
Abstract
Abstract
Background:
Management of an infected groin wound after vascular surgery may be a challenge. We report a retrospective series of cases of the management of groin defects and an algorithm for their management based on our own experience and related literature.
Patients and Methods:
We conducted a retrospective chart review from June 2008 to February 2012 of patients with infected groin wounds after vascular surgical procedures. The review disclosed six patients with a history of femoral cannulation or extracorporeal membrane oxygenation (ECMO), one patient with a femorofemoral bypass, one patient with an intra-aortic balloon pump (IABP), and one patient with a thoracoabdominal aneurysm following stent implantation. Exposure of femoral vessels was noted in seven of these nine patients, and wound cultures of all nine patients yielded positive results.
Results:
The mean age of the nine patients (five males and four females) was 54.6 years (range 17–79 years). The mean follow-up was 13.6 months (range 8–30 months). Four of the patients were treated with a pedicled gracilis flap; one with a local flap; one with a myocutaneous flap of the anterolateral thigh (ALT) combined with a partial tensor fascia lata (TFL) flap; one with primary closure; and two with a myocutaneous island pedicle flap of the ALT. No donor-site complications were noted. There was partial skin cyanosis in the patient treated with a myocutaneous flap of the ALT combined with a TFL flap, which resolved after one week. The scheduled follow-up of the patients showed that all of their groin wounds had healed well.
Conclusions:
A pedicled flap of gracilis muscle is an ideal and effective option for covering infected groin wounds of <10 cm with exposure of femoral vessels. According to a literature review, a sartorius muscle flap is another option for accomplishing this. A myocutaneous island flap of the ALT is indicated for infected groin wounds >10 cm with exposure of femoral vessels. The literature indicates that myocutaneous flaps of rectus abdominis (RA) muscle and flaps of rectus femoris (RF) muscle are also suitable for groin wounds larger than 10 cm. Bilateral flaps of ALT and bilateral myocutaneous flaps of RA or RF muscle are suggested for the reconstruction of bilateral groin wounds. For infected groin wounds without exposure of femoral vessels, a local flap or primary closure are suggested, depending on the size of the defect.
Patients and Methods
For the purpose of our study, we reviewed retrospectively from June 2008 to February 2012 the records of patients at our institution who had developed infected groin wounds after vascular surgery. On this basis we identified nine patients (five males and four females) with such wounds who had undergone reconstruction and who were included in the study. The patients' ages ranged from 17 to 79 years (with an average of 54.5 years). The mean duration of follow-up of these patients was 13.6 mos (range 8–30 mos). All of the patients' groin wounds had resulted from various vascular surgeries, including coronary artery bypass graft (CABG) surgery, implantation of a cannula for extracorporeal membrane oxygenation (ECMO), bypass surgery for an aneurysm, or implantation of a stent. Three of the nine patients in the study had received expanded polytetrafluoroethylene (ePTFE) grafts, venous grafts, or woven polyester endovascular stent grafts (Endurant; Medtronic, Minneapolis, MN). Wound cultures during the patients' groin operations had shown positive findings in all nine cases. Of the nine patients, six had a right groin wound; one had a left groin wound; and the remaining two patients had bilateral groin wounds. Exposure of femoral vessels was found in seven cases. Details relating to the patients are shown in Table 1 and described below.
CABG=coronary artery bypass graft; CAD=coronary artery disease; D=depth; ECMO=extracorporeal membrane oxygenation; ePTFE=expanded polytetrafluoroethylene; IABP=intra-aortic balloon pump; L=length; MRSA=methicillin-resistant Staphylococcus aureus; TB=tuberculosis; W=width.
Case Reports
Case 1
A 28-year-old male with tuberculosis-induced constrictive pericarditis was treated with pericardiectomy and ECMO. Active bleeding over the groin wound site of insertion of the ECMO cannula, accompanied by a pseudoaneurysm, were noted four days after catheter removal. Emergent interposition vein grafting was performed, but 4 d thereafter the patient developed wound dehiscence with exposure of the graft. Wound culture revealed Escherichia coli. After debridement, a local gracilis muscle flap was used for coverage of the wound, on the basis of the medial circumflex femoral artery. A split-thickness skin graft (STSG) was harvested later for muscle surfacing. The donor site of the graft was closed with the insertion of a Jackson–Pratt drain. The wound had healed uneventfully at 10-mo follow-up (Fig. 1).

Case 1. A right groin wound (8×5×4.5 cm; upper left) was treated with a gracilis muscle flap (upper right) designed to provide coverage of the wound with an appropriate skin graft (lower left). A follow-up at 6 mos revealed that the flap had survived (lower right).
