
Abstract

A 50-year-old patient with 64% total body surface area (TBSA) burns resulting from an explosion and fire had a complicated hospital course. Inhalation injury was documented by pulmonary medicine evaluation within 24 h of admission. He developed ventilator-dependent respiratory failure and pan-sinusitis. An echocardiogram demonstrated a patent formina ovalis. Thirteen ring-enhancing brain abscesses were noted on computed tomography scan on the 25th post-burn day. Magnetic resonance imaging confirmed the diagnosis of brain abscesses (Fig. 1), and surgical drainage directed the selection of antifungal therapy. Intraoperative culture demonstrated Staphylococcus aureus and P. boydii. These abscesses were treated initially with an echinocandin, but echinocandins are not effective against P. boydii; and abscess culture directed treatment with voriconazole. The patient recovered after long-term intravenous and then oral antifungal therapy.
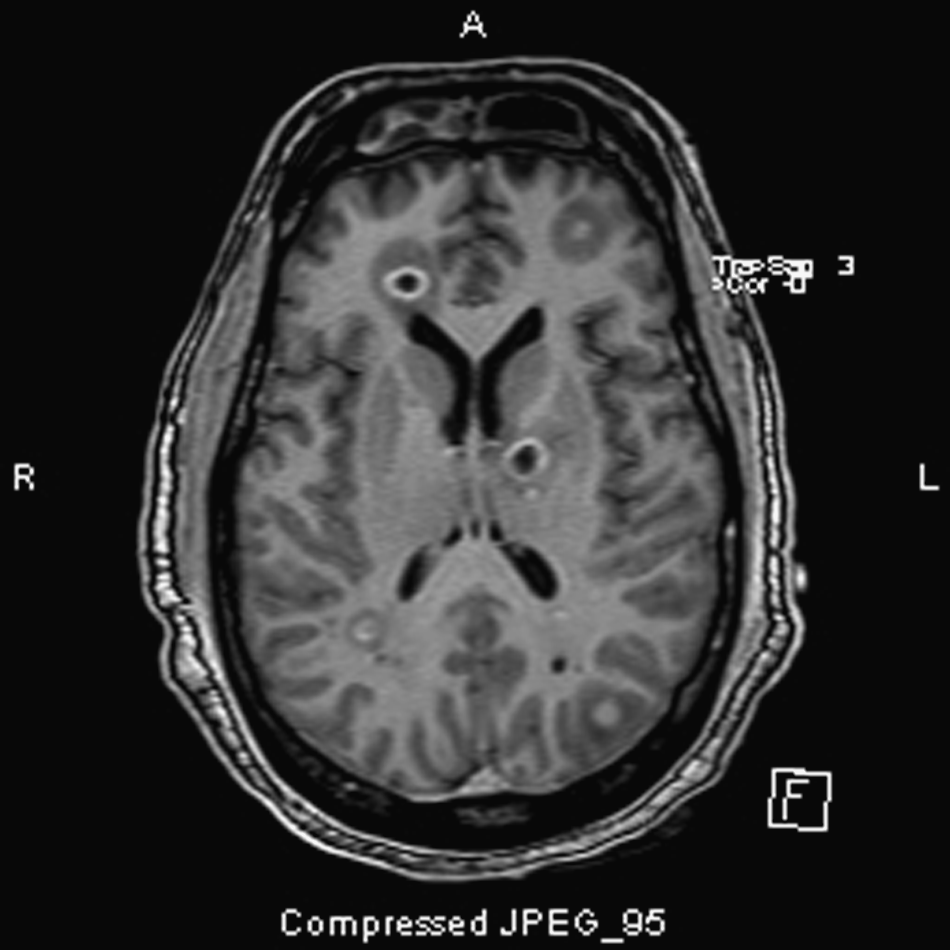
Two views of fungal abscesses revealed by magnetic resonance imaging.
Most central nervous system P. boydii infections occur in patients with predisposing conditions, immunosuppression, near-drowning, or trauma [1]. Chronic sinusitis may predispose individuals to infection with Aspergillus species and other filamentous fungi [2]. Multiple fungal isolates in broncheoalveolar lavage liquid, as was seen in this patient, are common in patients with chronic rhinosinusitis [3]. Fungal brain abscesses have been associated with a patent foramen ovale, as was noted in this patient [4]. Between 18% and 27% of persons in the community have this often-benign cardiac anomaly [4].
The importance of isolating P. boydii with aggressive drainage of brain abscesses cannot be overstated, as on the basis of bronchoalveolar lavage, the presumptive infecting organism was Aspergillus fumagatus [5]. Antifungal therapy directed exclusively at A. fumagatus would have resulted in treatment failure and possibly death.