This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of the American College of Surgeons and the Surgical Infection Society. The American College Surgeons is accredited by the ACCME to provide continuing medical education for physicians.
AMA PRA Category 1 Credits™
The American College of Surgeons designates this educational activity for a maximum of 18 AMA PRA Category 1 Credits™.
Physicians should only claim credit commensurate with the extent of their participation in the activity.
AMERICAN COLLEGE OF SURGEONS
DIVISION OF EDUCATION
Program
Wednesday, May 11, 2011
11:00–12:00
Committee Meetings
Living Room
12:00–13:00
Council Lunch
Mizner Room
13:00–17:00
SIS Council Meeting
Banyan Room
17:00–18:00
Nominating Committee
Banyan Room
19:00–21:30
Presidential Dinner (By invitation)
Royal Poinciana I
Thursday, May 12, 2011
08:00–12:00
SURGICAL INFECTIONS SYMPOSIUM: ANNUAL UPDATE Moderator: John Mazuski, MD, PhD
Flagler Ballroom
08:00–08:10
Welcome. John Mazuski, MD, PhD
08:10–08:30
Vagal nerve stimulation and sepsis. Jared Huston, MD
08:30–08:50
Routine screening for MRSA. Martin A. Croce, MD
08:50–09:20
An update in the treatment of cholera. Fred Luchette, MD
09:20–09:40
Racial differences in sepsis. Todd R. Vogel, MD, MPH
09:40–10:00
Discussion
10:00–10:15
Break
10:15–10:35
Adherence to SCIP measures and postoperative SSI. Samir S. Awad MD
10:35–10:55
Common home medications and their influences on infections. Sam Arbabi, MD
10:55–11:15
Hyperglycemia and infection risk. Grant Bochicchio, MD, MPH
11:15–11:35
Perioperative oxygen and the control of surgical infections. Samir Fakhry, MD
11:35–11:50
Discussion and closing remarks
LUNCHEON SYMPOSIUM I(Industry–sponsored satellite;not part of scientific program)
Royal Poinciana Ballroom
13:30–16:00
PLENARY SESSION IThe Art and Science of Surgical Infections (Papers 1–8)Moderators: Henri R. Ford, MD, MHA and Pamela A. Lipsett, MD, MHPE
Yan T. Ortiz-Pomales, MD, Luis G. Reys, MD, Gerald A. Cheadle, BS, Michael J. Krzyzaniak, MD, Nicole E. Lopez, MD, Ann-Marie Hageny, BS, Brian Eliceiri, PhD, Andrew Baird, PhD, Vishal Bansal, MD, Raul Coimbra, MD, PhD. University of California-San Diego (resident)
Discussant: Ronald V. Maier, MD
O2. OUTCOMES OF OPTIMIZED FLUID RESUSCITATION AFTER SEVERE BURN INJURY UTILIZING HEMODYNAMIC MEASUREMENTS BY TRANSPULMONARY THERMO-DILUTION
Robert Kraft, MD, David N. Herndon, MD, Ludwik Branski, MD, Celeste C. Finnerty, PhD, Marc G. Jeschke, MD, PhD. University of Texas Medical Branch, Galveston
Discussant: Basil A. Pruitt, MD
O3. INTERFERON REGULATORY FACTOR-1 (IRF-1) MEDIATES SPLENOCYTES AND MACROPHAGES APOPTOTIC AND AUTOPHAGIC RESPONSES IN ENDOTOXEMIA
Lemeng Zhang, MD, Pinhua Pan, MD, Jon Cardinal, MD, Gary Nace, MD, John Evankovich, Timothy Billiar MD, Allan Tsung, MD. Department of Surgery, University of Pittsburgh
Discussant: Henri R. Ford, MD, MHA
O4. VASCULAR CATHETER CULTURES FOR SUSPECTED CATHETER-RELATED BLOOD STREAM INFECTION IN THE ICU: A TRADITION WHOSE TIME HAS PASSED?
Lisa Flynn, MD, Lisa Hall Zimmerman, PharmD, Alexander Rose, MD, Jing Zhao, PharmD, Krista Wahby, PharmD, Bryan Dotson, PharmD, Robert Wilson, MD, Steven Tennenberg, MD. Wayne State University School of Medicine (resident)
Discussant: Lena M. Napolitano, MD
O5. IMMUNE CELL APOPTOSIS IS TRIGGERED BY SHOCK MESENTERIC LYMPH AND IS MEDIATED THROUGH THE TLR4 PATHWAY
Gregory Tiesi, MD, Diego Reino, MD, Dave Palange, BS, Qi Lu, MD, Leonard Mason, MD, Sharvil Sheth, MD, Jacquelyn Tomaio, BS, Nick Arora, BS, Edwin Deitch, MD. University of Medicine and Dentistry of New Jersey-New Jersey Medical School (resident)
Discussant: Ori D. Rotstein, MD
O6. FUNGUS IN THE ABDOMEN: WHO HAS IT, IS IT LETHAL, AND DOES IT MATTER IF WE TREAT IT?
Amani D. Politano, MD, Tjasa Hranjec, MD, MS, Laura H. Rosenberger, MD, Kristin T. Campbell, MD, Lin M. Riccio, MD, George J. Stukenborg, PhD, Robert G. Sawyer, MD, Carlos A. Tache-Leon, MD. University of Virginia (resident)
Discussant: Pamela A. Lipsett, MD, MHPE
O7. PSEUDOMONAS AERUGINOSA EXPRESSES A LETHAL PHENOTYPE IN RESPONSE TO A DELICATE BALANCE BETWEEN LOCAL PHOSPHATE CONCENTRATION AND EXPOSURE TO KAPPA OPIOIDS
Alexander V. Zaborin, PhD, Christopher Holbrook, MD, Donald Liu, MD, PhD, Olga Y Zaborina, PhD, John C. Alverdy, MD. University of Chicago
Discussant: William G. Cheadle, MD
O8. THE CHASM BETWEEN CDC DIAGNOSIS AND BRONCHOALVEOLAR LAVAGE DIAGNOSIS OF VAP MAY AFFECT PAYMENTS FOR CRITICALLY ILL TRAUMA PATIENTS
Daithi S. Heffernan, MD, Sean F. Monaghan, MD, Zach Gregg, MD, Michael D. Connolly, MD, Shea Gregg, MD, Charles A. Adams, MD, William G. Cioffi, MD. Alpert Medical School of Brown University-Rhode Island Hospital
Discussant: Donald E. Fry, MD
16:00–16:15
FELLOWSHIP AWARD RECIPIENT PRESENTATIONSModerator: Craig Coopersmith, MD
Flagler Ballroom
16:15–17:00
WILLIAM A. ALTEMEIER MEMORIAL LECTURE
Flagler Ballroom
Nod-like Receptors in Host Defense and Disease
Gabriel Nunez, MD
Paul H. De Kruif Professor of PathologyUniversity of Michigan Medical School and Health System
Introduction: Henri R. Ford MD, MHA
University of Southern California Keck School of Medicine
17:00–18:00
SIS MULTICENTER STUDY OF DURATION OF ANTIBIOTICSFOR INTRA-ABDOMINAL INFECTIONS
SURGICAL INFECTION SOCIETY FOUNDATION BOARD MEETINGBy Invitation
Ocean Bistro
18:00–20:00
WELCOME RECEPTION
Pool Terrace
FRIDAY, May 13, 2011
SUNRISE SYMPOSIUM(Industry-sponsored satellite; not part of scientific program)The Potential Role of Antibiotic Diversity in Optimizing Antibiotic SelectionModerator: Lewis Kaplan, MD
Royal Poinciana Ballroom
08:00–10:30
PARALLEL SESSION IFundamental Mechanisms of Surgical Infection (Papers 9–16)Moderators: William G. Cheadle, MD and Stephen F. Lowry, MD, MBA
Royal Poinciana Ballroom
O9. TGF-BETA EXPRESSION IS REQUIRED FOR ENTEROBACTER SAKAZAKII-INDUCED EPITHELIAL INJURY IN A MOUSE MODEL OF NECROTIZING ENTEROCOLITIS
Claudia N. Emami, MD, MPH, Rahul Mittal, PhD, Henri R. Ford, MD, MHA, Nemani V. Prasadarao, PhD. Childrens Hospital Los Angeles-University of Southern California Keck School of Medicine (resident, new member)
Discussant: Lawrence Diebel, MD
O10. TOLL-LIKE RECEPTOR 2 SIGNALING PREVENTS THE DEVELOPMENT OF NECROTIZING ENTEROCOLITIS THROUGH NEGATIVE REGULATION OF THE INNATE IMMUNE RECEPTOR TLR4
Ibrahim Yazji, MD, Sodhi Chhinder, PhD, Matthew Neal, MD, Thomas Prindle, BS, Maria Branca, BS, Anthony Russo, BS, Congrong Ma, BS, Christopher Vos, BS, David J Hackam, MD, PhD. University of Pittsburgh (resident)
Discussant: Jose M. Prince, MD
O11. INSULIN RESTORES APOPTOSIS OF TRAUMA NEUTROPHILS (PMN) BY SUPPRESSING THE NICOTINAMIDE PHOSPHORIBOSYL TRANSFERASE (NAMPT) ACTIVITY OF PRE-B CELL COLONY-ENHANCING FACTOR (PBEF)
Sangyang Jia, Song H. Jia, MD, PhD, Emmanuel Charbonney, MD, Zeenat Malam, BSc, Jean Parodo, BSc, John C Marshall, MD. St. Michaels Hospital-University of Toronto
Discussant: Jared Huston, MD
O12. NON-INVASIVE DETECTION OF PULMONARY PATHOGENS IN VENTILATOR CIRCUIT FILTERS BY PCR
Richard J. Isaacs, PhD, Kenneth A. Debelak, PhD, Patrick R. Norris, PhD, Judith M. Jenkins, MSN, Jeffery C. Rooks, Matthew J. Eckert, MD, Addison K. May, MD, Erik M. Boczko, PhD. Vanderbilt University Medical Center
Discussant: Martin A. Croce, MD
O13. POST-OPERATIVE MRSA CONVERSION AND INFECTION IN MRSA-NEGATIVE PATIENTS: ASSOCIATED FACTORS
Youmna E. Abi-Haidar, MD, Kalpana Gupta, MD, MPH, Judith Strymish, MD, Sandra Williams, MS, Kamal M.F. Itani, MD. Boston University School of Medicine-Veterans Affairs Boston Healthcare System (resident, new member)
Discussant: Greg R. Beilman, MD
O14. CALCIUM/CALMODULIN-DEPENDENT KINASES (CAMK) REGULATE ORGAN DYSFUNCTION DURINE MURINE ENDOTOXEMIA
Gina Howell, MD, Lanping Guo MD, Xianghong Zhang PhD, Richard D. Collage BS, Matthew R. Rosengart, MD, MPH. University of Pittsburgh
Discussant: James Lederer, PhD
O15. MODULATION OF THE MUCUS COMPONENT OF INTESTINAL BARRIER DEFENSE IN VITRO
Mark Diebel, BS, David M. Liberati, MS, Lawrence N. Diebel, MD. Wayne State University (resident)
Discussant: Edwin A. Deitch, MD
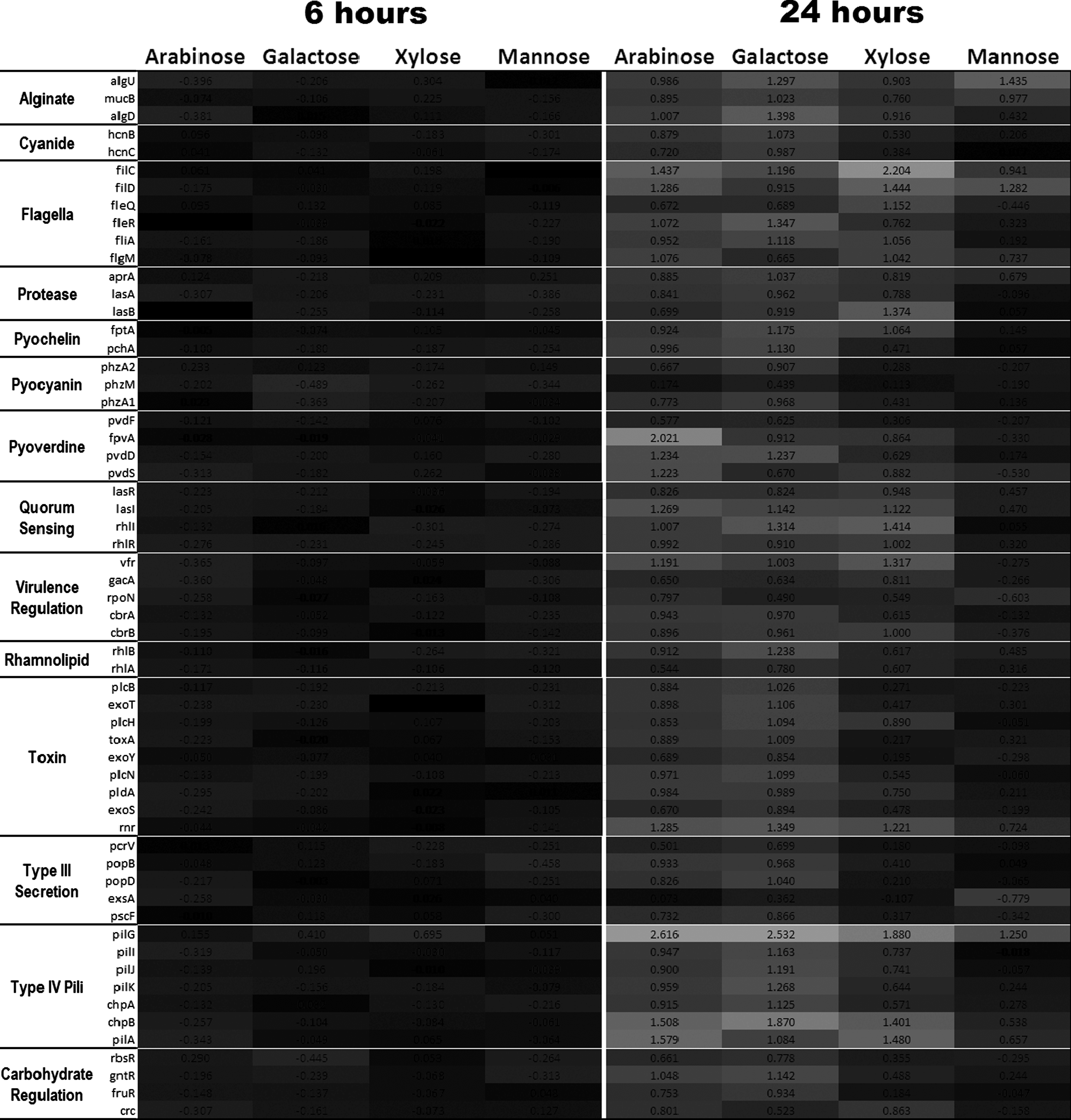
O16. THE EFFECT OF DIETARY MONOSACCHARIDES ON PSEUDOMONAS AERUGINOSA VIRULENCE
Ryan K. Nelson, BA, Valeriy Poroyko, PhD, John C. Alverdy, MD, Michael J. Morowitz, MD. University of Chicago
Discussant: Daithi S. Heffernan, MD
08:00–10:30
PARALLEL SESSION IIClinical Investigations in Surgical Infection (Papers 17-24)Moderators: Lena M. Napolitano, MD and Nick Namias, MD, MBA
Flagler Ballroom
O17. SMALL POSTOPERATIVE CHANGES IN SERUM CREATININE ARE ASSOCIATED WITH POSTOPERATIVE SEPSIS AND SURGICAL INFECTIONS
Charles E. Hobson, MD, Meghan Brennan, MStat, Shahab Bozorgmehri, MD, Philip A. Efron, MD, Azra Bihorac, MD. University of Florida (new member)
Discussant: Samir Fakhry, MD
O18. HYPOGLYCEMIA INCREASES THE RISK OF HOSPITAL-ACQUIRED INFECTIONS IN A SURGICAL INTENSIVE CARE UNIT
Holly K. Sheldon, MD, Joanna Ng, MD, Gustavo Bauza, MD, Juan Mella, MD, Melanie L. Gainsbury, MD, Suresh Agarwal, MD, Peter Burke, MD. Boston University School of Medicine (resident)
Discussant: Philip S. Barie, MD, MBA
O19. A CONSERVATIVE APPROACH TO THE INITIATION OF ANTIMICROBIALS IN CRITICALLY ILL PATIENTS WITH SUSPECTED INFECTION IS ASSOCIATED WITH IMPROVED SURVIVAL
Tjasa Hranjec, MD, MS, Brian R. Swenson, MD, Laura H. Rosenberger, MD, Amani D. Politano, MD, Lin M. Riccio, MD, Rosemarie Metzger, MD, MPH, Kimberly A. Popovsky, RN, Addison K. May, MD, Robert G. Sawyer, MD. University of Virginia (resident)
Discussant: Joseph S. Solomkin, MD, PhD
O20. METHICILLIN-RESISTANT STAPHLOCOCCUS AUREUS AS A CAUSATIVE PATHOGEN IN EARLY VENTILATOR-ASSOCIATED PNEUMONIA: CAUSE FOR CONCERN?
David M. Hill, PharmD, Thomas J. Schroeppel, MD, Louis J. Magnotti, MD, Lesley P. Clement, PharmD, Peter E. Fischer, MD, MS, Timothy C. Fabian, MD, Martin A. Croce, MD. University of Tennessee Regional Medical Center at Memphis
Discussant: John E. Mazuski, MD, PhD
O21. A PROSPECTIVE, PROTOCOLIZED STUDY EVALUATING THE RELIABILITY OF SPUTUM CULTURES OBTAINED AFTER ADMINISTRATION OF ANTIBIOTICS IN INJURED PATIENTS
Matthew C. Byrnes, MD, Eric Irwin, Patty Reicks, Greg J. Beilman. University of Minnesota
Discussant: Robert G. Sawyer, MD
O22. FRESH FROZEN PLASMA TRANSFUSION IS AN INDEPENDENT RISK FACTOR FOR BACTEREMIA IN CRITICALLY ILL TRAUMATIC BRAIN INJURY PATIENTS
Gerard P. De Castro, MD, Grant V. Bochicchio, MD, MPH, Ian R. Driscoll, MD, Deborah M. Stein, MD, MPH, Kelly M. Bochicchio, RN, MS, Shijun Zhu, PhD, Manjari Joshi, MBBS, John R. Hess, MD, MPH, Thomas M. Scalea, MD, R. Adams Cowley Shock Trauma Center-University of Maryland Medical Center (resident)
Discussant: Addison K. May, MD
O23. SYSTEMIC ENDOTOXEMIA FOLLOWING MULTIPLE TRAUMA IS ASSOCIATED WITH EARLY SHOCK AND PREDICTS SUBSEQUENT MORTALITY
Emmanuel Charbonney, MD, Yangmei Li, David Klein, MD, MBA, Alexander Romaschin, PhD, Avery B. Nathens, MD, PhD, John C. Marshall, MD, Keenan Research Centre, Li Ka Shing Knowledge Institute, St. Michael's Hospital-University of Toronto
Discussant: Jeffrey A. Claridge, MD, MS
O24. THE IMPACT OF INFECTIOUS COMPLICATIONS AFTER ELECTIVE SURGERY ON HOSPITAL READMISSION AND LATE MORTALITY IN THE U.S. MEDICARE POPULATION
Todd R. Vogel, MD, MPH, Viktor Y. Dombrovskiy, MD, MPH, PhD, Alan M. Graham, D, Stephen F. Lowry, MD. The Surgical Outcomes Research Group. University of Medicine and Dentistry of New Jersey-Robert Wood Johnson Medical School
Discussant: R. Lawrence Reed, II, MD
10:30–11:00
BREAK - VISIT EXHIBITS
11:00–12:00
PRESIDENTIAL ADDRESS
Flagler Ballroom
Passing in the Night: A Tipping Point in Surgical Training
Pamela A. Lipsett, MD, MHPE
Professor of Surgery, Anesthesiology and Critical Care Medicine, and NursingProgram Director, General Surgery and Surgical Critical CareCo-Director of the Surgical and Weinberg ICUThe Johns Hopkins HospitalPresident, Society of Critical Care Medicine
Introduction: Henri R. Ford, MD, MHAUniversity of Southern California Keck School of Medicine
LUNCHEON SYMPOSIUM I(Industry-sponsored satellite;not part of scientific program)
Royal Poinciana Ballroom
Using a Topical Skin Adhesive to Help Protect Patients against the Risk Factors for Bacterial ContaminationModerator: Adam Singer, MD
13:30–16:00
PARALLEL SESSION IIIUnderstanding the Host Response to Surgical Infection (Papers 25-32)Moderators: John C. Alverdy, MD and Ronald V. Maier, MD
Royal Poinciana Ballroom
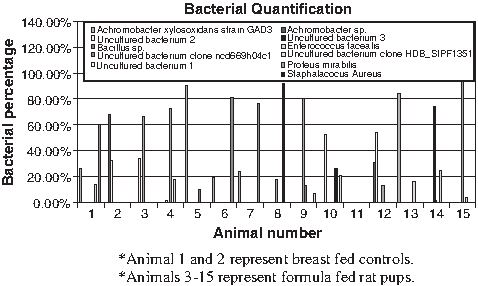
O25. GUT MICROFLORA IS SIGNIFICANTLY ALTERED AFTER 72 HOURS OF FORMULA FEEDING
Erica M. Carlisle, MD, Valeriy Poroyko, PhD, Michael S. Caplan, MD, John C. Alverdy, MD, Michael J Morowitz, MD, Liu Donald, MD, PhD. University of Chicago (resident)
Discussant: Jeffrey Upperman, MD
O26. PARALLEL MICRO-RNA-155 AND TNF-ALPHA PRODUCTION COULD EXPLAIN MICROBIAL TOLERANCE IN A NOVEL PERITONITIS MODEL
Ziad Kanaan, MD, PhD, Sarah Gardner, BS, Jim Peyton, MS, William G. Cheadle, MD. University of Louisville (resident)
Discussant: Michael A. West, MD, PhD
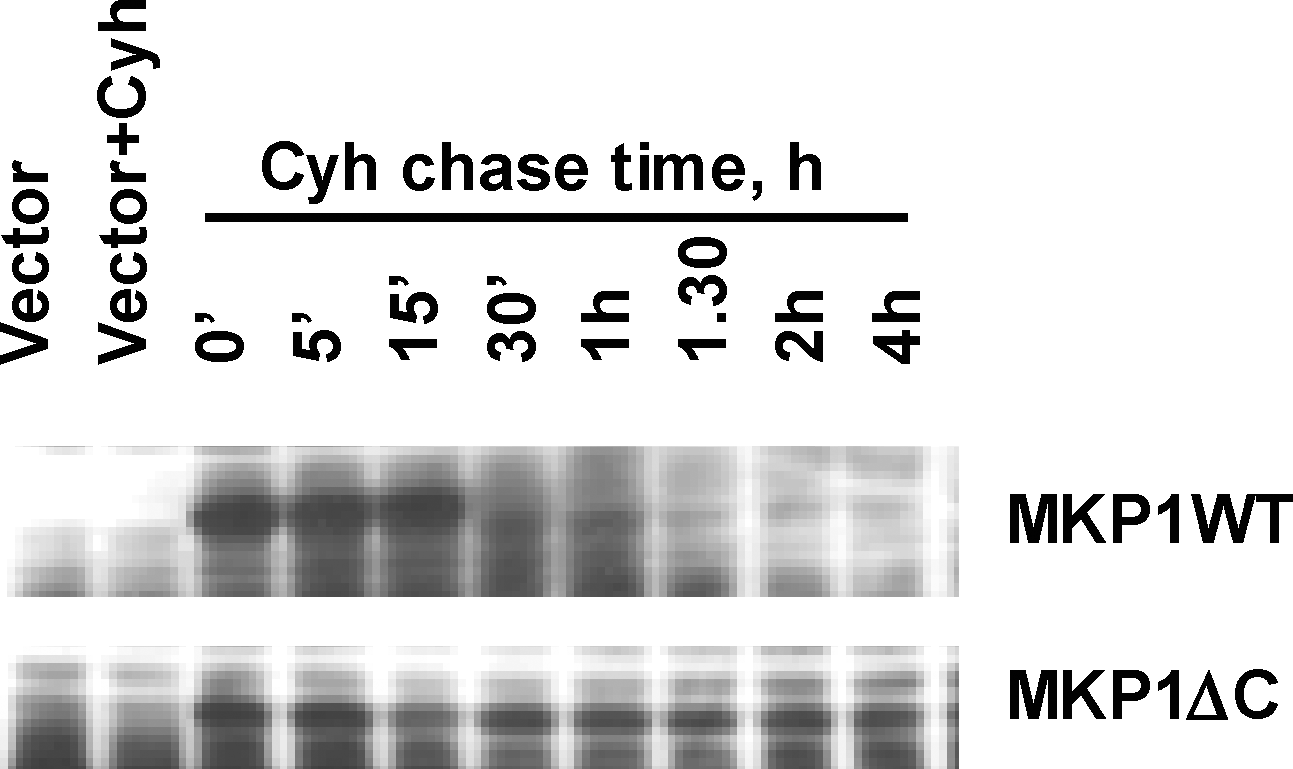
O27. ROLES OF C-TERMINAL NON-CATALYTIC DOMAIN AND ERK PHOSPHORYLATION IN RAPID PROTEOLYSIS OF THE MKP-1 PHOSPHATASE
Jin Wang, MS, Anatoly V. Grishin, PhD, Henri R. Ford, MD, MHA. Children's Hospital Los Angeles-University of Southern California Keck School of Medicine
Discussant: Sam Arbabi, MD
O28. CALCIUM/CALMODULIN-DEPENDENT PROTEIN KINASE I MEDIATES LPS-INDUCED AUTOPHAGY IN MACROPHAGES VIA AMPK AND APG7.
Lanping Gou MD, Xianghong Zhang PhD, Richard D. Collages BS, Jennifer L. Stripay, Stephen M. Robert MD, Allan Tsung MD, Gina Howell MD, Janet S. Lee MD, Matthew R. Rosengart MD, MPH. University of Pittsburgh
Discussant: Lewis Kaplan, MD
O29. THE IMPORTANCE OF HEME-OXYGENASE 1 IN MITOCHONDRIAL BIOGENESIS IN SEPSIS
Evie Carchman, Jay Rao, Sruti Shiva, Brian Zuckerbraun. University of Pittsburgh (resident, new member)
Discussant: Daithi S. Heffernan, MD
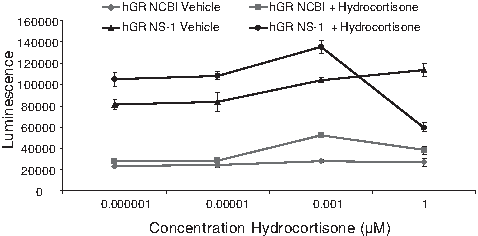
O30. NOVEL ALTERNATIVE SPLICE VARIANT OF THE HUMAN GLUCOCORTICOID RECEPTOR AUGMENTS THE RESPONSE TO HYDROCORTISONE
Aaron C. Baker, MS, MD, Amiri Amini, MD, Kelly Tung, MD, Victoria Chew, BS, Debora Lim, BA, Tajia Green, BS, Kiho Cho, PhD, DVM, David Greenhalgh, MD. University of California-Davis (resident)
Discussant: Marc G. Jeschke, MD, PhD
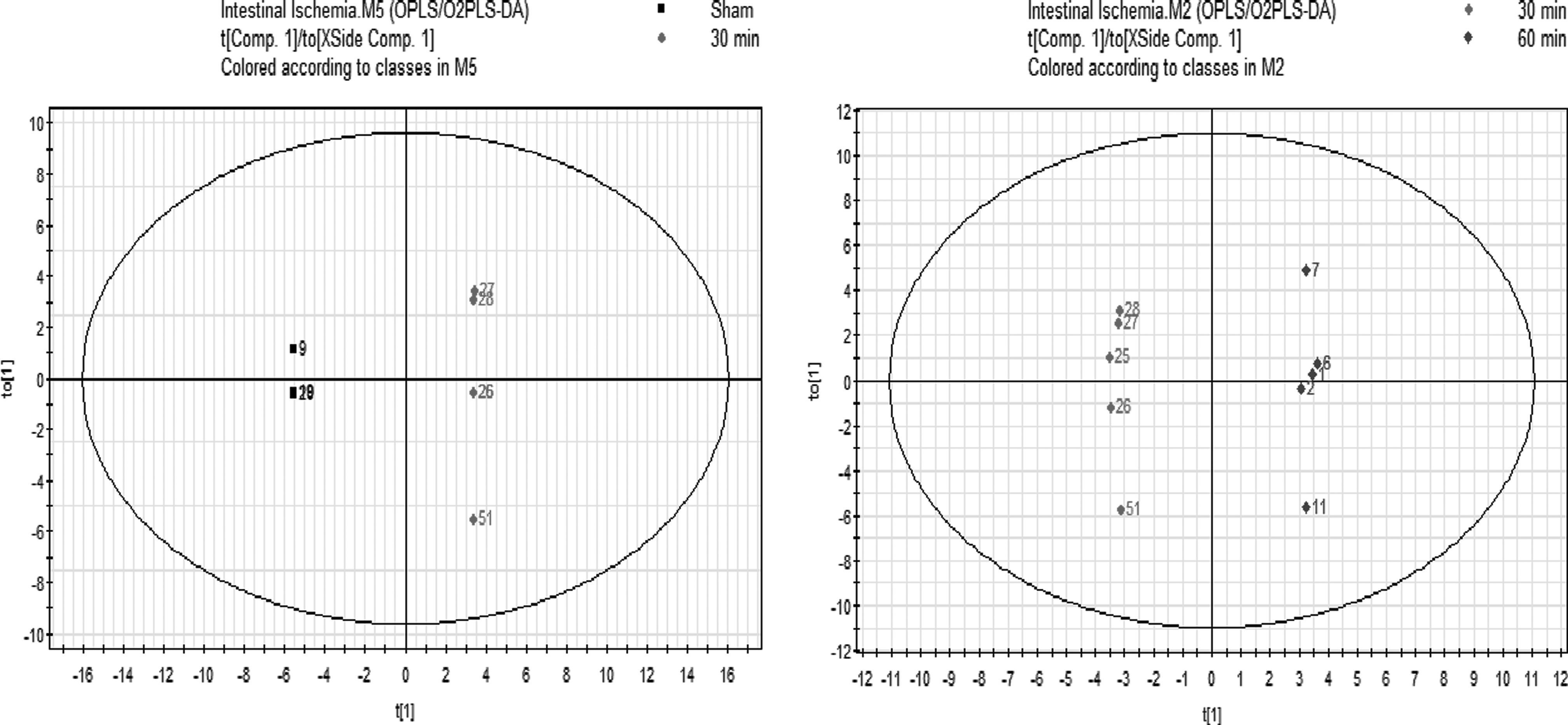
O31. METABOLOMIC PROFILING TO CHARACTERIZE ACUTE INTESTINAL ISCHEMIA/REPERFUSION INJURY
Rachel G. Khadaroo, MD, PhD, Thomas A Churchill, PhD, Christopher M Lukowski, MSc, Richard N Fedorak, MD, Karen L Madsen, PhD. University of Alberta
Discussant: Joseph P. Minei, MD, MBA
O32. NO ASSOCIATE INCREASE IN ARDS OR SEPSIS WITH BETA-BLOCKER USE IN ADULT BURN PATIENTS: A MULTI-CENTER STUDY
Itoro E. Elijah, MD, MPH, Celeste C. Finnerty, PhD, Don C. Bywater, BS, Brett A. Arnoldo, MD, FACS, Richard L. Gamelli, MD, FACS, Nicole S. Gibran, MD, FACS, Marc G. Jeschke, MD, PhD, Matthew B. Klein, MD, Ronald G. Tompkins, MD, ScD, David N Herndon, MD. University of Texas Medical Branch, Galveston (resident, new member)
Discussant: Brian Zuckerbraun, MD
13:30–16:00
PARALLEL SESSION IVOutcomes Studies in Surgical Infection (Papers 33-40)Moderators: Philip S. Barie, MD, MBA, and Robert G. Sawyer, MD
Flagler Ballroom
O33. BACTEREMIA AND VAP: A MARKER FOR CONTEMPORANEOUS EXTRA-PULMONIC INFECTION
Anastasia Kunac, MD, Ziad C. Sifri, MD, Alicia M. Mohr, MD, Helen Horng, PharmD, Robert Lavery, MS, David H. Livingston, MD. University of Medicine and Dentistry of New Jersey-New Jersey Medical School (new member)
Discussant: Felix Y. Lui, MD
O34. BLADDER PRESSURE MEASUREMENTS AND UTI IN TRAUMA PATIENTS
Therese M. Duane, MD, Andrew Young, MD, William Webber, BS, Luke G. Wolfe, MS, Ajai K. Malhotra, MD, Michel B. Aboutanos, MD, MPH, James F. Whelan, MD, Julie Mayglothling, MD, Rao R. Ivatury, MD. Virginia Commonwealth University (new member)
Discussant: Amy McDonald, MD
O35. LOW PHOSPHORUS IS PREDICTIVE OF THE DEVELOPMENT OF INFECTIONS AFTER SURGERY: A STUDY OF HUMANS TO PROVE MURINE DATA.
Sean F. Monaghan, MD, Daithi S. Heffernan, MD, Jason T. Machan, PhD, David T. Harrington, MD, Charles A. Adams, MD, William G. Cioffi, MD. Alpert Medical School of Brown University-Rhode Island Hospital (resident)
Discussant: Olga Zaborina, PhD
O36. DOES ELEVATED GLYCOSYLATED HEMOGLOBIN PREDICT POST-OPERATIVE INFECTIOUS COMPLICATIONS?
I. Michael Leitman, MD, Margaret Bower, MD, Glenn Kashan, MD, Thomas Illic, MD, Vincent De Chavez, Mathew Seigerman, MD, Warren E. Enker, MD, Martin S. Karpeh, Jr, MD, Mariya Huralska. Albert Einstein College of Medicine-Beth Israel Medical Center (resident)
Discussant: Brian Harbrecht, MD
O37. INCREASED MORBIDITY AND MORTALITY ASSOCIATED WITH POST-LIVER TRANSPLANT INTRA-ABDOMINAL INFECTIONS CAUSED BY CANDIDA SPECIES AND VANCOMYCIN-RESISTANT E. FAECIUM (resident)
Harry F. Dorn, MD, Timothy M. Schmitt, MD, Sean C. Kumer, MD, PhD, Kenneth L. Brayman, MD, PhD, Avinash Agarwal, MD, Robert G. Sawyer, MD. University of Virginia
Discussant: Philip S. Barie, MD, MBA
O38. NASAL MRSA PREDICTS VENTILATOR-ASSOCIATED PNEUMONIA AND MICROBIOLOGY
Zachary A Gregg, MD, Daithi S. Heffernan, MD, Sean F. Monaghan, MD, Michael D. Connolly, MD, Shea C. Gregg, M.D, Matthew S. Kozloff, MD, Charles A. Adams, MD, William G. Cioffi, MD. Alpert Medical School of Brown University-Rhode Island Hospital (resident)
Discussant: Preston Miller, MD
O39. VENTILATOR-FREE DAYS AS A PREDICTOR FOR PNEUMONIA: IS IT ACCURATE?
Alicia M. Williams, MD, Grant V. Bochicchio, MD, Shijun Zhu, PhD, Kelly Bochicchio, RN, MS, Thomas Scalea, MD. University of Maryland and Walter Reed Army Medical Center (resident)
Discussant: Nick Namias, MD, MBA
O40. THE EFFECT OF ADOPTING A CLINICAL PATHWAY FOR THE MANAGEMENT OF PEDIATRIC APPENDICITIS AND COMPARISON TO THE PEDIATRIC HEALTH INFORMATION SYSTEM DATABASE
Felix C. Blanco, MD, Katherine P. Davenport, MD, Evan P. Nadler, MD, Anthony D. Sandler, MD. George Washington University-Childrens National Medical Center
Discussant: John Mihran Davis, MD
16:00–17:20
POSTER SESSION (Posters 1–70)Basic and Clinical Studies in Surgical Infection
Royal Poinciana III/Foyer
Moderators:
Session 1. (Posters 1- 9) David Greenhalgh, MD and Sam Arbabi, MD
Session 2. (Posters 10-19) Matthew Rosengart, MD, MPH and Heather Evans, MD
Session 3. (Posters 20-29) Marc Jeschke, MD, PhD and Lewis Kaplan, MD
Session 4. (Posters 30-39) David Blake, MD and Greg J. Beilman, MD
Session 5. (Posters 40-49) Jose Prince, MD and Sandra Swoboda, RN, MS
Session 6. (Posters 50-59) Gary An, MD and Evan Nadler, MD
P1. INTEGRATED SAFETY SUMMARY OF CEFTAROLINE FOSAMIL: OVERALL AND FORPATIENTS WITH COMPLICATED SKIN AND SKIN STRUCTURE INFECTION (CSSSI)
Douglas R. Rank, MD, H. David Friedland, MD, MBA, Tanya Baculik, MD, Alexander Smith, MS, Dirk Thye, MD. Cerexa, Inc., Oakland, CA
P2. A NOVEL MODEL TO STUDY THE COMBINED EFFECTS OF MICROBES AND OXIDANTS ON THE DEVELOPMENT OF NECROTIZING ENTEROCOLITIS
Erica M. Carlisle, MD, Olga Zaborina, PhD, Donald Liu, MD, PhD, John C. Alverdy, MD. University of Chicago
P3. DISCOVERY OF MECHANISTIC INTERACTIONS BETWEEN PSEUDOMONAS AERUGINOSA AND WOUNDED EPITHELIAL CELLS WITH AN AGENT-BASED MODEL: IMPLICATIONS FOR THE PATHOGENESIS OF ANASTOMOTIC LEAKS
Jordan R. Stern, MD, Andrea D. Olivas, MD, Vesta Valuckaite, MD, Scott Christley, PhD, Olga Zaborina, PhD, John C. Alverdy, MD, Gary An, MD. University of Chicago
P4. NECROTIZING SOFT TISSUE INFECTION SECONDARY TO CANDIDA ALBICANS IN AN IMMUNOCOMPETENT PATIENT
Patrick J. Buchanan, BS, Tad Kim, MD, Larry Lottenberg, MD, Philip A. Efron, MD, Darwin Ang, MD, PhD, MPH. University of Florida
P5. VIDEO-ASSISTED SINGLE PORT APPENDECTOMY: ZERO SURGICAL SITE INFECTIONS
Gonzalo Gómez, MD, María C. Arroyave, MD, Diego Penagos, MD, María C. García, MD, Juan D. Martínez, MD, Rogelio Matallana, MD, Felipe Vanegas, MD, María C. Mendoza, MD, Sergio Díaz, MD. CES University, Medellin, Colombia
P6. NEGATIVE VALUE OF IMAGING IN MANAGEMENT OF NECROTIZING SOFT TISSUE INFECTIONS
Yana Etkin, MD, Victoria Lai, MD, Joseph Lindner, PA-C, Peter Kyunghwan Kim, MD. Albert Einstein College of Medicine
P7. EAA HELPS TO DETECT THE CAUSE OF ARDS AT BEDSIDE
Junichi Kitayama, MD, Takeyuki Kiguchi, MD, Kazuma Yamakawa, MD, Yasushi Nakamori, MD, Satoshi Fujimi, MD. Osaka University School of Medicine
P8. GENE EXPRESSION IN THE MOUSE JUVENILE INTESTINE IN RESPONSE TO MILK AND FORMULA FEEDING
Valeriy Poroyko, PhD, Erica M. Carlisle, MD, Neil Bahroos, Alex Rodriguez, Michael S. Caplan, MD, John C. Alverdy, MD, Michael J. Morowitz, MD, Donald Liu, MD, PhD. University of Chicago
P9. CONTACT ISOLATION: THE PATIENT EXPERIENCE
Christina Bess, BS, Steven Allen, MD, Heidi Frankel, MD. Penn State Hershey College of Medicine
P10. INTERMITTENT EXPOSURE TO ANTIMICROBIAL SOLUTIONS DECREASES PSEUDOMONAS AERUGINOSA BIOBURDEN IN AN IN VITRO BIOFILM MODEL
Chris Lessing, PhD, Melinda Hayman, PhD, Amy McNulty, PhD. Kinetic Concepts, Inc., San Antonio
P11. SURGICAL SITE INFECTION IS ASSOCIATED WITH PATIENT SURVIVAL AT A HOSPITAL LEVEL: EVIDENCE FOR SYSTEMS BASED INTERVENTION
Makesha V. Miggins, MD, Larry Lottenberg, MD, Huazhi Liu, MS, Lyle L. Moldawer, PhD, Philip A. Efron, MD, Darwin N. Ang, MD, PhD, MPH. University of Florida
P12. BEYOND CORE MEASURES: IDENTIFICATION OF MODIFIABLE RISK FACTORS FOR THE PREVENTION OF SURGICAL SITE INFECTION AFTER ELECTIVE TOTAL ABDOMINAL HYSTERECTOMY
Heather Young, MD, Robin Bliss, PhD, J. Chris Carey, MD, Connie S. Price, MD. University of Colorado-Denver Health Medical Center
P13. POLYMORPHONUCLEAR (PMN) AND RED BLOOD CELL FUNCTION ARE RAPIDLY ALTERED FOLLOWING MAJOR TRAUMA
Leonard L. Mason, MD, Gregory Tiesi, MD, Garima Dosi, MD, Eleonora Feketeova, MD, Lauren Blackwell, MD, Diego Reino, MD, Sharvil Sheth, MD, Dave Palange, BS, Edwin A. Deitch, MD. University of Medicine and Dentistry of New Jersey-New Jersey Medical School
P14. MEDICAL STUDENTS AND HOSPITAL HAND HYGIENE-WHAT DO THEY KNOW, AND WHAT DO THEY DO?
Hanna Alemayehu, MD, Vanessa P. Ho, MD, MPH, Julie I. Leviter, BS, Lewis M. Drusin, MD, MPH, Philip S. Barie, MD, MBA. Weill Cornell Medical College and New York Medical College
P15. APRV TREATMENT OF SEVERE INHALATION PNEUMONITIS
Mary Lou Patton, MD, Sondra Waldecker, PhD, Bruce H. Ackerman, PharmD, Cynthia L. Reigart, RN, Diane Herder, RN, Robert E. Guilday, MD, Linwood R. Haith, MD. Nathan Speare Regional Burn Treatment Center, Crozer-Chester Medical Center
P16. BETA BLOCKADE FOLLOWING INJURY: A CRITICAL LINK BETWEEN HEART RATE AND IMMUNOMODULATION
Gregg M. Baranski, MD, Kristin M. Cook, MD, Ziad C. Sifri, MD, Walter D. Alzate, MS, MBS, David H. Livingston, MD, Alicia M. Mohr, MD. University of Medicine and Dentistry of New Jersey-New Jersey Medical School
P17. OCCURRENCE OF ENTEROBACTER CLOACAE AND E. AEROGENES IN INTRA-ABDOMINAL INFECTIONS DURING 2009: ACTIVITY OF TIGECYCLINE AND COMPARATOR AGENTS (T.E.S.T. 2009)
Stephen Hawser, PhD, Daryl Hoban, PhD, Meredith Hackel, PhD, Sam Bouchillon, MD, Jack Johnson, MBA, Michael Dowzicky, BS. IHMA Europe Sàrl, Epalinges, Switzerland
P18. ACTIVITY OF TIGECYCLINE AND COMPARATORS AGAINST NORTH AMERICAN K. PNEUMONIAE FROM GASTROINTESTINAL INFECTIONS (T.E.S.T. 2005-2009)
Robert Badal, BS, Daryl Hoban, PhD, Meredith Hackel, PhD, Sam Bouchillon, MD, Brian Johnson, BS, Stephen Hawser, PhD, Michael Dowzicky, BS. IHMA Europe Sàrl, Epalinges, Switzerland
P19. INCIDENCE OF ESCHERICHIA COLI, EXTENDED-SPECTRUM BETA-LACTAMASE PRODUCTION (ESBL), AND THE ACTIVITY OF TIGECYCLINE AND COMPARATORS IN INTRA-ABDOMINAL INFECTIONS (IAI) IN THE UNITED STATES. (T.E.S.T. 2005-2009)
Sam Bouchillon, MD, Brian Johnson, BS, Robert Badal, BS, Daryl Hoban, PhD, Meredith Hackel, PhD, Stephen Hawser, PhD, Michael Dowzicky, BS. International Health Management Association, Inc., Schaumberg, IL
P20. ACTIVITY OF TIGECYCLINE AND COMPARATORS AGAINST CLINICAL ISOLATES FROM MEDICAL AND SURGICAL INTENSIVE CARE UNITS (T.E.S.T. 2009)
Meredith Hackel, PhD, Sam Bouchillon, MD, Daryl Hoban, PhD, Brian Johnson, BS, Robert Badal, BS, Jack Johnson, MBA, Stephen Hawser, PhD, Michael Dowzicky, BS. IHMA, Inc., Schaumberg, IL
P21. SUSCEPTIBILITY OF STREPTOCOCCUS AGALACTIAE FROM MULTIPLE INFECTION SITES: RESULTS OF THE TIGECYCLINE EVALUATION SURVEILLANCE TRIAL (T.E.S.T. 2009-2010)
Daryl Hoban, PhD, Meredith Hackel, PhD, Robert Badal, BS, Sam Bouchillon, MD, Brian Johnson, BS, Stephen Hawser, PhD, Michael Dowzicky, BS. IHMA, Inc., Schaumberg, IL
P22. SUSCEPTIBILITY OF MRSA FROM RESPIRATORY AND WOUND SOURCES TO LINEZOLID AND COMPARATORS IN THE U.S. FROM THE T.E.S.T. PROGRAM-2004-2010
Brian Johnson, BS, Sam Bouchillon, MD, Jack Johnson, MBA, Daryl Hoban, PhD, Meredith Hackel, PhD, Robert Badal, BS, Stephen Hawser, PhD, Michael Dowzicky, BS. IHMA, Inc., Schaumberg, IL
P23. FACTORS AFFECTING THE INCIDENCE OF INFECTION AFTER COLORECTAL TRAUMA
Lisa M. Flynn, MD, Lisa G. Hall-Zimmerman, PharmD, Robert F. Wilson, MD. Wayne State University-Detroit Medical Center
P24. TRENDS IN SUSCEPTIBILITY OF INTRA-ABDOMINAL INFECTIONS IN NORTH AMERICA-SMART 2005-2010
Robert Badal, BS, Sam Bouchillon, MD, Daryl Hoban, PhD, Aaron Johnson, BA, Meredith Hackel, PhD, Stephen Hawser, PhD. IHMA, Inc., Schaumberg, IL
P25. SURGICAL SITE INFECTIONS AMONG PATIENTS WITH PROCEDURES INVOLVING ARTHROSCOPY
Connie Savor Price, MD, Heather M. Gilmartin, MSN, Allison Lee Sabel, MD, PhD, MPH. University of Colorado-Denver Health Medical Center
P26. SURGEONS' ACCEPTANCE OF SURGICAL SITE INFECTION RISK ADJUSTMENT MODELS
Heather Young, MD, Susan Moore, MSPH, Lucy Savitz, PhD, MBA, Connie S. Price, MD, Walter L. Biffl, MD. University of Colorado-Denver Health Medical Center
P27. INFECTIOUS COMPLICATIONS AFTER CABG: DOES MINIMALLY INVASIVE TECHNIQUE MAKE A DIFFERENCE?
