (n=503) [21]. Globally, ESBL rates (SMART) for E. coli and K. pneumoniae are 17.0% and 22.3%, respectively. The reasons for the discrepant ESBL production in cases of bacteremia and cIAIs, as documented in this study (7.6% vs. 41.2%), are unknown.
There are a number of limitations of this study, including the fact that no microbiological or clinical outcomes were recorded. Although appropriate empiric antibiotic use increases survival and shortens hospital stay, clinical outcome does not necessarily reflect in vitro susceptibility in cIAIs, as appropriate surgical procedures also are vital [22]. Furthermore, prior antibiotic use and risk factors for the different gram-negative organisms, including the ESBL producers and MDR pathogens that were isolated, were not determined; and it was not possible to differentiate community-acquired from hospital-acquired cIAIs. With regard to the latter, only SMART in the United States (13.3%) had an equivalent number of P. aeruginosa (12.6%), which usually accounts for <10% of all gram-negative organisms isolated in cIAIs [6,8]. The frequency of more resistant pathogens such as P. aeruginosa and ESBL-producing enteric bacteria including Proteus spp. in our study probably reflects a greater number of healthcare-associated cIAIs [15,23,24]. Additionally, although three of South Africa's largest cities were involved and surveillance included only private hospitals, the results might not apply to smaller centers or public hospitals. To help redress this deficiency, an additional site was recruited in 2011, and whether any differences exist should become apparent soon. Lastly, this report does not contain molecular characterization of the ESBLs and carbapenem-resistant Enterobacteriaceae, which in the future will be important epidemiologically. Substantial fluoroquinolone resistance is associated increasingly with CTX-M-type ESBLs as opposed to SHV or TEM phenotypes, and this may be the case here [4,8,25,26].
Although piperacillin-tazobactam and cefepime retained 89.3% and 86.8% activity, respectively, against all GNB in this study, these agents are not suitable for the empirical treatment of cIAIs when high ESBL rates (10%–20%) are present among the Enterobacteriaceae (inferred from Solomkin et al.) [15]. According to the results of this study, piperacillin-tazobactam probably would be the best choice for the empirical treatment of suspected pseudomonal cIAIs, which are more common in nosocomial infections, such as tertiary peritonitis [23,24]. Imipenem-cilastatin, with 87.1% activity inclusive of ESBL-producing Enterobacteriaceae and P. aeruginosa, probably should be reserved for nosocomial infections. Regarding the latter pathogen, imipenem-cilastatin in combination with another agent such as a fluoroquinolone or amikacin may be necessary, whereas ertapenem would be best suited for empirical monotherapy of community-acquired cIAIs in South Africa.
This study documents the evolution of antibiotic resistance among intra-abdominal GNBs in South Africa. It highlights the fact that application of the new CLSI breakpoints results in discrepancies between reported ertapenem and imipenem-cilastatin susceptibilities and the need for continued surveillance to monitor both the ESBL prevalence and the rate of MDR, as this may affect empiric antibiotic choice and outcome in cIAIs.
Footnotes
Acknowledgments
The authors thank the following investigators in South Africa: S. van der Linde and M. Pfister (Ampath, Johannesburg); D. Hari-Makkan (Ampath, Pretoria); and S. Lalloo, J. Saayman, M. Viljoen, and L. le Grange (Pathcare, Cape Town).
Author Disclosure Statement
The study was sponsored by Merck & Co., Inc. Doctor Brink has received recent research funding from Merck and Sanofi-Aventis and has served on speaker's bureaus for Merck, Pfizer, Sanofi-Aventis, and Janssen Pharmaceuticals. Doctor Senekal has acted on the advisory boards of Merck, Pfizer, Janssen-Cilag, and Aspen GSK. R. Badal is employed by IHMA, Inc., which receives funding from Merck & Co., Inc. to manage the SMART program. Dr. Grolman has served on the advisory boards or speaker bureaus for Sanofi-Aventis, Pfizer, Wyeth, Janssen-Cilag, Astra-Zeneca, and Roche. Doctor Richards has served on the speaker's bureau of and/or received funding for congress travel from Sanofi-Aventis, Pfizer, Merck and Co., Inc. and Bristol-Myers Squibb, Astra-Zeneca, Roche, Winthrop, Aspen, Bayer, GlaxoSmithKline (GSK), Janssen, Fresenius Kabi, and Abbott. Doctor Feldman has acted on the advisory board or received honoraria for lectures or assistance for congress travel from the following companies in relation to antibiotics they manufacture or market: Abbott, Merck, Aspen–GSK, Pfizer, Cipla, AstraZeneca, and Sanofi-Aventis.