
Abstract
Abstract
Background:
Catheter-related blood stream infections (CR-BSIs) are estimated to occur in 80,000 patients in intensive care units (ICUs) each year in the United States. We sought to determine the clinical utility of vascular catheter cultures in critically ill patients with suspected CR-BSI.
Methods:
We reviewed retrospectively all positive (≥15 colony forming units/roll) vascular catheter tip cultures (CTCs) documented over a four-year period in the ICUs of two hospitals. A CR-BSI was defined as matching positive blood and catheter cultures. The time interval between catheter removal and blood culture was recorded.
Results:
A total of 1,391 CTCs were obtained, of which 468 (34%) were positive and 143 (31% of the positive cultures) were associated with a diagnosis of CR-BSI. In 133 of these 143 cases (93%), the positive blood culture was obtained before or within 24 h after catheter removal and dictated antibiotic therapy. In only 10 of 143 cases (7%) did catheter removal and culture significantly (>1 day) precede the positive blood culture. In 55% of the CR-BSI cases, the catheter was removed empirically and close to the time of blood culture (−1.3±19.0 h). In the remaining 45%, the catheter was removed clinically (after a blood culture was positive), and this action was more remote in time (23.6±19.4 h; p<0.001 vs. empiric removal). Total microbiology laboratory costs for the CTCs were $75,300, and 600 microbiology technician hours were required.
Conclusion:
In an ICU patient population, only about one-third of vascular catheter cultures were positive, and only about one-third of the positive CTCs were associated with CR-BSI. Ninety-three percent of all CR-BSIs were identified by bacteremia either before or coinciding with catheter removal, and the results of the blood culture dictated antimicrobial therapy. Because CTCs rarely changed therapy, they may not be appropriate in the management of suspected CR-BSI in the ICU setting.
For CR-BSI management, catheter removal and antibiotics are recommended. In addition, specific antibiotic therapy is not required for positive CTCs in the absence of bacteremia [5], although a recent clinical practice guideline recommends treating patients with Staphylococcus aureus catheter colonization even in the absence of bacteremia [6,7]. Although it is recommended that CTCs not be obtained routinely, these same guidelines and others recommend that such cultures be performed when a catheter is removed for suspected CR-BSI [6,8,9].
In clinical practice, bacteremia with any known pathogen will necessitate a course of antimicrobial therapy, regardless of the CTC results. It has been our experience that in critically ill patients with bacteremia, the microbiologic status of appropriately removed catheters rarely alters clinical management. We therefore sought to determine the clinical utility of vascular catheter cultures in critically ill patients with suspected CR-BSI.
Patients and Methods
Subjects and study design
This study was approved by the Human Investigation Committee/Institutional Review Board of Wayne State University School of Medicine. The subjects were adult patients in the ICUs of Harper University Hospital (HUH) and Detroit Receiving Hospital (DRH) of the Detroit Medical Center. The former is a 470-bed tertiary-care university hospital with four mixed medical–surgical ICU units totaling 40 beds. The latter is a 340-bed Level 1 urban trauma center with four ICU units: Trauma, neurotrauma, medical, and burn, totaling 46 beds. The study period was from January 1, 2006, through December 31, 2009. Computerized records from the microbiology laboratory retrospectively identified all vascular CTCs from this patient cohort. The electronic medical records of these patients were reviewed to collect all other pertinent culture and antibiotic use data.
Microbiology techniques
Catheter tip and blood specimens
Catheter tips were obtained primarily by nurses and sent to the microbiology laboratory in sterile containers. Blood samples were drawn almost exclusively by the nursing staff, as a dedicated phlebotomy team is not used in the ICUs of these hospitals. Blood cultures were obtained both from central venous and arterial access catheters, as well as from peripheral veins.
Specimen processing
All CTCs were processed using the semi-quantitative roll-plate technique of Maki et al. [10]. Trypticase soy blood agar (5% sheep blood) plates were used. Colony growth was counted between 24 and 48 h. Specific inhibitors were not used during culture of antibiotic/antiseptic-coated catheters. Most multi-lumen central venous catheters were advanced-generation silver sulfadiazine/chlorhexidine-coated. Standard aerobic and anaerobic blood culture bottle sets were used, and positivity was assessed qualitatively. Blood was incubated for five days before being described as negative; seven days for fungal blood cultures. For all positive catheter tip and blood cultures, organism identification and susceptibility testing followed using standard microbiologic methodologies. Our blood culture contamination rates ranged from 1.4% to 2.6% during the study period.