Timothy F. Danish, MD, Viktor Y. Dombrovskiy, MD, MPH, PhD, George P. Batsides, MD, Todd R. Vogel, MD, MPH. The Surgical Outcomes Research Group. University of Medicine and Dentistry of New Jersey-Robert Wood Johnson Medical School
P28. EARLY CLINICAL RESPONSE (CR) ANALYSES OF TWO PHASE III (CANVAS 1 AND CANVAS 2) TRIALS OF CEFTAROLINE (CPT) FOSAMIL VS. VANCOMYCIN PLUS AZTREONAM (V/A) IN THE TREATMENT OF COMPLICATED SKIN AND SKIN STRUCTURE INFECTIONS (CSSSI)
Tanya Baculik, MD, Paul B. Eckburg, MD, H. David Friedland, MD, Lily Llorens, PhD, Alena Jandourek, MD, Gary Witherell, PhD, Dirk Thye, MD. Cerexa, Inc., Oakland, CA
P29. THE USE OF CD64 LEVELS TO DISCERN INFECTION IN THE PRESENCE OF MARKED FEBRILE RESPONSES AMONG PATIENTS WITH A SPINAL CORD INJURY OR TRAUMATIC BRAIN INJURY
Matthew C. Byrnes, MD, Eileen Eggenberger, Patty Reicks, Kristine Mulier, Greg J. Beilman, MD. University of Minnesota
P30. SURGICAL SITE INFECTION IS ASSOCIATED WITH PATIENT SURVIVAL AT THE HOSPITAL LEVEL: EVIDENCE FOR SYSTEMS-BASED INTERVENTIONS
Makesha V. Miggins, MD, Larry Lottenberg, MD, Huazhi Liu, MS, Lyle L. Moldawer, PhD, Philip A. Efron, MD, Darwin Ang, MD, PhD, MPH. University of Florida
P31. EVALUATING THE RELATIONSHIP BETWEEN ORGAN DYSFUNCTION AND MORTALITY IN SEVERE SEPSIS AND SEPTIC SHOCK FOLLOWING THE IMPLEMENTATION OF AN EARLY SEPSIS INITIATIVE
Garrett Coyan, BS, Steven Tenny, BS, Chad Cannon, MD, Charles Richart, MD, Michael Moncure, MD. University of Kansas
P32. HEMORRHAGIC SHOCK ACTIVATES ENDOTHELIAL INFLAMMASOME: ROLE OF HMGB1
Yuehua Li, MS, Xiaolian Shi, PhD, Jia Xu, MD, Mark Wilson, MD, Jie Fan, MD. University of Pittsburgh-Veterans Affairs Pittsburgh Healthcare System
P33. INCREASED INCIDENCE OF PERFORATED APPENDICITIS IN OBESE CHILDREN
Felix C. Blanco, MD, Pam Choi, MD, Faisal G. Qureshi, MD, Anthony D. Sandler, MD, Evan P. Nadler, MD. George Washington University-Childrens National Medical Center
P34. THREE SINGLE NUCLEOTIDE POLYMORPHISMS OF HUMAN GLUCOCORTICOID RECEPTOR RESULT IN ENHANCED ACTIVITY.
Amir Amini, MD, Aaron Baker, MS, MD, Kelly Tung, MD, Tajia Green, BS, Debora Lim, BA, Kiho Cho, DVM, PhD, David Greenhalgh, MD. University of California-Davis
P35. DIVERSITY OF POSTNATAL MICROBIOTA IN EXPERIMENTAL NECROTIZING ENTEROCOLITIS
Monica L. Williams, BS, Aaron J. Fried, Shannon Castle, MD, Anatoly Grishin, PhD, Henri R. Ford, MD, MHA. University of Southern California Keck School of Medicine-Childrens Hospital Los Angeles
P36. HEAT SHOCK PROTEIN 27 ASSOCIATED WITH POOR OUTCOMES IN HEMORRHAGIC SHOCK
Mark Muir, MD, Wieslaw Furmaga, MD, Valery Mikhailov, Rachelle Jonas, RN, Christopher Louden, MS, Stephen Cohn, MD, Joel Michalek, PhD. University of Texas Health Science Center at San Antonio
P37. PATIENT CHARACTERISTICS AND POSSIBLE RISK FACTORS OF C. DIFFICILE TOXIC MEGACOLON
Nasim Ahmed, MD, Yen-Hong Kuo, PhD, John M. Davis, MD. Jersey Shore University Medical Center
P38. HYPOGLYCEMIC EPISODES POST-BURN ARE ASSOCIATED WITH INCREASED POST-BURN MORBIDITY
Robert Kraft, MD, David N. Herndon, MD, Gabriela A. Kulp, Marc G. Jeschke, MD, PhD. University of Texas Medical Branch, Galveston-Shriners Hospital for Children
P39. HOLLOW VISCUS ABDOMINAL INJURY IS NOT ASSOCIATED WITH INCREASED INTRA-ABDOMINAL INFECTION FOLLOWING DAMAGE CONTROL LAPAROTOMY
Josephine Kweku, MD, Grant V. Bochicchio, MD, MPH, Gerard P. DeCastro, MD, Shijun Zhu, PhD, Anthony Harrera, MS, Kelly Bochicchio, RN, MS, Thomas M. Scalea, MD. University of Maryland School of Medicine-R. Adams Cowley Shock Trauma Center
P40. PERCUTANEOUS OR OPEN TRACHEOSTOMY? A COMPARISON OF PROCEDURES AND SURGICAL SITE INFECTIONS
Habeeba Park, MD, Gerard P. De Castro, MD, Grant V. Bochicchio, MD, MPH, Jennifer Kent, MHS, Shijun Zhu, PhD, Manjari Joshi, MD, Kelly Bochicchio, MS, Thomas Genuit, MD, MBA, Sharon M. Henry, MD, Thomas M Scalea, MD. Sinai Hospital of Baltimore and University of Maryland School of Medicine-R. Adams Cowley Shock Trauma Center
P41. WHERE'S THE DIFFERENCE? PRESENTATION OF NOSOCOMIAL INFECTION IN CRITICALLY ILL TRAUMA VERSUS GENERAL SURGERY PATIENTS
Katherine B. Kelly, MD, Adam A.M. Fadlalla, PhD, Jeffrey A. Claridge, MD, MS. Case Western Reserve University-MetroHealth Medical Center
P42. THE IMPACT OF PATIENT WORKLOAD AND TIME ON HAND HYGIENE (HH) COMPLIANCE
Sandy M. Swoboda, RN, MS, Aldeheide Weissmueller, BS, Stephen Lane, PhD, Pamela A. Lipsett, MD, MHPE. Johns Hopkins University
P43. BAD BUGS AND THE ELDERLY TRAUMA PATIENT: AN INDICATOR OF MORTALITY?
Tiffany K Bee, MD, Louis J Magnotti, MD, Thomas J Schroeppel, MD, Martin A Croce, MD. University of Tennessee Health Science Center, Memphis
P44. IN VIVO TRANSFORMATION OF PSEUDOMONAS AERUGINOSA TO A SWARMING PHENOTYPE AFTER ANASTOMOSIS FORMATION: A POTENTIAL ROLE IN ANASTOMOTIC LEAK
Andrea D Olivas, MD, Olga Zaborina, PhD, John C Alverdy, MD. University of Chicago
P45. MODELING COMMON TLR4 AND INJURY-INDUCED EARLY TRANSCRIPTION RECOVERY THEMES IN HUMAN LEUKOCYTES
Tara M. Balija, MD, Irina Bernescu, MD, Michael T. Reddell, Jacqueline E. Calvano, Susette M. Coyle, RN, Marie A. Macor, RN, Steve E. Calvano, PhD, Beatrice Haimovich, PhD, Stephen F. Lowry, MD. University of Medicine and Dentistry of New Jersey-Robert Wood Johnson Medical School
P46. TRIMETHOPRIM-ASSOCIATED HYPERKALEMIA IN A YOUNG TRAUMA VICTIM
Hugo J.R. Bonatti, MD, Carly Miller, MD, Michael Vella, MD, Chanjuan Shi, MD, Jose Diaz, MD, Addison K. May, MD, William H. Nealon, MD, Jeffrey S. Guy, MD. Vanderbilt University Medical Center
P47. PSEUDOMENBRANOUS CMV ASSOCIATED COLITIS IN A PATIENT WITH LOW NATURAL KILLER CELL COUNT
Hugo J.R. Bonatti, MD, Carly Miller, MD Jessica Lynn Hata, Michael A. Vella, MD Addison K. May, MD, William H. Nealon, MD, Chanjuan Shi, MD, Jeffery Guy, MD. Vanderbilt University Medical Center
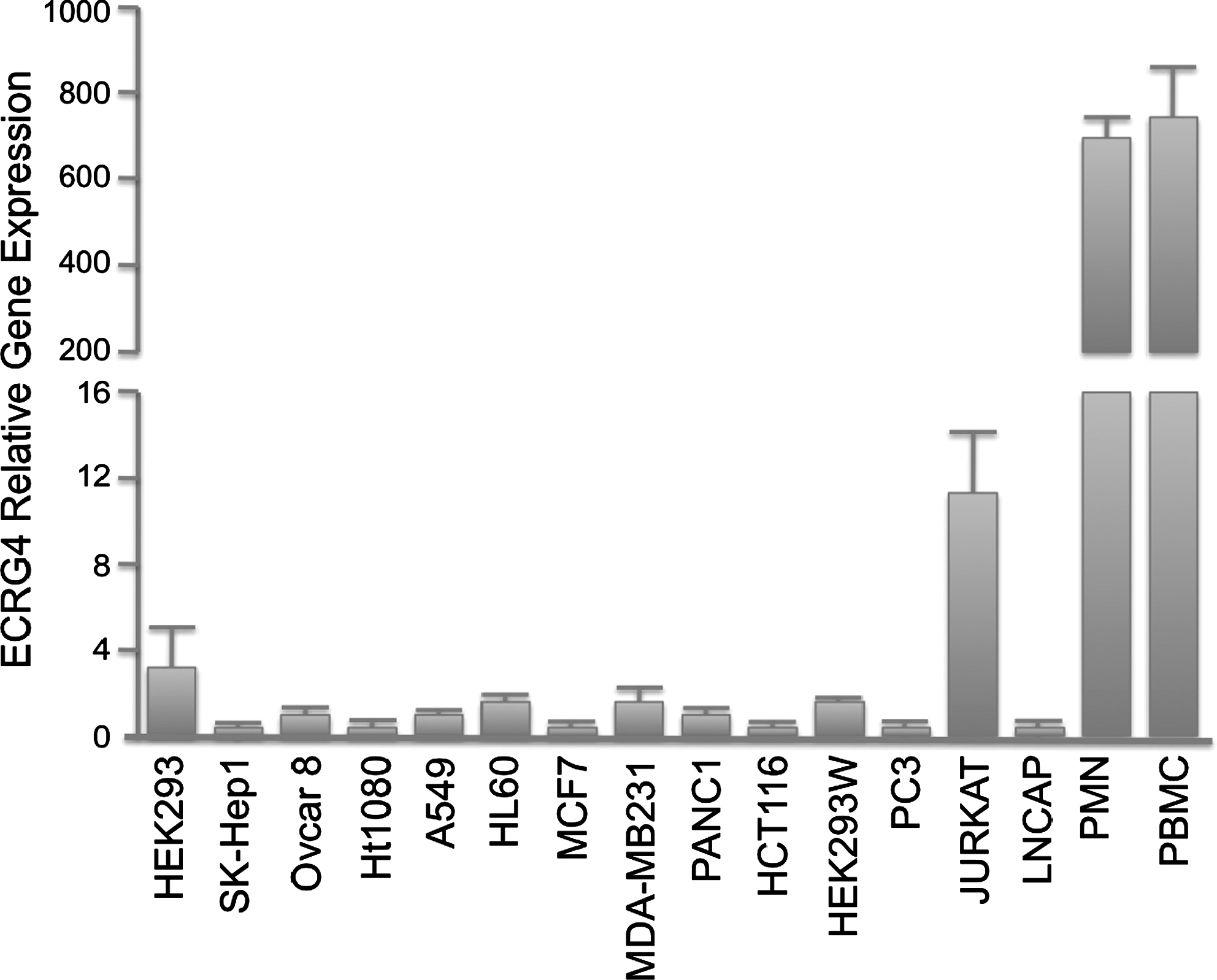
P48. AUGURIN, AN EPIGENETICALLY-REGULATED CANDIDATE TUMOR SUPPRESSOR, IS PRESENT IN NORMAL BLOOD MONONUCLEAR CELLS (PBMC) AND POLYMORPHONUCLEAR (PMN) LEUKOCYTES: IMPLICATIONS FOR SURGICAL INFECTION AND IMMUNITY.
Michael Krzyzaniak, MD, Xitong Dang, PhD, Andrew Baird, PhD, Brian Eliceiri, PhD, James Putnam, BS, Raul Coimbra, MD, PhD. University of California-San Diego
P49. USING FLOW CYTOMETRY TO MEASURE SIGNALING BY PERIPHERAL BLOOD LEUKOCYTES THROUGH CD11B/CD18 RECEPTORS DURING SEPSIS IN A PORCINE MODEL
Kenneth C Norbury, PhD, Shinil K Shah, DO, Fernando Jimenez, MS, Peter A Walker, MD, Karen S Uray, PhD, Charles S Cox, MD. Kinetic Concepts, Inc., San Antonio
P50. COMPARISON OF A NOVEL NEGATIVE PRESSURE THERAPY (NPT) SYSTEM AND STANDARD OF CARE IN A PORCINE MODEL OF SEPSIS AND GUT ISCHEMIA/REPERFUSION-INDUCED INJURY
Kenneth C Norbury, PhD, Barbara A Collins, BS, RVT, Richard P Mormino, PhD, Deepak V Kilpadi, PhD. Kinetic Concepts, Inc., San Antonio
P51. INCREASING INCIDENCE OF SURGICAL SITE INFECTIONS DUE TO RESISTANT ORGANISMS
Uroghupatei P. Iyegha, MD, Javariah Asghar, MD, MPH, Catherine Statz, RN, MPH, James J. Glover, BS, Greg J. Beilman, MD. University of Minnesota
P52. ANTIMICROBIAL FABRIC TECHNOLOGY REDUCES BACTERIAL CONTAMINATION: A NOVEL INFECTION CONTROL APPROACH
Carl I. Schulman, MD, MSPH, Fernanda Kuchkarian, MPH, Kelly Withum, BS, Robert Duncan, PhD. University of Miami Miller School of Medicine
P53. MICE SUBJECTED TO SEVERE PERIPHERAL TRAUMA ARE RESISTANT TO PSEUDOMONAS PNEUMONIA AT 24 HOURS
Marcus K. Hoffman, MD, Sophie S. Darwiche, MD, Lauryn K. Kohut, MA, Timothy R. Billiar, MD. Univeristy of Pittsburgh
P54. ICU-ACQUIRED PSEUDOMONAS AERUGINOSA AND ACINETOBACTER BAUMANNII ARE INDEPENDENT PREDICTORS OF MORTALITY POST BURN
Noe A. Rodriguez, MD, Celeste C. Finnerty, PhD, Jong O. Lee, MD, Sachin D. Hegde, MD, David N. Herndon, MD. The University of Texas Medical Branch, Galveston-Shriners Hospitals for Children
P55. INSTITUTIONAL SURGICAL SITE INFECTION PROGRAMS ARE COMPLEMENTARY TO AMERICAN COLLEGE OF SURGEONS NATIONAL QUALITY IMPROVEMENT PROGRAM FOR MONITORING EPIDEMIOLOGIC CHANGES IN SURGICAL SITE INFECTIONS.
Javariah I. Asghar, MD, MPH, Uroghupatei P. Iyegha, MD, Catherine L. Statz, RN, MPH, James J. Glover, BSc, Jeffrey G. Chipman, MD, Gregory J. Beilman, MD. University of Minnesota
P56. ERBB4 IS UPREGULATED IN A MOUSE MODEL OF NECROTIZING ENTEROCOLITIS
Shannon L. Castle, MD, Jessica K. Bernard, BS, Monica Williams, BS, Anatoly V. Grishin, PhD, Henri R. Ford, MD, MHA, Mark R. Frey, PhD. University of Southern California Keck School of Medicine-Childrens Hospital Los Angeles
P57. ANTISEPTIC WOUND CARE POLICY CONTRIBUTES TO REDUCTION OF SSI'S AND INCREASED TRANSPLANT SURVIVAL
Kaysie L. Banton, MD, Catherine L. Statz, RN, PHN, MPH, Jeffrey G. Chipman, MD, James J. Glover, BS, Gregory J. Beilman, MD. University of Minnesota
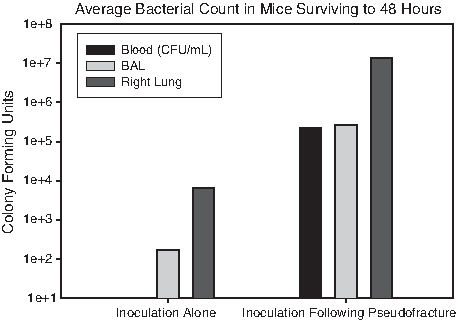
P58. PSEUDOFRACTURE: A MODEL FOR LATE POST-TRAUMATIC IMMUNOSUPPRESSION.
Sophie S. Darwiche, MD, Marcus K. Hoffman, MD, John P. Pribis, BSc, Xinmei Zhu, PhD, Juan B. Ochoa, MD, Timothy R. Billiar, MD. University of Pittsburgh
P59. A SIMPLE SCREENING TOOL FOR THE EARLY IDENTIFICATION OF SEPSIS IN A NON-ICU SETTING
Elsie Gyang, Lisa Shieh, MD, PhD, Lynn Forsey, RN, PhD, Paul Maggio, MD, MBA. Stanford University
P60. LINEZOLID INSENSITIVITY IN BACTERIAL ISOLATES FROM TRAUMA PATIENTS: AN UNCOMMON OCCURRENCE?
George O. Maish, MD, Chris Wood, PharmD, Tiffany Bee, MD, Benjamin Zarzaur, MD, Louis J. Magnotti, MD, Thomas Schroeppel, MD, Gayle Minard, MD, Martin A. Croce, MD, Timothy C. Fabian, MD. University of Tennessee Health Science Center, Memphis
P61. RISK FACTORS FOR MORTALITY IN PATIENTS ADMITTED WITH THE PRIMARY DIAGNOSIS OF CLOSTRIDIUM DIFFICILE COLITIS: A RETROSPECTIVE COHORT STUDY USING NATIONWIDE INPATIENT SAMPLE (NIS) DATABASE
Nasim Ahmed, MD, Yen-Hong Kuo, PhD, Yen-Liang Kuo, MD, John M. Davis, MD. Jersey Shore University Medical Center
P62. HYPERGLYCEMIA EARLY POST BURN HAS LITTLE EFFECT ON THE RISK OF INFECTION AND DEATH
Carla M. Carvalho, MD, Palmer Q. Bessey, MD, MS, Roger W. Yurt, MD. Weill Cornell Medical College
P63. CAN PROTEOMICS IMPROVE THE PREDICTION OF BURNS MORTALITY? RESULTS FROM REGRESSION SPLINE MODELING
Celeste C. Finnerty, PhD, Hyunsu Ju, PhD, Heidi Spratt, PhD, Sundar Victor, Marc G. Jeschke, MD, PhD, Sachin Hegde, MD, Suresh K. Bhavnani, PhD, Bruce A. Luxon, PhD, Allan R. Brasier, MD, David N. Herndon, MD. University of Texas Medical Branch, Galveston-Shriners Hospital for Children
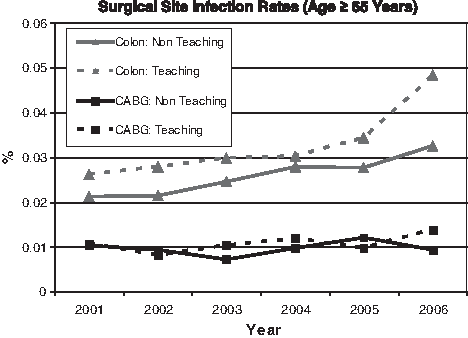
P64. SURGICAL SITE INFECTIONS IN ELECTIVE COLECTOMIES AND CABG: COMPARING AGE AND HOSPITAL TEACHING STATUS USING NIS DATA 2001-2006
John M. Davis, MD, Yen-Hong Kuo, PhD, Nasim Ahmed, MD, Yen-Liang Kuo, MD, Jersey Shore University Medical Center
P65. ERTAPENEM FOR THE TREATMENT OF PERFORATED APPENDICITIS IN CHILDREN
John D. Rutkoski, MD, Barbara A. Gaines, MD. University of Pittsburgh-Childrens Hospital of Pittsburgh
P66. FACTORS ASSOCIATED WITH POSTOPERATIVE PNEUMONIA IN PATIENTS WITH OPEN LUNG RESECTION: A RETROSPECTIVE COHORT STUDY USING 2006 NATIONWIDE INPATIENT SAMPLE
Yen-Hong Kuo, PhD, Yen-Liang Kuo, MD, Nasim Ahmed, MD, John M. Davis, MD. Jersey Shore University Medical Center
P67. CRITICAL CARE RESOURCE UTILIZATION IN SEVERE ARDS PATIENTS WITH 2009 INFLUENZA A (H1N1)
Muhammad F. Masood, MD, Pauline Park, MD, Lena M. Napolitano, MD. University of Michigan
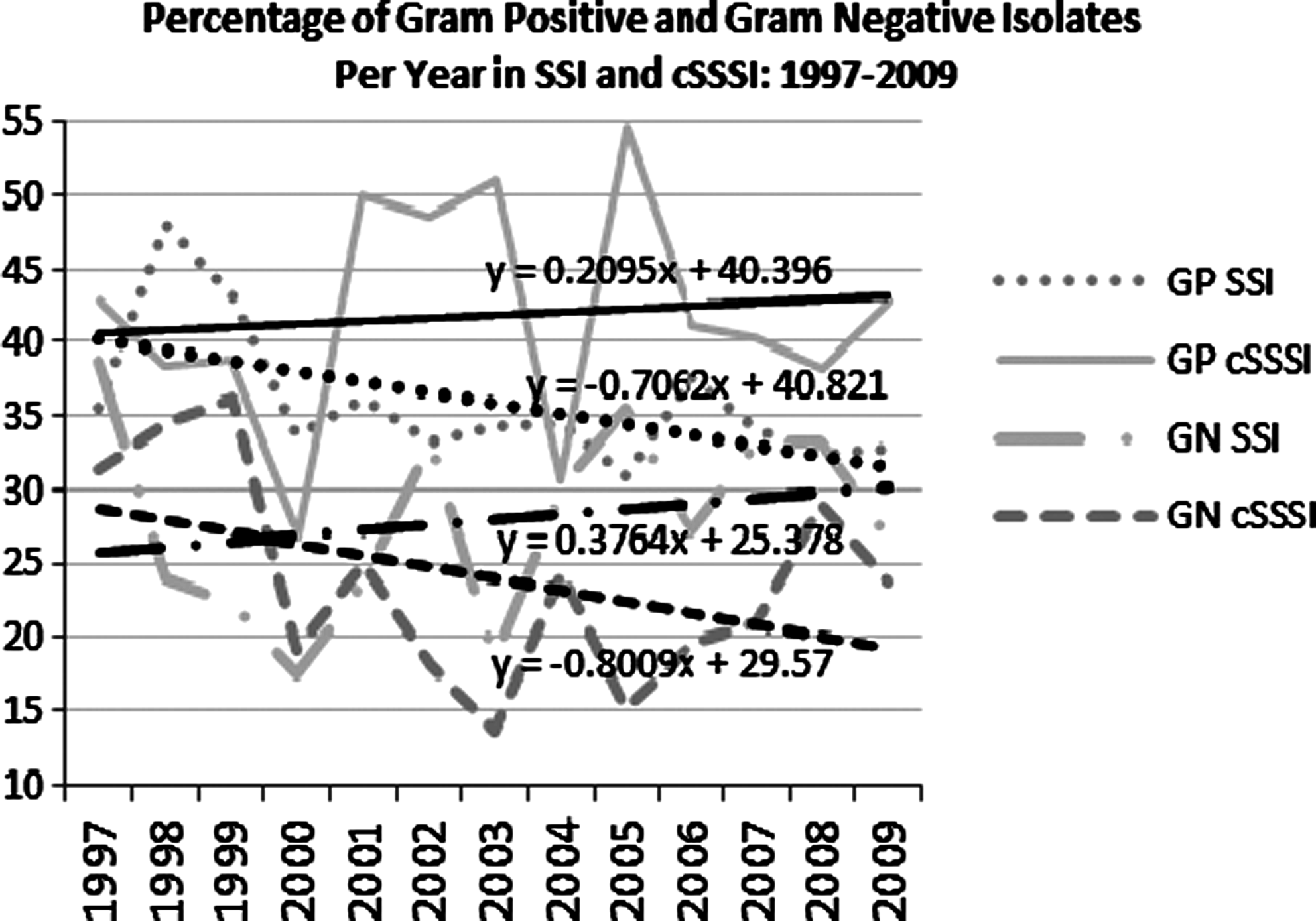
P68. EPIDEMIOLOGICAL TRENDS IN SURGICAL INFECTIONS OF THE SKIN
Lin M. Riccio, MD, Tjasa Hranjec, MD, MS, Robert G. Sawyer, MD. University of Virginia
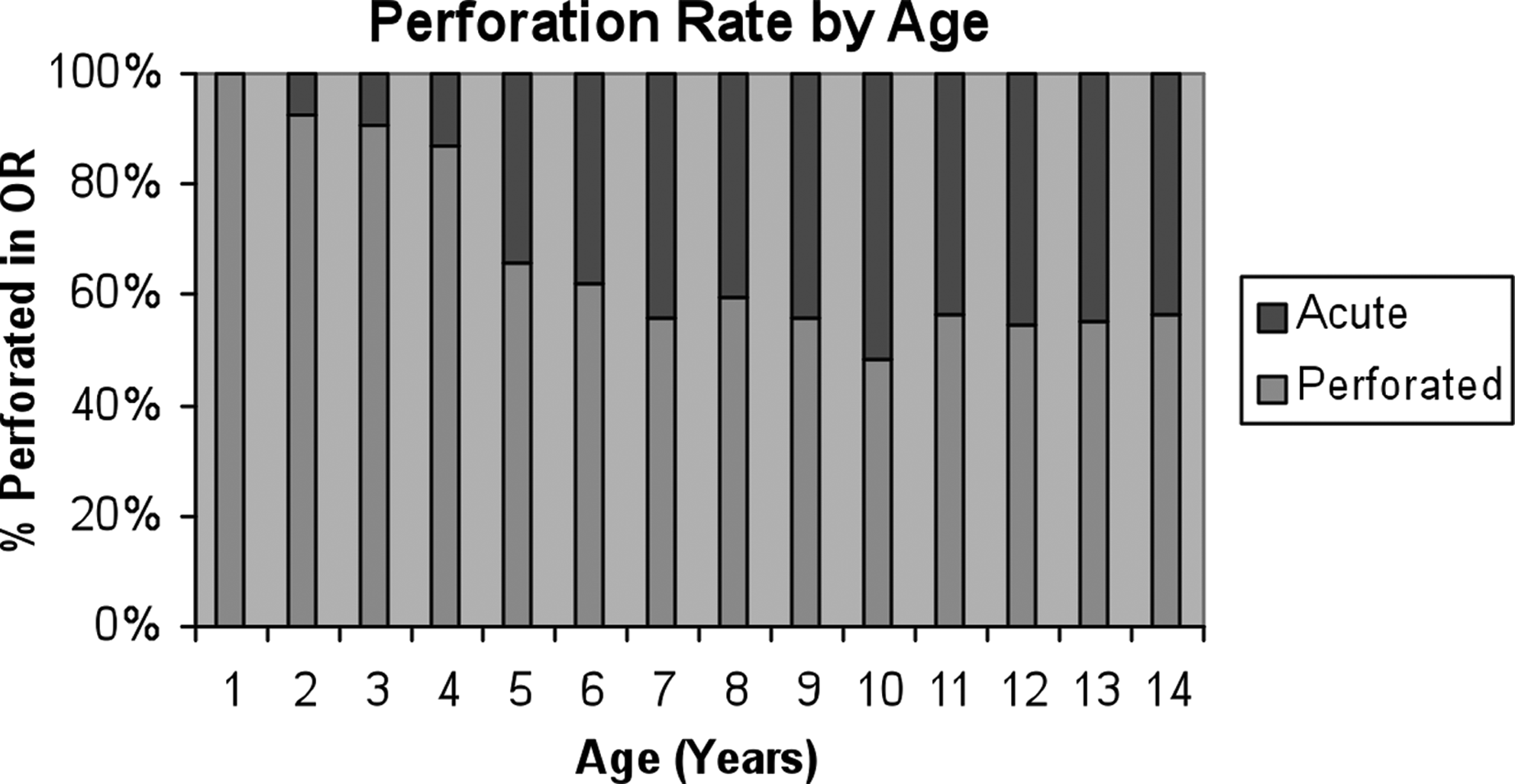
P69. APPENDICITIS PERFORATION RATES BY YEAR OF AGE
Lauren B. Nosanov, BA, Irene T. Ma, MD, Jeffrey S. Upperman, MD, Henri R. Ford, MD, MHA, James R. Pierce, MD. University of Southern California Keck School of Medicine
P70. NON-THERMAL FLOATING ELECTRODE-DBD-PLASMA: A NOVEL APPROACH TO CONTROL BACTERIA IN BIOFILMS
Utku K. Ercan, BS, Greg Fridman, PhD, Ari D. Brooks, MD, Suresh G. Joshi, MD, PhD. Surgical Infections Research Program, Drexel University
P71. ANTIBODY RESPONSES NOT LIKELY TO AFFECT EFFICACY AND SAFETY OF E-101 SOLUTION, A NOVEL MYELOPEROXIDASE (MPO)-BASED TOPICAL ANTISEPTIC FOR PREVENTION OF INCISIONAL INFECTIONS
Peter O'Hanley, Matt Pete, Kelly O'Hanley, Les Sabo, Robert Allen, and Jackson T. Stephens, Jr. Exoxemis, Inc., Little Rock, AR and Creighton University School of Medicine
17:30–18:30
SIS ANNUAL BUSINESS MEETINGPresiding: Henri R. Ford MD, MHA
Flagler Room
19:00–20:00
RECEPTION
Pool Terrace
20:00–22:00
AWARDS BANQUET
Royal Poinciana Ballroom
SATURDAY, May 14, 2011
07:00–08:00
SIS COUNCIL MEETING
Banyan Room
08:00–10:00
COMBINED SESSION IMechanistic Insights into the Development of Surgical Infection (Papers 41-47)Moderators: James Lederer, PhD and Addison K. May, MD
Flagler Ballroom
O41. PREVENTING INJURY-ASSOCIATED SEPSIS BY REDIRECTING THE IMMUNE SYSTEM
Akinori Osuka, MD, Sarasijhaa K. Desikan, BS, Marc Hanschen, MD, Goro Tajima, MD, James A. Lederer, PhD. Harvard Medical School-Brigham and Womens Hospital (resident)
Discussant: Heidi Frankel, MD
O42. CHOLINERGIC REGULATION OF ANP SIGNALING DURING SEPSIS
Jason R. Fritz, MSBE, Robert Gersch, PhD, Shu Pan, BA, Jared M. Huston, MD. Stony Brook University School of Medicine
Discussant: Gary An, MD
O43. THE ROLE OF ANTIBIOTICS IN OPEN FRACTURES REVISITED: CHARACTERISTICS OF STAPHYLOCOCCUS AUREUS (SA) AND SUSCEPTIBILITY PROFILE
Carla C. Saveli, MD, Steven J. Morgan, MD, Robert W. Belknap, MD, Erin Ross, BS, Philip F. Stahel, MD, George W. Chaus, MD, Walter L. Biffl, MD, Connie S. Price, MD. University of Colorado-Denver
Discussant: Carl Hauser, MD
O44. A COMPARISON OF INFECTIONS IN SOLID ORGAN TRANSPLANT RECIPIENTS AND IMMUNOSUPPRESSED NON-TRANSPLANT SURGERY PATIENTS: DOES THE ALLORESPONSE MATTER?
Laura H. Rosenberger, MD, Kristin C. Turza, MD, Lin M. Riccio, MD, Amani D. Politano, MD, Robert G. Sawyer, MD. University of Virginia
Discussant: James Lederer, PhD
O45. THE RELATIONSHIP OF STRESS-INDUCED HYPERGLYCEMIA AND INFECTIOUS COMPLICATIONS IN NON-DIABETIC ORTHOPAEDIC TRAUMA PATIENTS
Justin E. Richards, MD, Rondi Kauffman, MD, MPH, William T. Obremskey, MD, MPH, Addison K. May, MD. Vanderbilt University Medical Center (resident)
Discussant: Heather L. Evans, MD
O46. ROLE OF FEEDING-INDUCED OXIDATIVE STRESS AND TLR-RESPONSE ON CELLULAR POPULATION DYNAMICS IN THE PATHOGENESIS OF NECROTIZING ENTEROCOLITIS: INSIGHTS FROM AN AGENT-BASED MODEL (resident)
Moses Kim, MD, Scott Christley, PhD, Donald Liu, MD, John C. Alverdy, MD, Gary An, MD. University of Illinois at Chicago and University of Chicago
Discussant: Jeffrey Upperman, MD
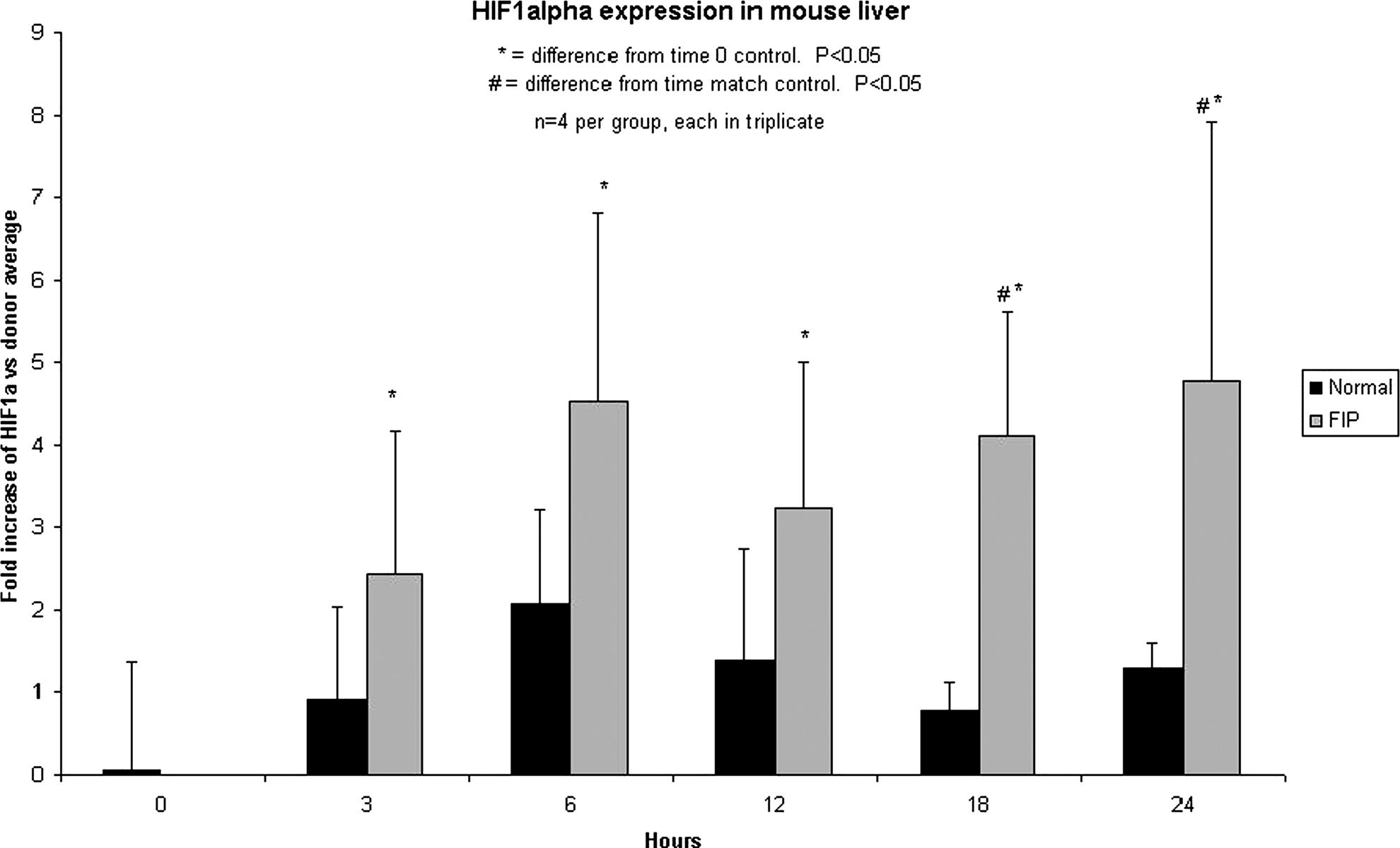
O47. THE ROLE OF HIF-1 IN THE PATHOGENESIS OF LIVER INJURY DURING SEPSIS
Brad Shrum, MSc, Tina Mele, PhD, MD. University of Western Ontario (new member)
Discussant: Brian Zuckerbraun, MD
10:00–10:15
BREAK–VISIT EXHIBITS
10:30–12:30
COMBINED SESSION IIClinical Investigations into Surgical Infections (Papers 48-56)Moderators: Donald E. Fry, MD and Jeffrey Claridge, MD, MS
Flagler Ballroom
O48. INITIATIONS OF QUALITY IMPROVEMENT MEASURES CAN LEAD TO DECREASING INFECTIOUS COMPLICATIONS IN EMERGENCY SURGICAL PATIENTS
Felix Akinbami, MBBS, MS, Jill Steinberg, RN, MPH, Maria Panizales, RN, MSN, Selwyn O. Rogers, Jr., MD, MPH, Reza Askari, MD. Department of Surgery and Center for Surgery and Public Health, Harvard Medical School-Brigham and Womens Hospital
Discussant: David T. Efron, MD
O49. MONTHLY PCR SCREENING FOR POLYOMA BK VIRUS WITH PRE-EMPTIVE IMMUNOSUPPRESSIVE THERAPY REDUCTION: LONG-TERM RESULTS AFTER RENAL TRANSPLANTATION
David J. Conti , Michael H. Gallichio, Nicholas Chandolias, Nicole Siparsky. Albany Medical College
Discussant: Robert G. Sawyer, MD
O50. INFECTIOUS OUTCOMES IN LIVING DONOR KIDNEY TRANSPLANT RECIPIENTS FOLLOWING MULTIMODAL PREOPERATIVE DESENSITIZATION TO OVERCOME HUMORAL BARRIERS
Kristin Turza Campbell, MD, Avinash Agarwal, MD, Michael Shafique, BS, Kenneth L. Brayman, MD, PhD, Robert G. Sawyer, MD. University of Virginia (resident)
Discussant: Donald E. Fry, MD
O51. COMPARING A LOCALLY-DERIVED VERSUS GUIDELINE-BASED APPROACH TO TREATMENT OF HOSPITAL-ACQUIRED PNEUMONIA IN THE TRAUMA INTENSIVE CARE UNIT
Robert D. Becher, MD, J. Jason Hoth, MD, PhD, Jennifer L. Kendall, BA, Jerry J. Rebo, PharmD, Preston R. Miller, MD. Wake Forest University School of Medicine (resident)
Discussant: Philip A. Efron, MD
O52. TLR4 PROTECTIVE ADJUVANT EFFECT TO MURINE POLYMICROBIAL SEPSIS IS TRIF, BUT NOT MYD88, DEPENDENT
Alex G. Cuenca, MD, James L. Wynn, MD, Kindra Kelly-Scumpia, PhD, Phillip O. Scumpia, MD, PhD, Dina C Nacionales, MD, Philip A. Efron, MD, Lyle L. Moldawer, PhD. University of Florida (resident)
Discussant: James Lederer, PhD
O53. HAND SANITIZER DISPENSERS AND ASSOCIATED HOSPITAL ACQUIRED INFECTIONS - FRIEND OR FOMITE?
Simon D. Eiref, MD, Robert C. Goldstein, MD, I. Michael Leitman, MD, William H. Riley, PhD, Albert Einstein College of Medicine-Beth Israel Medical Center (new member)
Discussant: Sandra Swoboda, RN, MS
O54. PERFORMANCE OF TWO SURGICAL SITE INFECTION RISK STRATIFICATION MODELS FOR PREDICTING INFECTION RISK IN PUBLICLY REPORTED DATA FROM A SAFETY NET HOSPITAL
Connie Savor Price, MD, Bryan Knepper, MS, M. Josh Durfee, MS, Heather Young, MD, Walter L Biffl, MD. University of Colorado-Denver Health Medical Center (new member)
Discussant: Heather L. Evans, MD
O55. THE EFFECT OF PROLONGED CORTISOL EXCESS ON SYSTEMIC AND CELLULAR RESPONSES TO ENDOTOXIN
Irina Bernescu, MD, Tara M. Balija, MD, Michael T. Reddell, Jacqueline E. Calvano, Susette M. Coyle, RN, Marie A. Macor, RN, Steve E. Calvano, PhD, Beatrice Haimovich, PhD, Stephen F. Lowry, MD, MBA. University of Medicine and Dentristry of New Jersey-Robert Wood Johnson Medical School (resident)
Discussant: Grant Bochicchio, MD, MPH
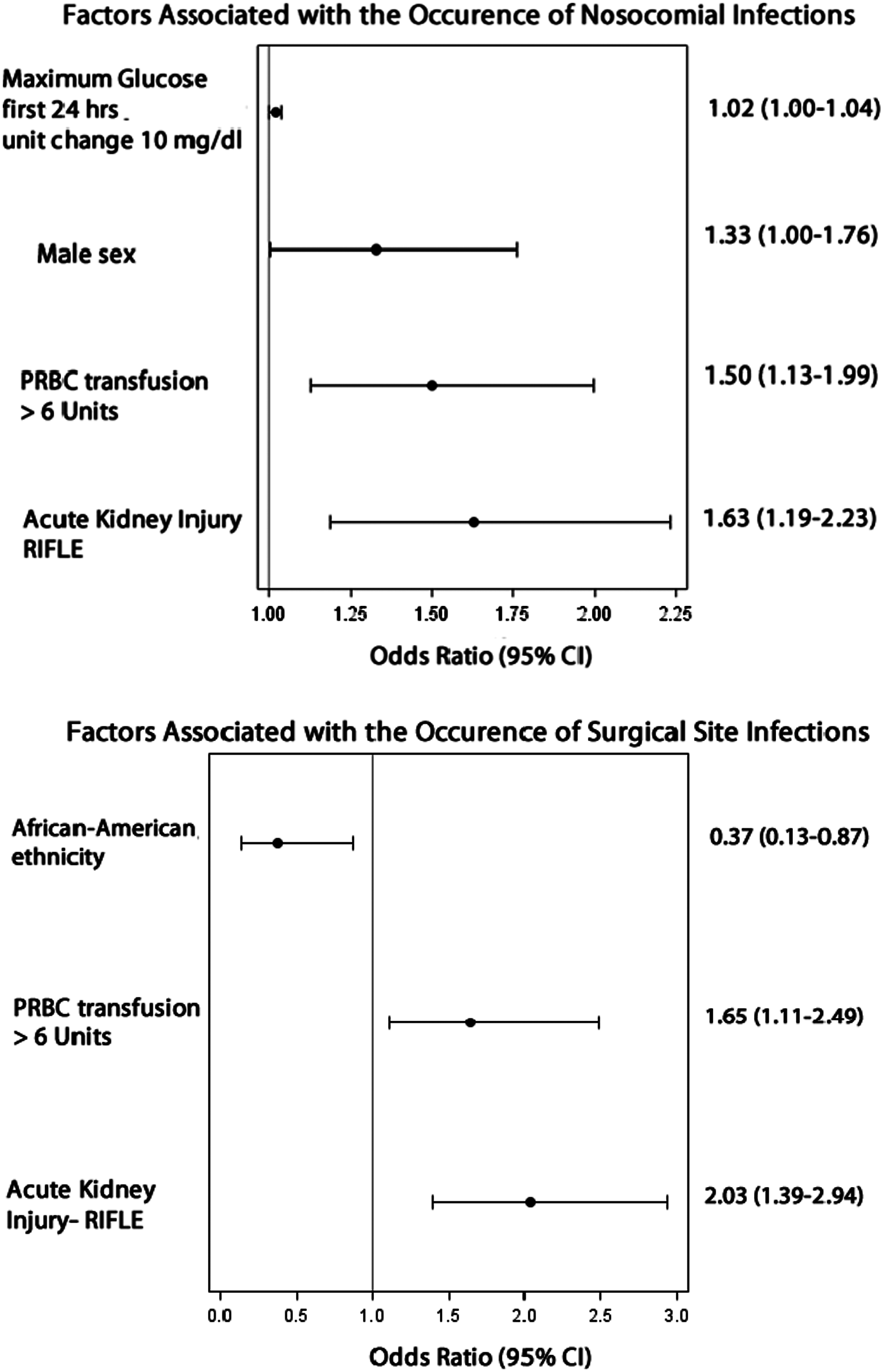
O56. ACUTE KIDNEY INJURY IS ASSOCIATED WITH NOSOCOMIAL INFECTIONS AND SURGICAL SITE INFECTIONS AFTER TRAUMA
Azra Bihorac, MD, Philip A. Efron, MD, Darwin Ang, MD, PhD, Ronald V. Maier, MD, Lyle L. Moldawer, PhD. University of Florida and University of Washington (new member)
Discussant: Therese M. Duane, MD
12:30
MEETING ADJOURNMENT
Oral Presentation Abstracts
Ortiz-PomalesYan T.MDReysLuis G.MDCheadleGerald A.BSKrzyzaniakMichael J.MDLopezNicole E.MDHagenyAnn-MarieBSEliceiriBrianPhDBairdAndrewPhDBansalVishalMDCoimbraRaulMD, PhD
University of California San Diego
Background: Trauma/Hemorrhagic shock (T/HS) induced gut injury is known to initiate a dysfunctional inflammatory response leading to secondary lung injury. Our group has shown that vagal nerve stimulation (VNS) protects the intestinal epithelial integrity, attenuates inflammatory cytokine formation, and protects the lung after a thermal insult. We hypothesize that VNS will protect the lung from injury following trauma/ hemorrhagic shock.
Methods: Male Balb/c mice were subjected to a trauma/hemorrhagic shock model (mean arterial pressure of 35 mmHg for one hour), with and without right cervical vagal nerve stimulation. A cohort of animals underwent abdominal vagotomy (Vx) at the gastro-esophageal junction prior to vagal nerve stimulation and trauma/hemorrhagic shock. Lung histology (H&E), myeloperoxidase (MPO) and ICAM-1 immuno-staining, and MPO enzymatic assay were analyzed 24 hours post-shock in all groups. Using NF-kβ-luciferase transgenic mice, NF-kβ-DNA binding was also analyzed by photon emission analysis (Ivis Spectrum) at 4hrs.
