
Abstract

Axial contrast-enhanced computed tomography scan of the lower extremities demonstrating a pseudoaneurysm of the left femoral artery prior to coil embolization.
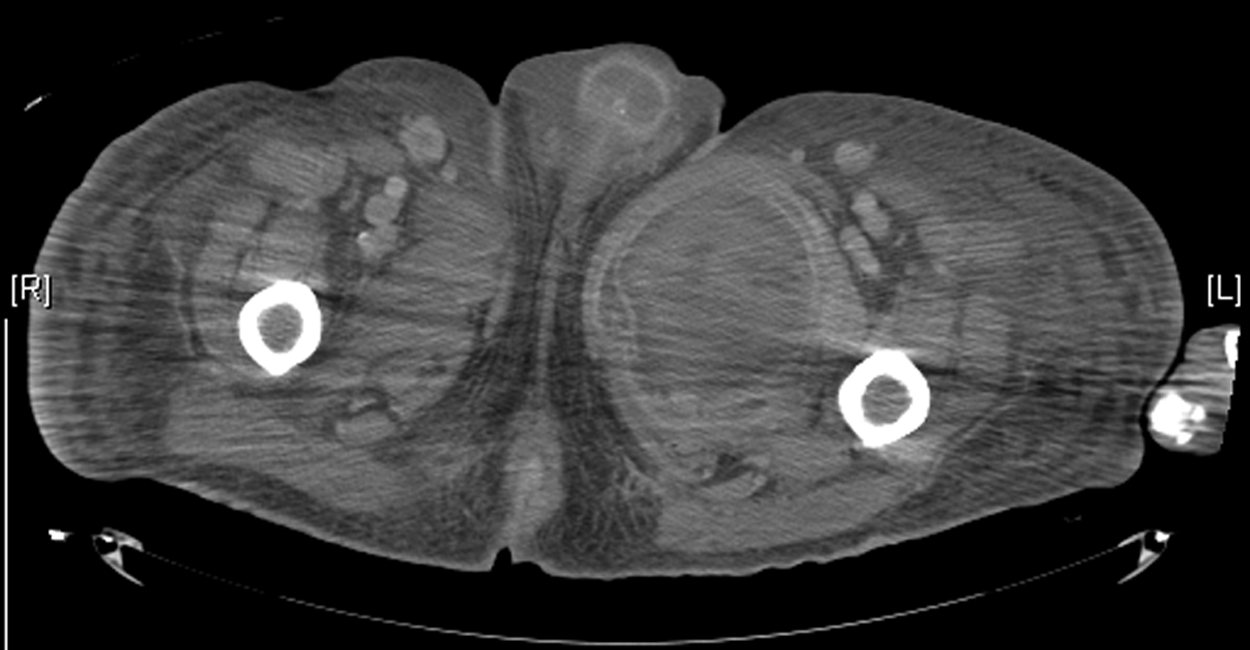
At 3 months after embolization, and having been well during this interval, the patient developed pain and an enlarging, tender mass in his left thigh. His vital signs were normal and his white blood cell count was 15,200 cells/mm3. A CT scan was notable for a 12.8x13.7-cm cavitary mass of the left groin that contained gas, fluid, and a foreign body consistent with a vascular coil (Fig. 2). Piperacillin–tazobactam was administered before surgical drainage and debridement of an infected clot and multiple vascular coils. Culture of the clot and hardware demonstrated E. coli with antibiotic susceptibilities identical to those of the prior isolates. Postoperatively the patient was treated with local wound care and piperacillin–tazobactam.

Axial contrast-enhanced computed tomography scan of the lower extremities demonstrating an abscess containing an air-fluid level and a foreign body. The abscess measured 13.7 cm by 12.9 cm.
Pseudoaneurysms occur after 0.1%–0.2% of diagnostic angiograms and 3.5%–5.5% of interventional procedures [1]. Pseudoaneurysms <2 cm usually resolve without intervention; larger or symptomatic pseudoaneurysms may require treatment, such as compression, ultrasound-guided thrombin injection, or ECE (especially for larger lesions), which is being used increasingly.
No prospective randomized trial has examined the role of antibiotic prophylaxis for ECE, but reports of infected coils are few [2]. Falagas et al. reviewed seven cases of ECE that were complicated by infection, with intervals between the procedure and infection ranging from 10 days to 3.5 years [2]. The most common presentation was abscess (85.7% of cases). Of the seven cases reviewed, three had infections caused by Staphylococcus aureus; other pathogens included Salmonella spp., Staphylococcus epidermidis, E. coli, and Bacteroides fragilis. Owing to the paucity of reports, conclusive association of risk factors with infection of endovascular coils is impossible. Two putative mechanisms of coil infection are probable: Introduction of an infecting organism during coil placement or hematogenous seeding of an endogenous pathogen.
Historically, a higher incidence of transient bacteremia is recognized after embolization of endovascular coils than with diagnostic angiography, although the relevance is unknown [3]. Routine prophylaxis for ECE is controversial; when used, prophylaxis is targeted against skin pathogens. We suspect that our patient developed infection of an ECE and his pseudoaneurysm sac as the result of transient bacteremia from a colonized urinary tract or as a residuum of his paraspinal abscess. In theory, coil-related pseudoaneurysms become isolated from the circulation and should create a low risk for hematogenous seeding [4]; however, loose packing of the aneurysm may lead to failure of the formation of fibrinous neoendothelium [5] and allow colonization or infection by hematogenous seeding.
Treatment of infected coils must be individualized. If the abscess can be drained and the coil can be removed, this is the preferred option for controlling the source of the infection. However, case reports have described intracranial coil-related abscesses that have been treated successfully with antibiotics [2]. If explantation is impossible because of the location or position of coils, prolonged administration of high-dose antimicrobial agents may be necessary.