Definitions
The CTCs were classified as negative (no growth), contaminated (<15 colony-forming units [CFU] by the semi-quantitative roll-plate technique), or positive (≥15 CFU/roll). A CR-BSI was defined microbiologically as a positive CTC and a matching positive blood culture obtained as much as 96 h before or up to 48 h after catheter removal. A blood culture set consisted of two bottles, one aerobic and one anaerobic. One positive blood culture from any number of bottles or sets was considered meaningful for all pathogens except coagulase-negative Staphylococcus. For this organism, at least two positive bottles from either one or two sets of blood cultures were required to confirm bacteremia and reduce the chance of a false-positive culture (reflecting a contaminant).
Overall, clinical documentation was deemed inadequate to ensure the accuracy of the source of all blood cultures as coming from suspected infected catheters, other catheters, or peripherally. Therefore, this information was not used in the definitive diagnosis of CR-BSI, and all blood cultures were considered equally significant in establishing or ruling out the diagnosis of CR-BSI. Medical records were not reviewed for clinical appropriateness of the diagnosis of CR-BSI. Antibiotic therapy was deemed appropriate if the causative organism of the CR-BSI was susceptible to the antibiotic used and the antibiotic was administered within 24 h of the positive blood culture. Therapy was deemed inadequate if the causative organism was not susceptible to the antibiotic used, if antibiotic was delayed beyond 24 h of the positive blood culture, or if no antibiotic was given.
Because all cultures are time-stamped at the time of collection and positivity/clinician notification, time intervals between catheter removal and blood cultures (time obtained and time positive) could be calculated. Catheter removal was considered empiric if the catheter was removed before the blood culture results were positive, and the time interval was defined as the time of the blood sampling to the catheter being removed and cultured. Catheter removal was considered clinical if the catheter was removed only after the identification of a positive blood culture and the time interval was from the time of blood culture positivity/notification to catheter removal and culture.
Microbiology costs
Unit laboratory costs, technician time, and labor costs were determined for catheter specimen processing, organism identification, and susceptibility testing. The cost of a CTC was $15, identification of a single bacterium cost $13, and antibiotic susceptibility testing cost $15 per organism. The technician time was 15 min for the CTC and 10 min each for bacterial identification and susceptibility tests. These unit costs were applied to the total cohort of catheters processed, taking into account the number of organisms identified and their subsequent susceptibility testing.
Data presentation and statistical analysis
Data are presented as descriptive, percentages, and mean±standard deviation. Comparison between groups utilized either the chi-square test or an unpaired Student t-test. A p value of ≤0.05 was considered statistically significant.
Results
A total of 1,391 CTCs were obtained during the study period. Catheter tips cultured included those of multi-lumen central venous catheters (antibiotic-coated), peripherally inserted central catheters, hemodialysis catheters, pulmonary artery catheters, venous and arterial sheaths, and arterial catheters. Clinical documentation often was lacking or obviously inaccurate as to catheter type, catheter removal versus guidewire exchange (which is strongly discouraged by hospital policy), and the specific venous or arterial site (i.e., subclavian, internal jugular, femoral). This and the retrospective nature of our study prevented correlation of any culture results with the anatomic sites of catheterization. According to our clinical experience in these ICUs, the majority of catheters were central venous and were placed in the upper body. Over the study period, central-line catheter utilization ratios (central-line days/patient days) ranged from 0.56 to 0.80 at HUH and 0.43–0.75 at DRH with no significant trends by unit or by year. Central line-associated BSI rates in the ICUs of the two hospitals over the study period ranged from 0.8 to 6.3/1,000 central line days.
The distribution of negative, contaminated, and positive CTCs is shown in Figure 1. There were 143 cases of CR-BSI, representing 10.3% of the total CTCs and 31% of the positive CTCs. By comparison, hospital epidemiology surveillance records showed 169 cases of clinically confirmed CA-BSI in this patient cohort.