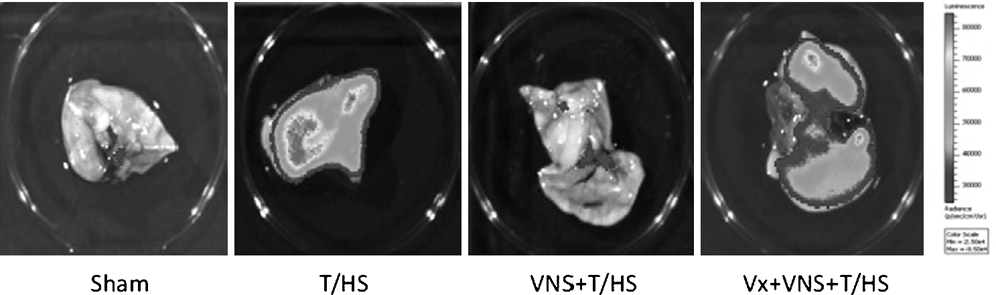
Results: T/HS caused acute lung injury at 24 hours characterized by: 1) pulmonary edema, alveolar hemorrhage and intra alveolar hyaline membrane formation, 2) increased number of MPO positive stained cells and MPO enzymatic activity, and 3) increased ICAM-1 expression in lung endothelium. Vagal nerve stimulation abated these lung injury patterns. Lung tissue analysis at 24hrs post VNS + T/HS showed: 1) H&E histology compared to Sham, 2) marked decrease in PMN infiltration demonstrated by MPO immune staining and MPO enzymatic activity, and 3) decreased ICAM-I expression. Lungs at 4hrs post VNS + T/HS demonstrate decreased DNA binding of inflammatory protein NF-kB; in the images below, red colors represent more intensity and more luminescence expressed as photons/sec/cm2/sr (see figure). Abdominal vagotomy blunted the protective effects of VNS in all experiments, with results comparable to the T/HS group.
Conclusion: Vagal nerve stimulation is effective in protecting against acute lung injury post-hemorrhagic shock. The protective properties of vagal nerve stimulation seem to be applicable in more than one shock model, providing promising potential for clinical applicability.
KraftRobertMDHerndonDavid N.MDBranskiLudwikMDFinnertyCeleste C.PhDJeschkeMarc G.MD, PhD
University of Texas Medical Branch, Galveston
Outcomes of Optimized Fluid Resuscitation after Severe Burn Injury Utilizing Hemodynamic Measurements by Transpulmonary Thermo-Dilution
Introduction: One of the crucial factors in the successful treatment of severe burns is appropriate fluid resuscitation during the initial phase following injury. At present, the calculation of fluid resuscitation is based on calculations of body weight, burn size and urinary outputs as accurate assessment systems of hydration status are not available. Optimizing the guidance of fluid administration during the critical initial phase would have beneficial effects on the outcome of burned patients. The aim of this study was to assess the benefit of utilizing transpulmonary thermo-dilution by a Pulse Contour Cardiac Output (PiCCO) system for optimized resuscitation.
Methods: A cohort of seventy-six severely burned pediatric patients with burns over 30% total body surface area who received adjusted fluid resuscitation by PiCCO (P) measurements were compared to 76 conventionally monitored patients (C) with similar injury characteristics. Clinical hemodynamic measurements, organ function (DENVER2 score), and biomarkers were recorded prospectively for the first 20 days after burn injury. Statistical analysis was performed using student's t-test and chi-square test as appropriate with significance set at p < 0.05.
Results: Both patient groups were similar in demographic and injury characteristics. Patients who received PiCCO-adjusted resuscitation showed a remarkable reduced incidence of sepsis (P: 9%, C: 17%) and mortality (P: 16%, C: 25%), as well as a significantly lower incidence of cardiac and renal failure during acute hospitalization. Patients in the P group received significantly less fluids (p < 0.05) at similar urinary output, resulting in a significantly lower positive fluid balance (p < 0.05). The CVP in the P group was maintained in a significantly more narrow range (p < 0.05), combined with a significantly lower heart rate at similar systemic blood pressure levels (p < 0.05).
Conclusions: Fluid resuscitation guided by transpulmonary thermo-dilution contributes to superior fluid management and balance during the critical initial phase after burn injury and results in beneficial effects on morbidity and mortality.
ZhangLemengMDPanPinhuaMDCardinalJonMDNaceGaryMDEvankovichJohnBilliarTimothyMDTsungAllanMD
Department of Surgery, University of Pittsburgh
Interferon Regulatory Factor-1(IRF-1) Mediates Splenocytes and Macrophages Apoptotic and Autophagic Responses in Endotoxemia
Objectives: The pathogenesis of sepsis is complex and unfortunately poorly understood. Recent studies indicate that an immunosuppressive status due to immune effecter cells apoptosis may contribute to sepsis related mortality. Another cellular process, autophagy, is also activated in sepsis and is primarily believed to play a protective role in the disease progression. Apoptosis and autophagy share a number of common signaling mediators. However, the upstream regulator of these two cellular processes is still incompletely defined. Interferon regulatory factor-1 (IRF-1) functions as pro-apoptotic signal. The function of IRF-1 in regulating autophagy has not been shown. In this study, we hypothesized that IRF-1 may participate in the regulation of both apoptotic and autophagic responses in lymphocytes and macrophages in the model of endotoxemia.
Methods: Male IRF-1 knockout (KO) mice and wild type C57BL/6 countertypes received LPS (20 mg/kg) intraperitoneal injection. Control mice received sterilized PBS. Lung was harvested for histopathology assessment. Spleen was harvested 16 h following LPS administration and analyzed by flow cytometry, western blot (WB), TUNEL staining, immunohistochemistry (IHC) and transmission electron microscope (TEM). In vitro, splenocytes and peritoneal macrophages were harvested and stimulated with LPS, and then were analyzed by WB and immunofluorescent microscope (IM). Raw 264.7 cell was infected by Ad IRF-1 and stimulated with SNAP, then were analyzed by WB, high content screening and caspase-3 activity.
Results: In vivo, IRF-1 KO mice were significantly protected from endotoxin induced mortality (p < 0.05) and acute lung injury. This protection was associated with less splenocytes apoptosis as demonstrated by decreased Annexin V positive cells, fewer TUNEL positive cells, less cleaved caspase-3 staining and decreased apoptotic bodies. Conversely, both splenocytes and peritoneal macrophages from IRF-1 KO mice exhibited evidence of increased autophagic flux as measured by LC3 II activation and p62, increased LC3 spots and increased mitophagy. In vitro, LPS induced IRF-1 activation occurred in a TLR4 dependent, TRIF dependent, MyD88 independent manner. To further explore the mechanism of how IRF-1 modulates autophagy and apoptosis, murine macrophages cell line Raw 264.7 cells were chosen. IRF-1 overexpression inhibits autophagy through the activation of mTOR/p70S6 signaling pathway. On the other hand, IRF-1 participates in both extrinsic and intrinsic apoptotic pathway. Furthermore, iNOS/NO is well demonstrated downstream of IRF-1. SNAP, a NO donor, can mimics the effects seen in IRF-1 WT immune cells, promoting extrinsic/intrinsic apoptotic pathway and inhibiting autophagy.
Conclusion: IRF-1 and NO play a pivotal role in the pathogenesis of endotoxemia by impacting two major mechanisms of cell death/survival, apoptosis and autophagy. IRF-1/NO appears to shift the balance to apoptosis, while IRF-1 depletion results in the opposite effect. Understanding the regulation of IRF-1 activity may serve as a target to improve sepsis related outcomes.
FlynnLisaMDZimmermanLisa HallPharmDRoseAlexanderMDZhaoJingPharmDWahbyKristaPharmDDotsonBryanPharmDWilsonRobertMDTennenbergStevenMD
Wayne State University School of Medicine
Vascular Catheter Cultures for Suspected Catheter-Related Bloodstream Infection in the ICU: A Tradition whose Time has Passed?
Introduction: Catheter-related bloodstream infection (CR-BSI) associated with central venous catheters is estimated to occur in 80,000 intensive care unit (ICU) patients each year in the USA. While traditional epidemiological criteria require matching catheter and blood culture (cx) organisms, more recent criteria only require bacteremia and the absence of an identified alternative source. Clinically, bacteremia from any known pathogen necessitates antimicrobial therapy, regardless of catheter cx results. We sought to expand our previous database and explore the clinical utility of vascular catheter cxs in critically ill patients.
Methods: We retrospectively evaluated all positive (>15 colony forming units by semiquantitative roll-plate technique) vascular catheter tip cultures (CTCs) from 2006 through 2009 from eight mixed medical-surgical and specialty ICUs in two academic hospitals. CR-BSI was defined as a matching positive blood cx obtained up to four days before or two days after catheter removal. Catheter removal was categorized as either empiric (catheter pulled before blood cx reported positive) or clinical (catheter pulled after blood cx reported positive). The time interval from catheter removal and blood cx draw (empiric) or blood cx positivity (clinical) was determined. Antimicrobial appropriateness was assessed.
Results: 1391 CTCs were obtained during the four year study period. 588 (42%) were negative, 335 (24%) were colonized (<15/roll), and 468 (34%) were positive. There were 143 cases of CR-BSI, representing 10% of all CTCs and 31% of positive CTCs.
P < 0.001 vs Empiric by Student's t-test, Power = 1.0.
In 130 (91%) of 143 cases of CR-BSI, the positive blood culture was drawn before or within 24 hrs of the catheter's removal and dictated antimicrobial therapy. In only 13 (9%) of 143 cases of CR-BSI did the catheter's removal and culture significantly (>1 day) precede the positive blood culture. 55% of CTCs were obtained empirically and with a significantly shorter time interval than those removed clinically. Antimicrobial therapy was deemed appropriate in 87% of CR-BSI cases. 32% of positive CTCs had > two organisms identified. The microbiology laboratory costs to process all CTCs, including organism identification, sensitivity testing and labor were approximately $75,300 and required 600 microbiology technician hours.
Conclusion: In our mixed ICU patient population, 34% of vascular catheters removed were culture positive. Only 31% of positive CTCs were associated with CR-BSI. 91% of all CR-BSIs were identified by bacteremia either prior to or coinciding with catheter removal. Antecedent or concomitant bacteremia, and not the CTC, dictated antimicrobial therapy. Therefore, routine culturing of vascular catheters in cases of suspected CR-BSI in the ICU is of negligible clinical (treatment) utility. Our data suggest that the traditional practice of obtaining CTCs in the ICU should be reconsidered.
TiesiGregoryMDReinoDiegoMDPalangeDaveBSLuQiMDMasonLeonardMDShethSharvilMDTomaioJacquelynBSAroraNickBSDeitchEdwinMD
UMDNJ-NJMS Department of Surgery
Immune Cell Apoptosis is Triggered by Shock Mesenteric Lymph and is Mediated through the TLR4 Pathway
Background: Recent literature has shown that in sepsis and hemorrhagic shock there is an associated increase in apoptosis of immune cells in animal models as well as human patients and some studies have correlated this with adverse outcomes in critically ill septic patients. However, to date, the potential trigger inducing this phenomenon is unknown.
Hypothesis: 1) Immune cell apoptosis that occurs after shock is triggered by factors carried in the mesenteric lymphatic system. 2) Immune cell apoptosis that occurs after shock is mediated through the TLR4 receptor pathway.
Methods: In experiment #1, male SD rats were subjected to trauma (laparotomy) plus hemorrhagic shock (30-35 mmHg for 90 minutes; T/HS) or T/HS plus mesenteric lymph duct ligation (LDL). A third group, trauma-sham shock (T/SS) was used as controls. Animals were sacrificed at 3 and 24 hours post shock, spleens and thymi were harvested and assessed for apoptosis by TUNEL and Caspase-3 immunohistochemistry (IHC). In experiment #2, male C57bl mice were challenged with T/HS or T/SS lymph (0.03 ml/gm over 3 hours) followed by sacrifice. The spleen was harvested and assessed for apoptosis via TUNEL and IHC. In experiment #3, TLR4 WT or KO animals were subjected to actual T/HS or received T/HS or T/SS lymph. Animals were sacrificed at 3 hours and spleens were harvested and assessed for apoptosis using TUNEL and IHC.
Results: Due to spatial limitations only the 3-hour TUNEL data will be presented, although similar statistical observations were seen with Caspase-3 and at 24 hours. Splenic and thymic apoptosis was 2-3 fold higher in rats subjected to T/HS (11.07 + 2.8 cells/hpf, 27.94 + 2.41 cells/hpf) than T/SS (5.78 + 0.49 cells/hpf, 8.42 + 1.92 cells/hpf). T/HS + LDL prevented the apoptotic response (6.51 + 1.04 cells/hpf, 11.82 + 2.70 cells/hpf), p < 0.01. Injection of T/HS lymph into C57bl mice increased splenic TUNEL levels compared to mice injected with T/SS (36.55 + 9.04 cells/hpf vs. 20.12 + 5.71 cells/hpf), p < 0.001. This indicated that T/HS lymph is sufficient by itself to cause apoptosis.
Lastly, we found that splenic apoptosis was decreased in the TLR4 KO mice compared to their WT littermates after actual T/HS or after being challenged with T/HS lymph (Table)
p < 0.01, **p < 0.001, Data for T/SS and T/SS lymph injection in the WT or KO mice are not shown. They are not statistically significantly different from the TLR4 KO mice.
Conclusion: 1) T/HS leads to the development of immune cell apoptosis and LDL abrogates those effects suggesting that factors carried in the mesenteric lymphatics after shock contribute to immune cell apoptosis and may be a direct trigger. In addition, splenic apoptosis can be recreated with T/HS lymph injection which further supports this hypothesis. 2) TLR4 KO animals did not show increased apoptosis with T/HS or T/HS lymph injection suggesting that immune cell apoptosis is mediated through the TLR4 pathway.
PolitanoAmani DMDHranjecTjasaMD, MSRosenbergerLaura HMDCampbellKristin TMDRiccioLin MMDStukenborgGeorge JPhDSawyerRobert GMDTache-LeonCarlos AMD
University of Virginia Department of Surgery
Fungus in the Abdomen: Who has it, is it Lethal, and does it Matter if we Treat it?
Introduction: In intra-abdominal infections, empiric antibiotics are started until definitive treatment can be employed. Whether antifungal treatment is included is often decided prior to culture availability and based on poorly delineated clinical characteristics. The efficacy of antifungal therapy in these patients is unproven. We hypothesized that isolation of fungus from intra-abdominal infections can be predicted by the organ of origin and hospitalization status at time of infection, that mortality is increased in these patients, and that early antifungal therapy improves patient survival.
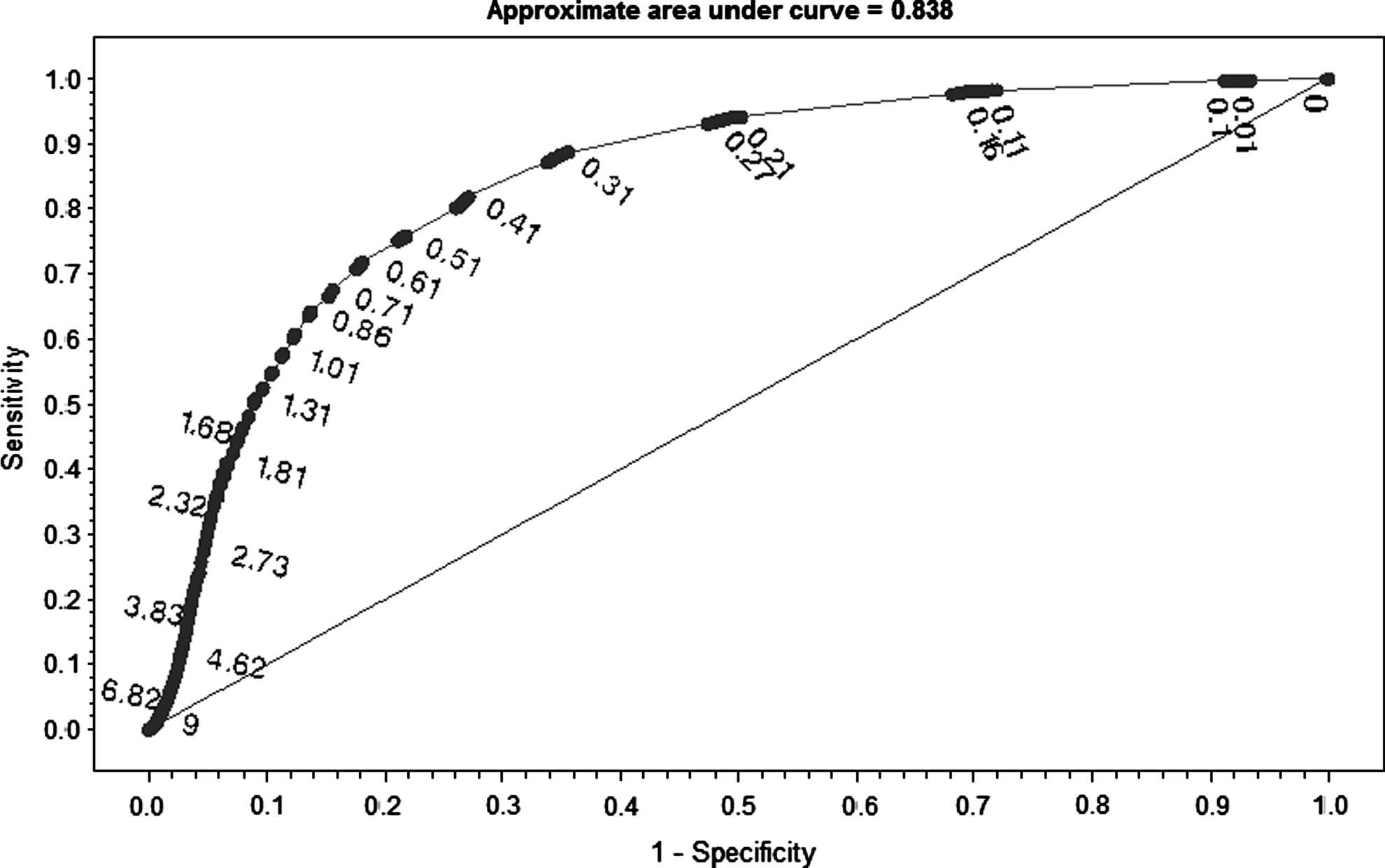
Methods: All intra-abdominal infections in patients treated between December 1996 and September 2010 in a single large tertiary care hospital were identified and classified by presence of fungus by culture results. Logistic regression was used to estimate the probability of fungal infection based on patient demographics, comorbidities, nosocomial nature, previous operation, and the organ of origin. The discriminatory function of the statistical model was measured using the C statistic. The independent contribution of each covariate to the predictive model was assessed using the Wald Chi-square test, and the effects of individual covariates were expressed as odds ratios. All-cause in-hospital mortality was assessed according to presence or absence of fungus by Kaplan-Meier analysis. Logistic regression with propensity score matching by treatment group was performed to further assess contributors to mortality.
Results: We identified 3050 infections. Demographic information is shown (table). The predictive model for fungal infection demonstrated adequate performance (c-statistic 0.692), and identified duodenal origin (OR 2.58, CI 1.40-4.76), nosocomial infection (1.88, 1.38–2.57), and previous operation (1.58, 1.23–2.04) as the most significant contributing variables. All-cause in-hospital mortality was not affected by isolation of fungi. Crude mortality was higher for patients who received antifungal therapy for all infections (16.1% vs. 6.2%, p < 0.0001) and mixed bacterial/fungal infections (18.9% vs. 7.2%, p = 0.01), but not for fungi alone (17.5% vs. 0%, p = 0.28). After propensity score matching (n = 1344, c-statistic 0.882), the variables associated with mortality were age (1.05, 1.03–1.07), liver disease (32.28, 6.38–163.30), Crohn's disease (0.12, 0.02–0.64), and transfusion (3.80, 2.27–6.36), but not presence of fungus (1.40, 0.77–2.53) or treatment with antifungals (1.20, 0.80–1.81).
Mean ± SE, *Independent t-test, †Chi-square w/ Yates correction.
Conclusion: Duodenal source, nosocomial origin, and prior surgery are risk factors for isolation of fungi from an intra-abdominal infection. Patient mortality is not dependent on the presence of fungus. We were unable to demonstrate that treatment with antifungal medications contributed to improved outcomes in any group. Patients with higher mortality likely have more severe illness unrelated to the presence or treatment of fungi.
ZaborinAlexander VPhDHolbrookChristopherMDLiuDonaldMD, PhDZaborinaOlga YPhDAlverdyJohn CMD
University of Chicago
P. Aeruginosa Expresses a Lethal Phenotype in Response to a Delicate Balance between Local Phosphate Concentration and Exposure to Kappa Opioids
Introduction: From the standpoint of colonizing microbes, the intestinal tract of a critically ill host represents hostile, nutrient scarce environment in which their virulence circuitry can be activated by secreted host factors (i.e cytokines, ischemic end-products, opioids) and physico-chemical “cues” (i.e low phosphate). Using Pseudomonas aeruginosa as the model pathogen, we created nutrient depleted conditions and determined whether this pathogen processes multiple cues within the local environment (i.e phosphate and the specific kappa-opioid U-50,488) to induce a lethal phenotype from within the digestive tube of the nematode C. elegans.
Methods: C. elegans were allowed to feed on P. aeruginosa pre-grown in nutrient poor media (0.1xTY tryptone, 1 g/L, yeast extract 0.5 g/L) supplemented with either 0.1 mM or 25 mM inorganic phosphate and 200 μM U-50,488 and followed for mortality. Genome wide transcriptional analysis, direct virulence factor production (pyocyanin, pyoverdin) and transmission electron microscopy (TEM) were assessed and correlated to lethality. Based on the above analysis, various mutants of P. aeruginosa were screened in reiterative C. elegans killing assays to identify the key genes and pathways involved in lethality and verified using complementary bioluminescent reporter strains of P. aeruginosa.
Results: Growth in nutrient poor media prevented P. aeruginosa from reaching high cell density (i.e quorum sensing activation) and therefore all experiments were performed at low cell density (OD 600 nm = 0.2–0.3). Under these conditions C. elegans displayed high mortality (∼80% at 24 hrs) when P. aeruginosa was exposed to U-50,488, low mortality (∼20%) in the absence of U50,488, and low (∼10%) mortality when exposed to U50,488 but under high phosphate conditions (25 mM) (n = 50/group, p < 0.01). TEM revealed active formation of flagella and the production of secreted microbial exoproducts (vesicles) during exposure to U-50488 and low phosphate conditions which was prevented when phosphate conditions remained high (i.e 25 mM). Direct assay revealed increased production of pyocyanin and pyoverdin under similar media conditions (p < 0.001). Microarray analysis revealed significant and robust expression of genes encoding multiple virulence factors including pyocyanin, cyanide, proteases, siderophores, and antibiotic resistance Mex pumps among others during low phosphate and U-50488 exposure. Mutational analysis identified PqsE (pqs operon) as a key regulator involved in the development of a lethal phenotype. Use of a bioluminescent reporter to measure the expression of the pqs operon revealed that U-50,488 significantly increased pqs expression in response to exogenous administration of a cognate quorum sensing (QS) signaling molecule HHQ suggesting that kappa opioids enhance P. aeruginosa sensitivity to their own QS signals in a phosphate dependent manner.
Conclusion: These results demonstrate multi-component context dependent virulence activation in P. aeruginosa whereby additive cues can induce a lethal phenotype. Host factors secreted in response to stress such as opioids are directly processed by key regulators of the quorum sensing systems resulting in enhanced virulence. This effect appears to be abrogated during phosphate abundance and highlights the important of understanding bacterial information processing at the molecular level.
HeffernanDaithi SMDMonaghanSean FMDGreggZachMDConnollyMichael DMDGreggSheaMDAdamsCharles AMDCioffiWilliam GMD
Brown University, Rhode Island Hospital
The Chasm Between CDC Diagnosis and Bronchoalveolar Lavage Diagnosis of Vap May Affect Payments for Critically Ill Trauma Patients
Background: The chasm between CDC diagnosis and Bronchoalveolar lavage diagnosis of VAP may affect payments for critically ill trauma patients.
Background: Ventilator Associated Pneumonia (VAP) remains a significant cause of morbidity and mortality in trauma patients but despite this, there is no gold standard for the diagnosis of VAP. A significant discrepancy exists between diagnosis of VAP made by Infection Control (IC) Departments relying on CDC criteria and clinical diagnosis based on quantitative broncheoalveolar lavage (BAL). Trauma patients typically have significant pathology on chest radiographs secondary to their traumatic insult that confounds diagnosing VAP. The heavy reliance of the IC definition of VAP upon changing pulmonary infiltrates or worsening chest radiographs potentially leads to higher false positive rates in trauma patients. Conversely, the absence of terms suggestive of pneumonia on a radiology report trigger leads to under-diagnosing VAP by IC's methods. In light of potential non-payment for secondary diagnoses of VAP due to the Center for Medicare/Medicaid Service's “Never Events”, physicians may be faced with the impossible choice of treating their patient or ruining their institution's financial health.
Materials and Methods: this is a retrospective chart review of all intubated trauma patients over the last 3 years. The Infection Control (IC) database, which relies upon the CDC criteria to diagnose VAP, was compared to the clinical practice of the trauma team which relies on quantitative BALs to diagnose pneumonia. Patients with suspected VAP underwent BAL, and this was considered positive for pneumonia if the microbiology data returned with > / = 100,000 colony forming units per ml. The IC database was reviewed to assess why patients with negative BAL were assigned a diagnosis of VAP by IC and the clinical chart was reviewed to assess why BAL positive patients were considered negative for VAP by IC practioners.
Results: Over the study period, 48 patients were diagnosed with pneumonia by IC. 13 of these 48 patients (27%) had a negative BAL, never underwent BAL, or were never treated for pneumonia by the trauma team. Among these 13 patients, the most common reasons cited in the IC database for diagnosing pneumonia were “radiology report stating evolving infiltrate suggestive of pneumonia” (13/13 patients) and “worsening ventilator settings” (8/13 patients). Over the same period, 154 patients were diagnosed with pneumonia via BAL by the trauma team. 119 of these 154 patients (77%) were considered negative for pneumonia by IC. The predominant reasons for IC not diagnosing pneumonia included a lack of significant change in radiology reports, and under-appreciation of increasing ventilator requirements (change of mode of ventilation, rising PEEP and FiO2 requirements).
Conclusions: There is a clear discrepancy between VAP diagnosed by IC and the trauma team. This discrepancy may have several untoward effects including improper denial of payment, or adverse quality indicators for VAP in Trauma Intensive Care Units (TICU). The CDC and IC practioners need to recognize that VAP is much bigger problem in TICUs and should acknowledge that VAP can never be “Never Event” and adjust their definitions and expectations accordingly.
EmamiClaudia NMD, MPHMittalRahulPhDFordHenri RMD, MHAPrasadaraoNemani VPhD
CHLA-USC Keck School of Medicine
TGF Beta Expression is Required for Enterobacter Sakazakii-Induced Epithelial Injury in a Mouse Model of Necrotizing Enterocolitis
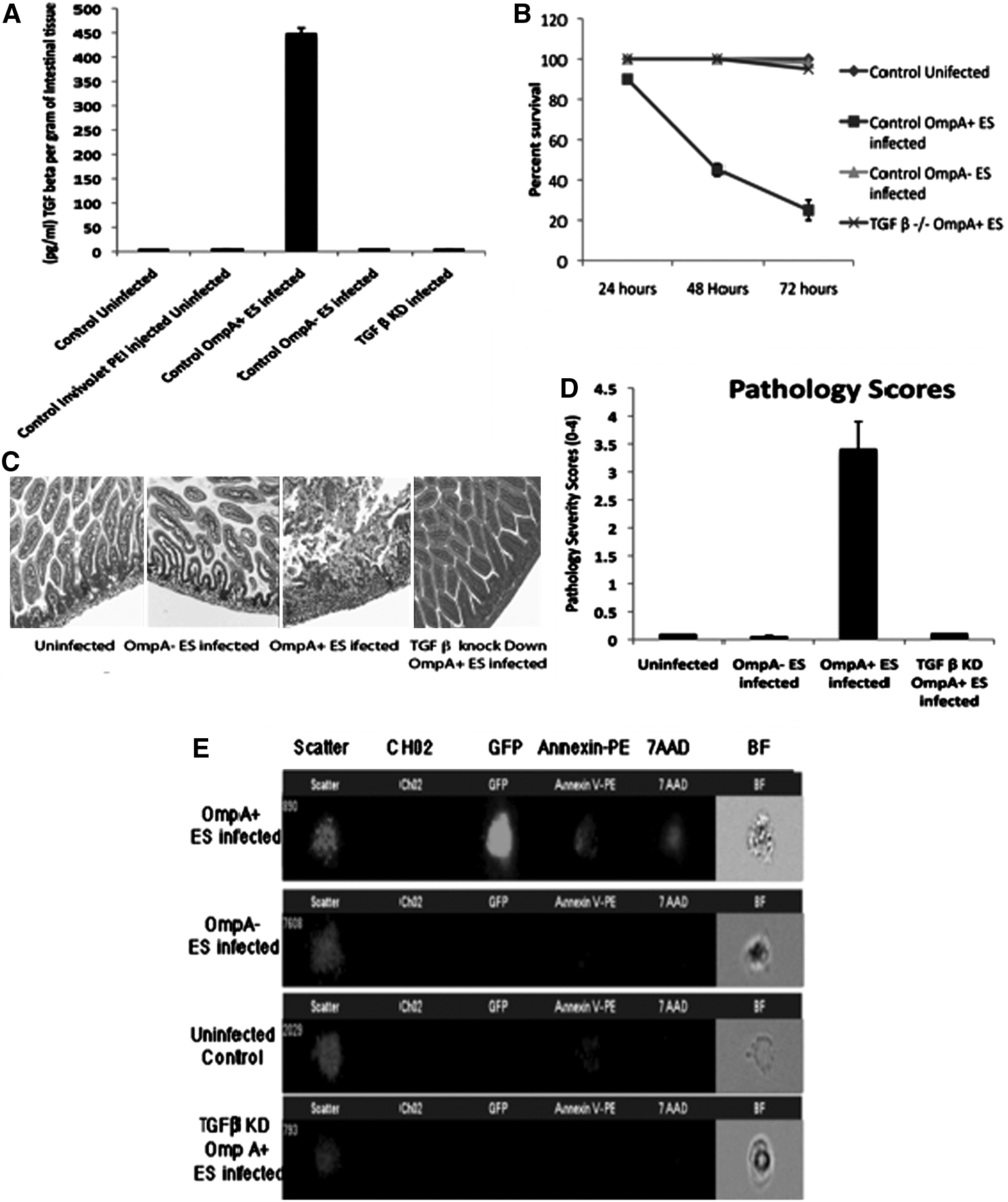
Introduction: Necrotizing enterocolitis (NEC) is the leading cause of gastrointestinal emergency in neonates. Bacterial translocation through the injured mucosal barrier plays a detrimental role in the pathogenesis of NEC. Enterobacter sakazakii (ES) is a gram-negative opportunistic pathogen that has been implicated in clinical outbreaks of NEC. We have developed an animal model of NEC based on enteral ES feeding to newborn, breast-fed mouse pups. We have discovered that ES infection increases levels of pro-inflammatory cytokines as well as TGFβ in the serum, and they remain elevated until the animal succumbs to the disease. Bacterial virulence factor outer membrane protein A (OmpA), ubiquitous to all gram-negative bacteria, is necessary for the pathogenesis of ES induced injury. Based on our preliminary findings, we hypothesize that intestinal epithelial injury caused by ES is mediated by up regulation of mucosal TGFβ.
Methods: C57Bl6 3-day old mouse pups were infected with 10^3 CFUs of OmpA + /- ES. We used a novel technology for creating knock down animals using TGFβ siRNA in vivo. Wild type animals received 4 doses of TGFβ siRNA by intra- peritoneal injections. The suppression of TGFβ expression in enterocytes was confirmed in animals using flow cytometry and PCR. Tissue cytokine level was measured from fresh homogenized intestines using ELISA. TGFβ expression in CaCo2 cells was knocked down (KD) using siRNA. Apoptosis was measured in these cells post-infection using Annexin/7 AAD staining by Image Stream analysis. Tight junction function and barrier permeability was measured in transfected CaCo2 monolayers seeded on transwells. Monolayers were infected with OmpA + /- ES for 4 hours. Trans-epithelial electrical resistance (TEER) was measured at one-hour time intervals after infection using a voltmeter. Barrier permeability was also measured using macromolecule Horse Radish peroxidase (HRP). Results were confirmed in primary mouse intestinal epithelial cells. Results: TGFβ levels are significantly increased in the intestine of the animals infected with OmpA + ES. (Figure 1A, p < 0.0001) Knock down of TGFβ expression in vivo protects against ES induced NEC. The TGFβ KD animals survive the infection and show normal intestinal histology (Figure 1B-D). Intestinal epithelial cells in KD animals show no apoptosis compared to positive controls (Figure 1E). TGFβ KD in vitro prevents OmpA + ES-induced apoptosis. Monolayer integrity and permeability remain intact despite infection with OmpA + ES in the absence of TGFβ expression.
Conclusion: ES infection results in significant up-regulation of TGFβ expression in the intestinal epithelium. OmpA expression in ES is necessary for up-regulation TGFβ. KD of TGFβ expression protects the animals from ES-induced NEC by preventing tight junction dysfunction and apoptosis. Blocking TGFβ activity may serve as a potential therapeutic target to prevent ES-induced NEC.
YazjiIbrahimMDChhinderSodhiPhDNealMatthewMDPrindleThomasBSBrancaMariaBSRussoAnthonyBSMaCongrongBSVosChristopherBSHackamDavid JMD, PhD
University of Pittsburgh
Toll Like Receptor 2 Signaling Prevents the Development of Necrotizing Enterocolitis through Negative Regulation of the Innate Immune Receptor TLR4
Introduction: Necrotizing enterocolitis (NEC) is a devastating intestinal disorder characterized by an uncontrolled and exuberant inflammatory response to bacterial colonization of the gastrointestinal tract of the premature infant. Despite a longstanding appreciation that bacterial-enterocyte signaling is required for NEC development, the mechanisms by which enteric microbes lead to NEC, and the factors that control the degree of bacterial-mediated signaling and inflammation in the newborn intestine, remain largely unknown.
Background: Our lab has recently shown that activation of the innate immune receptor Toll-like receptor 4 (TLR4) on the intestinal epithelium by gram-negative bacterial lipopolysaccharide (LPS) leads to NEC through increased enterocyte apoptosis and reduced mucosal healing. Surprisingly, recent studies have shown that gram-positive bacteria can protect against NEC development, suggesting the intriguing possibility that the receptor for gram-positive bacteria, ie Toll-like receptor 2 (TLR2), may exert anti-inflammatory properties in the gut, potentially through inhibition of TLR4. We now hypothesize that TLR2 signaling protects against NEC development through inhibitory effects on TLR4 signaling or expression.
Methods: NEC was induced in newborn wild-type, TLR2- and TLR4-deficient mice through a combination of formula gavage and hypoxia, and the extent of NEC development was assessed by evaluation of weight loss, mucosal cytokines, ileal histology and enterocyte apoptosis. To activate TLR2 and TLR4 in vivo or in vitro, mice or cultured IEC-6 enterocytes were treated with the specific ligands Pam3CSK4 or LPS respectively, and the degree of NFkB activation was assessed by immuno-confocal microscopy. To evaluate potential interactions between TLR2 and TLR4, IEC-6-enterocytes were treated with lentiviral particles containing short hairpin TLR4 RNA for 48 hours, which completely and stably restricted TLR4 expression, and the extent of TLR2 expression was determined.
Results: Compared to wild-type mice, TLR4 mutant mice had significantly reduced NEC severity, confirming the importance of TLR4 in NEC pathogenesis from our prior work. Strikingly, TLR2 deficient mice showed significantly increased NEC severity compared to wild-type mice, suggesting increased TLR4 signaling after TLR2 inhibition. In support of this possibility, injection of LPS resulted in significantly increased enterocyte apoptosis in the ilea in TLR2-deficient mice compared with wild-type counterparts, while colonization of the intestinal tract resulted in increased inflammatory signaling at baseline in TLR2-deficient mice compared to controls. In seeking to determine the pathways involved, the expression of TLR4 was significantly increased in the intestinal mucosa in TLR2-deficient mice. Strikingly, TLR4-deficient enterocytes and mice were found to have a significant increase in the expression of TLR2 and increased TLR2 signaling, confirming the reciprocal inhibitory relationship between these two innate immune receptors.
Conclusion: These data provide evidence for a novel and unexpected reciprocal relationship between TLR2 and TLR4, and demonstrate that TLR2 exerts a restraining influence on the extent of TLR4 signaling in the newborn intestine. These findings provide insight into the molecular events leading to NEC, and identify TLR2 as a possible therapeutic target in this devastating disease.
JiaSangyangJiaSong HMD, PhDCharbonneyEmmanuelMDMalamZeenatBScParodoJeanBScMarshallJohn CMD
St. Michaels Hospital, University of Toronto
Insulin Restores Apoptosis of Trauma Neutrophils (PMN) by Suppressing the Nicotinamide Phosphoribosyl Transferase (NAMPT) Activity of Pre-B Cell Colony-Enhancing Factor (PBEF)
Introduction: Hyperglycemia in association with insulin resistance is a prominent feature of acute critical illness. The role of insulin therapy remains controversial. PBEF is a highly conserved 52 kDa protein having pleiotropic activities as an inflammatory cytokine, an enzyme in a salvage pathway of NAD biosynthesis (Nampt), and a ligand for the insulin receptor (IR). We have previously shown PBEF expression to be increased in neutrophils (PMN) from septic patients, and necessary for the inflammation-induced inhibition of apoptosis. We sought to clarify the contribution of the various biologic activities of PBEF to delayed PMN apoptosis in trauma.
Methods: Circulating PMN from healthy volunteers or trauma patients (ISS > 16) were isolated by density gradient centrifugation. PMN-like HL-60 cells were used in some studies. Apoptosis was quantified as the nuclear uptake of propidium iodide in permeabilized cells. Wild-type myc-tagged PBEF or mutant PBEF in which dimerization and Nampt activity was blocked through mutation of S199 to A199 was expressed in E. coli. NAD was measured colorimetrically using thiazolyl blue and quantified in pmol/L against a standard curve.
Results: Rates of constitutive apoptosis were reduced in circulating PMN from trauma patients (23.5 ± 5.9 vs. 54.2 ± 7.5%, N = 6; p < 0.001). Transfection of HL-60 cells with wild-type, but not S199A mutant PBEF enhanced NAD generation in HL-60 cells (31.7 ± 8.5 vs 14.3 ± 3.8 pmol, p < 0.05). Rates of PMN apoptosis in healthy volunteers were 54.2 ± 7.5% at 24 hours, and were not altered by in vitro exposure to insulin (20 μU/ml). Incubation of trauma patient cells with insulin restored rates of apoptosis to control levels, an effect that could be overcome by exposure to wild-type, but not S199A mutant PBEF (Table). Co-immunoprecipitation studies showed a physical interaction between wild-type PBEF and the β chain of the IR in both PMN and HL-60 cells, however this interaction that was not seen with mutant S199A PBEF.
p < 0.05 vs no insulin; **p < 0.05 vs + insulin; †NS vs + insulin alone.
Conclusion: The Nampt activity of PBEF is necessary for its anti-apoptotic effects in PMN, and appears to be contingent on interactions between PBEF and the IR. Exogenous insulin competitively inhibits the Nampt activity of PBEF in trauma PMN. Since PMN contribute to tissue injury in trauma and sepsis, therapies targeting the PBEF:IR axis may attenuate the severity of PMN-mediated tissue injury.
IsaacsRichard JPhDDebelakKenneth APhDNorrisPatrick RPhDJenkinsJudith MMSNRooksJeffery CEckertMatthew JMDMayAddison KMDBoczkoErik MPhD
Vanderbilt University Medical Center
Non-Invasive Detection of Pulmonary Pathogens in Ventilator Circuit Filters by PCR
Introduction: Our goal is to develop techniques for rapid, non-invasive, inexpensive detection of ventilator-associated pneumonia and its pathogens. Exhaled breath is known to contain bacterial and viral particles which correlate with pulmonary infection in animal models. In mechanically-ventilated patients the in-line disposable hygroscopic condenser humidifier (HCH) filter collects exhaled aerosols, potentially containing organisms indicative of evolving pneumonia. We have refined and applied rapid, inexpensive genetic assays (real-time polymerase chain reaction, PCR) to identify and quantify bacteria in these filters (Figure). However, the extent to which HCH filter pathogens correlate with clinically relevant infections has not been evaluated.
Hypothesis: Pathogens in ventilator filters, identified and quantified using PCR, correspond to quantitative broncho-alveolar lavage (BAL) cultures.
Methods: A pilot study was conducted, following controlled laboratory experiments to establish bacteriologic properties of HCH filters and calibrate counts. Seventeen filters from 14 surgical ICU patients were obtained. Organisms were detected and quantified in these filters using PCR, and correlated with BAL performed for clinical indications.
Results: Control experiments: Bacteria quantities remain stable in HCH filters, and counts and identity of pathogens can be reliably determined via PCR. Pilot study: Quantitative PCR confirmed absence of pneumonia in all cases (see table, italics indicate quantitative results > 104) and identified predominant organism in 4/5 patients with pneumonia. Overall, observed correlations were highly significant (P < .0025, exact binomial test).
Patients w/o Pneumonia
Patients w/ Pneumonia
ID
HCH
BAL
ID
HCH
BAL
A
Acinetob.
Acinetob.
J1
E. faecalis
E. faecalis
B
C. albicans
C. albicans
J2
S. aureus
S. aureus, others
C
S. coag. negative
None
K
Enterobacter sp.
Enterobacter sp.
D
None
None
L
S. coag.
S. coag.
E
None
S. aureus
negative
neg,others
F
None
Multiple
M1
Acin. sp.
None
G
None
None
M2
None
Acin. sp.
H
None
None
N
None (dry filter)
Multiple
I1
None
S. aureus
I2
None
None
Conclusions: This pilot study illustrates: 1) Pathogenic pulmonary bacteria are present in ventilator HCH filters; 2) These bacteria can be identified and quantified using PCR much faster than with BAL cultures; and 3) PCR findings correlate with established clinical standards for pneumonia diagnosis. Ongoing improvements to our techniques, and larger clinical trials currently underway, may enable rapid, inexpensive, and non-invasive diagnosis of pneumonia.
Abi-HaidarYoumna EMDGuptaKalpanaMD, MPHStrymishJudithMDWilliamsSandraMSItaniKamal MFMD
VA Boston Healthcare System, Boston University School of Medicine
Post-Operative MRSA Conversion and Infection in MRSA-Negative Patients: Associated Factors
Background: Hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) is associated with morbid, invasive infections in hospitalized patients, and has been implicated in nearly every type of nosocomial infection. We aimed at analyzing the risk factors for patient conversion from MRSA-negative pre-operatively to MRSA-positive post-operatively.
Methods: We retrospectively reviewed all patients at the VA-Boston HCS who underwent clean or clean-contaminated surgical procedures between the years of 2008 and 2009 and also had documented pre-operative nasal PCR testing for MRSA. We abstracted post-operative MRSA microbiologic testing results, MRSA infections, surgical site infections (SSI), surgical prophylaxis data, and SSI risk index as calculated using the VA Surgical Quality Improvement Project (VASQIP) database variables. All patients who had a negative nasal MRSA PCR in the 31 day pre-operative period and did not have any positive MRSA clinical cultures in the one year pre-operative period were defined as MRSA-negative. These patients were classified as converters to MRSA-positive if they had at least one documented positive nasal MRSA PCR swab, clinical culture, nosocomial infection, or SSI within 31 days post-operatively.
Results: Among 4,238 eligible patients, 1,550 (36.6%) qualified as MRSA-negative pre-operatively. Eighty-three of these patients (5.4%) converted to MRSA-positive, and 1,467 (94.6%) remained MRSA-negative post-operatively. On multivariate logistic regression analysis, chlorhexidine-alcohol skin preparation was the only protective variable (OR 0.514; 95% CI 0.297;0.889) against conversion. Non-significant risk factors for conversion were Tier 1 surgery (or surgery with a high likelihood for inclusion in a targeted decolonization program) (OR 1.158; 95% CI 0.708;1.894), and number of days elapsed between nasal sampling for MRSA and operation (OR 1.001; 95% CI 0.958;1.045). Vancomycin surgical prophylaxis (OR 6.919; 95% CI 4.103;11.666), SSI risk index (OR 2.200; 95% CI 1.312;3.688), and age at time of surgery (OR 1.032; 95% CI 1.011;1.053) were significantly associated with conversion to MRSA-positive post-operatively.
Conclusion: In MRSA-negative pre-operative patients, vancomycin prophylaxis, SSI risk index, and age were significant risk factors for conversion to MRSA-positive post-operatively. Chlorhexidine-alcohol skin preparation had a protective effect against conversion. Further evaluation of the modifiable risk factors for hospital acquisition of MRSA in the post-operative period is warranted.
HowellGinaMDGuoLanpingMDZhangXianghongPhDCollegeRichard DBSRogengartMatthew RMD, MPH
University of Pittsburgh
Calcium/Calmodulin-Dependent Kinases (CAMK) Regulate Organ Dysfunction Durine Murine Endotoxemia
Introduction: Autophagy, an ancient cytoplasmic homeostasis process regulating cellular biomass quantity, quality, and distribution, endows cells with the ability to sacrifice and reuse portions of their cytoplasm to support vital functions during periods of stress. Recent data support a fundamental role in innate immunity as an anti-microbial effector of Toll-like receptors. The calcium/calmodulin-dependent protein kinase cascade (CaMK), a family of serine/threonine kinases responsive to intracellular Ca2+ concentration [Ca2+]i, is also integral to the immune response. In light of the calcium dependency of autophagy, we hypothesized that the CaMK regulate autophagy during sepsis.
Methods: Mice were subjected to LPS (5mg/kg, IP). CaMK activity was inhibited using the broad CaMK inhibitor KN93 (12mg/kg, IP) or its less functional analogue KN92 (12mg/kg, IP) administered 1 hour prior to experimentation. We also utilized mice genetically deficient in the expression of CaMKIV, one of two downstream effector kinases in the cascade. After LPS, blood was collected by cardiac puncture and organs were harvested. Autophagy of total cellular protein was assessed by immunoblot, using antibodies targeting LC3b. Serum cytokine concentration of IL-6, IL-10 and TNFα were analyzed by ELISA. We assessed renal function by assaying serum blood urea nitrogen (BUN) or the more GFR-specific cystatin.
Results: Endotoxemia induced marked elevations in systemic cytokine concentrations, of which IL-6 was inhibited by KN93 (2366 vs. 748, p = 0.12). Autophagy was induced in the kidney as evidenced by the induction of LC3b, which was also attenuated by KN93. The attenuation in inflammation and autophagy with KN93 correlated with reduced renal injury as evidenced by reduced BUN (95 vs. 72, p = 0.12) and cystatin (891 vs. 540, p = 0.12). To explore the specific CaMK mediating these events, we utilized CaMKIV-/- mice. Similar to KN93, CaMKIV-/- mice exhibited reduced IL-6 (3395 vs, 1664, p = 0.08) but also elevated IL-10 concentrations (245 vs. 383, p = 0.08). They demonstrated reduced autophagy in the kidney, but worse renal injury as evidenced by elevated BUN (80 vs. 96, p = 0.08) and cystatin (773 vs. 1014).
Conclusions: These results suggest that the CaMK, and specifically CaMKIV, regulate inflammation and autophagy during endotoxemia. However, though broadly inhibiting the entire family reduced renal dysfunction, specific inhibition of one downstream CaMK species, CaMKIV, worsened the degree of renal dysfunction. Further studies are needed to determine the regulatory roles of other CaMK species (i.e. CaMKK, CaMKI) in the autophagic and inflammatory response underlying the renal dysfunction of sepsis.