Case 2
A 79-year-old male had an aneurysm of the left common iliac artery treated with woven polyester bifurcated endovascular stent. Because of difficulties in cannulating the contralateral limb anterograde or retrograde, an Aorto-Uni-Iliac (AUI) stent graft (Medtronic) was implanted followed by creation of a femorofemoral bypass with an 8-mm reinforced PTFE graft. The patient later developed ischemic enteritis that required laparotomy and resection; the abdominal incision was left open. Non-healing wounds with exposure of femoral vessels were noted bilaterally in the patient's groins, and culture of these wounds showed Proteus mirabilis, Enterococcus faecalis, and Acinetobacter baumannii. After adequate debridements with graft preservation, a myocutaneous flap of the ALT with part of the TFL, based on the descending and transverse branches of the lateral circumflex femoral artery, was harvested from the patient's left thigh for simultaneous bilateral coverage of his groin wounds and reconstruction of his abdominal wall defect combined with a split-thickness skin graft. Cyanosis of the flap margin was noted but resolved one week later. A 14-mo follow-up visit found no complications of either the bilateral groin wounds or the lower abdominal wound (Fig. 2).

Case 2. Non-healing wounds were noted over the abdomen (upper left; 5.5×2.5×3.5 cm) and bilaterally in the groin (upper right; 6×3×3 cm). An enterostomy wound was also found in the left abdomen (upper right). A combined TFL–myocutaneous ALT flap was designed for coverage of the patient's wounds and was transposed for bilateral groin wound coverage. The abdomen wound was covered with a skin graft (lower left). The wounds had healed successfully in this six-month follow-up view (lower right).
Results
Of the nine patients in our study, one patient underwent primary wound closure; one patient underwent reconstruction with a local tissue flap; four patients underwent reconstruction with pedicled gracilis muscle flaps followed by skin grafts; two patients were treated with myocutaneous flaps of the ALT; and one patient underwent reconstruction with a myocutaneous flap of the ALT and TFL. No donor-site complications were noted. Flap cyanosis was noted in the patient treated with a myocutaneous flap of the ALT and TFL, with resolution within one week. The vascular grafts in three patients were preserved. All of the patients' wounds were healed completely at regularly scheduled follow-up examinations. The patients' outcomes are shown in Table 2.
ALT flap with TFL=myocutaneous flap of anterolateral thigh combined with partial tensor fascia lata.
ALT=myocutaneous island flap of anterolateral thigh.
Discussion
The reconstruction of infected groin wounds after vascular surgery presents a challenge to surgeons. The gold standard treatments for such wounds are debridement, an extra-anatomic bypass, or graft removal. Adequate debridement, good wound care, nutritional support, and flap coverage can therefore provide a better outcome in the reconstruction of infected groin wounds.
The vacuum-assisted closure (VAC) system is considered both a less-invasive means and an alternative to the harvesting of a muscle flap for the reconstruction of infected groin wounds. Pinocy et al. found a decrease in positive wound cultures from 100% on day 0 to 25% and zero, respectively, on days 7 and 14 after the use of a muscle flap harvested with a VAC system, with histologic findings over the same period showing progressive growth of granulation tissue that matched the clinical findings with such treatment [10]. Another study found similar results [11]. Although a VAC system is widely suggested for the closure of infected groin wounds, we consider it appropriate only for those wounds in which there is no exposure of femoral vessels yet debridement is needed. The VAC system may create the risk of bleeding when the femoral vessels are exposed. For infected groin wounds in which the femoral vessels are exposed, muscle or myocutaneous flaps not only provide better resistance to infection but better vessel protection. The use of flaps also shortens the duration of hospitalization.
For wounds smaller than 3 cm in which the femoral vessels are not exposed and in which the wound tension is not high, primary closure is recommended. If the wound bed is not clean, the VAC system can be used temporarily with or without debridement for delayed primary closure. For groin wounds in which there is greater tension or which are larger than 3 cm, a fasciocutaneous flap or a local tissue flap may be considered. One of the patients in our study underwent primary wound closure and another was treated with a local flap on the basis of the sizes of their defects.