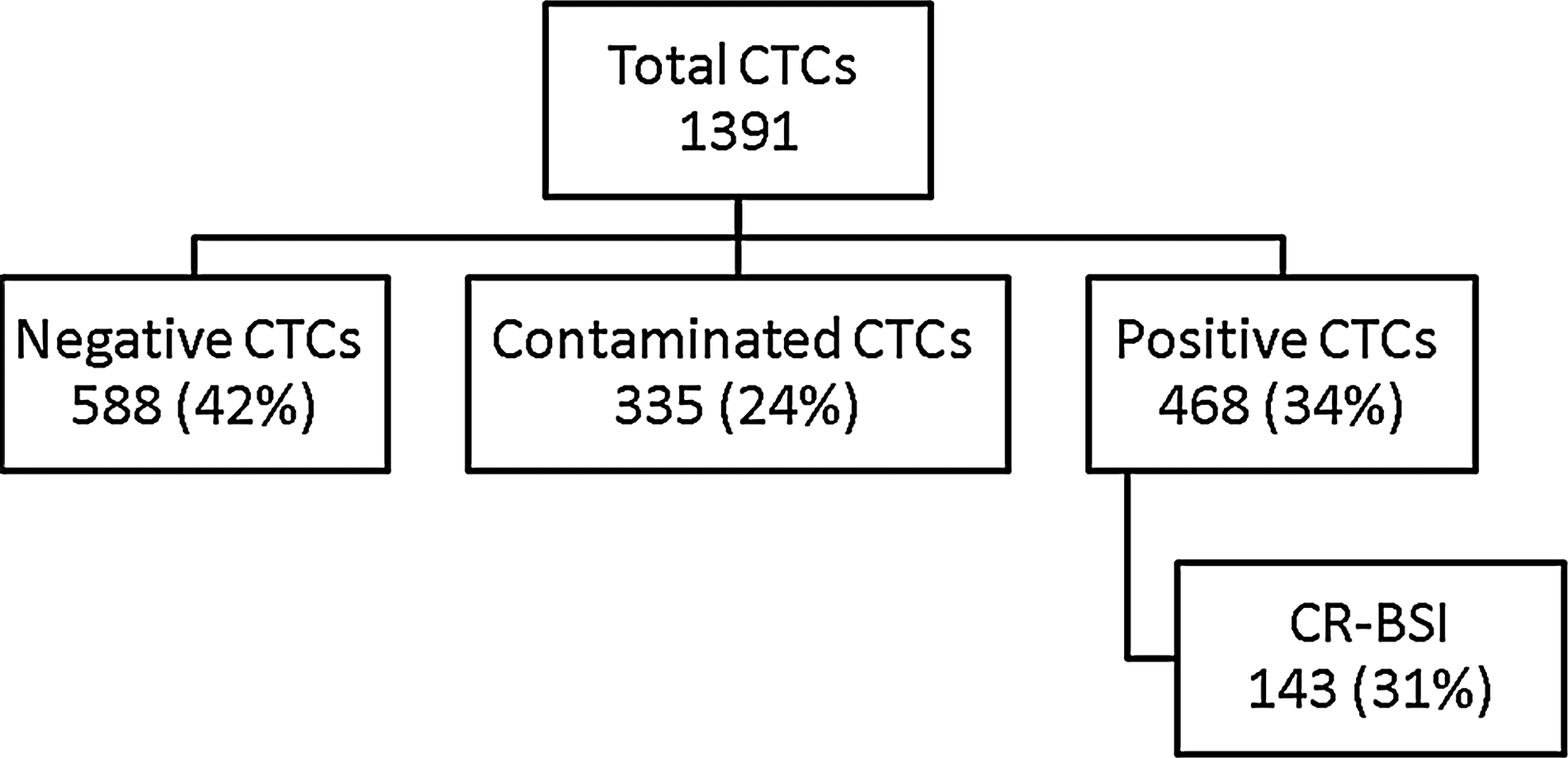
Microbiologic distribution of catheter tip cultures (CTCs).
In 133 of the 143 cases of microbiology-identified CR-BSI (93%), the positive blood culture was obtained before or within 24 h after catheter removal and dictated appropriate antibiotic therapy. In only 10 of 143 cases of CR-BSI (7%) did catheter removal and culture precede the positive blood culture by >24 h. Antibiotic therapy was deemed appropriate in 126 of 143 cases of CR-BSI (88%).
In 55% of the patients with a CR-BSI, the catheter was removed empirically and close to the time of the blood culture (−1.3±19.0 h) (Table 1). In the remaining cases, the catheter was removed after a blood culture was positive, and these removals took place later (23.6±19.4 h; p<0.001 vs. empiric removal). In only 32 of 143 cases (22%) was the catheter removed either empirically or clinically within a±4-h window of the positive blood culture.
Mean±standard deviation. Negative time interval for the empirical removal group indicates that catheter was removed before blood culture became positive.