DiebelMarkBSLiberatiDavid MMSDiebelLawrence NMD
Wayne State University
Modulation of the Mucus Component of Intestinal Barrier Defense in Vitro
Introduction: An increased incidence of gut-related as well as other nosocomial infections such as pneumonia in ICU patients have been associated with the use of Histamine2 (H2)receptor antagonists including cimetidine. Important factors in gut barrier function include the intestinal mucus layer and secretory IgA (SIgA) related immune protection. The effect of H2 blockers on the collaboration between the intestinal mucus layer and SIgA in gut barrier function is unknown. We compared the barrier protection of mucus and mucin producing intestinal epithelial cells (IEC) as well as the effect of cimetidine and its effect on mucus production in an in vitro model.
Methods: HT-29 MTX (a mucus producing IEC) monolayers were established in a two-chamber cell culture system. Dimeric IgA was added to the basal media of IEC monolayers to allow binding of IgA to the polyimmunoglobulin receptor on the basal side of IEC followed by uptake and delivery of SIgA to the IEC apical surface (transcytosis). Cimetidine was added to the media of a subset of the HT-29 MTX intestinal cells and E. coli (EC) to the apical media of HT-29 MTX cell monolayers. Either fluorescein-labelled E. coli (FITC-EC) or unlabelled EC were added to subsets to quantify bacterial adherence (60 minute co-culture) and bacterial passage (240 minutes) thru IEC monolayer's respectively. Mucus content was indexed by O-linked oligosaccharide chain (OSC) content and Western blot analysis.
p < 0.001 vs. HT-29 MTX, #p < 0.001 vs. other groups. Decreased mucus content of HT-29 MTX treatment with cimetidine was confirmed by Western blot analysis.
Conclusion: Bacterial trapping in the intestinal mucus layer enhances SIgA interaction with luminal bacteria and contributes to intestinal barrier integrity. Loss of the intestinal mucus layer associated with cimetidine administration impairs barrier function in this model. Use of cimetidine may contribute to systemic inflammation and remote organ dysfunction in at risk patients especially with subsequent insults to gut homeostasis.
NelsonRyan KBAPoroykoValeriyPhDAlverdyJohn CMDMorowitzMichael JMD
University of Chicago
The Effect of Dietary Monosaccharides on Pseudomonas Aeruginosa Virulence
Introduction: Pseudomonas aeruginosa is an opportunistic, gram-negative pathogen associated with many hospital-acquired infections and disease states. In particular, P. aeruginosa has been identified as a critical factor in the pathogenesis of neonatal necrotizing enterocolitis (NEC). NEC presents more frequently in infants fed a formula-based diet – a finding that may be based on the monosaccharide content of this diet class. Thus, we hypothesized that P. aeruginosa would differentially express virulence genes when exposed to monosaccharides present in formula versus those present in human milk.
Methods: Using the results of a metabolomics study on infant diets and their resulting fecal samples, we identified several monosaccharides that distinguished milk from formula diets. Of these diet-distinguishing monosaccharides, four were found to be metabolized by P. aeruginosa. We subsequently grew P. aeruginosa in tryptic soy broth (TSB) supplemented with these four monosaccharides and used qRT-PCR to measure the expression of 59 major P. aeruginosa virulence genes. Results were standardized to an external control of P. aeruginosa grown in TSB alone.
Results: P. aeruginosa did not differentially respond to monosaccharides after six hours of growth. After 24 hours, however, P. aeruginosa grown in arabinose (present in formula), xylose (present in human milk), and galactose (present in feces from milk-fed infants) displayed a significant increase in virulence gene expression in all categories of genes tested. In contrast, P. aeruginosa grown in mannose (also present in the feces from milk-fed infants) displayed a significant decrease in virulence gene expression when compared to the other experimental conditions.
Figure: Numerical values represent the log of the fold-difference in gene expression between the experimental group and the external control. The table was conditionally formatted so the intensity of red correlates with the magnitude of gene up-regulation and the intensity of green correlates with the magnitude of gene down-regulation.
Conclusion: These preliminary studies demonstrate the importance of nutrient content on the relative expression of virulence genes in pathogens that commonly colonize the gut of infants. Understanding the effect of current dietary formulas on virulence gene expression across such gut-colonizing pathogens may present a new approach to elucidate the differences between human milk and formula in the development of NEC.
HobsonCharles EMDBrennanMeghanMStatBozorgmehriShahabMDEfronPhilip AMDBihoracAzraMD
University of Florida
Small Postoperative Changes in Serum Creatinine are Associated with Postoperative Sepsis and Surgical Infections
Background: Postoperative mild and moderate AKI, characterized by small changes in serum creatinine (sCr), is common and is associated with increased short and long-term mortality. Small changes in sCr may be predictive of postoperative sepsis and surgical infections.
Methods: A retrospective, single center study of 40533 adult surgical patients admitted to a tertiary academic center from 2000–2008 for ≥2 days. Maximum change in sCr from baseline sCr (BsCr) was calculated for each patient. AKI was defined using modified RIFLE classification as postoperative change in sCr ≥ 0.3 mg/dl. Area under the curve (AUC) was used to determine the predictive ability of a maximum change in sCr for postoperative sepsis and surgical infections. The level of change from BsCr that best predicts outcome was determined by maximizing sensitivity and specificity along the ROC curve.
Results: The prevalence of postoperative sepsis and surgical infections was 5% and 5.5%, respectively. Patients with AKI were more likely to develop both sepsis (OR 20, 95% CI 15-25) and SI (OR 2.2, 95% CI 2.1-2.5) compared to patients without AKI. Multivariate logistic analysis revealed that age, maximum change in sCr, number of comorbidities, baseline GFR, Medicaid insurance status, weekend admission and type of surgical service were independently associated with the occurrence of sepsis (c statistic 0.622). Maximum change in sCr from baseline in the first seven postoperative days was predictive of sepsis (AUC range 0.84). ROC analysis indicated that a change of 0.3 mg/dl or greater from BsCr is predictive of sepsis (sensitivity range 0.8–0.9, specificity range 0.76–0.85).
Conclusion: Postoperative sCr change as low as 0.3 mg/dl is predictive of postoperative sepsis.
Change in sCr in the first seven days and sepsis.
SheldonHolly KMDNgJoannaMDBauzaGustavoMDMellaJuanMDGainsburyMelanie LMDAgarwalSureshMDBurkePeterMD
Boston University Medical Center
Hypoglycemia Increases the Risk of Hospital Acquired Infections in an Surgical Intensive Care Unit
Background: Strict glucose control with intensive insulin therapy has been reported to reduce mortality and morbidity in critically ill adults. The results of these trials lead to widespread support and implementation of intensive insulin therapy protocols. However, considerable controversy has developed over the benefit of tight glucose control and the subsequent risk of hypoglycemia.
Methods: Retrospective review of prospectively collected data on all patients admitted to a Surgical Intensive Care Unit at a large, urban, level 1 trauma center from January 2005 until August 2009. Inclusive criteria consisted of an ICU admission, with hospital length of stay of at least 48-hours, and a minimum of 8-Point of Care (POC) glucose readings. Data were collected via the Clinical Database Warehouse and Trauma Registry (TRACS). Each subjects glucose values were averaged over the length of stay. Each glucose value was designated as either hypoglycemic (<80 mg/dL), or not hypoglycemic (>80 mg/dL), and percent hypoglycemia was calculated as number of hypoglycemic events / total glucose readings. Hospital-acquired infections (HAI), including urinary tract infection, blood stream infections, and ventilator-associated pneumonia were assigned by an independent Infection Control Committee.
Results: Of the 1,561 patients included, 1,039 (66.6%) were admitted with a trauma diagnosis, and 873 (56%) had at least one hypoglycemic event. These hypoglycemic patients were 5-times more likely to develop a HAI when compared to patients with no hypoglycemic events (18.0% v. 3.4%, p < 0.01). Additionally, they were older (53.7 years v. 49.9 years, p < 0.01), more injured (19.5 average ISS v 16.7 average ISS, p < 0.01), and with a higher co-morbidity of diabetes (12.5% v 7.1%, p < 0.01). Multivariate analysis demonstrated that hypoglycemia was and independent risk factor for the development of HAI (see table). HAIs were associated with a significant increase in ICU LOS (21.4 days v. 6.3 days, p < 0.01) and hospital LOS (31.1 days v 14.1 days, p < 0.01).
Regression analysis of characteristics associated with the development of HAIs
Results are expressed such that OR > 1.0 predicts the outcome of interest.
Conclusion: We demonstrate that in the critically ill surgical patient, any degree of hypoglycemia is an independent risk factor for the development of hospital acquired infections. Furthermore, HAI leads to a significant increase in both hospital and ICU length of stay.
HranjecTjasaMD, MSSwensonBrian R.MDRosenbergerLaura HMDPolitanoAmani DMDRiccioLin MMDMetzgerRosemarieMD, MPHPopovskyKimberly ARNMayAddison KMDSawyerRobert GMD
University of Virginia
A Conservative Approach to the Initiation of Antimicrobials in Critically Ill Patients with Suspected Infection is Associated with Improved Survival
Introduction: Appropriate, early antibiotic therapy is associated with improved outcomes, but the optimum timing for initiation of antibiotics is unknown. Two strategies exist: commencement of antimicrobials as soon as infection is suspected or initiation of treatment only after objective data (i.e., culture, x-ray, etc) confirms infection. We hypothesized that a more aggressive approach would improve patient mortality without affecting ICU-wide infection rates or ICU flora.
Methods: This two-year study included all patients admitted from 9/08 to 8/10 to the surgical ICU at a single tertiary care hospital. During year one, aggressive treatment was employed, where patients suspected of having an infection based on clinical grounds (fever, change in white blood cell count, or other clinical change consistent with new infection) had blood cultures sent and antibiotics started (Aggressive period). During the second year, a conservative strategy was used, with antimicrobials started only after objective findings confirmed infection, i.e., positive gram stain/culture, radiologic study, etc (Conservative period). Univariate (chi square and t-test) and multivariate analysis (logistic regression) were used.
Results: Admissions for the first and second year were 762 and 721, respectively. 247 ICU-acquired infections occurred during the aggressive year and 237 during the conservative year (Table). For ICU-acquired infections, the initiation of antibiotics was significantly delayed in the conservative year (34.8 ± 2.4 vs 20.9 ± 1.8 hours from culture to initiation of antibiotics, p < 0.0001, and 28.1 ± 2.4 vs 9.9 ± 1.1 hours from fever to initiation of antibiotics, p < 0.001); however, duration of antibiotics was shorter (12.5 ± 0.7 vs 17.7 ± 1.8 days, p = 0.008). Resistant Gram positive cocci (MRSA and VRE) were isolated more frequently in the aggressive period than the conservative period (42 versus 24 infections, respectively). Rates of initial adequate empiric antimicrobial use were similar (67.4% and 70.4% for aggressive and conservative, respectively). All cause mortality on a per infection basis was lower during the conservative period for all infections, pneumonia, and abdominal infections. 27/101 (26.7%) patients with ICU-acquired infections died during the aggressive period while 13/100 (13.0%) died during the conservative period (p = 0.015 for the difference). After adjusting for age, gender, location of acquired infection (home, ICU or ward), involvement in trauma, APACHE II score and site of infection, conservative treatment resulted in a 76% reduction in mortality risk (OR = 0.244, 95%CI (0.089 – 0.667)).
AggressiveN/mortality
ConservativeN/mortality
p
All infections
247/40.1%
237/20.1%
<0.0001
APACHEII
19.8 ± 0.4
20.9 ± 0.5
0.068
Pneumonia
75/30.7%
93/16.1%
0.025
BSI
49/38.8%
46/32.6%
0.53
Abdominal infection
31/41.9%
22/27.3%
0.27
Conclusion: Waiting for objective data to diagnose infection prior to the initiation of antimicrobials does not worsen mortality. In fact, a conservative approach to antimicrobial initiation may lead to better outcomes and minimize antimicrobial use in uninfected patients.
HillDavid MPharmDSchroeppelThomas JMDMagnottiLouis JMDClementLesley PPharmDFischerPeter EMD, MSFabianTimothy CMDCroceMartin AMD
Regional Medical Center at Memphis, University of Tennessee
Methicillin-Resistant Staphlococcus Aureus as a Causative Pathogen in Early Ventilator-Associated Pneumonia: Cause for Concern?
Introduction: Staphylococcus aureus (SA) remains a common cause of ventilator-associated pneumonia (VAP) in trauma patients. The prevalence of community acquired methicillin-resistant Staphylococcus aureus (MRSA) has increased over the last decade. The purpose of this study was to evaluate the incidence and trend of MRSA VAP over a 6-year period and to examine the adequacy of our current empiric antibiotic regimen.
Methods: All patients with VAP (≥105 CFU/mL in BAL effluent) over a 6-year period were identified from the VAP database maintained in our Level I trauma center. All patients received empiric therapy based on duration of ICU stay (ampicillin/sulbactam (<7 days) or cefepime plus vancomycin (>7 days) or equivalent in penicillin allergic patients). Patients were stratified by gender, age, severity of shock (24-hour transfusions) and injury severity (GCS and ISS). Outcomes (ventilator days, ICU days, hospital length of stay (LOS) and mortality) were compared between patients with early MRSA VAP and those with all other causes of early VAP. Linear regression was used to determine differences in incidence over the six year time period. Multi-variable logistic regression was then performed to determine whether early MRSA was an independent predictor of mortality in patients with early VAP.
Results: 727 patients with 997 VAP episodes (1.4 episodes per patient) were identified. 512 episodes were early VAP of which 63 were MRSA. The incidence of SA in early VAP, MRSA by all early SA VAP, and MRSA by early VAP are shown in the table. Linear regression shows that the incidence of early SA VAP (slope = − 0.911, p = 0.490) is stable, but the incidence of MRSA in all early SA VAP (slope = 3.95, p = 0.0154) and the incidence of MRSA in early VAP are increasing (slope = 1.35, p = 0.0028). There was no statistical difference in gender, age, 24-hour transfusion requirements, ISS, or GCS in those patients that got early MRSA compared to other organisms. There was no difference in mortality (17.5 vs.18.7%, p = 0.81), ventilator days (18.5 vs. 18.1, p = 0.89), ICU days (23.8 vs. 23.1, p = 0.80), or LOS (34.9 vs. 33.7, p = 0.76) comparing MRSA with other early VAP episodes. Multivariable logistic regression performed on all pts with early pneumonia failed to show early MRSA as an independent predictor of mortality (OR = 0.815, p = 0.59) after adjusting for age, ISS, and 24-hour transfusion requirements.
Year
Incidence of SA in early VAP (%)
Incidence of MRSA in early SA VAP (%)
Incidence of MRSA in early VAP (%)
2004
33.6
23.7
10.4
2005
30.6
22.9
9.5
2006
22.9
31.6
11.5
2007
31.9
31.8
12.9
2008
22.3
44.0
14.7
2009
30.4
38.7
16.4
Conclusions: The incidence of early MRSA as a causative pathogen of VAP and in all SA early pneumonias has increased significantly in trauma patients. While MRSA is being seen more frequently within seven days of admission, outcomes and resource utilization from episodes of inappropriate empiric antibiotic treatment are unchanged from other early pneumonias. The current empiric antibiotic algorithms for VAP are adequate and no changes are warranted.
ByrnesMatthew CMDIrwinEricReicksPattyBeilmanGregory JMD
University of Minnesota
A Prospective, Protocolized Study Evaluating the Reliability of Sputum Cultures Obtained after Administration of Antibiotics in Injured Patients
Introduction: Appropriate utilization of antibiotics in critically ill patients involves tailoring antibiotics to culture results; however, the culture results must be reliable. It is generally believed that administration of antibiotics before obtaining cultures can have a significant effect on culture results; however, this has never been prospectively evaluated in injured patients. We hypothesized that the antimicrobials would significantly reduce the reliability of cultures obtained between 1 and 24 hours after antibiotic administration.
Methods: Patients admitted to a Level I trauma center were prospectively evaluated. Patients were eligible for the study if they were mechanically ventilated and were suspected to have pneumonia. Informed consent and IRB approval were obtained. After enrollment, sputum cultures were obtained and broad spectrum antibiotics were started. Sputum cultures were then repeated at 1 hour, 6 hours, 12 hours, and 24 hours after completion of the first dose of antibiotics. Cultures were incubated in standard broth and were allowed to grow until a final report was generated by the microbiology laboratory (48-72 hours). Patients whose initial culture was positive were included in the analysis. The culture results before antibiotics were administered were compared with the culture results at each subsequent time point. Additionally, patient demographics and hospital course were noted. Categorical data were analyzed with chi square tests and continuous variables were analyzed with t-tests.
Results: There were 21 patients included in the study. The average patient age was 49.4 years. The average injury severity score was 27.7. The average ICU and hospital lengths of stay were 20.2 days and 24.7 days, respectively. All of the organisms that were grown from the pre-antibiotic cultures were also grown in the cultures obtained 1 hour after antibiotics were given. A significant number of these organisms were unable to be grown in subsequent cultures. The rate of negative cultures increased to 21%, 32%, and 42% among the 6 hour, 12 hour, and 24 hour groups (p < 0.01 for each group). Gram positive organisms accounted for 42.9% of infections, with S. aureus being the most common organism. There was a significantly reduced effect of antibiotics on subsequent S. aureus cultures. All cultures positive for S. aureus prior to antibiotic administration remained positive at each subsequent time point, despite the adequacy of initial antibiotic selection.
Conclusion: Antibiotics have a significant effect on culture results. This effect is most pronounced in gram negative organisms and is seen in cultures obtained more than 1 hour after antibiotics are given. As a result, cultures obtained more than one hour after antibiotics are administered cannot be used to tailor antibiotics in injured patients with suspected infections.
De CastroGerard P.MDBochicchioGrant V.MD, MPHDriscollIan R.MDSteinDeborah M.MD, MPHBochicchioKelly M.RN, MSZhuShijunPhDJoshiManjariMBBSHessJohn R.MD, MPHScaleaThomas M.MD
R Adams Cowley Shock Trauma Center - University of Maryland Medical Center
Fresh Frozen Plasma Transfusion is an Independent Risk Factor for Bacteremia in Critically Ill Traumatic Brain Injury Patients
Introduction: Traumatic brain injury patients are at high risk for FFP transfusion and infection due to complex injury and prolonged ICU length of stay. To our knowledge, few studies however, have evaluated the impact of FFP transfusion on infection in traumatic brain injury (TBI) patients. The objective of this study was to evaluate the impact of FFP transfusion as an independent predictor of infection in critically injured TBI patients.
Methods: Prospective data were collected on 630 consecutive critically injured trauma patients diagnosed with traumatic brain injury (confirmed by CT scan) over a 4 year period. Data collected included demographic information including age, gender, race, mechanism of injury, Injury Severity Score (ISS) and head Abbreviated Injury Score (hAIS). The admission coagulation profile of each patient in the study was recorded in addition to the total number of units of FFP and packed red blood cells (pRBC) transfused in the 1st 24 hours of hospital admission. Clinical outcomes including mortality, ICU days, nosocomial infection, and hospital length of stay were also evaluated.
Results: Seventy-four percent of patients were male (N = 469) and the majority were Caucasian (N = 399). Mean age, ISS, and HAIS were 43 ± 21 years, 31 ± 12, and 4 ± 1, respectively. Of the 632 TBI patients, 252 (40%) patients received FFP transfusions in the 1st 24 hours of admission. Mean number of units of FFP transfused in the 1st 24 hours of admission were 2 ± 5 units (Range 0 - 64 units).The mean number of ICU days and hospital days were 13 ± 10 days and 16 ± 12 days. The overall mortality was 18.5% with an infection rate of 63%. The 3 most common infections were urinary tract infections (25%), pneumonia (22%), and bacteremia (19%). Patients who received FFP had a significant greater incidence of bacteremia (24%) compared to those who did not receive FFP (15%) in the 1st 24 hours (p = 0.005). Logistic regression analysis, controlling for age, gender, race, mechanism of injury ISS, HAIS, and baseline coagulation profile, show that FFP transfusion in the 1st 24 hours of admission was found to be a independent predictor of bacteremia (OR 1.88, p-value = 0.010). There was no significant difference in pneumonia and UTI rates between the two groups.
Conclusion: Fresh frozen plasma transfusion is an independent risk factor for bacteremia in patients with traumatic brain injury. Further research regarding the potential etiology of this finding in TBI patients is warranted.
CharbonneyEmmanuelMDLiYangmeiKleinDavidMD, MBARomaschinAlexanderPhDNathensAvery B.MD, PhDMarshallJohn C.MD
University of Toronto
Systemic Endotoxemia following Multiple Trauma is Associated with Early Shock and Predicts Subsequent Mortality
Background: Multiple trauma is associated with innate immune activation and inflammatory morbidity, even in the absence of superimposed infection. The potential etiologic role of bacteria or bacterial endotoxin (LPS) translocating from the gut has been controversial. We undertook a serial evaluation of circulating LPS levels in a cohort of trauma victims.
Methods: We performed a prospective observational cohort study of patients sustaining severe multiple trauma (ISS > 16). We measured LPS levels on days 0, 1, 3, and 5 using the Endotoxin Activity (EA) Assay® - a whole blood assay based on LPS-primed neutrophil chemiluminescence that quantifies endotoxin on a scale from 0 to 1.0 activity (EA) units. EA levels were stratified as low (<0.40 EA units), intermediate (≥0.40-0.59 EA units), or high (≥0.60 EA units). We collected data on demographics, resuscitation, length of stay (LOS), and mortality. Statistical analyses used ANOVA, Fisher's exact or Student t tests, as appropriate, with an α level of p < 0.05.
Results: We recruited 22 patients having a mean age of 43 ± 23 years and mean ISS of 40 ± 15. Most (82%) were male, and 17/22 had sustained blunt trauma. We analyzed only those patients having a minimum of three EAA values (N = 20). Their median ICU LOS was 9 days (2–29) and their duration of mechanical ventilation, 9 days (1–27). Four patients died (20%) at 10 ± 1 days post admission. The mean initial (Day 0) EA value was low, but increased significantly over time (Table; ANOVA for trend p = 0.0013). Maximal EA values were reached at an average of 80 ± 40 hours; four (20%) patients recorded high EA levels, while in 12 (60%) the maximal levels were intermediate. EA levels exceeded 0.4 on at least 2 occasions in all 4 non-survivors, but in only 3/16 survivors (p = 0.007). Both maximal EA levels (0.65 ± 0.15 vs 0.45 ± 0.11; P = 0.009), and average EA across Day 0 to Day 5 (0.48 ± 0.06 vs 0.32 ± 0.10; P = 0.008) were higher in non-survivors than in survivors. The average EA level correlated significantly with the presence of shock at admission (r2 = 0.2; P = 0.04).
Conclusion: Endotoxemia is not present immediately following trauma, but develops over time during the early post-injury period. Its presence predicts adverse outcome. The association of endotoxemia with systemic hypoperfusion suggests that the GI tract is the source of circulating endotoxin in the victim of multiple trauma.
VogelTodd RMD, MPHDombrovskiyViktor YMD, MPH, PhDGrahamAlan MDLowryStephen FMD
Robert Wood Johnson Medical School, Department of Surgery, The Surgical Outcomes Research Group, UMDNJ-RWJS, New Brunswick, New Jersey
The Impact of Infectious Complications after Elective Surgery on Hospital Readmission and Late Mortality in the us Medicare Population
Introduction: While the negative impact of infectious complications (IC) after elective surgery during the index hospitalization is well established, the long-term ramifications of hospital acquired post-operative infections are not well studied. This analysis evaluated the impact of a hospital acquired IC after open abdominal vascular surgery on readmission rates as well as 30-day and 90-day mortality after discharge.
Methods: Data from all hospitals in the US that performed elective open abdominal vascular surgeries in Medicare population from 2005 to 2007 were extracted from the national MedPAR database. The cohort included all open abdominal vascular surgeries including aortic, iliac, and visceral procedures. Infectious complications evaluated included: pneumonia (PNA), urinary tract infection (UTI), postoperative sepsis (sepsis), surgical site infection (SSI), and Clostridium difficile (CDiff). For comparison, patients were categorized from their index procedure as either developing an IC during their initial hospitalization (Index + INF) or not developing an IC (No INF). Longitudinal evaluation of rates of 30-day readmission, 30-day infectious complications, and 30-day and 90-day mortality after the initial discharge was performed and these rates were compared between groups.
Results: 29,549 open abdominal vascular procedures were identified. 4,016 (13.6%) patients developed an IC during their index hospitalization: PNA (5.1%), UTI (2.7%), sepsis (1.6%), SSI (1.4%), and CDiff (0.6%). Additionally, 1.13% of patients developed PNA, UTI, SSI or CDiff complicated by sepsis. Hospital mortality during the initial hospitalization was 13.7% (Index + INF) vs. 4.0 (No INF), p < 0.0002. Infectious processes (PNA, UTI, SSI, and CDiff) which were complicated with the development of sepsis significantly increased in-hospital mortality compared to an IC alone (39.1% vs. 5.5%, p < 0.0001). Mortality 30-days and 90-days after the initial discharge from the index procedure was significantly higher for Index + INF compared to No INF (4.4% vs. 1.2% and 8.6% vs. 2.6%, respectively, p < 0.0002). The greatest 30-day mortality rates after discharge were found after CDiff + sepsis (30%), PNA + sepsis (12.6%), and postoperative sepsis alone (8.6%). The same rank was found for 90-day mortality: 30%, 22.5%, and 13.8%. Overall, readmission was higher for Index + INF compared to No INF (33.7% vs. 21.5%, p < 0.0002). Rates of 30-day readmission after index IC ranged between 32.0% and 50.0%.
Conclusion: For Medicare beneficiaries undergoing elective open abdominal vascular procedures, the development of any infectious complication significantly increased not only hospital mortality, but also the 30-day and 90-day mortality after discharge from the hospital. Index infectious complications were also associated with increased 30-day readmission after discharge. Hospital acquired infections have a profound late effect on outcomes after discharge, and future programs targeting high risk patients may improve long term survival and minimize readmissions.
CarlisleErica M.MDPoroykoValeriyPhDCaplanMichael S.MDAlverdyJohnMDMorowitzMichael JMDDonaldLiuMD, PhD
University of Chicago Medical Center
Gut Microflora is Significantly Altered After 72 Hours of Formula Feeding
Introduction: Infants exposed to formula feeding are at increased risk for intestinal diseases with a bacterial etiology (e.g. necrotizing enterocolitis). However, the impact of diet on infant gut bacterial colonization has not been fully elucidated. Formula feeding may alter the normal gut flora in such a way that confers this heightened vulnerability to disease. Here, we utilize 16S bacterial DNA pyrosequencing, a culture independent technique, to quantitatively analyze the colonic microbiota of mice fed formula as compared to mice fed maternal milk to test the hypothesis that diet impacts the relative abundance of bacterial species in the gut.
Methods: C3HeB/FeJ pups were born vaginally and remained housed with the mother until DOL7. On DOL7 half of each litter was assigned to formula feeding (liquid puppy formula via orogastric catheter 4x/day) while the remaining pups were allowed exposure to maternal feeding. All pups were euthanized at 72 h, and colonic tissue was collected for DNA extraction. After colonic microbial DNA was extracted, sequences encoding the 16 S ribosomal subunit were amplified and sequenced on the Roche GS-FLX pyrosequencing platform. Taxonomy was assigned to sequences using the Ribosomal Database Project classifier tool. Statistical tests for differentially abundant 16S-based taxonomic annotations between populations were performed using Metastats methodology to compute nonparametric p-values.
Results: After only 72 h of differential feeding, 16S pyrosequencing demonstrated that Firmicutes (p < 0.001) was the dominant phylum in the maternal fed pups while Proteobacteria (p < 0.001) was the dominant phylum in formula fed animals. At the genus level, colonic microflora of formula fed animals had significantly more Streptococcus (p < 0.001) than that of maternal fed animals. However, the colonic microflora of maternal fed animals had a greater abundance of Lactobacillus (p < 0.001) and Enterococcus (p < 0.001) than that of formula fed animals.
Conclusion: Overall, 72 h of differential feeding resulted in marked alterations in the relative abundance of bacterial species in the gut. Firmicutes was the dominant phylum in maternal fed animals, while Proteobacteria was the dominant phylum in formula fed animals. Interestingly, while Lactobacillus and Enterococcus were more abundant in animals fed maternal milk, the gut microflora of formula fed animals was dominated by Streptococcus. Presumably such alterations in gut bacterial community structure could be responsible for differential disease development in infants fed formula as compared to breast milk. The finding that these changes were observed after only 72 h of differential feeding demonstrates the plasticity of the gut in that gut microflora can undergo relatively rapid repopulation based upon environmental conditions. Future work will evaluate changes in host and microbial gene expression in response to differential feeding.
KanaanZiadMD, PhDGardnerSarahBSPeytonJimMSCheadleWilliam GMD
University of Louisville
Parallel Microrna-155 and TNF-α Production could Explain Microbial Tolerance in a Novel Peritonitis Model
Introduction: We observed persistent peritoneal bacteria despite a transient early innate immune response to intra-peritoneal (IP) Klebsiella pneumoniae. Pretreatment with lipopolysaccharide (LPS) prior to peritonitis induced a tolerant pattern of pro-inflammatory cytokine protein production but not at the messenger RNA (mRNA) level. MicroRNAs (miRNA)s regulate inflammatory cytokines and may explain this paradox.
Methods: 24 hours after pretreatment with IP LPS (0.01 mg/g) or saline, C57BL/6 mice were given 103 colony forming units of K. pneumoniae IP. Gentamicin was given 4 hours prior to infection and BID thereafter. Peritoneal exudate cells (PEC)s were obtained through peritoneal lavage and total RNA was isolated (n = 3) at 4, 24, and 48 hours following infection. TNF-α levels were detected using ELISA. MicroRNA (miRNA) expression levels were detected using SA Biosciences mouse immuno-pathology RT2 miRNA PCR array (MAM-104A). mRNA detection was done using SA Biosciences RT2 Profiler PCR array mouse Toll-like receptor signaling pathway (PAMM_018A). Data were analyzed by Ingenuity Pathway Inc. analysis (IPA). Student's t-tests were used to determine significance of fold changes.
Results: TNF-α production increased at 4hours and was significantly decreased at 24 and 48 hours in the LPS as compared to the PBS pre-treated group (p < 0.05). In concordance, miR-155 expression at 48 hours was greater in the PBS and LPS pre-treated groups (p < 0.05). There was no significant difference in TNF-α mRNA expression between groups at 4, 24, and 48 hours suggesting no tolerance at the mRNA level (p > 0.05) IPA analysis of the mRNA data showed that 6 main canonical pathways were constantly dysregulated, and in the same significance order, in both the saline and LPS group at 4, 24, and 48 hours. These are: Toll-like receptor and NF-KB signaling, hepatic cholestasis, interleukin-6 and LPS mediated MAPK signaling pathways, and pattern recognition receptors of bacteria pathway.
Group
Marker
At 4hrs
At 24 hrs
At 48 hrs
PBS Pre-treated
TNF-α (pg/ml)
32 ± 10
18 ± 5
67 ± 30
miR-155
6x
10x
27x
TNF-α mRNA
70x
4x
8x
LPS Pre-treated
TNF-α (pg/ml)
22 ± 5
7 ± 1
9 ± 5
miR-155
21x
10x
9x
TNF-α mRNA
87x
11x
3x
Conclusion: Peritonitis increased PEC gene expression associated with sepsis and a pro-inflammatory response, which was further augmented by LPS pretreatment over 24 hours only. Prior exposure to LPS did not induce PEC gene tolerance to subsequent infection with Klebsiella at the mRNA level. Up-regulated pathways were common to the early innate response, and macrophage reprogramming occurs at the genetic level. Lack of bacterial clearance in this model is due to an inadequate innate response which resolves despite incomplete clearance of intra-peritoneal bacteria. miR-155 production parallels TNF-α and not TNF mRNA production and suggests a mechanism for tolerance in this model and persistent peritoneal infection.
WangJinMSGrishinAnatoly V.PhDFordHenri R.MD, MHA
University of Southern California - Childrens Hospital Los Angeles
Roles of C-Terminal Non-Catalytic Domain and ERK Phosphorylation in Rapid Proteolysis of the MKP-1 Phosphatase
Introduction: Intestinal inflammatory disorders such as IBD or necrotizing enterocolitis may result from the failure to down regulate innate immune responses in the gut. Mitogen-Activated Kinase Phosphatase, MKP-1, is a critical regulator of epithelial innate immunity. To gain insight into MKP-1-dependent regulation, we sought to elucidate the mechanisms of negative regulation of MKP-1 by proteolysis.
Methods: ERK phosphorylation sites of MKP-1 were obliterated using site-directed mutagenesis. Wild type and mutant MKP-1 were ectopically expressed in human embryonic kidney HEK293 or rat intestinal epithelial IEC-6 cells. Half-life of MKP-1 proteins was determined using cycloheximide chase assay. ERK activity was blocked using the specific inhibitor, U0126.
Results: Half-life of wild type MKP-1 protein was about 30 min. Complete deletion of the C-terminal non-catalytic domain extended the half-life to over 4 h. Obliteration of ERK phosphorylation sites within the C-terminal non-catalytic domain, or pharmacologic inhibition of ERK extended the half-life of MKP-1 to only about 1 h.
Conclusion: The C-terminal non-catalytic domain of MKP-1 serves as a rapid degradation signal. ERK-dependent phosphorylation within this domain plays only a minor role in targeting MKP-1 for proteolytic degradation. Rapid degradation of MKP-1 is important for the dynamic regulation of the innate immune responses by this phosphatase.
GuoLanpingMDZhangXianghongPhDCollageRichard DBSStripayJennifer LBSRobertStephen MMDTsungAllanMDLeeJanet SMDRosengartMatthew RMD, MPH
University of Pittsburgh
Calcium/Calmodulin-Dependent Protein Kinaseiα Mediates LPS-Induced Autophagy in Macrophages VIA Camkiα, AMPK and APG7 Complex
Introduction: Autophagy, originally described as a stress response to nutrient deprivation, now is emerging as the chief rout for bulk degradation of aberrant organelle, protein aggregates, and invading foreign materials to keep cells homeostasis. It has been shown to be an important effecter arm of innate immunity. CaMKI is an ubiquitously expressed cytoplasmic enzyme that mediates calcium signaling in macrophages (Mϕ) responding to LPS. In light of the calcium dependency of autophagy, we hypothesized that CaMKI positively regulates autophagy in Mϕ responding to LPS.
Methods: In vitro: RAW 264.7 cells and murine peritoneal Mϕ were treated with LPS (100 ng/ml). We utilized the following inhibitors: KN62, Compound-C (AMPK inhibitor), AICAR (AMPK activator), and Rapamycin (mTOR inhibitor). We utilized a constitutively active CaMKI plasmid (CaMKI.293), its kinase-inactive mutant (CaMKI.293K49A), and siRNA CaMKIα to manipulate CaMKIα expression. Autophagy was assessed by immunoblot, immunfluorescent and electron microscopy. CaMKIα activity was measured by immunoblot. Cytokines IL-1ɑ, IL-6, IL-10 and TNF-α in medium released from RAW 264.7 were analyzed with ELISA after the RAW 264.7 was treated with LPS for 16 hours and siRNA APG5, APG7 and LC3B transfection. In vivo: Mice were subjected to cecal ligation and puncture or sham operations after 72 hours with RNAi of CaMKIα, LC3B in tissues were analyzed with immunoblot.
Results: LPS induced autophagy as evidenced by increased APG7, LC3B and APG5-12 conjugation, that was inhibited with CaMKIα siRNA, KN62, and Compound-C. LPS also induced p-AMPKα, p-mTOR, p-p70S6K, and p-S6, all of which were inhibited withsiRNA CaMKIα. Over expression of CaMKI transfection with CaMKI.293 induced APG7, LC3B, APG5-12, p-AMPKT, p-mTOR, p-p70S6K, and p-S6 to a greater extent than it's less active CaMKI-293K49A. The AMPK inhibitor, compound C, inhibited autophagy consequent to either LPS or CaMKI-293. There are complex between CaMKI, AMPKa and APG7. CaMK1 and AMPK complex were not influenced by APG7 siRNA, but there is no immunoprecipitation complex between APG7 and AMPKa after CaMKIα siRNA or compound-C pretreatment. Autophagy genes LC3B, APG5, and APG7 knockdown have different effects on cytokine releasing from RAW 264.7 after LPS treatment, they all reduced IL-1α release, siRNA LC3B increased IL-6, TNF-α release. In vivo, siRNA CaMKI inhibited expression of autophagy protein LC3B in mice subjected to CLP.
Conclusions: These results suggest that CaMKIα regulates autophagy in Mϕ responding to LPS, which depends upon complex between CaMKIα, AMPK and APG7. CaMKIα also directly regulates the mTOR (TORC1) pathway, suggesting that its regulation of autophagy occur independent of mTOR inhibition. Autophagy play a very important role in cytokine release in macrophages responding LPS. These events appear to be operant in vivo.
CarchmanEvieRaoJayShivaSrutiZuckerbraunBrian
University of Pittsburgh Medical Center
The Importance of HEME-Oxygenase 1 in Mitochondrial Biogenesis in Sepsis
Introduction: In sepsis there are various cellular pathways that are induced to prevent permanent organ injury and allow for the restoration of cellular homeostasis and metabolism. Central to these adaptive responses is the dynamic regulation of mitochondria to prevent bioenergetic failure. Damaged mitochondria must be removed and replaced with viable mitochondria to produce ATP and maintain basic cellular activities. Heme oxygenase-1 (HO-1) and its catalytic product carbon monoxide are known to be essential signaling molecules to limit inflammation, regulate cellular bioenergetics, and restore cellular homeostasis. Our objective was to test the hypothesis that mitochondrial biogenesis is necessary to prevent organ injury from sepsis, furthermore, to demonstrate that these processes are regulated by HO-1.
Methods: Primary mouse hepatocytes (MHC) with and without tin protophoryin treatment (SnPP) (50 uM), a non-specific inhibitor of heme-oxygenase were stimulated with lipopolysaccharide (LPS; 100 ng/mL) at various time points and mitochondrial function was examined by measuring the oxygen consumption rate, extracellular acidification rate, or mitochondrial membrane potential with JC-1 staining. ATP was also quantified as a measure of mitochondrial function in MHC with and without HO-1 siRNA transfection and LPS stimulation. Mitochondrial biogenesis was examined by immunofluorscene for PGC-1 alpha and NRF1, two important mitochondrial biogenesis transcription factors.
Cecal ligation and puncture was performed in C57Bl/6 mice with and without the administration of SnPP (50 ug/kg; IP). Immunofluorscene was done to evaluate for markers of mitochondrial biogenesis.
Results: Oxygen consumption rate (OCR) in MHC over time decreased until the 12 hour time point and then normalized by 24 hours. This normalization of mitochondrial function does not occur in those MHC which were pretreated with SnPP, in fact mitochondrial OCR continued to decrease over time. The decrease in the mitochondrial function after SnPP treatment was confirmed by looking at mitochondrial membrane potential with JC-1 staining. Looking at the ATP content, LPS stimulation lead to a decrease in ATP content compared to those without LPS stimulation. However, after inhibition HO-1 with siRNA there was an even more significant decrease in ATP content.
When looking at mitochondrial biogenesis transcription factors over time after LPS stimulation in MHC, there was a time dependent increase in PGC-1 expression in those MHC where HO-1 was functional. However, after the inhibition of HO-1 this induction was abrogated.
In the in vivo model of sepsis immunofluorscene confirmed the above in vitro data of the induction of PGC-1 alpha in those mice were HO-1 activity was not pharmacologically inhibited.
Conclusions: The induction of HO-1 after a septic insult is a protective mechanism to replace dysfunction mitochondria with functional mitochondria and to return cellular energetic homeostasis.
BakerAaron CMS, MDAminiAmirMDTungKellyMDChewVictoriaBSLimDeboraBAGreenTajiaBSChoKihoPhD, DVMGreenhalghDavidMD
University of California–Davis Medical Center
Novel Alternative Splice Variant of the Human Glucocorticoid Receptor Augments the Response to Hydrocortisone
Background: Since the initial trials evaluating steroid use in septic shock, little insight has developed as to why some patients respond to steroids and others do not. Prior clinical studies have identified five novel alternative splice variants of the human glucocorticoid receptor (hGR) as a contributor to a patient's inability to respond to steroid therapy in certain diseases. In order to further evaluate the role of hGR variations in humans, we hypothesized that glucocorticoid receptor polymorphisms influence the variability in the response to injury and may lead to individualized tailoring of steroid therapy.
Methods: Total RNA was isolated from ninety-seven healthy human volunteer blood samples and surveyed for the glucocorticoid receptor gene. A novel isoform termed hGR AS-1 resulting from an alternative splicing event and retention of intron H was identified. An hGR isoform matching the National Center for Biotechnology Information reference (hGR NCBI) was used for comparison. Transactivation potentials of TSA201 cells transfected with these hGR isoforms were measured using a reporter assay in the presence of equivalent doses of 0.9% saline or hydrocortisone. In order to further elucidate the mechanism of hGR AS-1, a deletion clone of hGR AS-1 was created in which the 3′ untranslated region (3′UTR) was removed and tested with hydrocortisone. Student's t-test was used for statistical analysis.
Results: Along with a retained intron, hGR AS-1 contains a frameshift mutation resulting in early termination of the coding sequence and a truncated protein of 118 amino acids (compared to the hGR NCBI of 777 amino acids). Isoform hGR AS-1 had decreased activity compared to hGR NCBI without hydrocortisone stimulation (p < 0.01). Most interestingly, a more than 10 fold increase in transactivation potential occurred in hGR AS-1 compared to hGR NCBI at a dose of 1 uM of hydrocortisone (p < 0.001) (Figure 1). A peak response was identified at 0.01 uM for hGR NCBI, whereas the peak response occurred at a higher dose of 1 uM for hGR AS-1. When the 3′untranslated region (3′UTR) was deleted from hGR AS-1, the resultant deletion clone no longer demonstrated a significant increase in transactivation potential when stimulated with hydrocortisone (p < 0.01). Western blot confirmed the protein lengths.
Transactivation potential after hydrocortisone stimulation of hGR AS-1 and hGR NCBI. A greater than 10 fold increase in activity occurs between hGR AS-1+ Hydrocortisone and hGR NCBI + Hydrocortisone at 1μM (*p < 0.001).
Conclusion: A novel glucocorticoid receptor alternative splice variant isoform caused by an intron retention exists in healthy humans. hGR AS-1demonstrates decreased transactivation potential at baseline, but displays an impressive hyperactive transactivation potential in response to exogenous hydrocortisone in a dose dependent fashion. The 3′UTR appears to be a key mediator of this increased transactivation potential. Additional characterization of such unique isoforms in humans may help explain the differential response to steroids in inflammatory states and allow for tailored steroid therapy.
KhadarooRachel GMD, PhD, FRCS(C)ChurchillThomas APhD, BScLukowskiChristopher MMScFedorakRichard NMD, FRCPC, FRCP(London)MadsenKaren LPhD
University of Alberta
Metabolomic Profiling to Characterize Acute Intestinal Ischemia/Reperfusion Injury
Introduction: Sepsis and septic shock are the leading causes of death in critically ill patients. The gastrointestinal tract is an important defense barrier for the body; in critically ill patients it can become a major pathogenic source of bacteria and inflammatory mediators leading to a septic response. Acute intestinal ischemia/reperfusion (AII/R) is an adaptive response to shock; mortality ranges from 60–90% and have not changed since the 1940s. The high mortality rate for AII/R is due to the severity of the disease and, more importantly, the failure of timely diagnosis.
Background: Metabolomics is the study of low molecular weight compounds generated by cellular metabolism. The metabolite profile of an organism can vary as a result of environment, activity, or disease. To date, there have been no studies applying this technology to the area of AII/R induced lung injury. The aim of this investigation is to correlate the development of AII/R with specific changes in metabolites which will aid in the diagnosis and understanding the metabolite fingerprint associated with local and distant organ injury.
Methods: We have established a model in 129/SvEv mice where AII/R results in acute lung injury (ALI) in a time dependent manner. Mice were subjected to intestinal ischemia by occlusion of the superior mesenteric artery. A time course of intestinal ischemia from 0.5 to 1 h was performed and followed by reperfusion for 2 h. Urine metabolomic profiles using nuclear magnetic resonance (NMR) spectroscopy were used to find differences in metabolites during the time course of AII/R. Principal component analysis (PCA) and partial least-squares-discriminant analysis (PLS-DA) were conducted using SIMCA P11.0 (Umetrics, Umea, Sweden).
Results: Metabolite concentrations were derived from analysis of NMR spectra from urine samples from mice exposed AII/R. Altogether, 57 compounds were identified in the spectra (e.g. alcohols, amino acids, fatty acids, lipids). PCA and PLS-DA of the data derived from measured urinary metabolite concentration demonstrate large differences in metabolomic profile could be delineated based on length of ischemia (Fig A and B). Interestingly, lactate was not an important metabolite driving the differences between these groups.
Conclusion: This study illustrates that urinary metabolites concentration may be effective at distinguishing AII/R progression in an animal model. The novel use of metabolomic studies to generate an AII/R metabolite profile is a much needed top-down approach to bridge existing knowledge gaps. The discovery of a fingerprint profile of AII/R will be a major advancement in the diagnosis, treatment, and prevention of systemic injury in critically ill patients.
ElijahItoro EMD, MPHFinnertyCeleste C.PhDBywaterDon CBSArnoldoBrett AMD, FACSGamelliRichard LMD, FACSGibranNicole SMD, FACSJeschkeMarc GMD, PhDKleinMatthew BMDTompkinsRonald GMD, ScD,HerndonDavid NMD, FACS
University of Texas Medical Branch–Shriners Burns Hospital, Galveston, Texas
No Associated Increase in ARDS or Sepsis with Beta-Blocker use in Adult Burn Patients: A Multi-Center Study
Introduction: The recently published POISE trial suggested that beta-blockade with metoprolol in patients older than 45 years of age with atherosclerotic heart disease increased mortality and other complications. Our group has successfully used propranolol to decrease the hypermetabolic response in both pediatric and adult burn patients. Here we examined data collected as part of a larger federally-funded multi-center program to determine the morbidity and mortality associated with beta-blockade in adult burn patients.
Methods: Patients admitted within 96 hours of injury and with burn size > 20% TBSA were consented to participate in a larger federally-funded study. Data from 251 patients (132 on beta-blockers (dose and agent not identified) and 119 controls) was down-loaded from the trial database. Two-tailed student t-tests were used to compare data from the two groups.
Results: No differences were found between the two groups for incidences of ARDS, sepsis, cardiac events, vascular events, bradycardia, or hypotension. Although patients on beta-blockers were more likely to develop pneumonia or blood stream infections, they were less likely to die from these infections. Survival was increased in the beta-blocker group (88% vs. 76%, p < 0.05).
Conclusion: In this preliminary evaluation, beta-blocker use in hospitalized adult burn patients improved survival and was not associated with increased cardiac or pulmonary events. As this trial was not a randomized prospective trial to test the efficacy or safety of a single beta-blocking agent, we do not know which beta-blockers were used nor the doses administered. However, the findings of this trial support the need for further demonstration of safety and efficacy testing of particular beta-blockade agents in adult burn patients.