Four of our patients underwent groin wound reconstruction with a pedicled gracilis muscle flap followed by a skin graft. A gracilis muscle flap has a type II vascular pattern, with one dominant and one minor vascular pedicle originating from the medial circumflex femoral artery. Indications for use of a gracilis muscle flap include the obliteration of soft-tissue defects [12], coverage of exposed bone or vessels [13], and restoration of absent or impaired neuromuscular function [14]. Several studies have shown satisfactory results of reconstruction of a groin defect with a gracilis muscle flap. Morasch et al. suggested that transposition of pedicled gracilis muscle flaps is an effective option for covering infected or exposed femoral vessels or salvaging prosthetic graft material in the groin [3]. However, some controversial issues surround the use of pedicled gracilis muscle flaps for treating groin wounds, including limited pedicle length (which may limit flap rotation), an inadequate volume for the obliteration of soft-tissue defects, and the need for a two-stage operation (unreliable perforator to skin paddle). Hussey et al. showed that the mean entry point of the dominant arterial pedicle in a pedicled gracilis muscle flap is 9.4 cm from the point of origin of the gracilis muscle, and recorded a mean length and width of the gracilis muscle as 38.4 cm and 6.2 cm, respectively, which suggests that a gracilis muscle flap can have adequate length and volume for the reconstruction of a defect in the groin that is less than 10 cm wide [15]. Because of the unreliable skin paddle of a myocutaneous flap of the gracilis muscle, it is suggested that the use of such a flap be followed by a skin graft to solve this problem. In our four patients whose groin wounds were reconstructed with gracilis muscle flaps, we found good coverage without complications at 13 mos of follow-up.
A TFL flap is a class I flap with a single dominant pedicle originating from the ascending branch of the lateral circumflex femoral artery. The longer pedicle (∼10–20 cm) and bulky volume (15 cm×40 cm) of this flap make it reliable for obliterating a large defect. In a reported case of a patient with a groin and urogenital defect, the TFL was used in a myocutaneous flap to repair the groin defect and the fascia was extended to create a neourethra [16]. The TFL also provided good wound coverage in a similar groin defect resulting from the dissection of a malignant inguinal lymphadenopathy [1]. Because of its characteristics, the TFL with or without the vastus lateralis muscle is recommended for the repair of groin wounds accompanied by defects in the fascia of the lower abdominal wall.
The ALT flap usually has a pedicle derived from the descending branch of the lateral circumflex femoral artery. For groin defects, the ALT flap has many advantages, including a large arc of rotation, minimal donor site morbidity, and a smaller loss of functional muscle. Evriviades et al. reported a good result with the use of an ALT perforator flap in repairing a groin defect resulting from the dissection of a malignant inguinal lymphadenopathy [2]. In our experience, a myocutaneous flap of the ALT has been preferable for reconstructing groin wounds >10 cm in cases of infected groin wounds and exposed femoral vessels. Although the reconstruction of bilateral groin wounds with fascia defects through the use of a myocutaneous flap with TFL was satisfactory in the patient in our study in whom this was done, the distal end of the flap may be subject to cyanosis, and we therefore suggest the use of bilateral myocutaneous ALT flaps for the reconstruction of bilateral groin wounds.
Other choices, such as the rectus abdominis myocutaneous (RAM) flap, have also been reported for the repair of groin wounds [17–19]. The RAM flap is supplied by two pedicles, from the deep superior epigastric and deep inferior epigastric arteries. respectively. To meet different requirements, this flap could be designed for vertical, periumbilical axial, and transverse skin paddles. Qi et al. described a good outcome with the use of a contralateral RAM flap for reconstruction of an infected groin defect resulting from vascular surgery, lymph node dissection and scar revision [17]. Khainga reported with the use of a contralateral RAM flap to repair a groin defect resulting from a failed bypass procedure for an aneurysm of the left femoral artery [18]. The use of ipsilateral RAM flaps for groin reconstruction has also been reported [19]. A RAM flap is therefore a candidate for the reconstruction of groin defects >10 cm wide. Whether RAM flaps are ipsilateral or contralateral, their use carries a risk of decreased abdominal strength and possibility of ventral hernia.
According to previous studies, flaps of the sartorius [20] and rectus femoris (RF) [6] muscles were preferred for the reconstruction of infected groin wounds. A RF muscle flap is suggested for reconstructing groin defects >10 cm wide, although it was suspected that this might decreases the strength of the knee extensors. However, Gardetto et al. suggested that there was no difference in the extensor function of the graft donor leg and the untreated leg [21]. The sartorius muscle flap has the advantages of being immediately adjacent to the groin, ease of preparation, and causing minimal functional morbidity when harvested. However, the segmental blood supply (type IV) of the sartorius muscle makes it difficult to harvest a long graft of this muscle. Moreover, preservation of the proximal pedicle of the sartorius muscle limits the arc of rotation of a graft [22]. Therefore, a sartorius muscle flap is suitable only for reconstructing groin defects <10 cm wide.