P=0.16 versus clinical by chi-square test.
P<0.001 versus empiric removal by unpaired Student t-test.
The microbiology findings of positive CTCs and CR-BSIs are shown in Table 2. The most common organisms in positive CTCs and causing CR-BSI were gram-positive cocci. Gram-negative bacilli were the second most common. Twenty-three percent of positive CTCs had growth of two or more organisms at ≥15 CFU/roll.
Based on 738 organisms cultured from 468 positive CTCs.
Based on 150 organisms in 143 cases.
Percentages for CTC are based on total number of cultures. The CR-BSI percentage is based on positive CTCs.
In only 24 cases (5% of the positive CTCs; 1.7% of all CTCs) was S. aureus identified in the confirmed absence of bacteremia. Twenty (83%) of these patients had been started on vancomycin or daptomycin prior to the index colonized catheter being removed. Eighteen of these patients (75%) were in the burn ICU.
The microbiology laboratory costs for the 1,391 CTCs, including specimen processing, organism identification, and susceptibility testing, were approximately $75,300; and 600 microbiology technician hours were required.
Discussion
It has been well accepted that positive vascular CTCs are required for the definitive microbiologic diagnosis of CR-BSI [2,3]. Current clinical guidelines recommend that catheter cultures be performed when a catheter is removed for suspected CR-BSI [6,8,9]. However, recent changes in the epidemiologic or surveillance diagnosis of CR-BSI no longer require a matching positive CTC [4]. Notwithstanding the epidemiologic significance of CTCs, we have questioned the clinical utility of this practice. It has been our impression that it is rare for positive or negative CTC results to alter antimicrobial therapy when bacteremia has been identified. To test this hypothesis, we reviewed all vascular CTCs over a four-year period in a large mixed population of critically ill patients in two hospitals to determine the clinical usefulness of CTCs in the management of suspected CR-BSI.
Most positive CTCs (69%) were not associated with a microbiologic diagnosis of CR-BSI. Of all the CTCs, only 10% were associated with a diagnosis of CR-BSI. More importantly, of the 143 cases of microbiology-identified CR-BSI identified over the study period, 133 (93%) had the positive blood culture inside a 24-h period, mostly before or after the removal of the index-positive CTC, and dictated appropriate antibiotic therapy. Therefore, it was rare for any antimicrobial therapy to be dictated solely by the CTC results; in fact, appropriate antimicrobial therapy almost always was dictated by the previously obtained blood cultures. In 12% of cases of CR-BSI, antibiotic therapy was deemed inadequate, either because of delay in starting an antibiotic or use of an incorrect antibiotic. This pattern likely reflects the common practice of obtaining blood cultures as part of the workup for systemic infection but removing and culturing catheters for suspected CR-BSI only once bacteremia is documented. Although one may question this common practice, it is clinically reasonable not to remove catheters too quickly, as they usually are difficult to replace and needed, and CR-BSI rates generally are low, at a pooled mean of 5/1,000 catheter days in the ICU [11].
Catheters that were associated with CR-BSI were removed and cultured in one of two situations: Empirically, when blood culture results were pending, or clinically, after blood culture results were known to be positive. In our study, catheter removal and culture was slightly more often done empirically (55%). As expected, under empiric conditions, the blood culture was obtained close to the time of catheter removal. However, we were surprised to see that under clinical conditions, the catheter was removed, on average, nearly 24 h after the blood culture became positive and therefore 36–48 h after the blood had been drawn for culture. There may be several reasons for this, including a higher suspicion or knowledge of other sources of bacteremia, lack of adequate suspicion for CR-BSI, or delay in removal. Our study was not designed to differentiate among these possibilities.
The prevalence of specific microorganisms present on positive CTCs and responsible for CR-BSI closely paralleled published data [12]. This also was true for the relative risk of specific microorganisms being responsible for CR-BSI.
Clinical guidelines issued recently by the Infectious Diseases Society of America recommend that a vascular CTC with S. aureus should lead to a course of antimicrobial drug even in the absence of bacteremia [6]. Although this has not been done routinely, and positive CTCs in the absence of bacteremia generally have been considered to be treated adequately by catheter removal alone, recent data from a general hospital patient population suggest that these patients have a high rate of subsequent bacteremia and that therapy significantly decreases the incidence of this complication [7]. Another recent study of isolated positive CTCs in an ICU patient population indicated that the rate of subsequent bacteremia is low, but a more specific quantitative catheter culture technique was used, so the data cannot be compared directly [13]. In our cohort of critically ill patients, we found only 24 cases of S. aureus-positive CTCs in the documented absence of bacteremia. This represented only 5% of all positive CTCs and 1.7% of all CTCs. In terms of its clinical relevance, 20 of these 24 patients (83%) were already receiving appropriate antimicrobial agents prior to catheter removal. More research will be needed to determine the appropriate management of isolated positive CTCs and whether the findings will justify more widespread catheter culturing.