KunacAnastasiaMDSifriZiad CMDMohrAlicia MMDHorngHelenPharmDLaveryRobertMSLivingstonDavid HMD
University of Medicine and Dentistry, New Jersey–New Jersey Medical School
Bacteremia and VAP: A Marker for Contemporaneous Extra-Pulmonic Infection
Introduction: Ventilator Associated Pneumonia (VAP) is a well known complication in severely injured patients. A subset of patients with VAP develops an associated bacteremia (B-VAP), and the risk factors, microbiology, morbidity and mortality are not well described. The goal of this study was to examine the incidence, predictors, and outcome of B-VAP in adult patients admitted to a level-I urban trauma center.
Methods: Retrospective review of trauma patients who developed VAP or B-VAP from 1/07-12/09. VAP was defined as a documented VAP along with positive respiratory cultures (BAL with ≥ 104 organisms or tracheal aspirate with moderate-many organisms and PMNs). Recurrent VAP was defined as positive respiratory cultures after ≥ 7 days of antibiotic therapy. B-VAP was defined as organism cultured from blood matching the lung pathogen. Demographic data, injury severity, transfusion and microbiology were reviewed. Outcome included ICU and hospital length of stay, ventilator days and survival. A student t-test, chi-square test or logistic regression was used as appropriate.
Results: 4,018 adult patients were admitted during a 36-month period. 206 patients were diagnosed with VAP (5%), and 13% had an associated bacteremia. Mean time from admission to the development of VAP was 5 days (95% CI 4.6-5.8). In our population, initial Gram-negative (G-) VAP were twice as common as Gram-positive (G+) and bacteremia was more common in G- vs. G + VAP (16% vs. 10%). Patients who had B-VAP received significantly more units of PRBC transfusion (see table). Of 206 patients, 70 (34%) had recurrent pneumonias—patients with B-VAP had higher rates of recurrent pneumonia (54% vs. 31%). Patients with B-VAP compared to VAP alone also had higher rates of simultaneous non-pulmonary infections (69% vs. 38%). Patients with B-VAP had increased days of mechanical ventilatory support, increased number of ICU days (ICU LOS) and hospital length of stay (H LOS) compared to patients with VAP alone (see table). Patients with B-VAP trended towards a lower survival, but B-VAP was not an independent predictor of mortality.
VAP (%)
Age (y) (95% CI)
ISS (95% CI)
PRBC (95% CI)
Vent Days (95% CI)
ICU LOS (95% CI)
H LOS (95% CI)
Mortality (95% CI)
VAP alone
45
27
9u
14d
17d
30d
15
N = 180
(42-48)
(25-28)
(7-11)
(13-15)
(15-18)
(27-33)
(8%)
B-VAP
46
27
23u
24d
26d
50d
6
N = 26
(37-54)
(22-34)
(13-34)
(17-30)
(19-33)
(33-66)
(23%)
p value
NS
NS
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p = 0.06
Conclusion: The number of blood transfusions received is the most significant risk factor for developing B-VAP and B-VAP is associated with a higher morbidity than VAP alone. Over two-thirds of patients with B-VAP have a contemporaneous infection and more than half develop recurrent VAP. Trauma patients with B-VAP may benefit from increased surveillance for additional concomitant infections or more aggressive antimicrobial coverage.
DuaneTherese MMDYoungAndrewMDWebberWilliamBSWolfeLuke GMSMalhotraAjai KMDAboutanosMichel BMD, MPHWhelanJames FMDMayglothlingJulieMDIvaturyRao RMD
Virginia Commonwealth University Medical Center
Bladder Pressure Measurements and UTI in Trauma Patients
Introduction: In an effort to decrease urinary tract infections (UTI) in our ICU we evaluated the role of bladder pressure measurements (BPM) as a possible risk factor. We demonstrated that BPM using an open technique was an independent predictor of UTI and correlated with a higher mortality rate in critically injured patients. The purpose of this trial was to determine if changing to a closed technique for BPM would eliminate it as a risk for UTI in trauma patients.
Methods: Data was collected prospectively from 1/06 until 12/09 by a dedicated epidemiology nurse and combined with data from the trauma registry at our Level 1 trauma center. All trauma patients admitted to the surgical trauma ICU (STICU) with and without UTI's were compared for demographics, injury severity (ISS), and epidemiologic data including urinary drainage catheter (UDC) use and bladder pressure measurements (BPM). CDC definitions were used to diagnose UTI. BPM were performed when there was a concern for intra abdominal hypertension. A closed system was used in which the UDC remained connected to the bag and 45cc of saline was injected through a two way valved sideport with subsequent measurements through the sideport.
Results: A total of 1641 patients were included in the trial. The UTI group was sicker, with longer LOS and UDC days compared to the no UTI group (Table 1). There were 285 patients with no UDC and 1 UTI (0.35%), 1292 patients with UDC but no BPM with 37 having a UTI (2.86%) and 64 patients who had UDC and BPM of whom 8 had UTI's (12.50%) (p < 0.0001). The BPM group had more UDC days (15.6 days ± 16.0 BPM vs. 5.4 days ± 7.3 no BPM, p < 0.0001) yet no differences in UTI rates/1000 UDC days (5.7 no BPM vs. 8.0 BPM, p = 0.5291). Subset evaluation of patients with BPM found that those patients who also had UTIs had more BPM obtained compared to those with no UTIs (22 ± 16.1 UTI vs. 9.34 ± 8.34 no UTI, p = 0.0147 yet there was no difference in UTI rates in those patients who had an elevated level (>20) compared to those with only normal measurements (p = 0.1771). Logistic regression demonstrated only UDC days (not BPM or ISS) to be a predictor of UTI (1.125, 1.097–1.154, p < 0.0001) while ISS (1.083, 1.063-1.104, p < 0.0001) and age (1.051, 1.037–1.065, p < 0.0001) were the only predictors of mortality.
No UTI
UTI
P value
ISS
18.7 ± 11.9
28.0 ± 10.7
<0.0001
Vent LOS(days)
2.0 ± 4.9
8.3 ± 8.6
<0.0001
ICU LOS (days)
5.5 ± 7.9
27.5 ± 17.4
<0.0001
Hosp LOS (days)
11.4 ± 12.4
37.9 ± 20.3
<0.0001
UDC days
4.3 ± 6.6
23.9 ± 16.6
<0.0001
Conclusion: Although BPM patients have more UTI's compared to those patients without BPM it is not an independent predictor of UTI using the closed system thereby proving the hypothesis. Regardless of BPM or ISS, patients with prolonged UDC use are at higher risk for UTI as are those patients who have more BPM obtained although this was not an independent predictor. These findings emphasize the judicious use of BPM using a closed system and more importantly the need for early removal of these catheters. Hence patients should be evaluated everyday for the need for BPM and UDC and should have discontinuation of both whenever possible.
MonaghanSean FMDHeffernanDaithi SMDMachanJason TPhDHarringtonDavid TMDAdamsCharles AMDCioffiWilliam GMD
Rhode Island Hospital/Alpert Medical School of Brown University
Low Phosphorus is Predictive of the Development of Infections after Surgery: A Study of Humans to Prove Murine Data
Background: Hypophosphatemia is known to occur after a surgical stress in humans. The low phosphorus is due to a combination of negligible dietary intake, increased renal excretion, and the movement of phosphorus intra-cellularly due to glucose/insulin administration. In addition, in murine models, low phosphate levels have been shown to increase the virulence of pathogens common in post surgical infections (Pseudomonas and Candida) and therefore should lead to an increase in the number of infections.
Methods: All adult patients who underwent an operation while admitted to a general surgery service (minimally invasive, colorectal, endocrine, surgical oncology, thoracic, renal transplant, vascular and trauma) from 2005 to 2010 and had at least one phosphate level drawn were included in the study. Patients were noted to have a postoperative infection if cultures from the wound, blood, urine, bronchial-alveolar lavage, catheter tip, or stool for C. difficile were positive. The lowest recorded serum phosphorus level was then used to predict the hazard of the development of a post-operative infection within 30 days of the operation. The institutional review board of Rhode Island Hospital approved this study.
Results: Over the five years, 6,493 patients were included in the analysis. 5,310 of these patients did not have a culture proven infection. The average lowest phosphate was 2.56 in the infection group and 2.78 in the group with out an infection (p < 0.0001). In a proportional hazards regression model to predict the development of a postoperative infection using phosphorus, each increase in phosphorus reduced the risk to develop an infection by 0.892 (Pr > ChiSq = 0.0019). When the patients were divided by type of surgical case (clean, clean-contaminated, contaminated/dirty) similar results were seen. In the proportional hazards model to predict infection, each increase in phosphorus reduced the risk by 0.842 in the clean-contaminated cases (Pr > ChiSq = 0.0242) and 0.864 in the contaminated/dirty cases (Pr > ChiSq = 0.0260). In the clean cases, the ability to predict infection by phosphorus level was lost.
Conclusion: Low levels of phosphorus have been previously shown to increase the virulence of common pathogens in murine models. Here we show that postoperative hypophosphatemia increases the risk of infection in humans. This study translates research initially done in mice and proves its applicability to humans. Based upon these findings we advocate for routine monitoring of phosphorus levels in post surgical patients as well as regular phosphorus replacement to achieve high-normal levels and to consider phosphorus supplementation pre-op.-.
LeitmanI. MichaelMDBowerMargaretMDKashanGlennMDIllicThomasMDde ChavezVincentSeigermanMatthewMDEnkerWarren EMDKarpehMartin SJR.MDHuralskaMariya
Albert Einstein College of Medicine- Beth Israel Medical Center
Does Elevated Glycosylated Hemoglobin Predict Post-Operative Infectious Complications?
Background: Previous studies have suggested an association between elevated pre-operative glycosylated hemoglobin (HbA1C) and complications following cardiac and bariatric surgical procedures. Recent literature has suggested that an elevated glycosylated hemoglobin level is a risk indicator for surgical site infection (SSI) and other adverse outcomes in patients with or without diabetes.
Methods: This was an IRB approved research project. A power analysis was performed to determine the necessary sample size to determine if there would be a statistical difference in a group of patients with an expected post-operative infection rate of 3%. 1610 consecutive patients had serum HbA1C levels obtained as part of their routine pre-operative surgical testing. The records from diabetic or non-diabetic patients undergoing elective surgery from January to August 2010 were analyzed. Patients whose surgery was cancelled in order to optimize their pre-operative glucose were excluded from this analysis. Post-operative outcomes were considered adverse if the patient developed a surgical site infection, deep wound abscess, urinary tract infection, or pneumonia within 30 days of their operation.
Results: 687 males and 923 females with a mean age of 46.9 years underwent elective surgery. Overall, 50 patients had an infectious complication (3.1%). There were 29 surgical site infections (1.8%), 13 urinary tract infections (0.8%), 4 pneumonias (0.2%) and 4 deep wound abscesses (0.2%). 26 percent of the patients that had an infectious complication had a preoperative HbA1C of greater than 6.0 percent; compared to 20 percent of uncomplicated post-operative patients (P = 0.293). The mean HbA1C in the group of patients that had infection was 5.9% compared to 5.8% in the group of patients that did not have post-operative infection (P = 0.4). There was no correlation between age, gender and the development of post-operative infectious complication.
Conclusion: Pre-operative measurement of HbA1C levels may be useful in the identifications of patients with occult diabetes but does not appear to predict the development of post-operative infectious complications in this population of patients undergoing elective surgery.
DornHarry FMDSchmittTimothy MMDKumerSean CMD, PhDBraymanKenneth LMD, PhDAgarwalAvinashMDSawyerRobert GMD
University of Virginia
Increased Morbidity and Mortality Associated with Post Liver Transplant Intra-Abdominal Infections Caused by Candida Species and Vancomycin-Resistant E. Faecium
Introduction: Intra-abdominal infection continues to be an important problem in surgical practice and is increasingly associated with the isolation of fungi and resistant pathogens.
Background: For liver transplantation, intra-abdominal infection presents a special challenge due to the complexity of the surgery and the need for immunosupression. In addition, transplant patients are at high risk for infections with fungi and vancomycin-resistant enterococci (VRE). We hypothesized that fungi, including, Candida species and unspeciated yeasts, and VRE would be common pathogens after liver transplantation and would be associated with significantly higher mortality, particularly when isolated together.
Methods: Review of all liver transplants in a single institution as well as episodes of intra-abdominal infection following liver transplantation. Specific isolates were analyzed and differences in outcomes were compared using Chi square analysis and Student's t-tests. Results: In our institution we performed 640 liver transplants from December of 1996 to October 2010; these were complicated by 410 episodes of intra-abdominal infection following transplantation. 306 occurred in males and 104 in females. Enterococcus faecium (100 isolates/24.4% of cases, including 65 VRE) and Candida species including unspeciated yeast (90 isolates/22.0% of cases) were the most common pathogens cultured. Demographics and outcomes, including hospital length of stay (LOS) and mortality, are given in the table below.
Conclusion: We conclude VRE and Candida species causing intra-abdominal infections result in significant morbidity and mortality for liver transplant patients, and their combination may be even more lethal. Empiric antimicrobial therapy with activity against VRE and yeast should be considered in all liver transplant patients suspected of having a new intra-abdominal infection. Whether these pathogens should also be targeted with perioperative antimicrobial prophylaxis deserves further study.
GreggZachary AMDHeffernanDaithi SMDMonaghanSean FMDConnollyMichael DMDGreggShea CMDKozloffMatthew SMDAdamsCharles AMDCioffiWilliam GMD
Rhode Island Hospital/Alpert Medical School of Brown University
Nasal MRSA Predicts Ventilator Associated Pneumonia and Microbiology
Introduction: Methicillin-resistant Staphylococcus aureus (MRSA) remains a common and problematic hospital pathogen. Previous reports have documented that nasal MRSA colonization increases the risk of developing MRSA in a subsequent infection. Ventilator associated pneumonia (VAP) remains a persistent problem in intensive care units. However, little study has been undertaken exclusively in surgical patients to evaluate the direct association between nasal MRSA colonization and subsequently having MRSA as the causative organism of pneumonia.
Methods: This is a retrospective chart review of surgical patients admitted over 3 years. Patients were included if they were aged 18 years and older, admitted to a general surgery or trauma service and underwent nasal MRSA screening. Patients who were clinically suspected of having pneumonia underwent bronchoalveolar lavage (BAL) with samples sent for culture and sensitivity. Pneumonia was defined as either ≥ 2+ organisms on qualitative culture, or a count of at least 10,000 organisms/ml on quantitative culture. Institutional review board approval was obtained for this study.
Results: Over the study period 4281 patients were included and of these 386 (9%) were positive for MRSA in the nares. Furthermore 4% (169/4281) of patients included developed pneumonia. Patients that were MRSA nares positive were twice as likely to develop pneumonia (7.5%, 29/386) compared to patients who were MRSA nares negative (3.6%, 140/3895, p = < 0.001). MRSA nares screening samples were also compared with the BAL microbiology in patients who developed pneumonia. In patients that developed pneumonia and were MRSA nares positive, 51.7% (15/29, p = < 0.001) had MRSA pneumonia. In patients that developed MRSA pneumonia, 83.3% (15/18, p = < 0.001) had been MRSA nares positive. In patients that developed pneumonia and were MRSA nares negative, only 2.1% (3/140, p = < 0.001) had MRSA pneumonia.
Conclusion: This is a unique description of a direct association between nasal MRSA carriage and subsequent MRSA pneumonia in an exclusively surgical population. Nasal MRSA colonization increases the risk of both developing pneumonia and specifically MRSA pneumonia. Furthermore, the current oral care alone may be inadequate to minimize MRSA pneumonia. We propose that all patients with anticipated intubation for greater than 24 hours should undergo nasal MRSA screening, and if positive, subsequent treatment with mupirocin. Finally, in patients who are MRSA nares negative, the empiric antibiotic regime could be narrowed to exclude MRSA coverage.
WilliamsAlicia MMDBochicchioGrant VMDZhuShijunPhDBochicchioKellyRN, MSScaleaThomasMD
Walter Reed Army Medical Center
Ventilator Free Days as a Predictor for Pneumonia: Is it Accurate?
Background: Recently, the use of ventilator free days VFDs28 (based on 28 days) in predicting outcomes in critically ill patients has been advocated in favor of total ventilator days. Our objectives of this study were to compare number of ventilator days to VFDs (28 day) versus actual ventilator free days in predicting pneumonia in critically injured trauma patients.
Methods: Prospective data were collected on 703 patients who were ventilated between 2001 and 2008 at a level one trauma center. Data collected included gender, race, ISS score, mechanism of injury (MOI). Primary outcomes include the diagnosis of pneumonia, number of ventilator days, number of ventilator free days (VFD), mortality, and hospital length of stay (HLOS). Three separate analyses were performed to predict pneumonia: 1: total number of ventilator days 2:number of VFDs using the 28 day criteria, 3: number of actual VFDs defined as (HLOS-x), where x is the number of days on ventilation. Univariate and logistic regression models were utilized in this model.
Results: 703 patients were enrolled in the study. The mean age and ISS were 40 ± 19 and 28 ± 13 respectively. The majority of patients were male (78%) and MOI was blunt (82%). The average HLOS and ILOS were 15 ± 16 and 13 ± 14. The mortality rate was 13.9%. The diagnosis of pneumonia was made in 146 patients. 91 patients (13%) were in the hospital longer than 28 days. Ventilator days were found to be a significant predictor of developing pneumonia (p < 0.001). Using the 28 day criteria of VFDs, the amount of time off of the ventilator decreased the likelihood of developing pneumonia (p < 0.001). Actual VFDs was not associated with a significant decrease in pneumonia (p = 0.234).
Conclusion: Actual ventilator free days was not found to be a useful predictor of outcome. Although VFDs was predictive of pneumonia, it did not account for 13% of our patient population. A new model is needed to better predict outcome in critically ill patients who are in the hospital beyond the 28 day study period.
BlancoFelix CMDDavenportKatherine PMDNadlerEvan PMDSandlerAnthony DMD
George Washington University School of Medicine-Children's National Medical Center
The Effect of Adopting a Clinical Pathway for the Management of Pediatric Appendicitis and Comparison to the Pediatric Health Information System Database
Introduction: Health care reform drives hospitals to adopt policies to reflect evidence-based medicine and optimize provision of care and utilization of resources. To achieve these goals, our children's hospital implemented a protocol for the management of appendicitis utilizing a single-agent antibiotic regimen and a uniform clinical pathway for discharge in 2007. We analyzed the effects of our protocol by comparing our outcomes before and after protocol implementation to those reported in the Pediatric Health Information Systems (PHIS) database.
Methods: Data were collected from medical record review of patients with perforated appendicitis at our institution between 2004 and 2009. A clinical pathway for the management of appendicitis was initiated in 2007 using a uniform single-agent antibiotic regimen (ertapenem) and detailed discharge criteria (afebrile for 24 hours, tolerating oral intake, adequate pain control, and decreasing white blood cell count.) Additionally, data were collected from the PHIS database which represents 41 free-standing children's hospitals from 2004–2009. Hospital length of stay (LOS) and thirty day readmission rates were calculated and compared pre- and post- protocol implementation. Additionally, our data were compared to those from the PHIS database pre- and post- protocol initiation. Mean values were compared using Student's t-test, and categorical data were compared using chi-square analysis.
Results: Between 2004 and 2009, there were 544 patients with the diagnosis of perforated appendicitis admitted to our institution, and the PHIS database registered 23,276 perforated appendicitis patients. After implementation of the protocol, the average LOS decreased from 6.4 ± 5.3 days to 4.5 ± 2.9 days (p = 0.0001). Prior to implementation of the protocol, our average LOS, though not statistically significant, was greater than the reported national average (6.4 ± 5.3 days versus 6.1 ± 4.3 days, p = 0.267), and following implementation is now lower than the national average (4.5 ± 2.9 days versus 6.0 ± 4.4 days, p = 0.0001). The number of hospital readmissions within thirty days did not change significantly following the initiation of the protocol (8.1% vs. 11.2%, p = 0.3). Additionally, the pre- and post-protocol readmission rates were comparable to the PHIS data.
Conclusion: Adopting a clinical pathway using a single-agent antibiotic regimen and uniform discharge criteria has led to decreased LOS for children with perforated appendicitis when compared to pre-protocol outcomes as well as national administrative data. Furthermore, the protocol implementation has not adversely affected patient outcomes as measured by thirty day readmission rates. We recommend the development and utilization of a clinical protocol including a single-agent antibiotic regimen and uniform discharge criteria for the management of perforated appendicitis in children to optimize patient care.
OsukaAkinoriMDDesikanSarasijhaa KBSHanschenMarcMDTajimaGoroMDLedererJames APhD
Brigham and Womens Hospital/Harvard Medical School
Preventing Injury-Associated Sepsis by Redirecting the Immune System
Introduction: Severe injury disrupts immune system homeostasis and predisposes trauma patients to infections and complications. In this study, we wished to test whether early intervention with Rapamycin - a drug that is used to prevent host rejection in organ transplantation – might help restore immune system homeostasis by changing the clinical trajectory of the injury response. Since Rapamycin is known to enhance the activation and expansion of CD4 + regulatory T cells (Tregs), an immune cell that is activated by injury and is counter-inflammatory, we hypothesized that Rapamycin may help counteract the pro-inflammatory response to burn injury in mice.
Methods: Mice underwent sham or burn injury under anesthesia and were treated with Rapamycin (1 mg/kg) or vehicle by intraperitoneal injection. Sepsis survival was evaluated by the cecal ligation and puncture (CLP) method at day 7 after sham or burn injury. Immunophenotyping was accomplished by FACS analysis of blood, spleen, and lymph node cells and by profiling changes in cytokine production by spleen cells that were stimulated with a variety of innate and adaptive immune cell stimuli.
Results: The timing for Rapamycin treatment was assessed by measuring Treg expansion at 7 days after injury in mice that were treated at 2 hours, 1 day, or 3 days post-injury. We observed that treatment at 2 hours after burn injury caused significant expansion of Tregs as compared to day 1 or day 3. Given this finding, we used 2 hour post-injury treatment to test whether Rapamycin might protect mice from two-hit sepsis mortality induced by CLP. We found that burn-injured mice treated with Rapamycin survived CLP sepsis significantly better than vehicle treated mice. Interestingly, there was no significant change in CLP mortality between sham and Rapamycin-treated sham mice. Immunophenotyping studies showed that Rapamycin treatment did not significantly alter the immune cell subset percentages in peripheral immune compartments and that innate responses were not markedly altered. However, we found that Th2-type cytokine production was significantly reduced by Rapamycin treatment. The results of in vitro studies indicated that Rapamycin potently blocked T cell cytokine responses suggesting that T cells represent the primary cell type that may be affected by Rapamycin treatment. We did not observe significant effects of Rapamycin treatment on innate immune cell responses to Toll-like receptor stimuli.
Conclusion: These findings support a potential for using Rapamycin as an early interventional drug treatment to restore immune system homeostasis and to reduce the morbidity and mortality of sepsis following major injury. Furthermore, these data suggest that Rapamycin may act by altering adaptive immune system activation following burn injury.
HustonJaredMD
State University of New York, Stony Brook
Cholinergic Regulation of ANP Signaling During Sepsis
Introduction: Atrial natriuretic peptide (ANP) is a hormone secreted primarily by cardiac myocytes that functions in regulation of blood volume and pressure. Evidence indicates that ANP also has potent immunomodulatory effects. ANP suppresses proinflammatory cytokine production and inhibits NFκB activation in tissue macrophages. ANP release from the spleen can cause hypotension and shock in murine endotoxemia. Clinical studies show that concentrations of circulating ANP correlate directly with morbidity and mortality in patients with lethal sepsis.
The cholinergic anti-inflammatory pathway is an endogenous, brain-to-immune pathway that inhibits pro-inflammatory cytokine production, prevents shock, and suppresses lethal organ damage in experimental sepsis. We found that this vagus nerve-mediated pathway specifically targets immune cells in spleen. Interruption of the hard-wired neural connection between the vagus nerve and the spleen abolishes the protective effects of the cholinergic anti-inflammatory pathway.
In light of these findings, we hypothesized that activation of the cholinergic pathway may regulate systemic cytokine production via modulation of ANP in spleen. Here we studied whether administration of the cholinergic agonist nicotine regulates systemic and splenic ANP and TNF production in murine models of systemic inflammation and sepsis.
Methods: Male 8–12 week old BALB/c mice received vehicle or endotoxin (15 mg/kg, i.p., E. coli LPS 0111:B4; Sigma-Aldrich). Plasma and organs were collected after 60 min. Nicotine (2 mg/kg, i.p., Invitrogen) or vehicle was administered 1–2 hrs prior to endotoxin. TNF and ANP concentrations were measured using ELISA (R&D Systems, Phoenix Pharmaceuticals). BALB/c mice underwent cecal ligation and puncture and splenectomy as described previously (Huston et al. 2006. J Exp Med 203; 1623–28). Plasma was collected after 24 hrs. One-way ANOVA using the Bonferroni correction or the Student's t test was used to compare mean values between multiple or two groups, respectively. p-values < 0.05 were considered statistically significant.
Results: Nicotine significantly reduces systemic and splenic TNF concentrations in endotoxemic mice. Nicotine also significantly reduces systemic ANP concentrations, but significantly increases ANP concentrations in spleen. Splenectomy significantly reduces systemic TNF concentrations in endotoxemic mice. There is a trend towards decreased ANP concentrations in splenectomized, endotoxemic mice (p < 0.07). In splenectomized mice, nicotine paradoxically increases systemic TNF, and fails to reduce systemic ANP concentrations. Splenectomy significantly improves survival and decreases systemic ANP during CLP sepsis.
Conclusions: The cholinergic anti-inflammatory pathway reduces systemic ANP and TNF concentrations, but only in the presence of the spleen. Nicotine reduces TNF concentrations, but increases ANP concentrations, in spleen. Splenectomy decreases ANP concentrations and improves survival in CLP sepsis. These findings suggest that the cholinergic pathway may inhibit systemic cytokine production by limiting splenic ANP release and enhancing ANP signaling in spleen. Further studies are needed to determine if specific ANP signaling in spleen is essential to the protective effects of the cholinergic anti-inflammatory pathway.
SaveliCarla CMDMorganSteven JMDBelknapRobert WMDRossErinBSStahelPhilip FMDChausGeorge WMDBifflWalter LMDPriceConnie SMD
University of Colorado-Denver
The Role of Antibiotics in Open Fractures Revisited: Characteristics of Staphylococcus Aureus (SA) and Susceptibility Profile
Background: The benefits of antibiotic prophylaxis in open fractures have been clearly demonstrated in several randomized controlled trials, but the choice of antibiotic remains controversial since the current guidelines do not recommend agents with methicillin resistant Staphylococcus aureus (MRSA) activity.
Methods: To develop preliminary data on the incidence of S. aureus (SA) colonization and surgical site infections (SSI) in patients with open fractures, a randomized prospective clinical trial was performed to compare the safety and benefits of adding MRSA coverage to standard antibiotic prophylaxis. Between April 2009 and November 2010, all consecutive adult patients with an open fracture who met study criteria were included. Patients were randomly allocated to receive either cefazolin alone (control arm) or vancomycin and cefazolin (experimental arm) from presentation to the ER until 24 hours after the surgery. Screening for SA carriage was performed with nares swabs and open fracture wound swabs. Patients underwent prospective assessment for the development of SSI within 30 days of the initial surgery.
Results: Over a 20-month period, 92 patients with an open fracture were randomized to one of the prophylactic antibiotic regimens (46 subjects in each study arm). Study demographics and baseline characteristics were balanced between the two groups. 21.7% of the subjects were identified as colonized with SA. The prevalence of methicillin sensitive SA (MSSA) and MRSA among the sample were 18.4% and 3.2% respectively. None of the open fracture wounds were found to be colonized with SA. Overall 8 of 92 patients (8.7%) developed a SSI, 4 of 46 in each study group. Selected characteristics of patients who developed a SSI are summarized in Table 1. No adverse events in either of the study arms were reported during the study period.
Selected Characteristics of Patients Who Developed a SSI
Conclusions: Preliminary findings demonstrate that addition of vancomycin to standard antibiotic prophylaxis is safe. SA was the most common cause of SSI after open fractures. SA colonization in orthopedic trauma patients is similar to the general population and methicillin resistance was shown in 3.2% of these patients. Pathogens inherently resistant to cephalosporins (i.e. Enterococcus) were also causative pathogens in two SSIs, one of which was susceptible to vancomycin. Further data are needed to determine whether the addition of vancomycin to standard antibiotic prophylaxis prevents the development of SSI compared to standard regimens.
RosenbergerLaura HMDTurzaKristin CMDRiccioLin MMDPolitanoAmani DMDSawyerRobert GMD
University of Virginia Health System
A Comparison of Infections in Solid Organ Transplant Recipients and Immunosuppressed Non-Transplant Surgery Patients: Does the Alloresponse Matter?
Introduction: One of the most common life-threatening complications in long-term immunosuppressive therapy populations is infection. A blunted inflammatory response is seen in the transplantation patient following induction of immunosuppression, and a high rate of infectious complications ensues. Whether the infectious morbidity is due entirely to iatrogenic immunosuppression or also depends on the immunomodulation induced by the presence of an allograft (the “alloresponse”) is unclear. We hypothesized that the transplant population, as compared to other non-transplant immunocompromised surgical patients, has a greater morbidity and mortality from infection, possibly due to the alloresponse.
Methods: Using a prospectively-collected dataset tracking surgical infectious complications over a 15-year time period, all non-viral infections were identified for solid organ transplant recipients and non-transplant immunocompromised surgical patients, defined as fulfilling the definition of immunosuppression by APACHE II criteria (chronic low-dose corticosteroids, acute high dose corticosteroids, etc.). Total infections, mortality following infection, crude mortality, length of stay, and APACHE II scores were obtained. Fisher's exact test and t-tests were used to compare the two groups.
Results: A total of 795 transplant and 412 non-transplant, immunocompromised patients with infections were identified. The most common indications for immunosuppression in non-transplant patients were inflammatory bowel diseases, rheumatoid arthritis/autoimmune diseases, and COPD/asthma. Transplant recipients had a total of 1781 infections, a mean of 2.24 infections per patient, and non-transplant patients had 659 infections, a mean of 1.60 infections per patient. APACHE II scores were 16.1 ± 6.4 and 15.3 ± 7.1 for transplant and non-transplant patients, respectively (p = 0.039). No significant differences were found between sites of infection or causative pathogens, with the exception that transplant patients had a higher percentage of infections caused by resistant organisms, most notably vancomycin-resistant enterococci. Hospital length of stay after the diagnosis of infection was 18.5 ± 23.0 days for transplant and 23.9 ± 35.8 days for non-transplant patients (p = 0.002). All-cause, in-hospital mortality following an infection for the transplant recipients was 9.6% and the non-transplant patients was 10.2% (p = 0.76).
Conclusion: Despite the fact that transplant recipients, when compared to non-transplant, immunocompromised surgical patients, have a greater severity of illness, more infections with resistant pathogens, and more infections per patient, their overall survival is similar. These findings suggest that the transplant patients' susceptibility to contracting an infection may be higher than other immunosuppressed patients but the ultimate ability to clear the infection is unchanged. Whether these findings are due to the alloresponse or level of immunosuppression remains unclear.
RichardsJustin EMDKauffmanRondiMD, MPHObremskeyWilliam TMD, MPHMayAddison KMD
Vanderbilt University Medical Center
The Relationship of Stress-Induced Hyperglycemia and Infectious Complications in Non-Diabetic Orthopaedic Trauma Patients
Introduction: Infection following orthopaedic surgery is a significant concern for the treating surgeon. The purpose of this investigation was to evaluate the effect of stress-induced hyperglycemia on infectious complications in a population of orthopaedic trauma patients.
Methods: Retrospective study of isolated orthopaedic trauma patients admitted to an academic Level-1 trauma center from January 2004-October 2009. Inclusion criteria: age ≥18 years, Intensive Care Unit (ICU) stay ≥1 day, orthopaedic injury requiring operative intervention, and more than 1 documented blood glucose (BG) value. Patients with a history of diabetes mellitus, corticosteroid use, immunologic disease, or Abbreviated Injury Scale scores other than Extremity were excluded. Demographic, injury severity, units of red blood cell transfusion, blood glucose (BG), and infectious complication data were obtained. Duration of ICU and hospital length of stay (LOS) was recorded. Infections considered were pneumonia, urinary tract infection (UTI), surgical site infection (SSI), and bacteremia. The Hyperglycemic Index (HGI) was calculated for each patient and reflects the mean BG level above 108 mg/dL. HGI was determined from BG values obtained prior to the diagnosis of infection. HGI was considered separately as a continuous variable and a dichotomous variable > 1.72 (equivalent to BG of 140 mg/dL). Multivariable logistic regression testing the effect of blood glucose on SSI was evaluated, after controlling for potential confounding variables. Significance was considered for p-value < 0.05.
Results: 187 patients were identified. All were managed with a tight glycemic protocol (target BG: 80-110 mg/dL). An average of 21.5 BG values was obtained for each patient. Mean age was 47.7 ± 23.2 years and 121 patients (64.7%) were male. Mean ICU and hospital LOS was 4.0 ± 4.9 and 10.0 ± 8.1 days, respectively. ISS was higher in patients with an infection (10.6 ± 3.7 vs. 9.5 ± 2.8; p = 0.03), but not clinically significant. Infections were recorded in 43 patients (23.0%) and SSI's specifically documented in 16 (8.6%). Open fractures were not associated with SSI (50% vs. 51.2%; p = 0.9). By univariate analysis there was no difference in admission BG or HGI and infection. However, there was a significant difference in HGI when considering SSI alone (2.1 ± 1.7 vs. 1.2 ± 1.1; p = 0.003). HGI > 1.72 was associated with SSI's (50% vs. 19.3%, p = 0.005). Patients with an SSI received a greater amount of blood transfusions (14.9 ± 12.1 vs. 4.9 ± 7.6, p < 0.001). No patient was diagnosed with a separate infection (i.e. pneumonia, UTI, bacteremia) prior to SSI. There was no difference in ISS among patients with an SSI (11.1 ± 4.0 vs. 9.6 ± 3.0; p = 0.06). Multivariable regression testing HGI as a continuous variable demonstrated a significant relationship (OR: 1.8, 95% CI: 1.2-2.6) with SSI after adjusting for blood transfusions (OR: 1.1, 95% CI: 1.1-1.2).
Conclusion: Stress-induced hyperglycemia is a common event and a significant risk factor for SSI's in non-diabetic orthopaedic trauma patients. Blood glucose monitoring should be considered in non-diabetic orthopaedic trauma patients; however, indications and implications for tight glycemic control in these patients cannot be determined from this study.
KimMosesMDChristleyScottPhDLiuDonaldMDAlverdyJohnMDAnGaryMD
University of Illinois at Chicago, University of Chicago
Role of Feeding-Induced Oxidative Stress and TLR-Response on Cellular Population Dynamics in the Pathogenesis of Necrotizing Enterocolitis: Insights from an Agent-Based Model
Background: Necrotizing enterocolitis (NEC) is a leading gastrointestinal cause of death in neonates. Risk factors include: prematurity, initiation of enteral feeding, oxidative stress and bacterial effects. We propose that the initial condition in the pathogenesis of NEC is immaturity of the ability of neonatal gut epithelial cells (NGEC) to manage oxidative stress (OS). Reduction in the distribution of OS tolerance across the cellular population is accentuated by enteral feeding, leading to a shift from apoptotic to inflammatory pathways, alterations in gut microenvironment, subsequent bacterial virulence activation, exacerbation of mucosal inflammation, and eventual necrosis. Toll -like receptors (TLRs) play an important role in this process and we propose that danger/pathogen associated molecular pattern molecules (DAMP/PAMPs) acting through TLRs tip the population dynamics of susceptible NGECs to a trajectory towards NEC. The multi-factorial complexity of these interacting processes requires characterization with computational modeling and agent-based modeling has been used to dynamically represent hypotheses in this fashion. We present an agent-based model (ABM) of NGEC to visualize the dynamics of the pathogenesis of NEC.
Methods: An ABM of the neonatal gut was created using NetLogo. Rules for NGEC computational agents, derived from the literature, incorporate pathways for OS, p53, apoptosis, tight junction metabolism, TLR-4, nitric oxide (NO), NF-kB and high mobility group box protein-1 (HMGB-1). Generically modeled bacteria were able to respond to environmental cues, activate virulence, produce PAMPs, adhere to and destroy host cells. Both DAMP/PAMPs could activate TLR-4. Experimental runs included baseline parameter sweeps of OS management capacity, subsequent response to feeding, and alterations in bacterial load and virulence potential.
Results: The ABM reproduced baseline behavior of nutrient uptake and production and clearance of OS. Reductions in either stress detection or clearance produced excess OS, which led to senescence, apoptosis or inflammation depending OS levels. Reduced capacity to manage OS led to increased generation of NO and subsequent disruption of tight junctions. Increased prevalence in the inflammatory phenotype led to a shift in NGEC population dynamics that enhanced bacterial virulence, and generated a forward feedback loop leading to further inflammation and necrosis.
Conclusion: NEC is a complex process of cascading systems failure. Our ABM incorporates known components in the pathogenesis of NEC and demonstrates that decreased capacity to manage OS can lead to the apoptosis and inflammation of individual cells and unstable population dynamics. The ABM demonstrates the importance of DAMP/PAMP/TLR in shifting NGEC population dynamics towards the pathogenic phenotype and further suggests that the pathogenesis of NEC is not necessitated by a particular microbe, but instead by a microbial population with greater virulizing potential in response to microenvironmental cues. By identifying conditions and components that increase the susceptibility of NGECs to NEC we may be able to suggest cellular processes and putative pathways/genes that are impaired in premature infants. This type of dynamic knowledge representation can be integrated into existing research programs and future research endeavors.
ShrumBradMScMeleTinaPhD, MD
University of Western Ontario
The Role of HIF-1 in the Pathogenesis of Liver Injury During Sepsis
Introduction: A well documented observation during severe bacterial infections leading to sepsis is the extensive loss of innate and adaptive immune cells via apoptosis. Interestingly, sepsis is also associated with increased apoptosis of liver cells. Moreover, various strategies used to inhibit apoptosis result in improved hepatic bacterial clearance, a reduction in liver damage and improved survival during sepsis. However, the mechanisms mediating these observations remain unclear. We sought to investigate a potential candidate, Hypoxia-inducible factor-1 (HIF-1), a transcription factor which influences cell survival and apoptosis pathways, during sepsis.
Methods: We created a mouse model of sepsis by injecting a fecal solution into the peritoneal cavity (FIP) of mice. At time points: 0, 3, 6, 12, 18 and 24 hours following FIP or a saline-sham control, mice (n = 4 per group/time point) were euthanized and the livers were harvested for analysis. RNA was extracted from the liver for quantitative reverse-transcriptase PCR (qRT-PCR) to determine expression of HIF-1α, FasL, bcl-2 (anti-apoptotic) and Bax (pro-apoptotic). Liver tissue was also formalin-fixed, paraffin-embedded, and stained with hematoxlyn and eosin to score for inflammation, cellular infiltrate and necrosis. Tissue sections also underwent TUNEL staining to detect apoptosis.
Results: Mice treated with FIP had a median mortality rate of 75% at 24 hours and significant liver injury compared to the sham controls. Using qRT-PCR, we were determined that liver HIF-1α (the regulatory subunit of HIF-1) gene expression was significantly increased over time when compared to sham-control mice (Figure 1). In situ TUNEL staining for apoptotic cells, demonstrated increased apoptotic cells within the liver of the FIP treated mice. To further characterize this apoptosis, we measured FasL, Bcl-2 and Bax gene expression in the liver. In the FIP mice, FasL gene expression increased over time and Bcl-2/Bax ratios decreased compared to the sham control mice confirming the TUNEL data and a state of increased apoptosis in the liver after induction of sepsis using FIP.
Conclusion: In sepsis, HIF-1α gene expression increased over time and was significantly increased compared with sham controls. The increased HIF-1α expression in the sepsis mice was paralleled by increased liver damage, increased number of apoptotic cells and increased pro-apoptotic gene expression compared to sham controls. In summary, during polymicrobial sepsis, HIF-1α expression in the liver is increased over time and is associated with increased levels of apoptosis of cells within the liver.
AkinbamiFelixMBBS, MSSteinbergJillRN, MPHPanizalesMariaRN, MSNRogersSelwyn OJr, MD, MPHAskariRezaMD
Department of Surgery and Center for Surgery and Public Health, Brigham and Womens Hospital, Boston, MA
Initiations of Quality Improvement Measures can Lead to Decreasing Infectious Complications in Emergency Surgical Patients
Introduction: Over the past decade, there has been a significant focus on reducing postoperative infections at both the national and hospital level. Despite focus on quality improvement in surgery, studies continue to show that emergency status contributes significantly to increased infectious complications and mortality of general surgery operations. We looked to see if the initiation of national and hospital wide quality measures at reducing infectious complications at our institution over the past several years have led to decreased morbidity and mortality in emergency general surgery (EGS) patients.
Background: Since 2007 several national and hospital wide quality and infection control initiative have been initiated at our institution. Some of these include, increasing compliance with The Surgical Care Improvement Program (SCIP), Implementation of Ventilator Associated Pneumonia (VAP) Bundle and urinary catheter guidelines.
Methods: We conducted a retrospective study of all American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) EGS operations performed at our tertiary medical center from 1/1/2002-12/31/2009. We compared the EGS operations performed between 2002–2006 (Group 1) to those of 2007–2009 (Group 2).
Results: Overall there has been a trend towards lower infection rates and mortality in the recent years. There has been a significant reduction in the total infection rate in the recent year (25.7% vs. 13%). In particular, there has been a significant reduction in rates of sepsis, septic shock, pneumonia, and UTI (Table 1).
Conclusion: Initiation of several national and hospital wide quality and infection control initiatives at our institution over the past several years have led to decreasing rates of sepsis, septic shock, pneumonia and UTI in our emergency surgical patients. There is also an overall downward trend in SSI rates and mortality.
ContiDavid JGallichioMichael HChandoliasNicholasSiparskyNicole
Albany Medical College
Monthly PCR Screening for Polyoma BK Virus with Pre-Emptive Immunosuppressive Therapy Reduction:Long-Term Results after Renal Transplantation
Background: BK nephropathy (BKN) is a serious complication after renal transplantation. In Jan. 2006, we initiated monthly serum BK PCR screening. Patients detected to have BK viremia underwent an immediate reduction in immunosuppression consisting of a discontinuation or 50% dose reduction of cellcept (CC). Serum PCR was repeated monthly and any recipient experiencing graft dysfunction underwent transplant biopsy.
Methods: Between 1/1/06 and 12/31/08, 174 renal transplants were performed at our center. Immunotherapy consisted of tacrolimus, CC and either sirolimus or prednisone. PCR became positive for BK in 29 (17%) patients (Group A). Mean time to positive PCR post-transplant was 6 months. Following CC dose reduction, 27/29 group A patients became negative for BK detection by PCR The mean time to a negative PCR was 4 months. Transplant dysfunction subsequently developed in only one Group A patient (3%), 4 months after discontinuation of CC therapy. Transplant biopsy in this case showed acute rejection and the graft eventually failed at 37 months due to chronic nephropathy. No group A patient developed BKN. Long-term outcomes in Group A patients, mean follow-up of 42 months, were compared to that of 29 concurrent matched renal transplant recipients who never developed BK viremia and thus never underwent a reduction in immunosuppression, (GroupB)
Results: Demographics were similar between the groups with respect to: age, gender, ethnicity, donor type, retransplant status, and follow-up. Long-term survival rates and renal function were similar between Group A and B patients as shown in the table below.
GROUP A
GROUP B
Pt.surv. (%)
100
97
Gft surv. (%)
96
93
Creat. mg/dl
1-year
1.4
1.6
2-yrs
1.4
1.6
3-yrs
1.6
1.6
4-yrs
1.5
1.5
Conclusion: Monthly screening for BK virus by PCR for early detection, with associated pre-emptive immunosuppressive therapy reduction, effectively prevents BKN. In addition, this screening protocol is associated with a low rate of acute rejection and preservation of excellent long-term renal function.
CampbellKristin TurzaMDAgarwalAvinashMDShafiqueMichaelBSBraymanKenneth L.MD, PhDSawyerRobert G.MD
University of Virginia
Infectious Outcomes in Living Donor Kidney Transplant Recipients following Multimodal Preoperative Desensitization to Overcome Humoral Barriers
Introduction: Preexisting humoral barriers significantly challenge transplantation of living donor kidneys (LDK) into highly sensitized ABO and HLA incompatible recipients. Aggressive conditioning of recipients' immune systems is required pre-transplantation. We hypothesized that pre-conditioning would result in higher infection rates post-transplant.
Methods: A matched case-control design was utilized to compare desensitized patients (DS) to non-desensitized (NDS) living donor kidney transplant recipients. Each desensitized patient was hand -matched with 2 or 3 non-desensitized patients. Patients were matched closely for cause of end stage renal disease (ESRD) by general categories (congenital, immune-related, diabetes mellitus (DM) type 1, DM type 2, hypertension) and age. Desensitization included Rituximab (anti-B cell antibody) and mycophenolate mofetil 6 to 8 weeks preoperatively followed by intravenous immunoglobulin (IVIG) and plasmapharesis 2 week preoperatively. Both desensitized and non-desensitized patients received induction therapy (rabbit anti-human thymocyte globulin) followed by maintenance immunosuppression (tacrolimus, mycophenolate mofetil, and prednisone). Primary outcomes included infections (opportunistic, local, systemic) within 12 months of transplant, while secondary outcomes included patient and graft survival, and acute rejection. Univariate and log-rank statistical analysis was completed.
Results: Twenty-five highly sensitized recipients underwent desensitization and LDK transplantation. Mean age for DS patients was 42.3 ± 18.4 years versus 40.8 ± 18.7 years in NDS patients (p = 0.7). Eighty eight percent (22/25) of DS patient matches were similar for diagnosis and 19/25 (76%) were within 5 years of the age of the controls. Patient survival was 100%. Graft survival was 96% in both groups (24/25 and 51/53). Average follow-up was 36.5 ± 14.7 months (desensitized) versus 25.5 ± 17.5 months (non-desensitized). Mean 3-month and 12 month creatinine was 1.16 ± 0.2 mg/dL and 1.2 ± 0.3 mg/dL in DS versus 1.3 ± 0.4 mg/dL and 1.4 ± 0.5 mg/dL in NDS patients. Thirty six percent of desensitized patients had one or more infections versus 28% in non-desensitized (p = 0.6). The average number of infections per infected patient was 1.6 (DS) versus 1.4 (NDS). No difference was observed in opportunistic infections (pathogens unlikely to cause infection in immune-competent hosts, viruses) between DS (16%) and NDS patients (13%, p = 0.7). The number of total local infections (single organ) was significantly greater in DS patients (56% vs. 30%, p = 0.04). No difference was found in number of systemic infections (disseminated) (p = 0.4).
Conclusion: Preoperative desensitization in highly sensitized living donor kidney transplant recipients is associated with a similar number of opportunistic and systemic infections compared to NDS patients. Total number of local infections was significantly greater in the desensitized, however. With careful monitoring for infectious complications, preoperative desensitization is a valuable tool enabling highly sensitized patients to be transplanted. Future studies are required to evaluate these observed outcomes.
BecherRobert D.MDHothJ. JASONMD, PhDKendallJennifer L.BAReboJerry J.PharmDMillerPreston R.MD
Department of General Surgery, Wake Forest University School of Medicine
Comparing A Locally-Derived Versus Guideline-Based Approach to Treatment of Hospital Acquired Pneumonia in the Trauma Intensive Care Unit
Background: Multidrug resistant (MDR) respiratory pathogens are an increasingly difficult problem in critically ill patients with pneumonia. MDR organisms restrict antibiotic treatment options, and are associated with poorer outcomes. This makes the selection of appropriate initial antibiotics for empiric coverage of pneumonia difficult. Given the high frequency of MDR pathogens in our surgical intensive care unit (SICU) of over 50%, we sought to compare differences in the antibiotic sensitivity profiles and the microbiology of early versus late pathogens, and determine the best empiric approach to initial antibiotic coverage in the SICU.