In summary, it is suggested that infected groin wounds without exposed femoral vessels be managed by primary closure for wounds <3 cm wide or by the use of a local flap for wounds >3 cm wide. Vacuum-assisted closure with or without debridement is suggested as an alternative method for wounds whose bed is not clear and in which there is no vessel exposure. For single groin wounds <10 cm wide with exposed femoral vessels, a gracilis or sartorius muscle flap followed by STSG is suggested, and for wounds >10 cm wide a myocutaneous ALT, myocutaneous RA, or RF muscle flap is suggested. A TFL graft with or without use of the vastus lateralis muscle is suggested for groin wounds accompanied by defects of the lower abdominal fascia. For bilateral groin wounds with femoral vessel exposure, bilateral ALT, myocutaneous RA, or RF muscle flaps are more reliable and are associated with a lower rate of morbidity. The myocutaneous ALT flap with TFL is not the first choice for the simultaneous reconstruction of bilateral groin wounds and defects in the abdominal fascia even though the outcome is satisfactory. The algorithm for reconstruction of infected groin wounds after vascular surgery is shown in Figure 3.
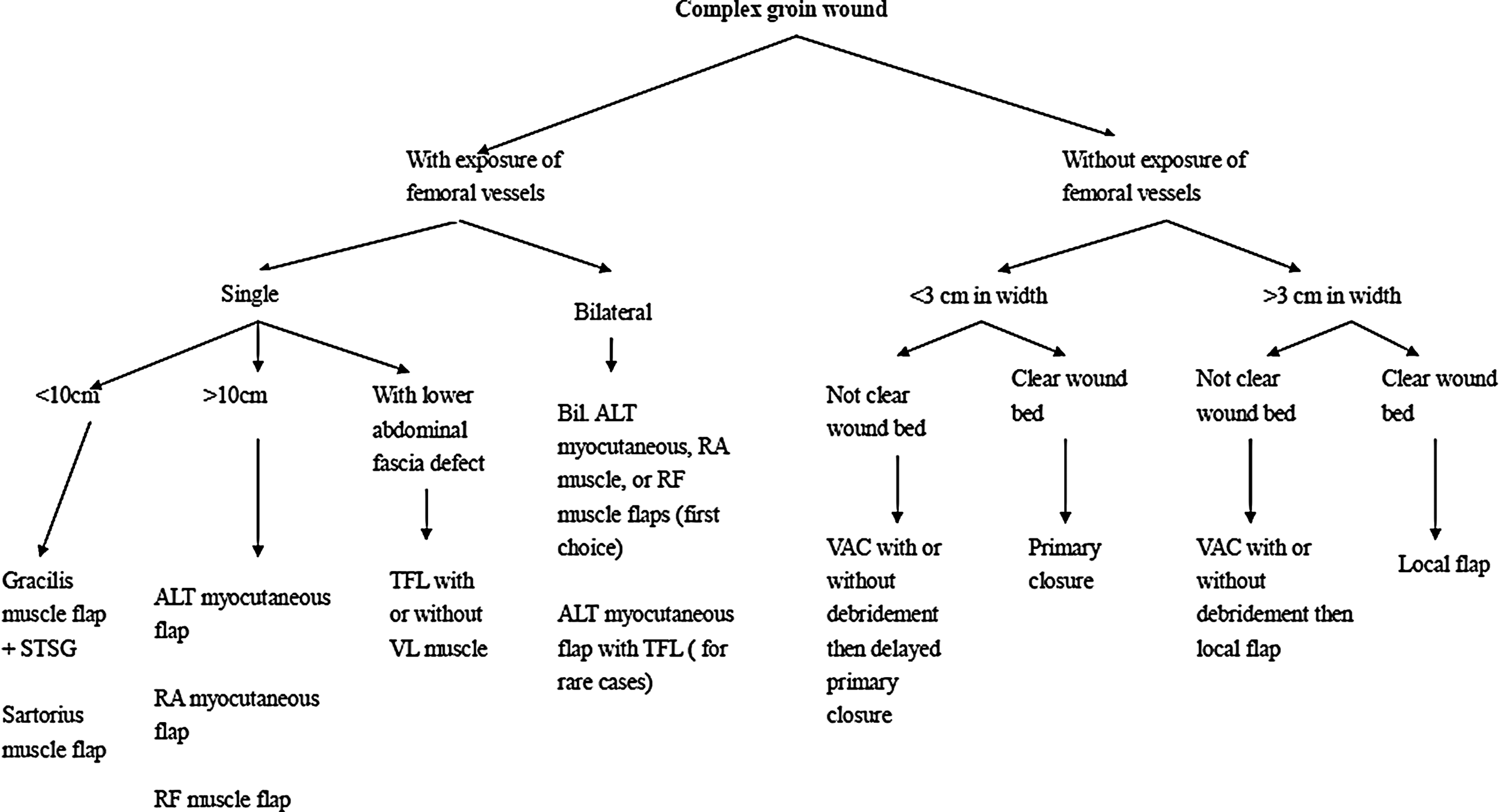
Algorithm for the management of infected groin wounds.
Author Disclosure Statement
No competing financial interests exist.