Cost, including materials and labor, for the 1,391 CTCs in our study cohort was $75,300, and 600 microbiology technician hours were required to support the diagnosis of 143 cases of CR-BSI. If we extrapolate these numbers to the estimated 80,000 ICU CR-BSIs per year in the United States, this would translate into $33.3 million and 342,000 technician hours per year. Extrapolation of these data to the estimated 250,000 total cases of CR-BSIs per year would produce even greater numbers.
We acknowledge that there may be a limited clinical role for CTCs in the workup of a potentially infected or bacteremic critically ill patient. First, a negative CTC can rule out the catheter as a source of infection and focus attention on other sources. However, most non-catheter sources of infection that lead to bacteremia are easily suspected and not difficult to diagnose. In addition, because CR-BSI rates are so low, clinicians always must evaluate patients for other potential sources of bacteremia. In addition, the clinical confusion added by positive and contaminated CTCs, not uncommonly having multiple organisms, is very real. It is for these reasons, along with the limited clinical utility and substantial costs associated with CTCs, that we do not advocate a liberal catheter culturing policy. A prospective study would be required to make a more definitive statement regarding whether catheter tips should, in fact, not be cultured at all. The overall trend in our study was to adopt a more conservative policy of culturing catheters only when the suspicion of CR-BSI was reasonably high, as there was rarely a change in treatment on the basis of the CTC results if bacteremia already had been identified.
There are some important limitations to our study. We used a retrospective microbiologic diagnosis of CR-BSI, as evidenced by matching CTC and blood cultures, without clinical assessment to rule out other, non-catheter sources of the bacteremia. This, combined with utilizing all blood cultures, both peripherally and catheter drawn, likely overestimated the true incidence of CR-BSI. Unfortunately, documentation was inadequate to determine the source of many blood cultures. On the other hand, we did not identify cases of CA-BSI in those patients with bacteremia without a non-catheter source when there was a negative, contaminated, or no CTC. Our methodology did not allow us to determine the precise number of cases of CA-BSI in our patient population, but hospital epidemiologic reporting documented 169 cases compared with the 143 cases we identified. It has been shown recently that CA-BSI rates significantly overestimate the true incidence of CR-BSI, and those authors recommend culturing all CTCs, despite the cost [14]. Our study shows that nearly all patients (93%) could have been treated appropriately on the basis of the blood culture and that the CTC only confirmed the absolute definition of CR-BSI. Finally, our study had limitations caused by inadequate clinical documentation. These limitations included our inability to differentiate between central venous and arterial catheters, to determine the anatomic site of catheter insertion, and to discover which central venous catheters were antibiotic coated. The literature does note that the incidence of arterial CR-BSI is lower than that associated with central venous catheters and that anatomic insertion sites and antibiotic coating play a role in infection [2,15]. However, our study was not intended to evaluate these relations.
Despite these limitations, the data from this large, clinically relevant and oriented retrospective two-center study lead us to question seriously the long-standing dogma that CTCs are necessary in the clinical diagnosis of CR-BSI and, more importantly, in the management of critically ill patients with suspected CR-BSI.
Conclusions
In an ICU patient population, only about one-third of vascular catheters cultured were positive for meaningful bacterial colonization, and only about one-third of the positive CTCs were associated with CR-BSI. The majority (93%) of CR-BSIs were identified by the finding of bacteremia prior to or coinciding with catheter removal, which dictated antimicrobial therapy. Because CTCs rarely contributed to the clinical management of bacteremia, our data suggest that vascular catheter cultures may not be required in suspected CR-BSI in the ICU setting.
Footnotes
Acknowledgments
Special thanks to Theresa Painter, MA, MT (ASCP), Microbiology Supervisor, University Laboratories, Detroit Medical Center, for her assistance in compiling catheter tip culture data.
Author Disclosure Statement
We certify that we have all participated sufficiently in the work to take public responsibility for the appropriateness of the experimental design and method and the collection, analysis, and interpretation of the data. We have no financial conflicts to disclose.