Methods: Retrospective analysis of continuous patients admitted to the SICU at a tertiary medical center over a one and a half year period with a diagnosis of first hospital-acquired (HAP) and ventilator-associated (VAP) pneumonia. Local microbiology and sensitivity profiles were analyzed. Risk factors for MDR pathogens were based on American Thoracic Society (ATS) guidelines, which define patients at risk based on time since admission (early being <5 days; late being ≥5 days) and other standardized criteria.
Results: A total of 64 first pneumonias were caused by 90 pathogens over the 1.5 year period. There were 25 (28%) early pathogens and 65 (82%) late. 24 of 25 (96%) early HAP/VAP pathogens fulfilled MDR risk criteria; 10 (40%) were true MDR organisms. Of the 24 early at risk patients, ATS guidelines recommend broad spectrum therapy; in our cohort, susceptibility varied: 72% with ceftriaxone/vancomycin (cftri/vanc), 92% with ciprofloxacin/vancomycin (cipro/vanc), 99% with cefepime/vancomycin (cefe/vanc), and 96% with piperacillin-tazobactam/vancomycin (p-t/vanc). Examining late HAP/VAP, there were 35 (54%) MDR organisms. ATS recommends broad-spectrum empiric coverage for all late HAP/VAP; susceptibilities were much poorer: 58% with cftri/vanc, 71% with cipro/vanc, 74% with cefe/vanc, and 71% with p-t/vanc. Addition of carbepenems or aminoglycosides to these late regimens failed to improve adequate coverage above 78%.
Conclusions: Late HAP/VAP is significantly more difficult to empirically treat compared to early pneumonia in the SICU, with the best available coverage only reaching no greater than 78%. This is concerning, as over 80% of SICU HAP/VAP occurs on day 5 or later, with 54% MDR organisms. We were unable to identify any single additional antimicrobial that significantly improves this coverage. Guideline driven treatment of SICU patients with early pneumonia yielded excellent coverage of >90%.
CuencaAlex GMDWynnJames LMDKelly-ScumpiaKindraPhDScumpiaPhillip OMD, PhDNacionalesDina CMDEfronPhilip AMDMoldawerLyle LPhD
University of Florida
TLR4 Protective Adjuvant Effect to Murine Polymicrobial Sepsis is Trif, but not MYD88, Dependent
Introduction: We have previously shown that pretreatment of murine neonates with toll-like receptor (TLR) 4 ligand, lipopolysaccharide (LPS), is able to significantly improve survival to polymicrobial sepsis. Although this effect was associated with increased activation/recruitment of innate immune effector cells, the mechanism is unknown. As TLR4 utilizes both TLR adaptor proteins, MyD88 and TRIF, and MyD88 but not TRIF has been linked to survival to polymicrobial sepsis in adult studies, we hypothesized that MyD88 signaling is critical for the observed TLR4 agonist protective adjuvant effect to neonatal sepsis.
Methods: Splenocytes from C57BL/6J (wild-type, WT), MyD88-/-, and TRIF-/- 5–7 days old were harvested and either stimulated via PMA to assay for neutrophil reactive oxygen species (ROS) production or stimulated in vitro with LPS for 24 hours and subsequently assayed for neutrophil phagocytic ability. For survival studies, WT, MyD88-/-, and TRIF-/- were pretreated with LPS (1 μg/g body weight) intraperitoneally (ip) followed by challenge with a cecal slurry ip 24 hours later. Mice were followed for survival for 7 days. A second cohort of neonates were euthanized at 0, 4, and 24 hours post LPS and assayed for serum concentrations of inflammatory and anti-inflammatory cyto/chemokines via Luminex assay.
Results: Surprisingly, though no differences in PMA elicited neutrophil ROS production or burst kinetics were noted between any of the groups, TRIF-/- neonates had significantly fewer phagocytic neutrophils compared to WT or MyD88-/- animals following LPS stimulation (71% vs 92% or 87%, respectively; p < 0.002). Similarly, in contrast to WT or MyD88-/- neonates, TRIF-/- neonates were not protected against polymicrobial sepsis following TLR4 adjuvant administration. This was associated with significantly lower serum concentrations of several cyto/chemokines in TRIF-/- neonates compared to WT neonates following LPS administration, including IL-1β, IFN-γ, TNF-α, and CXCL10.
Conclusion: These data provide a novel role for TRIF but not MyD88 signaling in both neonatal neutrophil phagocytic function following LPS stimulation and TLR4 adjuvant induced protection to polymicrobial neonatal sepsis.
EirefSimon D.MDGoldsteinRobert C.MDLeitmanI. MichaelMDRileyWilliam H.PhD
Albert Einstein College of Medicine - Beth Israel Medical Center, New York, NY
Hand Sanitizer Dispensers and Associated Hospital Acquired Infections - Friend or Fomite?
Introduction: Hand hygiene is the key weapon in preventing hospital-acquired infection (HAI). Waterless alcohol-based hand sanitizers are an increasingly popular method of hand hygiene. Hand sanitizer dispensers (HSD) have become ubiquitous in the hospital. Whether HSD may themselves harbor pathogens or act as potential fomites hasn't been previously reported. The goal of this study was to determine if HSD could become contaminated with pathogens that cause HAI.
Methods: The study took place in the SICU of an urban teaching hospital. The wall-mounted manual HSD (Purell FMX-12 Dispenser, Johnson & Johnson, New Brunswick, NJ) were located in the individual patient bays and in a centralized charting area. The dispensers delivered an alcohol solution containing 62% ethyl alcohol (Purell Instant Hand Sanitizer Foam, Johnson & Johnson, New Brunswick, NJ). Sterile cotton tipped swabs pre-moistened with sterile saline were used to sample three surfaces of each HSD unit: the dispenser's lever, the rear portion adjacent to the wall, and the area surrounding the dispensing nozzle. The swabs were subsequently cultured to trypticase soy blood agar (BBL, Becton Dickinson, Sparks, MD). All cultures were incubated at 35°C for 24 to 72 hours with observations at 24 hour intervals. At each observation, bacterial morphotypes were semi-quantified and presumptively identified using the Gram stain and select screening methods. Isolates determined to be of particular interest were identified using Vitek 2 (bioMerieux, St. Louis, MO). Methicillin resistance for the Staphylococcus aureus isolates was determined from a cefoxitin disk using the Kirby Bauer disk diffusion method
Results: All 17 HSD cultured positive for one or more bacterial species. Distribution of contamination included the lever in 82%, wall in 35%, and nozzle in 23% HSD. Multiple bacteria were obtained in 50% of contaminated sites. Growth ranged from 1 to 50 colonies, with a median of 5 and mean of 8.3. Gram-positive cocci predominated, with the majority being coagulase negative staphylococci in 16 (94%) HSD. Methicillin- sensitive S. aureus and Micrococcus grew from 2 (12%) and 1 (6%) HSD respectively. Gram-positive bacilli, including Bacillus species, diphtheroids, and aerobic actinomycetes, were together isolated from 6 (35%) HSD. Gram-negative bacilli, including non-lactose fermenting nonenterics and lactose-fermenting enterics, were together isolated from 5 (29%) HSD.
Discussion: This study showed that 100% of waterless alcohol-based HSD from a SICU were contaminated with bacteria. Colonization was greatest on the lever, likely due to direct hand contact. These bacteria were largely commensal skin flora, gram-positive cocci and gram-positive bacilli. In addition, 24% of HSD grew lactose-fermenting enterics, which may develop drug resistance and are major pathogens of HAI. The passage of pathogens from HSD to health care workers' hands could result in subsequent HAI if proper hand hygiene is ignored. The spread of these pathogens can be decreased by routine cleaning of HSD, correct sanitizer application, and use of gloves prior to patient contact.
PriceConnie SavorMDKnepperBryanMSDurfeeM. JoshMSYoungHeatherMDBifflWalter LMD
Denver Health and University of Colorado Denver
Performance of Two Surgical Site Infection Risk Stratification Models for Predicting Infection Risk in Publicly Reported Data from a Safety Net Hospital
Introduction: Since 2007, the Colorado Hospital-Acquired Infections Disclosure Act has required hospitals and ambulatory surgery centers to report selected surgical site infections (SSI) to the CDC's National Healthcare Surveillance Network (NHSN) to be analyzed and risk adjusted. The Colorado Department of Public Health and Environment uses that information to issue comparisons of facility-specific, risk-stratified infection rates to the public.
Background:. In order to provide reliable information to the public, risk adjustment models must be reliable for accurately comparing a facility's performance against that of other procedures with similar risk. However, risk adjustment models currently used for public reporting have not been widely validated. We sought to verify the NHSN basic risk index and standardized infection ratio (SIR) for their abilities to predict SSI in publicly reported herniorrhaphy, hysterectomy, and arthroplasty procedures from an academic public health safety net institution in Denver, CO.
Methods: Cases of arthroplasty (hip and knee) between January 2007 and October 2010; herniorrhaphy and hysterectomy (vaginal and abdominal) between January 2009 and October 2010 were entered into NHSN as mandated by State law. These were retrieved from the NHSN system database and duplicate patients were excluded. Cases were defined as SSI according to the NHSN definitions. The NHSN basic risk index and SIR was calculated for each procedure based on the following variables: wound class, age, anesthesia, ASA, duration of surgery, arthroplasty type, hospital beds, trauma, endoscope, and gender. Association between NHSN basic risk index and SSI were identified using the Cochran-Mantel-Haenszel test for categorical variables. Association between NHSN SIR and SSI were identified using the Wilcoxon two-sample test for continuous variables.
Results: A total of 1337 publicly reported cases were included (488 arthroplasty; 616 herniorrhaphy; 233 hysterectomy), of which 31 were defined as SSI (13 arthroplasty; 8 herniorrhaphy; 10 hysterectomy). The NHSN basic risk index did not correlate with SSI when assessed in aggregate (p = 0.19), after arthroplasty (p = 0.66), or after hysterectomy (p = 0.74); only SSI after herniorrhaphy showed a correlation with the basic risk index (p = 0.02). In contrast, the SIR correlated with SSI when assessed in aggregate (p < 0.001) and after herniorrhaphy (p = 0.001) and hysterectomy (p = 0.03); SIR did not correlate with SSI after arthroplasty (p = 0.09).
Conclusion: Neither basic risk index nor SIR currently used for risk stratification in publicly reported procedures in CO adequately predicted SSI at this institution. SIR predicted infection risk better than the basic risk index for the procedures that we examined. The SIR uses logistic regression modeling and takes into account more variables and procedure-specific risk factors. We hypothesize that improved risk adjustment is due to consideration of these extra risk factors. Given its inferior risk stratification performance, the basic risk index should no longer be used when analyzing SSI data for public reporting. Although superior, the SIR still is not broadly applicable to all procedures and settings, and further refinement is needed before it can be promoted as a tool to compare risk stratified rates of SSI from arthroplasty procedures at safety net institutions.
The Effect of Prolonged Cortisol Excess on Systemic and Cellular Responses to Endotoxin
Introduction: Prolonged illnesses are often associated with persistent cortisol levels. Thus, the aim of the current study was to create a model of chronic stress through prolonged cortisol infusion. Using this model, we sought to determine how persistent endocrine stress will impact the host inflammatory response to an acute inflammatory challenge induced by in vivo endotoxin (LPS) administration. We hypothesized that an extended period of prior cortisol excess would modulate both systemic and cellular markers of the host inflammatory response.
Methods: Healthy volunteers were randomized to receive either cortisol (3μg/kg/mim) (n = 3) or saline (n = 4) infusion for 24 h prior to receiving a bolus dose of LPS (1 ng/kg, CC-RE, Lot #2). Heart rate variability (HRV) data, vital signs, and blood samples were obtained at multiple time points before and after LPS infusion. HRV metrics were serially determined with standard technologies (CardioPro). We determined peripheral blood leukocytes' (PBL) energy levels (ATP) using lysed cells. Statistical analysis was by repeated measures ANOVA.
Results: Prior to endotoxin challenge, subjects receiving cortisol exhibited diminished nocturnal variability (p < 0.05) of an HRV metric of overall host adaptability, SDNN (standard deviation of normal-to-normal intervals), without an apparent influence on efferent vagal activity, RMSSD (square root of the mean squared differences of successive normal-to-normal intervals). No changes in cellular bioenergetics were observed in subjects infused with cortisol alone for 24 hours. Following endotoxin challenge, sustained prior cortisol infusion significantly attenuated the endotoxin-induced decrease of SDNN (p < 0.05) and RMSSD (p < 0.02). In vivo endotoxin elicited a transient decrease in ATP levels and a parallel transient increase in autophagy. These perturbations were not observed in PBL from subjects infused with cortisol prior to in vivo endotoxin challenge.
Conclusion: Despite similar systemic manifestations in vital signs exhibited by both groups following endotoxin, cortisol did attenuate the endotoxin-induced dysregulation of autonomic function. In addition, a prolonged period of hyper-cortisolemia appeared to influence the normal circadian cycling of some HRV parameters. The effect of an antecedent cortisol infusion on cellular bioenergetics was profound, in that it prevented the endotoxin-induced decline in ATP levels, as well as the induction of autophagy in PBL. It remains to be determined whether the net effect of the metabolic responses is protective or detrimental to the host.
BIhoracAzraMDEfronPhilip AMDAngDarwinMD, PhDMaierRonald VMDMoldawerLyle LPhD
University of Florida
Acute Kidney Injury is Associated with Nosocomial Infections and Surgical Site Infections after Trauma
Background: Infections and sepsis are important determinants of mortality in patients with trauma. Mild and moderate acute kidney injury (AKI) occurs in 26% of trauma patients and is associated with increased mortality. We studied the effect of posttraumatic AKI on the occurrence of infectious complications after trauma.
Methods: We performed a secondary analysis of the “Inflammation and the Host Response to Injury” (GlueGrant) database to include adult blunt trauma patients without history of kidney disease. AKI was defined by the RIFLE (Risk, Injury, Failure, Loss, and End-stage Kidney) classification, which requires a 50% increase in sCr and stratifies patients into three severity stages: risk, injury, and failure. Association between all stages of AKI and infectious complications was analyzed using a multivariable logistic regression analysis.
Results: The prevalence of surgical site infection (SSI) and nosocomial infections (NCI) after trauma was 16% and 49%, respectively. Patients with AKI had 2.3 times the odds of having SSI and 2.0 times the odds of having NCI compared to patients without AKI. Among NCI, the odds for pneumonia (1.96), bloodstream infections (3.07) and intravenous catheter-related infections (2.45) were higher for AKI patients. Multivariate logistic analysis revealed that male sex, AKI, hyperglycemia and transfusion of > 6 units of packed red blood cells (PRBC) in the first 24 hours were independently associated with the occurrence of NCI (c statistic 0.612). On the other hand, AKI and transfusion of > 6 units PRBC and African American ethnicity were associated with SSI (c statistic 0.628).
Conclusion: Post-traumatic AKI is an independent risk factor for infectious complications after trauma.
Poster Presentation Abstracts
RankDouglas RMDFriedlandH DAVIDMD, MBABaculikTanyaMDSmithAlexanderMSThyeDirkMD
Cerexa, Inc.
Integrated Safety Summary of Ceftaroline Fosamil: Overall and for Patients with Complicated Skin and Skin Structure Infection (CSSSI)
Introduction: Ceftaroline fosamil (CPT) is a broad-spectrum, parenteral cephalosporin prodrug approved for treatment of acute bacterial skin and skin structure infections (ABSSSI) and moderate to severe community-acquired bacterial pneumonia (CABP). We report an integrated safety summary of 4 CPT phase III trials, with a separate safety analysis of the 2 CANVAS studies.
Methods: In the phase III CANVAS and FOCUS trials, adult patients with complicated skin and skin structure infections and community acquired pneumonia, respectively, were randomized (1:1) to receive either 600 mg CPT q12h or 1 g vancomycin plus 1 g aztreonam (V/A) q12h × 5–14 days (CANVAS) or ceftriaxone 1 g q24h × 5–7 days (FOCUS, plus clarithromycin 500 mg q12h × 1 day in one trial). Treatment-emergent adverse events (TEAEs) occurring from first dose until the test-of-cure visit and serious adverse events (SAEs) occurring up to the late follow-up visit or within 30 days after the last dose were recorded. Laboratory tests were evaluated.
Results: The mean ± SD durations of treatment in the CANVAS trials were 8.4 ± 3.1 days (CPT) and 8.4 ± 3.3 days (V/A). Incidences of TEAEs in CANVAS 1 and 2 combined were similar to those observed in the integrated analysis (Table). Common TEAEs were similar between the CANVAS trials and integrated analysis, except for higher incidences of pruritis, pruritis generalized, and rash in both treatment groups of the CANVAS trials. The majority of TEAEs in both CPT and V/A groups were mild or moderate, and unrelated to study drug. There were no clinically meaningful differences in laboratory test results between the CANVAS trials and the integrated analysis or treatment groups, except for higher incidence of direct Coombs' seroconversion in the CPT group. There was no clinical evidence of hemolysis in any treatment group. SAEs and deaths were lower in the CANVAS trials. In the FOCUS trials, 1 death in each group was possibly related to study drug. No deaths in CANVAS were related to study drug.
All 4 phase III trials
CANVAS trials
Incidences, n (%)
CPT (n = 1305)
Pooled (n = 1301)
CPT (n = 692)
V/A (n = 686)
All TEAEs
597 (45.7)
607 (46.7)
309(44.7)
326 (47.5)
Diarrhea
60 (4.6)
42 (3.2)
34 (4.9)
26 (3.8)
Headache
57 (4.4)
40 (3.1)
36 (5.2)
31 (4.5)
Nausea
55 (4.2)
49 (3.8)
41 (5.9)
35 (5.1)
Insomnia
36 (2.8)
31 (2.4)
17 (2.5)
17 (2.5)
Constipation
27 (2.1)
24 (1.8)
18 (2.6)
18 (2.6)
Vomiting
27 (2.1)
20 (1.5)
20 (2.9)
18 (2.6)
Pruritus
25 (1.9)
59 (4.5)
24 (3.5)
56 (8.2)
Hypokalemia
24 (1.8)
30 (2.3)
10 (1.4)
15 (2.2)
Rash
24 (1.8)
19 (1.5)
22 (3.2)
17 (2.5)
Hypertension
23 (1.8)
26 (2.0)
9 (1.3)
10 (1.5)
Phlebitis
20 (1.5)
18 (1.4)
3 (0.4)
5 (0.7)
Dizziness
17 (1.3)
10 (0.8)
14 (2.0)
8 (1.2)
Pruritus generalized
15 (1.1)
19 (1.5)
15 (2.2)
19 (2.8)
SAEs
99 (7.6)
100 (7.7)
30 (4.3)
28 (4.1)
D/C
48 (3.7)
58 (4.5)
21 (3.0)
33 (4.8)
Deaths
18 (1.4)
12 (0.9)
3 (0.4)
0
D/C = discontinuation of study/study drug due to a TEAE.
Conclusion: This integrated safety summary of phase III clinical trial data indicates that CPT is well tolerated with a safety profile similar to other cephalosporins.
CarlisleErica M.MDZaborinaOlgaPhDLiuDonaldMD, PhDAlverdyJohnMD
University of Chicago Medical Center
A Novel Model to Study the Combined Effects of Microbes and Oxidants on the Development of Necrotizing Enterocolitis
Introduction: Necrotizing enterocolitis (NEC) affects 5–10% of preterm infants born weighing less than 1500 g and occasionally critically ill adults. Although NEC pathogenesis is multi-factorial there appears to be a correlation between oxidative stress and the development of NEC that involves bacteria and their exoproducts. While traditional animal models of NEC can create histologic mucosal necrosis that appears to mimic “pre-NEC,” it is rare to see full thickness transmural necrosis in animals as seen intra-operatively in humans. Here we describe a new model of full thickness intestinal necrosis following intraluminal administration of the endogenous oxidant monochloramine into isolated loops of mouse intestine. The aim of this study was to determine what role, if any bacteria have in this model.
Methods: 3wk old C57/Bl6 mice underwent creation of an intestinal loop via suture to isolate a 4 cm segment of ileum while preserving its blood supply. 200μl of the monocholoramine derivative Chloramine T (0.5% v/w) or 200μl of normal saline was injected into the loop. To expose mice to pathogens that might colonize premature babies, separated groups of mice underwent the loop prep followed by simultaneous intracecal injection of 100μl of Pseudomonas aeruginosa or 100μl of normal saline as a control. The isolated intestine was returned to the abdominal cavity and the incision closed. Mice were sacrificed 24 h later, the degree of necrosis assessed and then intestinal segments were harvested and analyzed histologically and microbiologically.
Results: The majority of mice survived to the time of sacrifice (saline 78%; 63% chloramine). Of animals that survived to 24 h, no gross necrosis was observed in the saline group, but 59% of animals in the Chloramine T group had gross, transmural necrosis (p < 0.001). Relative bacterial species abundance was calculated for the following groups: non-instrumented controls, saline injected isolated loops, Chloramine injected loops WITHOUT necrosis, and Chloramine injected loops WITH necrosis (Figure 1). Lactobacillus was present in 60% of non-instrumented controls but completely absent in all animals who underwent isolated loop construction. Methicillin-sensitive Staphylococcus aureus, Pseudomonas aeruginosa, and Enterococcus faecium were present only in animals that underwent isolated loop construction. Groups of animals that underwent cecal injection of P. aeruginosa following loop construction cultured positive for P. aeruginosa in the isolated loop despite suture ligation of proximal and distal loop ends suggesting endogenous homing of P. aeruginosa to the isolated loop.
Conclusion: Intraluminal chloramine causes full thickness intestinal necrosis in 3wk old mice. Surgical injury results in loss of protective lactobacillus species. Although bacterial quantity and species were not determinants of the development of necrosis, this model will allow for more in-depth metagenomic interrogation of host pathogen signaling within a confined space that consistently produces transmural necrosis similar to that observed during the human condition.
SternJordan RMDOlivasAndrea DMDValuckaiteVestaMDChristleyScottPhDZaborinaOlgaPhDAlverdyJohn CMDAnGaryMD
The University of Chicago Medical Center
Discovery of Mechanistic Interactions between Pseudomonas Aeruginosa and Wounded Epithelial Cells with an Agent-Based Model: Implications for the Pathogenesis of Anastomotic Leaks
Introduction: Despite extensive investigation and implemented interventions, intestinal anastomotic leaks remain a significant source of surgical morbidity. While not falling under the classical definition of “infection,” a complex, dynamic interplay between microbial and host factors affects healing. In particular, Pseudomonas aeruginosa is known to activate virulence factors in response to host damage and has been associated with anastomotic failure. Epithelial re-apposition at the suture line is an important step in anastomotic healing, and specific interactions at the anastomotic site, including spatial and temporal dynamics of bacterial phenotype transformation, need to be accounted for in order to properly understand the mechanisms involved in bacteria-influenced anastomotic disruption. Dynamic knowledge representation with agent-based modeling can be used to integrate and concatenate mechanistic knowledge for the generation of novel hypotheses. We used an agent-based model (ABM) of the interactions between wounded epithelial cells and P. aeruginosa to identify several putative binding sites for P. aeruginosa and the effects of their binding on downstream signaling pathways for epithelial cell migration.
Methods: An ABM of epithelial wound healing was constructed using NetLogo. Computational agents representing individual epithelial cells (IECs) and P. aeruginosa bacteria were implemented in an in-silico analog of an in-vitro epithelial scratch assay model. IEC rules incorporated known pathways for the epidermal growth factor receptor (EGFR), transforming growth factor beta (TGF-b), integrins and laminins. P. aeruginosa agents incorporated mechanisms for virulence activation, and response to reactive oxygen species (ROS) and adenosine. We hypothesized and then simulated putative binding sites between activated P. aeruginosa and integrins and laminins on the IECs, and the effect of that binding on pathways involved in IEC spreading. Patterns of normal and bacterially impaired wound healing were simulated in the presence and absence of radiation, and validated compared to in-vitro data.
Results: The ABM accurately reproduced epithelial wound healing dynamics in both baseline and radiation-treated conditions. Patterns of bacterial adherence were validated against results from in-vitro studies. Activation of P. aeruginosa by ROS and adenosine generated by wounded IECs led to increased bacterial adherence to those IECs having disrupted tight junctions. Specifically, we identified integrins α3β1 and α4β6 and laminin-332 as putative bacterial binding sites that interfered with lamellipodia protrusion and IEC spreading. Simulations of these effects resulted in decreased rates of wound apposition that corresponded to that seen in in-vitro experiments.
Conclusions: Dynamic knowledge representation with agent-based modeling can be used for visualizing and integrating known data to facilitate hypothesis generation and evaluation. Herein, an ABM was used to increase the range and resolution of representation of host-pathogen interactions at sites of anastomotic disruption, and by so doing generate novel mechanistic hypotheses to guide further study using traditional laboratory techniques. Investigation into the potential mechanisms of bacterial interference at healing anastomoses could have an impact on anastomotic leak rates in the clinical setting.
BuchananPatrick JBSKimTadMDLottenburgLarryMDEfronPhilipMDAngDarwinMD, PhD, MPH
University of Florida
Necrotizing Soft Tissue Infection Secondary to Candida Albicans in an Immunocompetent Patient
Background: Necrotizing soft tissue infections secondary to a Candidal infection are exceedingly rare with only a handful of case reports published. Patients at increased risk of developing a fungal induced necrotizing fasciitis are those who are immunocompromised, have poorly controlled diabetes, or have peripheral vascular disease. Physical findings of this disease include fever, erythema and necrosis. We present a case of an immunocompetent patient who did not exhibit these risk factors.
Case Presentation: 55 year-old Caucasian male admitted for thoracoabdominal injury secondary to gun shot wounds. Left tube thoracostomy was performed for pneumothorax and a left subclavian 9 French non antibiotic coated introducer was placed. Exploratory laparotomy revealed penetrating injuries to the greater curvature of the stomach, neck of the pancreas, and right kidney. Wedge gastrectomy, distal pancreatectomy, repair of the superior mesenteric artery, splenectomy, and open abdomen vacuum dressing were performed. The abdomen was closed following two second-look laparotomies. Four days following closure, the patient developed significant leukocytosis; peak white blood count of 44. Blood cultures were positive for Candida tropicalis and glabrata; systemic high dose diflucan was administered. The left subclavian central venous line was withdrawn and gross purulence was noted at the insertion site which cultured Candida albicans. The erythema, and induration did not resolve despite antifungal therapy and local drainage (Fig 1). The patient underwent emergent operative exploration for deep space infection of the neck. The neck was widely debrided from the deltoid muscle laterally, pectoralis major inferiorly, sternocleidomastoid muscle superiorly, and sternoclavicular joint medially. Pathologic analysis of debrided tissue revealed acute cellulitis and myositis with numerous fungi identified on a GMS stain. Diflucan was discontinued and anidulafungin 100 mg IV q24 h was started. Subsequent debridements were performed and pathologic analysis of debrided tissue revealed necrotic granulation tissue without fungal organisms. The patient was eventually discharged home with vacuum dressing.
Multiseparated absence of left lower neck and left supraclavicular region.
Discussion: Previous case studies have shown that poorly controlled diabetes is a risk factor in immunocompetent patients for the development of Candidal necrotizing fasciitis. However, this patient did not have diabetes and his blood glucose was well-controlled. The source of Candida was likely secondary to the gastric injury with seeding into the blood stream. He was on postoperative antibiotics and antifungal for 48 hours. This case highlights a new patient scenario for necrotizing fungal infection.
GómezGonzaloMDArroyaveMaría CMDPenagosDiegoMDGarcíaMaría CMDMartínezJuan DMDMatallanaRogelioMDVanegasFelipeMDMendozaMaría CMDDíazSergioMD
CES University, Medellin, Colombia
Video-Assisted Single Port Appendectomy: Zero Surgical Site Infections
Background: In 1980 Kurt Semm reported the first laparoscopic appendectomy in Switzerland. This procedure was performed with 3 entry ports. Since then, minimally invasive surgery has presented constant development. Today, the single port technique is rapidly evolving. Relation between appendectomy and surgical site infection (SSI) is well known in literature. SSI rate is lower than 10% for non-perforated appendicitis, 15–25% when perforated appendix is found and higher than 35% in patients with peritonitis. Laparoscopic approach shows significant reduction in wound infection in several surgical entities. This study presents a series of cases of single port appendectomy (SPA) with no SSI.
Methods: This was a prospective study. We recruited a total of 68 patients undergoing laparoscopic SPA from June to December 2009. Our port is a surgical glove attached to a 360° wound retraction device (Alexis®). All programmed patients with clinical impression of acute appendicitis will have the appendix removed no matter the operative findings; even with macroscopic appendix normality and another confirmed cause of acute abdomen the appendix will be removed per protocol. Exclusion criteria were pregnancy, generalized peritonitis and contraindications for pneumoperitoneum. Patients were given Ampicillin/Sulbactam 3 gr. IV; antibiotic prophylaxis therapy was infused 30 minutes before the procedure. All patients were followed-up at 8th and 30th day after surgery.
Results: A total of 68 patients underwent single port laparoscopic appendectomy (46 female, 22). Mean age was 29.3 years old (range 11–65). Abdominal pain presentation was longer than 13 hours in 62 cases (91%). The procedure was completed through laparoscopy in 66 patients (97%). Conversion cause was generalized peritonitis in both cases. Operative findings reported 26 edematous appendix (38.2%), 25 fibrinopurulent (36.7%), 6 gangrenous (8.8%), 2 perforated (2.9%), 2 generalized peritonitis (2.9%) and 7 did not have appendicitis on intrasurgical impression (10.2%) We identified the cause of abdominal pain in 6 of these 7 normal appendix cases: hemoperitoneum was found in 3 patients, colon adhesions in 1 case, ruptured ovarian follicles and uterine adenomyosis, in one case respectively. Appendix was removed in all patients as considered per protocol. Postsurgical ileus was the only complication found in our series, one case with successful medical treatment. Microscopic analysis reported acute suppurated appendicitis in 64 cases (94.1%) 3 of these cases with associated peritonitis; one case of appendicular gangrene (1.5%) and 3 cases without appendicitis on histopathological analysis (4.4%). Mean operative time was 29.8 minutes (range 11–65). Postoperative length of stay was less than 24 hours (mean 20 hours). Seven cases were ambulatory treated (discharged within 8 hours after procedure). There were no surgical site infections. Follow up was complete in all patients.
Conclusion: Single port laparoscopic appendectomy is feasible and safe with a very low complication rate. The outstanding zero percent infection rates found in our patients should bring the interest of surgeons to this new procedure.
EtkinYanaMDLaiVictoriaMDLindnerJosephPA-CKimPeterMD
Albert Einstein College of Medicine
Negative Value of Imaging in Management of Necrotizing Soft Tissue Infections
Introduction: Severe necrotizing soft tissue infections (NSTI) are uncommon, but overall mortality can approach 80% without timely surgical therapy. The goal of our analysis was to determine the role of imaging in the management of NSTI.
Methods: A retrospective review was performed for patients who underwent excisional debridement or amputation at a large, inner-city hospital between January 2009 and December 2009. Pathology and intra-operative findings confirmed the diagnosis of NSTI. Radiographic imaging that displayed subcutaneous emphysema or fascial thickening was considered positive for NSTI. Outcome was measured by time to surgery and mortality.
Results: Nineteen patients underwent surgery for NSTI. Demographics included: average age 48 (24–83), 63% male and 37% female, 42% Hispanic, 32% African American and 26% Caucasian. Mortality rate was 31%. All patients received plain film imaging, and only 26% were positive for NSTI. Seven patients with negative initial x-rays received a CT scan, which was positive for NSTI in only three patients (43%). Overall imaging was positive in only 42% of patients. The mean time from presentation to surgery in the deceased group was 33 hours (16-78) versus 16 hours (4–35) in the survival group (p = 0.036; C.I.1.3-34.3). Patients with negative imaging had a mean time from presentation to surgery of 30 hours (12–78) and a 45% mortality versus 9 hours (4–16) and 12% mortality in patients with positive imaging (p = .008; C.I.6.3-34.7).
Wound culture results showed no growth in 31.5% of patients, Streptococcus species in 21%, E.coli in 15.7%, Enterococci in 10.5%. MSSA, MRSA, Proteus and Klabsiella were found in 5% of wound cultures each. All patients in the deceased group had positive wound cultures. All patients received antibiotics in Emergency Room. 58% of patients received Zosyn, Vancomycin and Clindamycin. 26% of patients received Vancomycin and Zosyn. Only one patient received inappropriate antibiotics based on culture susceptibility.
Conclusion: Negative imaging for NSTI delayed surgery and was associated with increased mortality. Our findings suggest that imaging for NSTI has low sensitivity and may delay life-saving surgery. Timely surgery has a more significant impact on patient survival then broad spectrum antibiotics for treatment of NSTI.
KitayamaJunichiMDKiguchiTakeyukiMDYamakawaKazumaMDNakamoriYasushiMDFujimiSatoshiMD
Osaka University School of Medicine
EAA Helps to Detect the Cause of ARDS at Bed Side
Introduction: It is known that several serum markers are useful as a prognostic factor in septic patients. Endotoxin Activity Assay (EAA) is a first reported as a method for detecting endotoxin based on the ability of antigen-antibody complex to prime neutrophils and augmented respiratory burst response. Endotoxin assay (EA) levels were expressed in relative units derived from the integral of the basal (no antibody) and stimulated (4600 pg/ml LPS) chemiluminescent response. Several reports have shown that EA levels were significantly increased in septic patients.The most common predisposing causes of ARDS are sepsis, pneumonia and aspiration. The ARDS on the basis of pneumonia include infectious pneumonia with sepsis and noninfectious pneumonia such as interstitial pneumonia and aspiration pneumonitis. Whereas it is clear that the treatment for ARDS caused by infectious pneumonia with sepsis is the administration of the antibiotics, most cases of noninfectious pneumonias seem to respond to the early initiation of systemic corticosteroid.Although it is important to find the cause of ARDS on the basis of pneumonia, there was no report to show that serum biomarkers distinguish between infectious and noninfectious pneumonia.Since radiologic findings in ARDS patients show bilateral parenchymal infiltrates, it is difficult to distinguish the cause of ARDS definitely between infectious and noninfectious pneumonia.
Hypothesis: EAA may be an appropriate method for distinguishing the cause of ARDS between infectious pneumonia with sepsis and noninfectious in serum biomarkers.
Methods: 12 patients, who were fulfilled the diagnostic criteria for ARDS during our ICU stay from Sep.2009 to Aug.2010 and who did not have an organ disorder except for lung, were included. Blood was sampled at the first day fulfilled our criteria for measuring WBC, CRP, Procalcitonin (PCT) and EAA. After the serious search for the cause of ARDS, such as tuberculosis, atypical mycobacteriosis and atypical pneumonia, 6 patients were infectious pneumonia and the other 6 patients were noninfectious. Bacteria were cultured in all 6 patients of infectious pneumonia. There were 4 patients of interstitial pneumonia and 2 patients of chemical pneumonitis by aspiration in noninfectious pneumonia.
Results: There was no significant difference of WBC count, CRP and PCT levels between infectious pneumonia and noninfectious.In contrast, all patients of infectious pneumonia presented > 0.40 unit of EA and all patients of noninfectious presented < 0.40. Infectious pneumonia showed significantly higher levels of EA compared to noninfectious.
Conclusions: EAA may be an appropriate method for distinguishing the cause of ARDS between infectious pneumonia with sepsis and noninfectious at bed side.
infectious pneumonia
noninfectious pneumonia
P value
WBC (103/mm3)
16.2 ± 10.5
18.1 ± 10.0
0.76
CRP (mg/dl)
23.7 ± 15.1
21.0 ± 11.1
0.73
PCT (ng/ml)
19.92 ± 24.48
2.82 ± 4.96
0.12
EAA
0.61 ± 0.15
0.26 ± 0.10
<0.01
PoroykoValeriyPhDCarlisleErica MMDBahroosNeilRodriguezAlexCaplanMichael SMDAlverdyJohn CMDMorowitzMichael JMDLiuDonaldMD, PhD
Department of Surgery, University of Chicago
Gene Expression in the Mice Juvenile Intestine in Response to Milk and Formula Feeding
Introduction: While it is well established that breast fed (BF) compared to formula-fed (FF) pre-term infants have a lower incidence of necrotizing enterocolitis (NEC), the exact mechanism for this is still unknown. One commonly held hypothesis is that BF infants acquire protective features lowering the risk of gut derived lethal sepsis; in contrary, lack of such features predispose FF group to inflammatory complications. The objective of this study is to analyze the transcriptional profile of intestinal tissues to better understand the role of diet in the prevention of lethal gut-derived conditions such as NEC.
Methods: C3HeB/FeJ pups were born vaginally and remained housed with the mother until DOL7. On DOL7 half of each litter was assigned to formula feeding (liquid puppy formula via orogastric catheter 4x/day) (FF) while the remaining pups were allowed exposure to maternal feeding (BF). All pups were euthanized at 72 h, and colonic tissue was collected. The high-quality enriched mRNA was extracted from the animal cecums and cDNA libraries (FF n = 4, BF n = 4) were constructed and sequenced using Solexa sequencing platform. cDNA reads were annotated by BLAST search against mouse RNA database (NCBI build 37), and functionally classified using KOG database (NCBI). The differentially abundant features were identified using Metastats methodology.
Results: Solexa sequencing of 8 cDNA libraries, after quality filtering, resulted in 29,315,823 reads (∼7,300,000 per library) with average read length of 100 bp. Blast search against mouse RNA database yielded total 18,014,657 hits (∼2,251,000 per library) to 19,703 mouse mRNAs. Statistical analysis revealed relative similarity of transcriptional patterns between FF and BF animals. The highly expressed transcripts were similar in both groups (28S ribosomal RNA (LOC236598), 18S ribosomal RNA, leucyl-tRNA synthetase, microRNA 689-2, microRNA mir-2135-3, transmembrane protein 170). Functional annotation also revealed relative similarity of BF and FF animals, no significant differences were detected among general functional categories. Although Metastats identified 149 mRNAs differentially expressed between BF and FF groups; 65 were FF and 84 were BF specific. The prominent feature of FF group, with 25 folds increase, was heme oxygenase (decycling) 1 (Hmox1) (p = 0.006) postulated as a component of cellular defense mechanisms against oxidative stress-mediated injury. Among BF specific transcripts, increased more then two folds, were protein with antimicrobial activity Hmgn2 (p = 0.007), and fibronectin receptor alpha (Itga5) (p = 0.009) involved in macrophage recruitment. Among the other differentially abundant features were the transcription factors, genes involved in vascular development, apoptosis.
Conclusion: This study has evaluated the effect of diet on juvenile intestine. The oxidative stress marker Hmox1 suggests what the FF intestine experiencing ischemic conditions. In contrary BF group may acquire protective antimicrobial properties. Future studies will allow establishing the functional link between the known clinical outcomes associated with milk and formula diets.
BessChristinaBSAllenStevenMDFrankelHeidiMD, FACS
Penn State Hershey College of Medicine
Contact Isolation: The Patient Experience
Introduction: Prevention of healthcare associated infection is a Joint Commission national patient safety goal for 2010. Patients are increasingly placed on contact isolation as the result of more stringent screening for such infectious etiologies as Methicillin Resistant Staphylococcus aureus and Clostridium difficile. Patients' perspectives on contact isolation and its relation to inpatient care was studied to understand areas for future improvement in patient satisfaction, compliance and education related to proper isolation of infection. It was hypothesized that hospitalized patients on contact isolation precautions are less satisfied with their care, feel more isolated from the medical team and feel inadequately educated regarding hospital infectious precautions.
Methods: A survey was mailed to all adult patients (>18yo) admitted to the Emergency General Surgery (EGS) service from December 1, 2009 to November 1, 2010. Those who underwent elective and emergency procedures were included. Demographics between patients not on contact isolation (NC) and the contact isolation (CI) group included age, gender and length of stay. Survey questions focused on patients' overall satisfaction with medical care, feelings of isolation while in the hospital, patient perceptions of the healthcare team's attitude toward infection control and patient understanding and satisfaction with education related to infection control policies and procedures. Surveys were scored from 1 to 5. Higher scores reflect increased patient satisfaction.
Results: Four hundred forty seven surveys were mailed to adult EGS patients (NC patients n = 351 vs. CI patients n = 96) Sixteen percent of the surveys were returned (NC patients = 17% (n = 59) vs. CI patients = 13% (n = 12)). Demographics were similar between the NC and CI groups with the exception of a longer hospital stay in the CI group (CI group: 8.8 ± 10.7 days vs. NC group: 4.3 ± 4.7, P < 0.05). Survey questions focused on four major areas: 1) patients' overall satisfaction with medical care (NC group (avg ± SD) = 4.5 ± 0.3 vs. CI group = 4.1 ± 0.5, P = NS), 2) feelings of isolation from the medical team (NC group = 4.2 ± 0.9 vs. CI group = 4.2 ± 0.5, P = NS), 3) whether the patient felt the medical team took infection control methods seriously (NC group = 4.1 ± 0.8 vs. CI group = 4.5 ± 0.5, P = NS) and 4) if the patient was educated about infection control policies and procedures (NC group = 3.1 ± 0.5 vs. CI group = 3.3 ± 0.7, P = NS).
Conclusion: These preliminary data demonstrate no difference in satisfaction among those on contact isolation for various infectious etiologies compared to the group of patients not on contact isolation with relatively high satisfaction scores in regards to medical care received, a lack of feeling isolated from the medical team and the perception that the medical team took infection control measures seriously. Scores were lower in the area related to patient and family education of the infection control measures utilized at our medical center.
While patients on contact isolation were satisfied with the care they received, this study demonstrates a need for improved education of the patient and their family on the infection control policies and procedures within our institution.
LessingChrisPhDHaymanMelindaPhDMcNultyAmyPhD
Kinetic Concepts, Inc.
Intermittent Exposure to Antimicrobial Solutions Decreases Pseudomonas Aeruginosa Bioburden in an in Vitro Biofilm Model
Background: Wound colonization or infection contributes to wound chronicity by protracting the inflammatory response and consuming local energy resources. Estimates are that at least 60% of all chronic wounds contain bacterial biofilm. As such, therapies aimed at preventing the formation of biofilms or disrupting those already present are drawing more attention. Negative pressure wound therapy with controlled topical instillation (NPWTi) simplifies wound irrigation by allowing automated delivery of irrigation solutions at regular intervals. The objective of this study was to determine the effects of exposure to antimicrobial solutions at regular intervals on Pseudomonas aeruginosa biofilm formation in an in vitro model.
Methods: P. aeruginosa was prepared as a 105 solution in tryptic soy broth. Glass coverslips were dipped into the broth and incubated at 35°C for 4 hours with light agitation to initiate biofilm formation (method characterized by Harrison-Balestra et al., 2003). Following the biofilm initiation period, NPWTi wound irrigation was simulated by removing coverslips from the broth, dipping them in an irrigation solution for 5 minutes, and returning them to the broth; this was repeated every 2.5 hours for 24 hours. Irrigation solutions included normal saline, 5% mafenide acetate, 0.004% sodium hypochlorite with 0.003% hypochlorous acid, and 0.1% polyhexanide. Control coverslips were not removed from the broth during the experiment. After 24 hours, the biofilm was agitated off the coverslips (n = 3 per group) using 2 mL of diluent and plated onto Pseudomonas Isolation Agar for enumeration. Bacterial colony counts (CFU/mL) were analyzed by ANOVA using the general linear model (Minitab, Inc., State College, PA), and means were compared using a Tukey test to assess differences between the treatments. Additional coverslips were stained with Ziehl carbol fuchsin and Congo red for visualization of bacteria and exopolysaccharide (EPS) matrix.
Results: The control group resulted in approximately 108 CFU/mL P. aeruginosa at the end of the testing period, and compared to the control group there was no reduction in bacterial numbers on the coverslips treated with saline. Coverslips treated with 5% mafenide acetate or 0.1% polyhexanide exhibited approximately a 1 log10 reduction in bacterial numbers compared to controls (p < 0.05), while coverslips treated with 0.004% sodium hypochlorite with 0.003% hypochlorous acid exhibited approximately a 2 log10 reduction in bacterial numbers compared to controls (p < 0.05). Additionally, slides treated with antimicrobial solutions visually appeared to have less EPS matrix deposition than control or saline treated slides.
Discussion: NPWTi combines controlled and repeated topical delivery of wound cleansing solutions with the benefits of negative pressure wound therapy, and it has been shown to be effective through removal of wound exudates and infectious material. P. aeruginosa forms biofilm in the wound environment, and the data presented here showed that intermittent exposure to antimicrobial irrigation solutions reduced the number of these biofilm producing bacteria in vitro. These data suggest that NPWTi with antimicrobial solutions may facilitate wound bioburden management.
MigginsMakesha VMDLottenbergLarryMDLiuHuazhiMSMoldawerLyle LPhDEfronPhilip AMDAngDarwin NMD, PhD, MPH
University of Florida
Surgical Site Infection is Associated with Patient Survival at a Hospital Level: Evidence for Systems Based Intervention
Introduction: Surgical site infections (SSI) account for 15% of all hospital acquired infections and are the most common nosocomial infection occurring in surgical patients. Previous studies indicate SSI negatively impacts patient morbidity, mortality, and healthcare costs. These findings have led to the identification of risk factors associated with the development of SSI and research focused on prevention. To date no studies have examined the association between patient survival and SSI. We hypothesized that the development of SSI in trauma patients is related to hospital survivability.
Methods: This is a retrospective cohort study of University Healthsystem Consortium (UHC) academic trauma centers in the United States from 2004- 2009. The UHC is compromised of 90% of non-profit academic medical centers in the US. A subset of the database was used to identify patients at least 18 years of age who developed a SSI during their hospital admission. Hospitals were divided into low survival and high survival cohorts based on the average survival risk ratio (SRR). ICD-9 codes for the twenty-five most commonly preformed surgical procedures were used to compare the frequency of surgical site infections between the two hospital groups. Chi square tests were used to compare proportions. Univariate regression was used to test for association, while multivariate regression was used to match for potential confounding variables. The final RR values were matched and adjusted for age, gender, and insurance status.
Results: A total of 2632 patients were identified representing 111 hospitals. Sociodemographic variables were similar between the two cohorts. The patient population in hospitals with lower survival probability tended to have a higher risk of SSI, with an adjusted and matched RR 1.17 95% CI (1.01, 1.35). Significantly more patients in the low survival group developed SSI after exploratory laparotomy 2% compared to 0% in the high survival group (p-value 0.04). Free skin graft necrosis occurred in 6.4% compared to 2.8% in the high survival group (p-value 0.04). Skin grafting had the highest risk of SSI for low survival hospitals with OR 2.82 95% CI (1.22, 6.51).
Conclusion: This is the first study to show that overall survival for a hospital's trauma population is associated with an increased risk of surgical site infection, despite being matched for age, gender, and insurance status. The implications of these findings mean that at a systems level, SSI can be addressed. Focused research efforts are necessary to elucidate the reason for this difference however; targeted interventions at low survival hospitals may resolve this discrepancy and improve patient outcomes.
