
Abstract

Physical examination was normal, as was spirometry. Chest radiography revealed nodules in both lungs (Fig. 1). A computed tomography scan demonstrated the cavitary nature of some of the nodules (Fig. 2). The patient underwent left mini-thoracotomy through the fifth intercostal space, and nodules were extracted from both lobes of the left lung. Histologic examination revealed multiple granulomas (1–2 cm) with extensive central necrosis. In the periphery of the lesions, Aspergillus fumigatus was recognized. Cholestyramine was administered to decrease the plasma concentration of leflunomide, and long-term anti-fungal therapy was initiated.

Pulmonary aspergillosis as seen on anteroposterior chest radiography. (
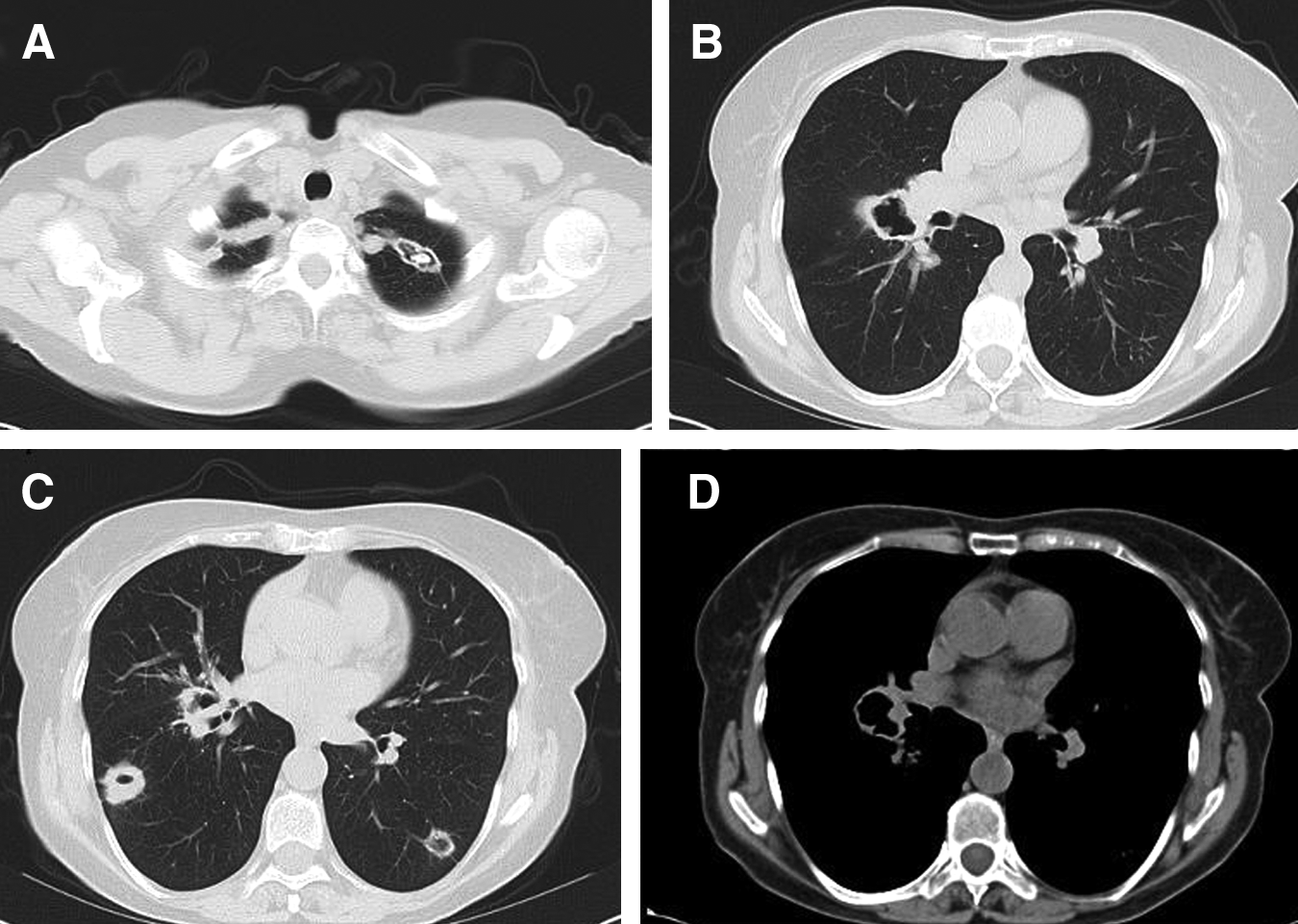
Computed tomography scan shows cavitation in the lesions
Chronic pulmonary aspergillosis (CPA) is a slowly progressive inflammatory disease caused by Aspergillus spp., with a survival rate of 50% at one year if left untreated and 50% at five years with anti-fungal therapy [1–3]. Semi-invasive types of infections include a wide spectrum of presentations such as chronic necrotizing pulmonary aspergillosis and chronic cavitary pulmonary aspergillosis, often overlapping [4].
Rheumatoid arthritis may cause pulmonary nodules with cavitations [5]. Rheumatoid nodules with Aspergillus invasion have been described in patients receiving immunosuppressive drugs or corticosteroids together with leflunomide. Recently, the U.S. Food and Drug Administration alerted physicians to the possibility of fungal diseases in patients receiving leflunomide. To the best of our knowledge, this is the first case of CPA in a patient receiving only leflunomide.