YoungHeatherMDBlissRobinPhDCareyJ CHRISMDPriceConnie SMD
University of Colorado Health Sciences Center, Denver Health Medical Center
Beyond Core Measures: Identification of Modifiable Risk Factors for the Prevention of Surgical Site Infection after Elective Total Abdominal Hysterectomy
Background: Despite adherence to the Centers for Medicare and Medicaid Services' (CMS) core measures for preventing surgical site infections (SSI), the rate of SSI after total abdominal hysterectomy (TAH) at our institution is 10%, well beyond the 90th percentile for SSI rates published in the 2009 National Healthcare Safety Network report.
Methods: This is a retrospective chart review of patients who underwent elective TAH at a public safety net hospital in Denver CO between December 2005 and March 2010. Clinical variables were abstracted from medical charts. The primary outcome was development of SSI within 30 days of TAH. A secondary outcome was adherence to CMS core measures designed to prevent SSI. Chi-square and t-tests evaluated for bivariate associations between the variables and outcomes of interest. Multivariate logistic regression models determined if the risk factors detected in bivariate analyses were independently associated with development of SSI. All tests were performed at the 0.05 significance level.
Results: 224 records were reviewed; 26 were excluded due to emergent TAH and 2 were excluded for no follow-up visits documented in the 30 days after TAH. Patients who developed SSI were similar to their non-SSI counterparts with respect to the indication for TAH, diabetes, and smoking. With regards to CMS core measures, > 95% of patients in both SSI and non-SSI groups received antibiotics in the 60 minutes before surgical incision and > 90% received an appropriate antibiotic. Compliance with PACU normothermia was suboptimal although equivalent in SSI and non-SSI groups (81% vs 75.7%, P = 0.60). Among non-modifiable risk factors, SSI was more common in obese (BMI ≥ 30) than non-obese patients (70% vs 43.5%, P = 0.02) and in patients who had operative estimated blood loss (EBL) ≥ 500 mL than those with EBL < 500 mL (47.6% vs 26.9%, P = 0.05). Obesity remained a significant risk factor in multivariate analyses (OR 3.17, CI 1.14-8.77, P = 0.03) while the effect of EBL ≥ 500 mL on SSI was reduced (OR 2.01, CI 0.76-5.26, P = 0.16). Among modifiable risk factors, SSI was associated with blood transfusion in bivariate analyses (28.6% vs 12%, P = 0.04) and trended toward significance in multivariate analyses (OR 2.87, CI 0.90-9.12, P = 0.08). Blood transfusion was not associated with the pre- to post-operative change in hematocrit values; rather it was associated with longer operative times (4.2 hrs vs 2.7 hrs, P < 0.001), EBL ≥ 500 mL (66.7% vs 22.6%, P < 0.001), and both pre- and post-operative hematocrit values (34.6% vs 39.8%, P < 0.0001; 26.4% vs 32.5%, P < 0.0001).
Conclusion: Obesity is associated with SSI after TAH in our population. Blood transfusion is a modifiable risk factor that trends toward significance and is not associated with the pre- to post-operative change in hematocrit values; larger studies are needed to confirm this result and determine appropriate thresholds for transfusion in this population.
MasonLeonard LMDTiesiGregoryMDDosiGarimaMDFeketeovaEleonoraMDBlackwellLaurenMDReinoDiegoMDShethSharvilMDPalangeDaveBSDeitchEdwin AMD, FACS
University of Medicine and Dentistry of New Jersey-New Jersey Medical School
Polymorphonuclear (PMN) and Red Blood Cell Function are Rapidly Altered following Major Trauma
Introduction: Preclinical and human studies have shown trauma-hemorrhagic shock (T/HS) is associated with acute alterations in red blood cell (RBC) and PMN function. Trauma-induced RBC microcirculatory rigidification/adhesiveness and PMN hyper-activation have been implicated in the development of early multiple organ dysfunction syndrome. Our lab has previously shown that these cellular changes occur early in different animal T/HS models. To date, there are few studies reporting abnormal patterns in RBC function and PMN activation in trauma patients. The purpose of this study, performed in severely injured trauma patients, was to measure neutrophil activation and RBC dysfunction during the early post injury period.
Hypothesis: Following major blunt or penetrating trauma, the majority of patients will exhibit neutrophil hyper-activation, decreased erythrocyte deformability and increased RBC adhesiveness occurring immediately upon or shortly after arrival to the Trauma Unit.
Methods: Study cohort consisted of 27 severely injured trauma patients (all males, age 35 ± 13, ISS 25 ± 7) and 11 age, gender matched controls. Mechanism of injury was blunt in 48% and penetrating in 52% of the cohort. Blood samples were collected upon admission (<1 hr after injury) to the Trauma Unit and at 3–6 hrs post admission. RBC deformability was determined at a low shear stress (0.30 Pa), using an ektacytometer. Changes in deformability were measured as changes in the elongation index (EI). Ex vivo RBC adherence to human umbilical vein endothelial cells (HUVEC) was quantified by counting cells adhered to the HUVEC monolayer in three randomly selected fields using an optical microscope. To evaluate PMN activation, respiratory burst (RB) and CD 11b receptor expression were assayed by flow cytometry. Data was expressed as mean fluorescence units (MFI).
Results: Following significant trauma, RBC dysfunction (decreased deformability, increased adherence) and PMN activation appeared immediately upon admission to the Trauma Unit (Table). Neutrophils become primed early after the initial injury and this level of activation persisted at 6 hours post injury as reflected by increased CD 11b expression and RB.
Lower EI numbers reflect decreased RBC deformability with data expressed as 10-2. Data expressed as mean ± SD; *p < 0.05 vs. volunteers.
Conclusions: RBCs undergo a spectrum of abnormalities including the novel observations of increased HUVEC adhesion and decreased deformability that appear early after the initial insult. PMNs become primed and the level of activation persisted. Trauma-induced RBC dysfunction and PMN hyper-activation may contribute to the development of impaired microcirculatory blood flow and early multiple organ failure. These cellular changes occur within an hour of major trauma suggesting a therapeutic intervention would be optimally initiated shortly after arrival in the Trauma Unit.
AlemayehuHannaMDHoVanessa PMD, MPHLeviterJulie IBSDrusinLewis MMD, MPHBariePhilip SMD, MBA
Weill Cornell Medical College and Westchester Medical Center
Medical Students and Hospital Hand Hygiene - What do they know, and What do they do?
Introduction: Although hand hygiene (HH) is the simplest, most effective measure to prevent transmission of nosocomial infections, compliance (CMP) with HH guidelines (HHG) among healthcare professionals is often suboptimal. This study examined medical student (MS) knowledge (KNO) and CMP with HHG and potential factors associated with improvement. We hypothesized that MS year, time, presence of a mentor who emphasized HH, presence of intensive care unit (ICU) experience, discussion of HH at rotation orientation, and specific core rotations would be associated with improved KNO and CMP.
Methods: Prospective anonymous surveys were serially administered to third-year (MS3) and fourth-year (MS4) students from an LCME accredited U.S. medical school over one academic year at the beginning of every core rotation (medicine, surgery, primary care medicine, pediatrics, obstetrics/gynecology, neurology, psychiatry). MS answered 10 items testing KNO of HHG (score range 0–100%) as well as reported CMP with HH measures (range 0–100%). Date of survey, current MS year, rotation, ICU experience, identification of a mentor, and rotation-specific orientation discussion of HH were also documented. Surreptitious direct observation of HH opportunities was also made. Temporal analysis compared June-December survey (EAR) with January-June survey (LAT) subgroups. Groups were compared using the Student t test, p < 0.05.
Results: 160 MS3 and 98 MS4 completed surveys; overall mean KNO was 64.5% (SD = 19.8) and CMP was 87.9% (SD = 9.8). Direct observations reported proper HH in 87.9% of encounters, which correlated with self-reported CMP. MS3 and MS4 similar showed similar mean KNO scores (62.9% and 65.3%, respectively; p = 0.21), but MS4 reported higher CMP (84.3% and 89.1%, respectively; p = 0.0001). Temporal analysis among MS3 showed improved mean self-reported CMP (82.6% (SD = 9.4), vs. 86.8% (SD = 9.6); p = 0.021) but no improvement in KNO, whereas MS4 showed improvement in KNO (EAR 62.6% (SD = 19.9) vs. LAT 67.4% (SD = 20.1); p = 0.031), but not CMP. Mentorship was associated with increased CMP (90.1% vs. 87.0%; p = 0.005), yet discussion of HH at orientation correlated with decreased CMP (84.5% vs. 87.3%; p = 0.03). ICU experience and specific core rotations did not have an effect on KNO or CMP. MS demonstrated better KNO about appropriate use of alcohol-based sanitizer than other HH modalities (KNO of 83.7%-95.8% for appropriate situations for alcohol-based sanitizer use (except prior to invasive procedures), vs. 2.3%-23.8% for situations requiring HH with soap and water).
Conclusions: KNO of HHG is universally poor for clinical MS, who are not receiving adequate education on appropriate HH practices, particularly when to wash hands with soap and water. Despite this, MS report relatively high CMP, which correlated with directly observed HH opportunities. However, observation occurred mostly in situations where alcohol-based sanitizer was appropriate, which may explain the high CMP with observation. The importance of mentors and their effect on MS education, especially in the area of HH, cannot be overemphasized.
Introduction: Pneumonitis associated with inhalation injury continues to be a significant challenge for the burn clinician.
Background: Progressive respiratory failure exceeding the limits of conventional ventilator strategies occurs in a select group of burn patients whom develop severe pneumonitis associated with inhalation injury. Airway pressure release ventilation(APRV) may represent an option when conventional modes are failing.
Methods: A five year IRB approved retrospective study was performed comparing patient characteristics and outcomes of APRV to conventional modes. Patients were diagnosed with inhalation injury based on the history of an enclosed space fire, physical and bronchoscopic findings. Pneumonitis was based on CXR, sputum and additional data. Severe respiratory distress was defined as a PO2/FIO22 ratio(P/F) < 200. Two groups of patients were identified retrospectively: those treated with conventional ventilation and those treated with APRV. A total of 78 patients were screened and complete data was available for 45 patients: conventional ventilation = 19 and APRV = 26.
Results: There were a greater number of males(p < 0.05) and fewer survivors in the sicker APRV group(p < 0.05). For the APRV group the P/F at initiation of APRV was 132.5(mean ± 39.3) with duration until attaining a P/F > 200 of 49.2 ± 63.9 hours and reaching a P/F > 250 at 54.9 ± 66.6 hours. For those patients who died, the average number of days on APRV was 10.0 ± 8.4 days. Over the last two year year periods, the mean duration of APRV until a P/F > 200 decreased from 33.2 hours to 10.1 hours. This was because of greater familiarity of a mode felt to be an option in the face of failing conventional ventilation modes.
Conclusion: APRV provided salvage ventilation with severe inhalation pneumonitis failing conventional ventilator support.
Beta Blockade following Injury: A Critical Link between Heart Rate and Immunomodulation
Introduction: Severe trauma induces a profound elevation of catecholamines that is associated with a persistent anemic state. The use of propranolol (BB) at 10 mg/kg in rats has previously been shown to prevent erythroid growth suppression in bone marrow (BM), prevent hematopoetic stem cell (HPC) mobilization, and decrease plasma G-CSF levels following injury. This study seeks to further investigate the dosing of BB to determine if lower doses of BB remain protective.
Methods: Male Sprague-Dawley rats (n = 4-8/group) were subjected to a combined lung contusion (LC), hemorrhagic shock (HS) model + /- BB. Those animals receiving BB were given propranolol at 1, 2.5, or 5 mg/kg IP following resuscitation. Peripheral blood and BM were obtained at 3hrs post resuscitation. Flow cytometry was used to determine the % of CD71 + /CD117 + lymphocytes, to estimate HPC mobilization. Plasma G-CSF levels were determined using a commercial ELISA. Heart rate (HR) was also recorded. (*p < .05 vs. control; **p < .05 vs. LC/HS by ANOVA and Tukey Kramer).
Results: Following LC/HS there is a significant increase in HPCs in peripheral blood as compared to control. Propranolol at 5 mg/kg significantly reduces HPC mobilization and restores BM cellularity (Table). Similarly, only 5 mg/kg BB decreased plasma G-CSF levels. Propranolol at 5 mg/kg was the only dose to significantly decrease HR (Table).
Conclusion: Administration of at least 5 mg/kg propranolol following resuscitation prevents HPC mobilization and preserves BM cellularity thus protecting the BM following shock and injury. BM protection is physiologically associated with a reduction in HR. Therefore, the beneficial effect of propranolol in attenuating BM dysfunction following injury occurs at a dose that also has a chronotropic effect.
HawserStephenPhDHobanDarylPhDHackelMeredithPhDBouchillonSamMDJohnsonJackMBADowzickyMichaelBS
IHMA Europe Sàrl
Occurrence of Enterobacter Cloacae and E. Aerogenes in Intra-Abdominal Infections During 2009: Activity of Tigecycline and Comparator Agents (T.E.S.T. 2009)
Background: Intra-abdominal infections (IAIs) represent some of the most frequently encountered nosocomial infections in the healthcare setting and are mostly caused by Gram-negative bacilli (GNB). Enterobacter spp., comprise an important part of the etiology of such infections, of which increasing drug-resistance may lead to a limitation in available therapies. In the current report we describe the occurrence of Enterobacter aerogenes and E. cloacae in IAIs and their susceptibility to tigecycline and comparator agents.
Methods: A total of 3,854 isolates were collected worldwide from gastro-intestinal (GI) sources during 2009. E. aerogenes (n = 53) and E. cloacae (n = 222) comprised 1.4% and 5.8% of all GI isolates, respectively All isolates were collected during the Tigecycline Evaluation and Surveillance Trial (T.E.S.T.). MICs were performed and interpreted according to CLSI and FDA guidelines (tigecycline) where appropriate.
Results: The activity of tigecycline and selected comparators are shown in the Table.
%S, percent of isolates susceptible (S), intermediate (I) or resistant (R).
Conclusions: Collectively, E. aerogenes and E. cloacae comprised 7.2% of all isolates from GI sources during TEST 2009. The most active agents against these two species were amikacin, cefepime, meropenem and tigecycline, and all consistently exhibited susceptibility > 90%. Overall, resistance to tigecycline was the lowest for all agents tested.
BadalRobertBSHobanDarylPhDHackelMeredithPhDBouchillonSamMDJohnsonBrianBSHawserStephenPhDDowzickyMichaelBS
IHMA, Inc.
Activity of Tigecycline and Comparators against North American K. Pneumoniae from Gastrointestinal Infections Test 2005-2009
Background: The Tigecycline Evaluation and Surveillance Trial (TEST) has tracked the in vitro activity of tigecycline and comparators against gram-negative organisms from a broad range of infections since 2004. This report summarizes that activity against Klebsiella pneumoniae (Kp) and extended-spectrum beta-lactamase (ESBL) producing Kp collected from 2005–2009 in North America (NA). Methods: 319 clinically significant Kp were obtained from intra-abdominal infections from 2005–2009 in NA. 12 isolates (3.8%) were ESBL + . MICs were determined using supplied broth microdilution panels. Results were interpreted according to CLSI or FDA (tigecycline) guidelines.
Results: The % Susceptible/Intermediate/Resistance for tigecycline and comparators is shown in the following table:
Drug
Organism
N
%S
%I
%R
Amikacin
K. pneumoniae
319
99
1
0
K. pneumoniae ESBL+
12
100
0
0
Cefepime
K. pneumoniae
319
96
1
3
K. pneumoniae ESBL+
12
42
17
42
Ceftazidime
K. pneumoniae
319
90
3
7
K. pneumoniae ESBL+
12
0
8
92
Ceftriaxone
K. pneumoniae
319
92
1
8
K. pneumoniae ESBL+
12
8
0
92
Levofloxacin
K. pneumoniae
319
91
1
8
K. pneumoniae ESBL+
12
0
0
100
Meropenem
K. pneumoniae
201
97
1
2
K. pneumoniae ESBL+
8
75
0
25
Minocycline
K. pneumoniae
319
84
6
10
K. pneumoniae ESBL+
12
67
0
33
Piperacillin-Tazobactam
K. pneumoniae
319
90
3
7
K. pneumoniae ESBL+
12
8
25
67
Tigecycline
K. pneumoniae
319
96
3
1
K. pneumoniae ESBL+
12
92
0
8
Conclusions: The ESBL + rate among Kp from IAI in NA was 3.8% from 2005–2009, but only 2.7% in 2009, suggesting no upward trend at this point. Against Kp overall, only minocycline among drugs evaluated in TEST had a %S value < 90%, while tigecycline was 96%. Against ESBL + Kp, however, only amikacin (100%) and tigecycline (92%) retained > 90% activity. If patients are at risk of having ESBL + Kp IAI, tigecycline appears to be a therapeutic option.
BouchillonSamMDJohnsonBrianBSBadalRobertBSHobanDarylPhDHackelMeredithPhDHawserStephenPhDDowzickyMichaelBS
IHMA, Inc.
Incidence of Escherichia Coli, Extended-Spectrum Beta-Lactamase Production (ESBL), and the Activity of Tigecycline and Comparators in Intra-Abdominal Infections (IAI) in the United States - Test, 2005-2009
Background: The Tigecycline Evaluation and Surveillance Trial (TEST) has tracked the in vitro activity of tigecycline and comparators against gram-negative organisms from a broad range of infections since 2004. This report summarizes that activity against Escherichia coli and extended-spectrum beta-lactamase (ESBL) producing E. coli collected from 2005–2009 in the United States. Methods: 522 clinically significant E. coli were obtained from intra-abdominal infections from 2005–2009 in NA. 7 isolates (1.3%) were ESBL producers. MICs were determined using supplied broth microdilution panels. Results were interpreted according to CLSI or FDA (tigecycline) guidelines.
Results: The % Susceptible/Intermediate/Resistance for tigecycline and comparators is shown in the following table:
Escherichia coli (n = 522)
Escherichia coli, ESBL (n = 7)
Drug
MIC50 | MIC90
%S | %I | %R
MIC50 | MIC90
%S | %I | %R
Amikacin
2 | 4
99.4 | 0.4 | 0.2
2 | 16
100 | 0 | 0
Amox-Clav
4 | 32
75.7 | 14.2 | 10.2
32 | >32
14.3 | 28.6 | 57.1
Cefepime
≤0.5 | ≤0.5
98.1 | 0.8 | 1.2
16 | >32
28.6 | 42.9 | 28.6
Ceftazidime
≤8 | ≤8
95.6 | 1.5 | 2.9
32 | >32
28.6 | 14.3 | 57.1
Ceftriaxone
≤0.06 | 0.25
93.7 | 1.2 | 5.2
>64 | >64
0 | 14.3 | 85.7
Imipenem
0.25 | 0.5
99.5 | 0 | 0.5
0.12 | 0.12
100 | 0 | 0
Levofloxacin
0.03 | > 8
81.2 | 1.3 | 17.4
>8 | >8
0 | 0 | 100
Meropenem
≤0.06 | ≤0.06
98.5 | 0.9 | 0.6
≤0.06 | 0.5
100 | 0 | 0
Minocycline
1 | 8
83.3 | 8.4 | 8.2
8 | >16
42.9 | 14.3 | 42.9
Pip-Tazo
1 | 4
97.5 | 0.6 | 1.9
8 | >128
71.4 | 0 | 28.6
Tigecycline
0.12 | 0.25
100 | 0 | 0
0.25 | 0.25
100 | 0 | 0
Conclusions: The ESBL positive rate among E. coli from IAI in the United States was 1.3% from 2005–2009. Overall, there has been a modest but steady increase in ESBLs each year from 0.8% in 2005 to 2.8% in 2009 (about 1 or 2 ESBL isolates per year). Amoxicillin-clavulanic acid, levofloxacin, and minocycline each demonstrated in vitro %S values < 90%, while all remaining study drugs demonstrated activity > 93%. Amikacin, imipenem, meropenem, and tigecycline each inhibited 100% of ESBL producing E. coli at their respective CLSI or FDA susceptible breakpoints.
HackelMeredithPBouchillonSamMDHobanDarylPhDJohnsonBrianBSBadalRobertBSJohnsonJackMBAHawserStephenPhDDowzickyMichaelBS
IHMA, Inc.
Activity of Tigecycline and Comparators against Clinical Isolates from Medical and Surgical Intensive Care Units (Test 2009)
Background: The increasing incidence of antimicrobial resistance represents a major threat to hospitalized patients, especially those in intensive care units (ICUs). The Tigecycline Evaluation Surveillance Trial (T.E.S.T.) program has monitored the in vitro activity of tigecycline and comparators since 2004. The current study investigated the activity of tigecycline and comparators against 10,616 isolates from medical and surgical intensive care units isolated during 2009. Methods: All isolates were identified to species level by participating sites in 45 countries and confirmed by the central laboratory. Isolates came from medical and surgical ICUs. Minimum inhibitory concentrations (MICs) were determined by the local laboratory using supplied broth microdilution panels and interpreted according to CLSI or FDA (tigecycline) guidelines.
Results: MIC90 (μg/ml) and %S of the 10,616 isolates are shown below.
Enterobacteriaceae (n = 7,481)
Acinetobacter spp (n = 868)
P. aeruginosa (n = 890)
Drug
MIC90
%S
MIC90
%S
MIC90
%S
Tigecycline
2
95.7
2
na
16
na
Amikacin
8
93.8
>64
39.3
64
83.2
Cefepime
>32
80.0
>32
30.9
32
66.6
Meropenem
0.25
97.9
>16
39.3
>16
66.7
Levofloxacin
>8
73.6
>8
27.8
>8
58.3
Minocycline
>16
59.2
8
77.7
>16
na
PipTazo
>128
71.8
>128
24.3
>128
76.2
Drug
S. aureus (n = 772)MIC90
Enterococcus spp (n = 605)%S
MIC90
%S
Tigecycline
0.5
100
0.25
99.5
Levofloxacin
32
55.0
>32
39.8
Linezolid
4
100
2
99.3
Minocycline
4
90.3
>8
42.3
Vancomycin
1
99.6
>32
87.6
na, no clinical breakpoint for this drug / organism combination.
Conclusion: Meropenem was the most active compound against Enterobacteriaceae, while tigecycline had the lowest MIC90 against gram-positive organisms, with activity comparable to linezolid and vancomycin. Tigecycline's in vitro activity was comparable to or greater than most commonly prescribed broad spectrum antimicrobials for all ICU strains tested in this study, including methicillin resistant S. aureus and extended spectrum beta-lactamase producers.
HobanDarylPhDHackelMeredithPhDBadalRobertBSBouchillonSamMDJohnsonBrianBSHawserStephenPhDDowzickyMichaelBS
IHMA, Inc.
Susceptibility of Streptococcus Agalactiae from Multiple Infection Sites: Results of the Tigecycline Evaluation Surveillance Trial (Test) 2009-2010
Background: Streptococcus agalactiae (GBS) is a major cause of neonatal and perinatal infections as well as a causative pathogen of bacteremia, respiratory, skin and skin structure and urinary tract infections. Although all GBS reported to date remain susceptible to penicillin, resistance to erythromycin and clindamycin has been documented. The Tigecycline Evaluation Surveillance Trial (TEST) examines the susceptibility of pathogens isolated from patients in countries worldwide. Methods: Clinically significant GBS were obtained from the following infection sites: blood, urine, respiratory, skin and skin structure and fluids. MICs were determined for 1,237 isolates of GBS isolated from a cumulative total of 322 sites in 49 countries during 2009–2010 utilizing supplied broth microdilution panels. Results were interpreted according to CLSI or FDA (tigecycline) guidelines. Results: The % Susceptible and MIC90 (μg/ml) for six selected antimicrobial agents is shown in the following table:
S. agalactiae – %S/MIC90 (μg/ml)
Drug
Blood
Skin/Structures
Urine
Respiratory
Fluids
Ampicillin
100/0.12
100/0.12
100/0.12
100/0.12
100/0.12
Ceftriaxone
100/0.12
100/0.12
100/0.12
100/0.12
100/0.12
Linezolid
100/1.0
100/1.0
100/1.0
100/2.0
100/2.0
Meropenem
100/≤0.12
100/≤0.12
100/≤0.12
100/≤0.12
100/≤0.12
Tigecycline
100/0.12
100/0.12
100/0.12
100/0.12
100/0.12
Vancomycin
100/0.5
100/0.5
100/0.5
100/0.5
100/0.5
N =
326
311
366
82
152
Conclusions: All GBS isolated in 2009–2010 remained 100 percent susceptible to the studied antimicrobials with the MIC90 for each antimicrobial remaining constant regardless of infection site. Global GBS isolated from a variety of clinical specimens continue to demonstrate complete susceptibility to the studied antimicrobials and stable MIC90.
JohnsonBrianBSBouchillonSamMDJohnsonJackMBAHobanDarylPhDHackelMeredithPhDBadalRobertBSHawserStephenPhDDowzickyMichaelBS
IHMA, Inc.
Susceptibility of MRSA from Respiratory and Wound Sources to Linezolid and Comparators in the U.S. from the T.E.S.T. Program - 2004-2010
Background: Staphylococcus aureus continues to be a therapeutic challenge for physicians despite the introduction of new antimicrobials to treat it. Linezolid has shown excellent activity against Staphylococcus spp., including methicillin resistant S. aureus. This study evaluated the in vitro activity of linezolid as compared to 5 comparators: levofloxacin; minocycline; vancomycin; and tigecycline; against isolates of methicillin-resistant Staphylococcus aureus (MRSA). Methods: The isolates originated from 567 cumulative US centers in the T.E.S.T. program. A total of 3,091 clinical isolates from wound and respiratory sources were identified to the species level at each of participating sites and confirmed by the central laboratory. MICs were determined by each participating laboratory using broth microdilution panels. All testing was performed and interpreted according to CLSI and FDA (tigecycline) guidelines and manufacturer's instructions.
Results: MRSA results are summarized in the following table:
Respiratory
Wounds
Antibiotic
N
MIC90
%S
N
MIC90
%S
Tigecycline
907
0.25
100
2184
0.25
100
Levofloxacin
907
> 32
11.5
2184
> 32
39.3
Linezolid
907
4
100
2184
2
100
Minocycline
907
0.5
99.2
2184
0.5
98.9
Vancomycin
907
1
100
2184
1
99.9
Conclusions: The in vitro activity of tigecycline, linezolid, minocycline, and vancomycin were all comparable against MRSA with %S above 98%. MIC90 values and %S were similar regardless of body source.
FlynnLisa MMDHall-ZimmermanLisa GPharmDWilsonRobert FMD
Wayne State University/Detroit Medical Center
Factors affecting the Incidence of Infection after Colorectal Trauma
Introduction: Infection is the most frequent serious complication following colorectal trauma in patients who survive at least 48 hours. Knowledge of the risk factors associated with an increased incidence and/or severity of infection should aid in the management of these patients.
Methods: This IRB-approved, retrospective study evaluated 193 patients from 1999 to 2010 who underwent emergency operation for colorectal trauma and had a hospital length of stay of at least 48 hours. The infections considered in this review included: pneumonia, bacteremia, intraabdominal abscess, urinary tract infection (UTI), or surgical wound infection. Infections were further categorized as traumatic or nosocomial. Intraabdominal and wound infections were considered traumatic and nosocomial infections included: UTI, pneumonia and bacteremia. The factors affecting the incidence of all types of infections were analyzed.
Results: Of 193 patients, 93 were considered critically ill and were admitted post-operatively to the surgical ICU. Overall, post-operative infections developed in 71/193 (37%) of the patients. Of these, 47 (66%) occurred in ICU patients and 24 (34%) occurred in regular surgical ward patients, (p < 0.001). The incidence of infection was higher in the ICU vs non-ICU patients, 47/93 (51%) vs 24/100 (24%), (p < 0.001). Of 52 patients with severe infections (pneumonia, abdominal abscess, and/or bacteremia), 39 occurred in ICU and 13 occurred in non- ICU patients (75% vs 25% respectively) (p < 0.001).
ICU patients with infection had a longer hospital length of stay (LOS) than patients without infection, [23.8 ± 18.1 vs 10.8 ± 10.3 days, p < 0.001]. The hospital LOS was evaluated for traumatic and nosocomial infections separately. In the traumatic infection group, the LOS was 22.7 ± 19.4 days vs 8.4 ± 6.9 days for patients without infection (p < 0.0001). The nosocomial infection group LOS was 20.3 ± 19.0 days vs 8.4 ± 6.9 days for those without infection (p < 0.0001). Specific factors associated with traumatic infections included: any administration of blood (p = 0.005), concomitant splenectomy (p = 0.003), severe colon injury (p < 0.001), and creation of an ostomy (p < 0.001). Factors associated with nosocomial infection included: any administration of blood (p < 0.001), severe colon injury (p = 0.004), and creation of an ostomy (p = 0.005).
The most significant predictor of infection was the administration of one or more units of blood.
Overall Summary of Results
Factor Any blood tx
Infection N = 71 44 (62%)
No Infect N = 122 41 (34%)
P-value 1.8 × 10-5
Ostomy
26 (39%)
18 (15%)
7.4 × 10–5
Sev colon inj
32 (45%)
24 (19%)
1.7 × 10–4
Splenectomy
10 (14%)
4 (3%)
0.005
ED SystBP<90
20 (28%)
16 (13%)
0.017
LOS (days±SD)
19.1 ± 16.4
8.4 ± 6.4
1.0 × 10–12
Conclusion: Infections occur frequently after colorectal trauma, especially in those who are critically ill. Options for reducing these infections can include rapid control of hemorrhage and tolerance of lower hemoglobin levels to avoid blood transfusion. One should also avoid ostomy creation and concomitant splenectomy whenever possible.
BadalRobertBSBouchillonSamMDHobanDarylPhDJohnsonAaronBAHackelMeredithPhDHawserStephenPhD
IHMA, Inc.
Trends in Susceptibility of Intra-Abdominal Infections in North America - Smart 2005-2010
Objectives: The Study for Monitoring Antimicrobial Resistance Trends (SMART) has monitored the in vitro activity of ertapenem (Etp), amikacin (Ak), cefepime (Cpe), cefoxitin (Cfx), ceftazidime (Caz), ceftriaxone (Cax), ciprofloxacin (Cp), imipenem (Imp), levofloxacin (Lvx), and piperacillin-tazobactam (PT) against aerobic gram-negative bacteria isolated from intra-abdominal infections (IAI) globally for many years. This report compares susceptibility rates from 2005 to those in 2010 for the most predominant IAI pathogens in North America (NA).
Methods: Eight labs in 2005 and 14 labs in 2010 in the NA collected up to 100 consecutive gram-negative isolates from IAI each year. Broth microdilution MICs were determined following CLSI guidelines. Extended-spectrum beta-lactamase (ESBL) production was determined using the CLSI phenotypic method. Percent susceptible (%S) rates in 2005 and 2010 were compared for the top 10 species isolated. Fisher's Exact Test, two tailed, was used to determine statistical significance.
Results: ESBL + rates (%) in 2005/2010 for Escherichia coli and Klebsiella pneumoniae were 1.7/5.4 and 3.2/15.2, respectively. The susceptibility percentages of the 10 species constituting > 95% of all IAI aerobic gram-negative pathogens are summarized in the following table:
Significant differences between years are boldened (P < 0.05).
Blanks = no breakpoints defined.
Percent Susceptible (%) (CLSI M100-S20-U).
Conclusions: ESBL + rates in IAI in NA for E. coli and K. pneumoniae have increased significantly since 2005, but are still lower than those seen in most other regions of the world. Despite relatively low ESBL + rates, %S of E. coli to the fluoroquinolones, cefepime, and pip-tazo has dropped significantly, while K. pneumoniae %S has decreased significantly only for the 3rd generation cephalosporins. Amikacin, cefepime, ertapenem, and imipenem remain effective in vitro vs. most Enterobacteriaceae isolated from IAI in NA, even after applying the lower interpretive carbapenem CLSI breakpoints recently published in document M100-S20-U.
PriceConnie SavorMDGilmartinHeather MMSN, RN, NP, CICSabelAllison LeeMD, PhD, MPH, CMQ
Denver Health and Hospital and University of Colorado Denver
Surgical Site Infections among Patients with Procedures Involving Arthroscopy
Background: Reported rates of postarthroscopy SSI are rare. An increase in surgical site infection (SSI) rates among patients who had procedures involving arthroscopes was noted in two surgery centers (A and B) at a Colorado hospital. During a 10 month period, 9 patients with SSI were identified, 3 of which were due to Enterobacter cloacae. We describe risk factors that contributed to an outbreak of post-arthroscopy SSI and the source of the E. cloacae cluster.
Methods: The medical record of each patient with postarthroscopy SSI during a 10-month period was reviewed and classified by CDC guidelines. 3 controls of non-infected orthopedic arthroscopy cases from the same time period were randomly selected for each infected case. A total of 9 case and 27 control charts were reviewed for a comprehensive list of exposures as part of a case-control study. Statistical analysis was performed for Fisher's Exact tests with odds ratios and confidence intervals. Environmental samples for culture were obtained. Central sterile processing and OR staff and surgeons were interviewed to assess knowledge of decontamination, sterile processing, and infection control practices. The physical plant of both surgery centers was toured and an arthroscopy case was observed. Relevant written procedures and risk management reports were reviewed.
Results: Between 1/1- 9/21/06, 9/ 2292 (0.39%) patients who had arthroscopic procedures at surgery center A and B developed SSI, a 3 ½-fold increase over a baseline of 0.11%. Of the 9, 6 developed SSI after arthroscopy at surgery center A (0.71% of 842 arthroscopies) and 3 developed infection after arthroscopy at surgery center B (0.21% of 1450 arthroscopies). No individual provider was present in more than 3 cases. Case patients were older, more commonly male, more likely to have a prior medical or orthopedic surgery history, and more commonly had an ASA classification of III or higher. Case patients were more likely to receive intra-articular corticosteroid injection intraoperatively and were more likely to have been prepped with betadine than control patients. However, only older age was a statistically significant (p = 0.01). All but one SSI was deep-incisional or joint space and microbiologically confirmed. 3 were due to E. cloacae after knee arthroscopy. The same center, room, surgeon, scrub nurse and camera were common to the 2nd and 3rd E. cloacae cases. E cloacae was not identified from any of the 63 samples from “clean” areas or equipment, but was identified in surgery center B aquaboxes. Several concerns around decontamination procedures in sterile processing were identified in risk management reports. Scopes were observed to sit unprocessed for prolonged periods of time
Conclusion: Overall rates may have been impacted by the higher than usual use of intra-articular steroid use in an older group of patients with higher rate of past medical and orthopedic problems. These risk factors, coupled with lapses in infection control and sterile processing, may have been responsible for the propagation of E. cloacae during this outbreak. An intervention to initiate enzymatic processing of scope lumens immediately postoperatively and limited intra-articular corticosteroid injections halted the outbreak.
YoungHeatherMDMooreSusanMSPHSavitzLucyPhD, MBAPriceConnie SMDBifflWalter LMD
University of Colorado Health Sciences Center Denver Health Medical Center
Surgeons' Acceptance of Surgical Site Infection Risk Adjustment Models
Background: To account for the wide range of reported surgical site infection (SSI) rates, current CDC/NHSN risk stratification models were designed to predict the expected risk of SSI in different groups of patients. Surgeon acceptance of comparative data and risk adjustment is critical to drive quality improvement. The purpose of this focus group was to assess surgeons' acceptance of current risk stratification models and to determine what factors surgeons felt are important for future models of SSI risk stratification.
Methods: Six academic surgeons with a research interest in SSIs, along with a facilitator, participated in a face-to-face focus group discussion held adjunct to the 5th Annual Academic Surgical Congress in San Antonio, TX. The surgeons represented multiple health system types, including academic (4), private (2), safety net (2), and veterans administration (1). Data were collected through audio recordings, transcribed notes, and observations by a qualitative researcher during the focus group session. Content analysis was conducted using an inductive approach with initial topics mentioned by participants identified through an open, heuristic coding process. Topics identified as duplicative were combined into a single occurrence. A topic was identified as a theme if at least 3 participants mentioned or agreed with a topic. Data were reviewed to the saturation point and discussed with the facilitator to ensure the most comprehensive identification of patterns.
Results: Multiple themes relevant to SSI risk stratification were identified and are combined here into five core concepts: (1) current risk adjustment models are inadequate; (2) surgeons acknowledged that they track an excessive number of variables that they feel contribute to SSI but emphasized the importance of focusing on factors that greatly affect the rate of SSI; (3) data are needed to determine which factors are most important and significant to the development of SSI, and risk stratification metrics must reflect this new data; (4) risks of SSI associated with emergency surgery should be considered separately from those of elective surgery; and (5) heterogeneous documentation (i.e., private vs public hospitals) affects the ability to both track and generalize the effects of potential risk factors on development of SSI.
Conclusion: Participating surgeons, representing multiple health system types, felt that the current models for SSI risk assessment are inadequate. While they believe that there are numerous factors that are likely important to accurately adjust risk, they agreed that many presumed risk factors may prove unimportant. A more refined risk adjustment model would likely improve surgeons' acceptance of benchmarks and comparative data, and may also drive quality improvement. These data suggest that further efforts at risk factor assessment are worthwhile.
Infectious Complications after CABG: Does Minimally Invasive Technique Make a Difference?
Introduction: Coronary artery bypass graft surgery (CABG) has remained a mainstay in surgical therapy for coronary artery disease, yet in recent years, the increased use of minimally invasive techniques has evolved with the theoretical goals of improving postoperative morbidity/complications, mortality, and healthcare resource utilization. We evaluated postoperative outcomes after traditional open CABG (full sternotomy) compared to minimally invasive CABG to evaluate whether a minimally invasive approach improves rates of infectious complications.
Methods: An Open Heart Surgery Registry at a University-based hospital was queried from January 2001-June 2010. Patients undergoing elective-only CABG surgery were identified and divided into two groups: traditional open CABG and minimally invasive CABG. Rates of postoperative infectious complications and total hospital length of stay (LOS) were evaluated and compared in these groups, utilizing SAS 9.2 software.
Results: 1,668 patients underwent elective CABG procedures during the study period: 1,325 (79.4%) had traditional CABG surgery and 343 (20.6%) underwent a minimally invasive CABG. The overall post-operative infection rate in patients undergoing traditional CABG surgery was significantly greater compared to patients in the minimally invasive group (4.68% vs. 2.04%; p < 0.03). Significant differences in the rates of postoperative pneumonia were found, with 2.19% after traditional CABG compared to 0.29% in patients after the minimally invasive technique (p < 0.02). No significant differences in the rates of urinary tract infection (UTI) (2.04% vs 1.46%, p = NS) or deep sternal infection (0.76% vs. 0.29%, p = NS) were found. UTI was the predominant infection after the minimally invasive procedure, whereas pneumonia was the leading infection following traditional CABG. No significant differences were found in rates of leg harvest site infection, and notably septicemia. Patients undergoing traditional CABG procedures were found to be 3.4 times (95%CI = 2.26-5.01) as likely to receive blood products as those with minimally invasive CABG. No differences in total hospital length of stay were found between traditional CABG surgery and minimally invasive CABG, utilizing a non-parametric Wilcoxon rank-sum test, with a winsorized mean of 6.6 days (95%CI = 6.41-6.72) versus 6.6 days, (95%CI = 6.25-6.87) respectively. Furthermore, the difference in hospital mortality rates between traditional CABG (1.06%) and minimally invasive CABG (0.29%) was not statistically significant (p = 0.18).
Conclusion: Rates of overall post-operative infection, pneumonia, and blood product usage were significantly lower after minimally invasive CABG. Despite this, minimally invasive techniques failed to reduce rates of common infectious problems such as UTI, wound infection, and septicemia. Furthermore, minimally invasive CABG did not decrease overall LOS or mortality. This analysis suggests that minimally invasive CABG offers some benefit from an infectious standpoint, but future programs are needed to reduce common infectious complications such as UTI, in both groups.
BaculikTanyaMDEckburgPaul B.MDFriedlandH. DavidMDLlorensLilyPhDJandourekAlenaMDWitherellGaryPhDThyeDirkMD
Cerexa, Inc., (a wholly owned subsidiary of Forest Laboratories, Inc., New York, New York)
Early Clinical Response (CR) Analyses of Two Phase III (Canvas 1 and Canvas 2) Trials of Ceftaroline (CPT) Fosamil Vs Vancomycin Plus Aztreonam (V/A) in the Treatment of Complicated Skin and Skin Structure Infections (CSSSI)
Introduction: There is growing interest among the infectious disease research community to assess antimicrobial noninferiority trials via early clinical endpoints as predictors of response in order to provide for greater sensitivity to detect possible differences between comparators. CPT fosamil (prodrug of CPT) was previously shown to be efficacious in the 2 global, double-blind, randomized Phase 3 CeftAroliNe Versus VAncomycin in Skin and Skin Structure Infections (CANVAS 1 and 2; NCT00424190 and NCT00423657) trials using clinical cure rates at the test-of-cure visit (TOC) as primary endpoint (Corey et al, 2010). In an effort to assess CANVAS 1 and 2 results based on early CR, we conducted a secondary analysis.
Methods: Subjects with cSSSI were randomized to receive intravenous (IV) CPT fosamil 600 mg q12h vs vancomycin/aztreonam (V/A) 1 g/1g q12h for 5–14 days. Analyses of CR at Day 3 were conducted in the exploratory modified intent-to-treat (MITT) population who received study drug, had lesion size ≥75 cm2, and either an infected surgical or traumatic wound, major abscess with erythema ≥5 cm, deep/extensive cellulitis, infected arthropod bite, or lower extremity abscess or cellulitis with diabetes mellitus or peripheral vascular disease. CR was achieved if subjects had cessation of infection spread (no increase in baseline lesion width and length measurement), were afebrile at Day 3, and were not considered clinical failures by the investigator on Day 3.
Results: CR rates at Day 3 were 74.0% (296/400) for CPT fosamil and 66.2% (263/397) for V/A in the exploratory MITT population of the pooled CANVAS trials (95% CI: 1.3% to 14.0%). In the individual Phase 3 studies, absolute treatment differences of 9.4% (CANVAS 1) and 5.9% (CANVAS 2) in favor of CPT fosamil were observed.
Conclusion: The CR rate from the pooled CANVAS trials at Day 3 was higher for patients receiving CPT fosamil versus V/A, with a lower limit of the 95% CI > 0. CPT fosamil appears to provide benefit over V/A early in the course of cSSSI, in terms of cessation of lesion spread and resolution of fever.
ByrnesMatthew CMDEggenbergerEileenReicksPattyMulierKristineBeilmanGregory JMD
University of Minnesota
The use of CD64 Levels to Discern Infection in the Presence of Marked Febrile Responses among Patients with a Spinal Cord Injury or Traumatic Brain Injury
Introduction: Patients with spinal cord injury or traumatic brain injury are at significant risk of thermoregulatory dysfunction. Marked febrile responses represent a concerning clinical finding. Clinicians often attribute very high fevers in this patient population to infection; however, many injured patients develop these responses as a result of temperature dysregulation rather than infections. We hypothesized that neutrophil surface expression of CD64 could distinguish between infectious and noninfectious states in patients with spinal cord injuries or traumatic brain injuries.
Methods: Patients admitted to a Level I trauma center were prospectively evaluated. Patients with either a severe traumatic brain injury or spinal cord injury and a marked febrile response (temperature > = 102.5 degrees Fahrenheit) were eligible for the study. IRB approval and informed consent were obtained. Blood samples were obtained within 24 hours of fever and stained using the Leuko64 assay (Trillium Diagnostics, ME) for flow cytometry on the FacsCalibur (BD Biosciences, MD). The assay uses three monoclonal antibodies, CD64 clones 22 and 32.2 and CD163, and fluorescence quantitation beads to measure neutrophil CD64 expression as an index and to establish internal controls. Leuko64 QuantiCALC software (Trillium Diagnostics, ME) was used for analysis. Medical records were evaluated to denote the presence of infection. The average CD64 levels among infected and non-infected patients were calculated. Additionally, sensitivity and specificity of CD64 in screening for infection were calculated.
Results: Nine patients were included in the study. The average age was 35 (18–66). The average injury severity score was 30 (20–54). There were no deaths in the study. The average ICU length of stay was 19 days, and the average number of days the patients were mechanically ventilated was 15. Five patients had clinical and microbiological evidence of infection. There was a trend towards higher CD64 index levels among patients with infection compared to patients without infection (2.42 vs. 1.08, p = 0.17). The CD64 index levels were highest among the patients with bacteremia (3.58) and secondary peritonitis (4.98). We used a cutoff of 1.19 to evaluate the sensitivity and specificity of the test. Among all patients, the sensitivity was 80% and the specificity was 75%. Among patients with spinal cord injuries, the sensitivity and specificity were significantly higher (100% and 100%, respectively).
Conclusion: CD64 index levels can be a useful adjunct to define infectious states in injured patients with a marked febrile response. The test appears to be most useful among patients with spinal cord injuries.
MigginsMakesha VMDLottenbergLarryMDLiuHuazhiMSMoldawerLyle LPhDEfronPhilip AMDAngDarwinMD, PhD, MPH
University of Florida
Surgical Site Infection is Associated with Patient Survival at the Hospital Level: Evidence for Systems Based Interventions
Introduction: Surgical site infections (SSI) account for 15% of all hospital acquired infections and are the most common nosocomial infection occurring in surgical patients. Previous studies indicate SSI negatively impacts patient morbidity, mortality, and healthcare costs. These findings have led to the identification of risk factors associated with the development of SSI and research focused on prevention. To date, no studies have examined the association between patient survival and SSI after trauma. We hypothesized that the development of SSI in trauma patients is related to hospital survivability.
Methods: This is a retrospective cohort study of the University Healthsystem Consortium (UHC) academic trauma centers in the United States from 2004 to 2009. The UHC is comprised of 90% of non-profit academic medical centers in the US. A subset of the database was used to identify trauma patients at least 18 years of age who developed a SSI during their hospital admission. Hospitals were divided into low survival and high survival cohorts based on the average survival risk ratio (SRR). ICD-9 codes for the twenty-five most commonly performed surgical procedures were used to compare the frequency of SSI between the two hospital groups. Chi square tests were used to compare proportions. Univariate regression was used to test for association, while multivariate regression was used to match for potential confounding variables. The final relative risk (RR) values were matched and adjusted for age, gender, and insurance status.
Results: A total of 2,632 trauma patients with SSI were identified from 111 hospitals. Socio-demographic variables were similar between the two cohorts. The patient population in hospitals with lower survival probability tended to have a higher risk of SSI, with an adjusted and matched RR of 1.17 (95% CI 1.01, 1.35). Significantly more patients in the low survival group developed SSI after exploratory laparotomy 2% compared to 0% in the high survival group (p = 0.04). Occurrence of free skin graft necrosis was 6.4% in the low compared to 2.8% in the high survival group (p = 0.04). Skin grafting had the highest risk of SSI for low survival hospitals with RR 2.82 (95% CI 1.22, 6.51).
Conclusion: This is the first study to show that overall survival for a hospital's trauma population is associated with an increased risk of SSI, despite being matched for age, gender, and insurance status. Focused research efforts are necessary to elucidate the reason for this difference however; targeted interventions at low survival hospitals may resolve this discrepancy and improve patient outcomes.
CoyanGarrettBSTennyStevenBSCannonChadMDRichartCharlesMDMoncureMichaelMD
University of Kansas
Evaluating the Relationship between Organ Dysfunction and Mortality in Severe Sepsis and Septic Shock following the Implementation of an Early Sepsis Initiative
Introduction: Organ dysfunction (OD) has been shown to be related to mortality rates in severe sepsis and septic shock (SS/SS). SS/SS has also been associated with significant morbidity and mortality in the surgical patient population. Implementation of an early sepsis initiative (ESI) has been shown to significantly reduce mortality in the surgical patient population. This study examines the relationship between OD and mortality both pre and post implementation of an ESI in the surgical patient population.
Background: A previous review of the SS/SS data set revealed significant decreases in mortality after the implementation of an ESI, along with significant resource savings in the surgical patient cohort at our institution. It was believed that OD data could be used as a further indicator to evaluate the success of implementing an ESI in the surgical patient population.
Methods: A retrospective review of 2831 patients who developed SS/SS after undergoing major surgery was examined from June 2003 to December 2009 in an academic medical center. OD for each patient was organized into six categories according to ICD-9 codes gathered from the charts: Central Nervous System (CNS), Blood and Coagulopathy (Coag), Pulmonary (Pulm), Cardiovascular (CV), Liver, and Renal. Mortality rates were also obtained for the pre intervention group (June 2003-December 2005, N = 720) and post intervention group (January 2006-December 2009, N = 2111). Pre and post intervention cohort mortality was compared, stratified independently by number of organ systems dysfunctional (1 to 6 organ systems dysfunctional) and specific organ system dysfunctional (CNS, Coag, Pulm, CV, Liver, or Renal). A chi-squared analysis was carried out with p < 0.05 considered significant. Results: Significant decreases in mortality rates for patients who had 1 (7% to 4%, p = 0.0015) or 2 (25% to 13%, p < 0.001) OD were observed between the pre and post intervention period. Decreases were also observed for patients with 3 to 6 OD; however, these decreases were not statistically significant. A statistically significant survival advantage was also realized in the post intervention group individually for OD in the CNS, Coag, Pulm, and Renal groups (p < 0.05 for all categories). CV and Liver did not show a significant survival advantage with ESI intervention when compared to the pre intervention cohort.
Conclusion: The use of an ESI in the surgical patient population significantly reduces mortality in the presence of several measures of OD. OD survival could be successfully used as a parameter to measure success of ESI implementation and provide a means of quality control in the SS/SS surgical patient population.
LiYuehuaMSShiXiaolianPhDXuJiaMDWilsonMarkMDFanJieMD
University of Pittsburgh and VA Pittsburgh Healthcare System
Hemorrhagic Shock Activates Endothelial Inflammasome: Role of HMGB1
Introduction: Systemic inflammatory response syndrome (SIRS) and multi-organ failure (MOF) are common complications following trauma, severe surgery, and hemorrhagic shock (HS) that exhibit high mortality and mobility. Acute lung injury (ALI) is an important component of MOF and often serves as a direct cause of death in these patients. HS promotes the development of ALI by inducing the immune system for an exaggerated inflammatory response when responding to endogenous and exogenous danger signals. IL-1β critically contributes to the development of ALI following HS, and the lung endothelial cells (EC) are one of important sources of IL-1β. The production of active IL-1β is tightly controlled by the formation and activation of the inflammasome, which is comprised of NALPs, caspase-1 and ASC. Our previous studies have shown that HMGB1 and PMN NADPH oxidase-derived reactive oxygen species (ROS) mediate HS-induced lung EC activation. The current study is to address whether HMGB1 and ROS are able to mediate HS-induced activation of inflammasome in lung EC and therefore the maturation of IL-1β.
Methods: In vivo studies: WT, TLR4-/-, TLR2-/- and gp91-/- (a component of NADPH oxidase) mice were subjected to HS for 2 h and then resuscitated with Ringer's Lactate. In some mice, anti-HMGB1 antibody (HMGB1 Ab) was injected (i.p.) 10 min prior to the HS. In other groups, PMN were depleted by anti-PMN antibody injection at 16 h prior to HS. At 2 to 6 h after resuscitation, IL-1β in bronchoalveolar lavage fluids (BALF) was measured by ELISA, and inflammasome assembly and caspase-1 activation in the lung tissue were detected using immunoprecipitation and immunoblotting. In vitro studies: WT and gp91-/- mouse lung EC were co-cultured with or without PMN isolated from either WT/HS mice or gp91-/-/HS mice, and treated with HMGB1 for 2 to 6 h. IL-1β release, NLAP3 inflammasome assembly and caspase-1 activation in the EC were then assessed.
Results: In vivo, HS caused increases in IL-1β in BALF and assembly of NALP3 inflammasome and activation of caspase-1 in the lung in the WT/HS mice as compared to WT/sham group. However, these alterations were markedly attenuated in the TLR4-/-/HS, TLR2-/-/HS, gp91-/-/HS, and HMGB1 Ab/WT/HS mice, as well as in the WT/HS mice with PMN depletion. In vitro, HMGB1 induced IL-1β release, NLAP3 inflammasome assembly and caspase-1 activation in the WT lung EC, but not in the gp91-/- EC. Furthermore, the co-culture of WT EC with the HS-activated WT PMN, but not the HS-activated gp91-/- PMN, enhanced the HMGB1-induced IL-1β release, NLAP3 inflammasome assembly and caspase-1 activation in the EC.
Conclusion: HMGB1 and NADPH oxidase-derived ROS play an important role in mediating HS-induced activation of lung endothelial inflammasome and therefore the release of IL-1β.
BlancoFelix CMDChoiPamMDQureshiFaisal GMDSandlerAnthony DMDNadlerEvan PMD
George Washington University School of Medicine, Children's National Medical Center
Increased Incidence of Perforated Appendicitis in Obese Children
Introduction: The impact of obesity on hospital outcomes and chronic illness is well known but its effect on acute surgical disease is not well documented, especially in children. Based on our clinical impression, we hypothesized that obese children may suffer a higher rate of perforated appendicitis (PA). Therefore, we reviewed our experience to determine whether obesity impacted the stage of appendicitis at presentation.
Methods: After obtaining appropriate IRB approval, we reviewed all patients diagnosed with appendicitis at our institution from July 2008 to June 2010. Demographic variables included age, gender, height, and weight. Outcome variable assessed were διαγνoστιχ imaging used, length of stay (LOS), and complication rate. Children were stratified based on obesity using CDC guidelines (BMI > 95 percentile for age and gender). Continuous variables were compared using student's t-test and categorical variables were compared using chi square analysis.
Results: A total of 319 patients with appendicitis were identified during the studied period. There were 62 (19%) obese patients and 257 (81%) non-obese patients. There was no difference in mean age or in gender distribution between the obese and non-obese cohorts. Obese children were more likely (p = 0.026) to present with perforation (28/62, 45%) than their non-obese counterparts (78/257, 30%). Neither mean LOS nor complication rate was impacted by the presence of obesity.
Conclusions: Our data suggest that obese children are more likely to present with PA in comparison to their non-obese counterparts. However, obesity did not increase the risk for postoperative infections or increase LOS. The potential causes for the higher rate of perforation in obese patients remain speculative and is likely multi-factorial, but the increased morbidity is significant.
AminiAmirMDBakerAaronMS, MDTungKellyMDGreenTajiaBSLimDeboraBA,ChoKihoDVM, PhDGreenhalghDavidMD, FACS
University of California–Davis Medical Center
Three Single Nucleotide Polymorphisms of Human Glucocorticoid Receptor Result in Enhanced Activity
Introduction: The glucocorticoid receptor is integrally involved in the endogenous inflammatory response. Given this receptor's unique ability to modulate the immune response, steroids have become important therapy in diseases of inflammation. Prior studies have identified glucocorticoid receptor polymorphisms to alter glucocorticoid sensitivity in certain disease states, sometimes rendering steroid therapy ineffective.
Objective: Identify isoforms of the human glucocorticoid receptor (hGR) within a healthy human population, and determine if they contribute to variability in steroid response.
Methods: Through the survey of 97 healthy human adults, our lab identified a novel glucocorticoid isoform (hGR NS-1). This isoform has three unique single nucleotide polymorphisms (σNΠσ) and displays a hyperactive transactivation potential when compared to the reference National Center for Biotechnology Information human glucocorticoid receptor (hGR NCBI). In this study, we compared the functional activity of hGR NS-1 with that of an hGR derivative matching NCBI reference at baseline and after administration of exogenous hydrocortisone. These receptors were cloned into expression vectors and transfected into TSA201 cells. These cells were then τρɛατɛδ with 4 different graded concentrations of hydrocortisone; 0.000001μM, 0.00001μM, 0.001μM, and 1 uM. Luciferase activity was measured 24 hours later to measure transactivation potential. The enhanced activity of hGR NS-1 was also analyzed through cotransfection of this isoform with hGR NCBI and hGR DL-1. hGR DL-1 is a novel truncated and hypofunctional isoform also identified by our lab.
Results: At baseline, hGR NS-1 demonstrated a greater than 3-fold incr ease in functional activity when compared to hGR NCBI. In addition, the vehicle activity of hGR NS-1 was greater than hGR NCBI stimulated with hydrocortisone at all 4 doses (p < 0.0001). When treated with hydrocortisone doses of 0.000001μM, 0.00001μM, and 0.001μM, hGR NS-1 demonstrated significantly greater transactivation potential when compared to hGR NS-1 vehicle (p < 0.0001) (Figure 1). A peak response occu rred at a hydrocortisone concentration of 0.001μM. Interestingly, transactivation potential of hGR NS-1 decreased significantly compared to baseline activity at a dose of 1 μM (p < 0.001). When the hyperactive isoform hGR NS-1 was cotransfected with either hGR DL-1 or hGR NCBI, enhanced transactivation potential occurred in comparison to hGR NCBI (p < 0.01) or hGR DL-1 alone (p < 0.00001), but decreased when compared to hGR NS-1 alone (p < 0.001).
Transactivation potentials of hGR NCBI and hGR NS-1 at baseline and after stimulation with hydrocortisone.
Conclusion: This experiment demonstrates the hyperactive function of a novel glucocorticoid receptor isoform at baseline and after exogenous hydrocortisone treatment. It also suggests that this response to hydrocortisone treatment is dose dependent. The difference in response to steroid stimulation between this isoform and reference hGR may help explain variability of response to steroid therapy in patients.
WilliamsMonica LBSFriedAaron JCastleShannonMDGrishinAnatolyPhDFordHenri RMD, MHA
Childrens Hospital Los Angeles
Diversity of Postnatal Microbiota in Experimental Necrotizing Enterocolitis
Background: Necrotizing enterocolitis (NEC) is one of the most devastating gastrointestinal disorders that affect 1-5% of all pre-mature infants. Although it is commonly believed that the development of NEC requires colonization of the GI tract with opportunistic pathogens, little is known about the microbial flora associated with NEC. The aim of this study was to characterize bacterial populations of the small intestine in the rat model of NEC.
Methods: Newborn Sprague-Dawley rats (Harlan) from the same litter were fed sterile formula or allowed to breast feed. On day 4 of life, 1 cm of terminal ileum was aseptically excised and flushed with 300 μl sterile PBS. Serially diluted samples were plated on blood agar. Bacterial colonies were counted and classified into groups according to their appearance, typical colony size, and type of hemolysis. The species of representative colonies were identified by sequencing the V6-V8 fragment of the 16S rRNA gene and searching the DNA database for matching sequences using the BLAST algorithm.
Results:
Conclusion: Despite common origin and environment, different animals show dramatic differences in the composition of culturable bacteria populating their small intestines during the early postnatal period. These differences may account for differential susceptibility to NEC.
MuirMarkMDFurmagaWieslawMDMikhailovValeryJonasRachelleRNLoudenChristopherMSCohnStephenMDMichalekJoelPhD
University of Texas Health Science Center at San Antonio
Heat Shock Protein 27 Associated with Poor Outcomes in Hemorrhagic Shock
Objectives: We sought to determine the relationship between serum levels of Heat Shock Protein 27 (HSP27) and clinical outcomes in trauma patients with hemorrhagic shock.
Methods: Serum was collected from a convenience sample of twenty subjects participating in a study of trauma patients with hemorrhagic shock. Samples were collected at admission and three hours later, and HSP27 levels were measured with ELISA by individuals blinded to subject identity and clinical course. Total serum protein levels were also measured, and corrected HSP27 levels were calculated as the ratio of HSP27 to total protein (pg HSP27/mg protein).
Results: Subjects who died (N = 5) had significantly higher initial HSP27 levels than those who did not (median [IQR]: 23.7 [16.7, 24.9] pg/mg vs. 4.2 [2.9, 14.3] pg/mg, p = 0.003). Subjects who developed multiple organ dysfunction syndrome (MODS; N = 2), defined as MODS score ≥ 6 during days 3-30, had significantly higher HSP27 levels at three hours than those who did not (median [IQR]: 14.1 [12.9, 15.3] pg/mg vs. 2.4 [1.2, 5.6] pg/mg, p = 0.026). Three-hour HSP27 values greater than 10 pg/mg appeared predictive (accuracy = 100%) of the development of MODS.
Conclusions: In trauma patients with hemorrhagic shock, elevated HSP27 levels were strongly predictive of the subsequent development of organ dysfunction and death.
AhmedNasimMD, FACSKuoYen-HongPhDDavisJohn MMD, FACS
Jersey Shore University Medical Center
Patient's Characteristic and Possible Risk Factor of C-Difficile Toxic Megacolon
Introduction: Toxic megacolon is the most severe clinical condition of clostridium difficile (c-diff) colitis. Rapid progression of the disease results in high mortality and morbidity. Early diagnosis and prompt intervention may improve outcome.
Method: Data of all patients who were diagnosed with toxic megacolon and underwent subtotal colectomy were reviewed. Patient's demography, clinical characterizes and comorbidities were collected.
Result: Twelve patients underwent subtotal colectomy for toxic megacolon between in 2003 to 2008. Four of twelve patients diagnosed with were excluded from the study: one patient had ischemic, other had ulcerative, another one had malignancies and the fourth one data could not be retrieved. Eight out of twelve patients diagnosed with c-diff colitis result in toxic megacolon. All patients underwent emergency subtotal colectomy. Average age of these patients was 69.5 years, slightly higher incidence in female (63%). Majority of the patients had either very high or very low WBC count (>30000 or < 1.5). The average number of comorbidity was 4.6. The average Charlson index score was 3.4. Two out of eight patients (25%) died, despite emergency subtotal colectomy.
Conclusion: C-diff colitis infection can rapidly progress to life threatening toxic megacolon. Despite subtotal colectomy, mortality is very high. Advanced age, very high or very low WBC count and co-morbidities may be the risk factors for the disease.
KraftRobertMDHerndonDavid N.MDKulpGabriela A.JeschkeMarc G.MD, PhD
Shriners Hospitals for Children
Hypoglycemic Episodes Post-Burn are Associated with Increased Post-Burn Morbidity
Background: Hyperglycemia has been described as detrimental and tight euglycemic control as beneficial in terms of clinical outcomes. Tight euglycemic control however is associated with an increased risk for hypoglycemia and hypoglycemia is suggested to be associated with adverse events. The exact consequences of hypoglycemia are however unknown, thus the aim of this study was to determine the incidence of hypoglycemic episodes post-burn and the effect of hypoglycemia on outcomes.
Methods: Seven-hundred sixty-one pediatric patients were included in this analysis and stratified according the incidence of hypoglycemic episodes defined as < 60 mg/dl during their ICU stay. A sub analysis in a representative group enclosing patients with burns between 50–70% TBSA was conducted. Plasma cytokines, acute phase proteins, and constitutive proteins were analyzed during the first 60 days post admission. Demographics and outcome variables (length of stay, sepsis, multi organ failure (MOF), and mortality) were recorded. Statistical analysis was evaluated by Student's t-test, Chi Square test and linear regression analysis. Statistical significance is set at p < 0.05.
Results: A total of 193 patients had at least one hypoglycemic episode (H1) or more (H2). 568 patients had no hypoglycemic episode (N) throughout the hospital course. H1 (62 ± 17%) and H2 (70 ± 18%) patients had a significant (p < 0.01) larger TBSA burn size compared to N (52 ± 16%). We therefore matched patients according to burn size (N: 75, H1: 19, H2: 27) and analyzed subsequent outcomes. We found that patients with hypoglycemia had an increased MOF (N: 5 [7%] H1: 7 [37%] H2: 19 [70%]) (p < 0.001), Sepsis (N: 5 [7%] H1: 4 [21%] H2: 9 [33%]) (p < 0.01) and infections (N: 2.3 ± 2.0 H1: 3.4 ± 3.0 H2: 3.5 ± 3.0) (p < 0.05). Markers for infection and inflammation such as IL-6, IL-1β, MCP-1, G-CSF, and CRP were significantly (p < 0.05) increased in H1 and H2 compared to N. Renal function was significantly (p < 0.05) worsen in the H1 and H2 compared to the N group during the first 20 days post admit (p < 0.05). Similarly, liver function was significantly worsened in the H1 and H2 group compared to N reflected by significantly higher bilirubin levels (p < 0.05) and reduced total protein (p < 0.05).
Conclusion: The incidence of hypoglycemic episodes correlates with injury severity and is associated with a significantly higher complication rate and increased morbidity. Hypoglycemic episodes are associated with infectious complications and organ dysfunction.
KwekuJosephineMDBochicchioGrant V.MD, MPHDeCastroGerard P.MDZhuShijunPhDHarreraAnthonyMSBochicchioKellyRN, MSScaleaThomas M.MD
University of Maryland School of Medicine, R. Adams Cowley Shock Trauma Center
Hollow Viscous Abdominal Injury is not Associated with Increased Intra-Abdominal Infection following Damage Control Laparotomy
Background: Damage control laparotomy (DCL) is a well-established practice for the abdominal trauma patient suffering from hemorrhagic shock. Many of these patients have incurred penetrating abdominal injuries which put them at increased risk for developing serious infection due to the high possibility of intestinal injury. The current standard of care is to administer a prophylactic dose of cefoxitin pre-operatively to cover for anaerobic and aerobic organisms. This current study compares DCL patients who have incurred hollow viscous abdominal injury (HVAI) to those who have not. Our aim is to determine whether DCL patients with HVAI are at increased risk of intra-abdominal infection.
Methods: Prospective data were collected on 182 patients who underwent a DCL between 2001 and 2008 at the R. Adams Cowley Shock Trauma Center. Data collected included gender, race, ISS, mechanism of injury (MOI), the presence of abdominal hollow viscous injury and intra-abdominal culture data. Primary outcomes included diagnosis of infection (overall, intra-abdominal infection, and bacteremia), mortality, hospital length of stay (LOS), ICU LOS, and number of ventilator days. Univariate analysis and logistic regression models were utilized for data analysis.
Results: 182 patients were enrolled in our study. The mean age was 33 (±14), mean ISS was 34 (±16), and the patient population was predominantly male (83%). The presence of HVAI was identified in 15% of patients. When comparing the patients with HVAI to those without there was no significant difference in overall infection rate (78% vs. 75%; p = 0.7), intra-abdominal infection rate (41% vs. 41%; p = 0.95), and rate of bacteremia (48% vs. 40%; p = 0.4) on both univariate and logistic regression analysis. There is also no significant difference in mortality, hospital LOS, and number of ventilator days. Patients with HVAI did, however, have a longer ICU LOS (27 vs. 18; p < 0.01). Intra-abdominal infections were diagnosed later in the patients with HVAI (hospital day 16 vs. 11; p < 0.05). The most frequently isolated bacteria from intra-abdominal cultures were Enterococcus species (22%), Pseudomonas aeruginosa (15%), Acinetobacter species (11%), MRSA/VRE (7%), and streptococcus pneumonia (4.4%). (Figure 1).
Intra-abdominal culture data.
Conclusion: Our findings demonstrate that the presence of HVAI does not cause an increase in intra-abdominal infection rate in patients undergoing DCL. This could be attributed to the negative pressure therapy that they receive. Most importantly, our findings indicate that broad spectrum antibiotic therapy is needed due to a high incidence of resistant gram positive pathogens. Further study is warranted.
ParkHabeebaMDDe CastroGerard PMDBochicchioGrant VMD, MPHKentJenniferMHSZhuShijunPhDJoshiManjariMDBochicchioKellyMSGenuitThomasMD, MBAHenrySharon MMDScaleaThomas MMD
Sinai Hospital of Baltimore
Percutaneous or Open Tracheostomy? A Comparison of Procedures and Surgical Site Infections
Background: Tracheostomy is one of the most common procedures performed in the ICU in trauma patients. Advantages to open tracheostomy are a larger incision, better visualization, and potentially improved ability to control bleeding, while a disadvantage is that patients must be transferred to the OR. Benefits of the percutaneous procedure include bronchoscopic visualization, minimal surgical scar, and ability to perform the procedure at the bedside in the ICU. Few studies have evaluated the incidence of surgical site infections specifically in a trauma population. Our objective was to compare the incidence of surgical site infections comparing open to percutaneous tracheostomy and discern if there were any differences in outcome.
Methods: A prospective single-institution study was conducted on 676 patients admitted to the ICU over an 8-year period who underwent either an open or percutaneous tracheostomy. Age, sex, gender, race, admission ISS and APACHE scores, and mechanism of injury were obtained. Diagnosis of surgical site infection was established in a multidisciplinary fashion using clinical indicators, leukocytosis, fever, positive site cultures, and the presence of erythema, cellulitis, abscess, or surgical site necrosis post-procedure. Outcome was measured by hospital (HLOS) and intensive care unit length of stay (ILOS), duration of mechanical ventilation, infection rate, and mortality.
Results: A total of 676 patients were evaluated over the study period. The majority of patients were male (56.1%) and white (62.5%) with a mean age of 43.2 ± 20.2 years, ISS 30.7 ± 13.2, and APACHE score of 13.3 ± 6.3. The majority of patients were admitted for blunt traumatic injury (85.1%). 330 open tracheostomies and 310 percutaneous tracheostomies were evaluated. A total of 36 surgical site infections (5.3%) were found. Patients who underwent percutaneous tracheostomy had a statistically significant lower rate of surgical site infections (3.4%) as compared to the open group (7%) (p = 0.04). With regard to HLOS, ILOS, ventilator days, and mortality, however, we found no significant difference between open and percutaneous tracheostomies (Table 1).
Outcomes
Percutaneous N = 310
Open N = 330
OR (95% CI)
P value
HLOS
28.1 ± 17.8
27.2 ± 16.0
NS
ILOS
23.4 ± 28.9
20.2 ± 12.6
NS
Ventilator days
21.8 ± 14.5
20.7 ± 13.8
NS
Infection
11 (3.4%)
25 (7.0%)
0.47
0.041
Mortality
23 (8.2%)
27 (7.6%)
1.08
0.795
Data presented as mean ± SD.
Conclusion: To our knowledge, this is the largest study that has evaluated the benefit of percutaneous vs open tracheostomy in a critically injured trauma population. The risk of infection is significantly lower in the percutanous tracheostomy group. In addition there is the benefit of a significant decrease in cost, equipment charges, transportation costs, and OR charges. Based on the benefits of cost and decreased surgical site infection, percutaneous tracheostomy should be considered to become the standard of care in critically ill trauma patients.
KellyKatherine BMDFadlallaAdam AMPhDClaridgeJeffrey AMD, MS
Department of Surgery, Case Western Reserve University, MetroHealth Medical Center Campus
Where's the Difference? Presentation of Nosocomial Infection in Critically ILL Trauma Versus General Surgery Patients
Introduction: Diagnosing infection in a timely manner is an integral and difficult function of rounding in the intensive care unit (ICU). For intensivists, it would be potentially useful to recognize differences in how trauma and general surgery patients present with new infectious complications. We hypothesized that these two populations would show significant differences in clinical parameters collected on the first day of a new nosocomial ICU infection.
Methods: An analysis was performed on prospectively collected data on all trauma and general surgery patients consecutively admitted to the surgical and trauma ICU over a 21 month period (3/07-11/08). General demographic and clinical data along with specific clinical parameters from the day of a newly diagnosed nosocomial infection were compared between critically ill trauma and general surgery patients. A p-value of 0.05 or less was considered statistically significant.
Results: 1,657 critically ill trauma and general surgery patients were included in the analysis. 82% of the patients were trauma patients and 18% were general surgery admissions. These patients accounted for 10,424 total ICU days. 175 patients were diagnosed with 267 nosocomial infections. The comparison of the 11% of trauma and 13% of general surgery patients who developed ICU infections are shown in the table.
Trauma n = 211
General Surgery n = 56
p-value
General Demographics and Clinical Data
Age
50
62
0.000
Male gender
78%
46%
0.000
ICU days
28
30
NS
Urinary Catheter
100%
95%
0.009
Ventilator
86%
80%
NS
Central Line
63%
88%
0.000
ICU Day of Infection
14
16
NS
Clinical Parameters on First Day of New Infection
Maximum Temperature
38.4
37.7
0.000
Systolic BP
130
121
0.009
Hypotensive
2%
13%
0.002
Heart Rate
95
91
NS
Respiratory Rate
20
21
NS
Blood Glucose
136
132
NS
Leukocyte Count
13.5
15.8
0.013
Fluid Balance >2L
13%
27%
0.020
Type of Infection
Blood
17%
23%
NS
Respiratory
40%
7%
0.000
Urine
19%
36%
0.011
Conclusion: There were significant differences in how new nosocomial ICU infections manifested clinically in trauma and general surgery patients. Routinely collected clinical parameters demonstrated that the general surgery patients appeared sicker on their first day of infection as evidenced by higher WBC count, lower blood pressure, and a significantly positive fluid balance. These findings highlight that an intensivist may need differing thresholds for triggering an infectious workup when rounding in a mixed unit.
The Impact of Patient Workload and Time on Hand Hygiene (HH) Compliance
Introduction: Initiatives to monitor and improve hand hygiene (HH) compliance abound. Hand hygiene is the most effective means of decreasing nosocomial infection rates. Despite increased access to HH stations and institution initiatives to improve HH compliance, rates range from 40–70%. Increased workload (measured by ICU census data, patient assessments, examinations, weekday and time of shift) may impact staff compliance with HH. We hypothesized that HH compliance decreases with increased workload.
Methods: This was a prospective single institution study in which continuous electronic monitoring occurred at all alcohol based gel dispensers and sinks with soap and water in a 20 bed surgical intensive care unit. Hourly reports of HH activity were generated for every day of the week over a 2 week time period. Hours were categorized by day of the week (weekend vs. weekday) and by shift day (7AM to 7PM) and hourly HH rates were calculated per patient based on hourly ICU census. HH events were normally distributed and student's t test and linear regression were used as appropriate.
Results: 26,586 HH events occurred during 15 days of observation with a mean of 1,772 events per day (±362). The mean patient census was 14 (±3.5) with an average of 126 HH events per patient per day. Weekday hours had a higher rate of HH events than weekend hours (79 (±27) vs. 58 (±17), p < 0.01), and dayshift hours (7a-7p) further showed increased HH rates (83 (±24) vs. 65 (±25), p < 0.01). Multivariate regression showed that an increase of one patient to the hourly census accounted for 3.5 additional HH events (95% CI 2.8-4.2), dayshift hours increased compliance by 19 events (95% CI 14.8-23.3) and weekend hours had 6.6 less HH events (95% CI − 12.2, − .98). Other nursing workload factors such as change of shift and times of routine assessments had no impact on the rate of HH events (P > 0.12).
Conclusion: Contrary to the belief that increased workload lends to decreased time for basic hand hygiene, this dataset shows in this single ICU that staff perform HH more frequently with a higher census, during the weekdays and on the day shift. Activities of patient care such as assessment and change of shift do not impact hand hygiene behavior.
BeeTiffany KMDMagnottiLouis JMDSchroeppelThomas JMDCroceMartin AMD
University of Tennessee Health Science Center
BAD Bugs and the Elderly Trauma Patient: An Indicator of Mortality?
Background: Elderly trauma patients have increased morbidity and mortality when compared to their younger counterparts. It has been shown that patients with prolonged intensive care unit (ICU) stays become more susceptible to life-threatening infections (pneumonia and bacteremia) secondary to pathogens such as Pseudomonas aeruginosa, MRSA, Candida spp., Stenotrophomonas maltophilia, and Acinetobacter baumannii. We propose that elderly trauma patents who survive long ICU stays have a lower incidence of these infections compared to their counterparts who do not survive a similar ICU stay. The absence of infection with these pathogens may help us to determine earlier a patient's likelihood for survival and thereby enable us to better counsel families regarding end of life decisions.
Methods: All patients > 64 years old admitted to a Level 1 trauma center from Jan 2004-March 2010 with an ICU LOS > 14 days were analyzed. Data including demographics, severity of injury (as measured by admission GCS and ISS), severity of shock (as measured by 24-hour transfusions and admission base excess), comorbidities, serious infections (ventilator associated pneumonia and bacteremia), microbiology and survival were recorded. Multivariable logistic regression analysis was performed to determine independent predictors of mortality.
Results: 245 patients were identified: 191 patients (78%) survived to discharge, 54 patients died. The two groups were clinically similar in terms of gender, base excess, 24-hour blood transfusions, initial GCS, and ISS. Those who died were slightly older, (77 vs. 72.5; p = .01) and had more comorbidities (2.4 vs. 2.0; p = .01). Developing pneumonia with at least one of these pathogens did not predict mortality. However, mortality was greater for those with at least one episode of bacteremia (p = .05). After adjusting for age, number of comorbidities, incidence of bacteremia and incidence of pneumonia, multivariable regression analysis identified only age as an independent predictor of death in this population (OR = 1.1, 95% CI:.90-.99).
Conclusion: Our data show that there are no reliable factors that can predict death in this cohort other than increasing age. Therefore aggressive treatment should be continued in the critically ill and injured elderly patient even if they develop life-threatening infection. Withdrawal of support should be reserved only for those grave cases.
OlivasAndrea DMDZaborinaOlgaPhDAlverdyJohn CMD
University of Chicago
In Vivo Transformation of Pseudomonas Aeruginosa to a Swarming Phenotype after Anastomosis Formation: A Potential Role in Anastomotic Leak
Introduction: Colorectal anastomotic leak rates continue to be high, especially in those patients who receive preoperative chemoradiation. We have recently demonstrated that rats subjected to fractionated, preoperative radiation followed by a distal colon resection and colorectal anastomosis develop high rates of gross anastomotic leakage (>70%) when they are intestinally colonized by Pseudomonas aeruginosa. The aim of this study was to determine whether strains of P. aeruginosa recovered from anastomotic sites are transformed in vivo to express enhanced virulence.
Methods: Adult, male rats (250–300 g) received fractionated, pelvic irradiation for a total of 25 Gy (5 Gy for 5 days) followed 1 week later by a low colon resection and colorectal anastomosis. At the time of surgery, the bowel was directly contaminated with P. aeruginosa PAO1 via injection into the cecum. An additional group underwent anastomosis formation and P. aeruginosa injection without radiation. Six days after surgery, rats were euthanized, the anastomosis was excised, and P. aeruginosa was isolated from the tissue on selected media. One hundred individual colonies where then sub-cultured from each group and virulence was assessed by observing the ability of bacteria to swarm on semisolid agar, a type of flagella-mediated motility that promotes rapid outward movement of bacterial cells and fast, coordinated colonization, incorporation within the host cell membrane, and disruption of epithelia. Recovered strains were then compared to the stock parental strain initially used to colonize the rats. Random amplification of polymorphic DNA (RAPD) fingerprinting was performed to verify that recovered strains were of the same genotype as the original inoculating strain.
Results:P. aeruginosa recovered from anastomoses of rats were confirmed to be from the same genotypic background as the original PAO1 parental strain as shown by RAPD comparison analysis. Swarming assays revealed that P. aeruginosa retrieved from anastomoses consistently swarmed regardless of radiation exposure (86% and 98% of colonies in irradiated and non-irradiated rats, respectively), whereas the stock parental PAO1 strain did not swarm the majority of the time (1% of colonies).
Conclusion: The presence of pathogenic flora as a result of patient complexity, use of antibiotics, and preoperative radiation may play an underappreciated role in anastomotic leaks. Pathogens such as P. aeruginosa appear to undergo in vivo transformation to a swarming phenotype in response to tissue damage, which may enhance their ability to disrupt the healing and tissue integrity of a high risk anastomosis.
Modeling Common TLR4 and Injury- Induced Early Transcription Recovery Themes in Human Leukocytes
Introduction: The tracking of clinical trajectory among critically-ill patients may enhance therapeutic interventions and improve outcomes. Systemic inflammatory responses trigger dose- and time-dependent changes in human peripheral blood leukocytes (PBL) transciptome and cellular bioenergetics. We have compiled a database that includes micrroarays derived from PBL samples that were obtained from healthy subjects challenged with in vivo endotoxin as well as trauma patients. In this study, we hypothesized that early recovery following an acute systemic inflammatory response induced by in vivo endotoxin (LPS) challenge, or sustained inflammatory responses induced by injury/trauma, will elicit changes in expression of genes associated with common transcriptional themes.
Methods: Leukocytes were obtained from adult human subjects. Four subjects received saline, 7 subjects received LPS (2 ng/kg), and 7 subjects received hydrocortisone (3 mg/kg/min) for 6 hours prior to LPS. Trauma patients (n = 5) were accrued from the adult Surgical ICU. Patient blood was first drawn within one to five days of ICU admission and at nine to twelve days later. The leukocytes were analyzed for gene expression using a 8,793 probe microarray platform (GeneChip® Focus, Affymetrix). Chip data CEL files were analyzed using GeneSpring software (Agilent Technologies). Significantly expressed probes were defined as those with a p < 0.05, and ≥ 1.2 fold change from baseline.
Results: We previously identified a group of 488 differentially expressed genes during the peak of LPS-induced systemic inflammatory response and in PBL obtained from trauma patients 0–5 days post admission. Of the 488 genes, 155 genes reversed their expression trends in all trauma patients by 9–12 days post-admission. These genes also demonstrated an early recovery pattern following endotoxin challenge. Ingenuity Pathway Analysis (Ingenuity, Palo Alto CA, USA) classified the 155 selected genes into 2 major modules. One module, including approximately 70 genes, is related to cell death and cell cycle. The second module, including approximately 96 genes, is related to inflammation and inflammatory diseases. Also included among the 150 genes are genes implicated in the regulation of cellular metabolism, transcription factors, and in ribosomal biogenesis and protein synthesis.
Conclusion:In this analysis, we have identified a distinct group of approximately 150 differentially expressed genes that reflect the dynamic recovery phase following either acute (LPS challenge) or chronic (trauma/critical care) inflammatory conditions. These genes may provide a tool for monitoring patient trajectories and provide insight into the cellular pathways indicative of recovery.
BonattiHugo JRMDMillerCarlyMDVellaMichaelMDShiChanjuanMDDiazJoseMDMayAddisonMDNealonWilliam HMDGuyJeffrey SMD
Vanderbilt University
Trimethoprim Associated Hyperkalemia in a Young Trauma Victim
Background: Trimethoprim sulfamethoxazole (TMPS) is a commonly used antibiotic for urinary tract infection, prophylaxis and therapy in a number of settings. Certain pathogens in the ICU setting call for the use of intravenous TMPS as therapy. The sulfa compound associated side effects are well recognized; whereas trimethoprim associated hyperkalemia is less known.
Methods: We report on a 36 year old female motor vehicle crash victim, who sustained severe closed head injury with frontal lobe intracerebral hemorrhage, multiple facial and skull fractures, bilateral posterior arch fractures of C1, and an odontoid fracture.
Results: She was stabilized in our trauma intensive care unit and underwent sequential repair of her injuries. Her course was complicated by pneumonia due to by Stenotrophomonas maltophilia and Acinetobacter spp., for which TMPS therapy was started. Two days after initiation of TMPS therapy, the patient developed polyuria and elevated serum potassium, peaking at 6.1 mg/dl. Kayexalate, insulin, and 40 mg of furosemide were administered, however, her serum potassium declined to only 5.8 mg/dl. TMPS was recognized as a potential cause of the hyperkalemia, the drug was stopped and the serum potassium declined to 4.8 mg/dl within six hours, normalizing after 36 hours. Her pneumonia had improved clinically and the patient recovered from her injuries.
Conclusion: TMPS associated hyperkalemia originates from the compounds chemical similarity to amiloride and amiloride's potassium sparing diuretic action. As noted, this side effect may cause life threatening hyperkalemia and should be recognized by clinicians.
BonattiHugo JRMDMillerCarlyMDHataJessica LynnA VellaMichaelMDMayAddisonMDNealonWilliam HMDShiChanjuanMDGuyJeffrey SMD
Vanderbilt University
Pseudomenbranous CMV Associated Colitis in a Patient with Low Natural Killer Cell Count
Background: CMV disease mainly affects immunosuppressed individuals such as stem cell and solid organ recipients as well as patients infected with human immunodeficiency virus. CMV colitis has been increasingly diagnosed in normal hosts.
Methods: We report on a 52 year old male with a history of significant alcohol abuse, who had been hospitalized with severe bloody diarrhea for 3 months in an outside hospital.
Results: He was transferred to our intensive care unit in septic shock and multiorgan failure with bloody diarrhea and a megacolon on CT-scan. Emergency sigmoid colectomy was performed, however, the patient continued to have bloody diarrhea and subsequently completion subtotal colectomy with ileostomy was performed. On immunohistochemistry a diagnosis of CMV colitis was made; blood CMV PCR was positive, the patient tested positive for anti CMV IgG but non IgM antibodies. Ganciclovir was started and his CMV PCR became negative within one week. The patient developed multiple other complications but ultimately recovered from the infection. A very low NK cell count (<1%) was found on immunological work up, the patient tested negative for HIV.
Conclusion: CMV colitis is a rare disease in the non immunocompromised host; it is tempting to assume that the low NK cell count, which has been associated with alcohol abuse and increases the risk of CMV disease, was responsible for the inability of the patient to control the latent CMV infection.
KrzyzaniakMichaelMDDangXitongPhDBairdAndrewPhDEliceiriBrianPhDPutnamJamesBSCoimbraRaulMD, PhD
University of California-San Diego
Augurin, an Epigenetically-Regulated Candidate Tumor Suppressor, is Present in Normal Blood Mononuclear Cells (PBMC) and Polymorphonuclear (PMN) Leukocytes: Implicates for Surgical Infection and Immunity
Introduction: Investigators have long suspected that the molecular changes that characterize the host response to infection resemble, and are sometimes nearly identical, to those observed in the host response to cancer. To this end, we mined publicly available cancer gene expression databases for candidate genes suspected of being involved in cell transformation – but not yet associated with the homeostatic response to infection. We report the identification of a gene called Ecrg4 that encodes a candidate extracellular tumor suppressor. We show that its product, called “augurin” is found in peripheral blood mononuclear cells (PBMC) and polymorphonuclear (PMN) leukocytes, and that its expression in these cells is inversely related to methylation of its promoter.
Methods: DNA hypermethylation of the Ecrg4 promoter was measured using a methyl profiler kit (SA Biosciences qPCR Primer Assay for Human C2orf40). Real Time PCR was performed using primers that were designed to quantitatively measure the expression of Ecrg4 and used on cDNAs prepared from mRNA isolated from 14 human cell lines and fresh human PMN and PBMCs. Immunoblotting for augurin was performed using antibodies generated in chickens using the recombinant protein as antigen.
Results: We found the levels of gene expression in most cancer-derived cell lines to be low to undetectable. In contrast, an established human cell line originally derived from a cancer of leukocytic lineage, (Jurkat cells), expressed 5–10 fold more mRNA then any other cell in culture examined (Figure 1). For this reason we examined gene expression in purified PMN and PBMC from normal human volunteers and found that gene expression was 100–400 times higher than in cultured cells (Figure 1). Just as the levels of Ecrg4 promoter methylation are elevated in the cancer cell lines when gene expression is low, this methylation is virtually absent in normal PMN and PBMCs. Immunoblotting with antibodies to augurin confirmed the presence of protein in PMN, PBMC, and in human blood.
Conclusion: The findings described here are the first report of Ecrg4 gene expression in PMN and PBMC, the first to demonstrate that augurin is present in blood, and the first to evaluate the levels of DNA methylation of its gene in peripheral blood cells. These data suggest the possibility that this blood-borne candidate tumor suppressor may play a role in the biological responses classically attributed to PMN and PBMCs and specifically in inflammation and immunity.
NorburyKenneth CPhDShahShinil KDOJimenezFernandoMSWalkerPeter AMDUrayKaren SPhDCoxCharles SMD
Kinetic Concepts, Inc.
Using Flow Cytometry to Measure Signaling by Peripheral Blood Leukocytes through CD11B/CD18 Receptors During Sepsis in a Porcine Model
Introduction: The systemic inflammatory response associated with traumatic injuries and sepsis can result in disruption of vascular permeability and subsequent pathophysiological derangements that may contribute to the development of abdominal compartment syndrome, multiple organ failure, and death. The ability to detect potentially lethal progression of inflammation following injury and sepsis is of paramount clinical importance. Activation of polymorphonuclear cells (PMNs) resulting in expression of surface adhesion markers (CD11b and CD18) and subsequent activation are intricately involved in injury related inflammation. We hypothesize that ascites is capable of activating naïve neutrophils (NEU) and that measuring the NEU priming capability of ascites could be a useful way to monitor progression of systemic inflammation and treatment effectiveness.
Methods: Injury was induced in 10 female Yorkshire swine via intestinal ischemia/reperfusion and induction of intra-sepsis by placement of a fecal clot in the peritoneal cavity followed by abdominal closure. An additional 6 swine were not injured and served as controls. Peritoneal fluid was collected from controls and from septic swine after 12 hr of injury. Naïve human PMN's were primed with swine peritoneal fluid and then activated with fMLP (n-formyl-met-leu-phe) or PMA (phorbol 12-myristate 13-acetate). Flow cytometry was used to quantify PMN superoxide anion production and PMN surface adhesion marker expression of integrins (CD11b, CD18).
Results: Periotoneal fluid primed neutrophils from septic swine showed significantly increased CD11b and CD18 expression and superoxide production via receptor dependent (fMLP) and receptor independent (PMA) mechanisms compared to control uninjured swine (p < 0.05).
Conclusion: Ascites from septic swine induced a pro-inflammatory signal in peripheral blood naïve neutrophils as measured by flow cytometry expression of cell adhesion molecules and superoxide production. Detection of this signal may serve as a useful diagnostic approach to aid in the early determination of the severity of the inflammatory response in traumatic injury and sepsis and as a means of monitoring effectiveness of interventions.
NorburyKenneth CPhDCollinsBarbara ABS, RVTMorminoRichard PPhDKilpadiDeepak VPhD
Kinetic Concepts, Inc.
Comparison of a Novel Negative Pressure Therapy (NPT) System and Standard of Care in a Porcine Model of Sepsis and Gut Ischemia/Reperfusion-Induced Injury
Introduction: Abdominal trauma causes edematous swelling of the intestine that can lead to increased intra-abdominal pressure, which when coupled with secondary organ injury due to a systemic inflammatory response results abdominal compartment syndrome (ACS). ACS significantly increases morbidity and mortality in trauma patients. To relieve abdominal pressure a laparotomy is often performed with the wound remaining open for days, which can increase the potential for co-morbidities the longer it takes to close the abdomen. This study compared the application of a novel system for delivering negative pressure therapy versus a standard of care (SOC) to the open abdomen using a clinically relevant porcine model combining ischemia, reperfusion, and sepsis.
Methods: Injury was induced in 12 female domestic swine (n = 6/group) via intestinal ischemia/reperfusion and induction of sepsis by placement of a fecal clot in the peritoneal cavity followed by abdominal closure. After 12 hours, treatments lasting up to 36 hours were initiated, specifically either ABThera™ Open Abdomen Negative Pressure Therapy (NPT; Kinetic Concepts, Inc., San Antonio, TX) or Bogota Bag without negative pressure (SOC). Animals were monitored throughout the study, including cardiopulmonary physiology, intra-abdominal pressure, clinical pathology, tissue edema, and terminal histopathology.
Results: The log-rank test was performed for comparing the survival data in this study. The Odds ratio was 4, indicating that survival was 4 times higher in the NPT group than the SOC group. Intra-abdominal pressure (IAP) was generally lower in the NPT group compared to SOC. Lung function as measured by PaO2/FiO2 showed a statistically significant difference between the groups, with the NPT group being higher than the SOC group (p < 0.05). No other statistically significant differences were observed.
Conclusion: In a porcine model of sepsis coupled with ischemic and reperfusion injury ABThera™ Open Abdomen Negative Pressure Therapy was demonstrated to increase survival, while reducing IAP and secondary organ injury (lung) compared to the Bogota bag technique, a standard of care that does not utilize negative pressure.
IyeghaUroghupatei PMDAsgharJavariahMD, MPHStatzCatherineRN, MPHGloverJames JBSBeilmanGreg JMD
University of Minnesota
Increasing Incidence of Surgical Site Infections Due to Resistant Organisms
Introduction: Methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococcus (VRE) are nosocomial pathogens that represent a broader pattern of increasing antimicrobial resistance and a source of significant morbidity and mortality. Many risk factors exist for the development of antimicrobial resistance, including exposure to broad-spectrum antibiotics. Such antibiotics are routinely administered prior to surgical procedures to prevent surgical site infections (SSI). In addition, community acquired MRSA has increased in incidence over the past decade and has been responsible for an increasing number of hospital-acquired infections. We hypothesized that the incidence of SSI in which multi-drug resistant isolates are present, particularly MRSA and VRE, is increasing in light of these observations.
Methods: We performed a retrospective review, utilizing a database prospectively maintained by our institutional SSI surveillance program. The SSI rate for several surgical disciplines was obtained over a 5-year period, 2005–2009. We calculated the rate of SSI in which MRSA and VRE isolates were present.
Results: A greater than 6-fold increase in surgical site infection with VRE isolates was observed in transplant operations in 2009. Cardiac surgery was associated with a high rate of MRSA + SSI in 2007 and 2008 (16.7% and 12.5%, respectively) although the rate decreased the following year. Similarly, neurosurgical operations experienced a 25% rate of MRSA + SSI in 2008. This rate decreased the following year, coinciding with an intensive perioperative infection control effort. The decrease in MRSA + SSI in orthopedic operations over the same time period (17% in 2008 compared to 7.4% in 2009) was also attributed to this effort.
2005
2006
2007
2008
2009
All Surgical Procedures
SSI rate (%)
3.4
2.9
1.9
2.2
2.5
% VRE+ SSI
0.9
2.9
3.9
1.9
5.2
% MRSA+ SSI
5.0
7.7
5.2
9.6
5.5
General
SSI Rate (%)
4.3
3.3
2.4
3.0
3.3
% VRE+ SSI
0.0
3.0
7.4
2.9
5.7
% MRSA+ SSI
4.2
9.1
2.1
6.5
8.3
Neurosurgery
SSI Rate (%)
1.6
2.2
2.3
1.9
2.4
% VRE+ SSI
0.0
0.0
0.0
0.0
0.0
% MRSA+ SSI
0.0
5.6
0.0
25.0
0.0
Orthopedics
SSI Rate (%)
2.6
1.3
0.9
1.0
1.0
% VRE+ SSI
0.0
0.0
2.5
1.9
0.0
% MRSA+ SSI
15.6
15.6
12.5
17.0
7.4
Cardiac
SSI Rate (%)
2.4
2.6
2.4
2.9
3.4
% VRE+ SSI
0.0
0.0
0.0
0.0
4.8
% MRSA+ SSI
0.0
0.0
16.7
12.5
4.8
Transplant
SSI Rate (%)
8.5
10.6
7.1
6.4
8.6
% VRE+ SSI
5.7
9.3
3.4
4.3
27.6
% MRSA+ SSI
2.9
0.0
0.0
0.0
0.0
Conclusion: Although the overall rate of SSI has remained stable, the incidence of multi-drug resistant isolates in SSI is increasing. In specific surgical cohorts, an increase in MRSA and VRE isolates is seen. This change may be attributable to changes in the selection of preoperative antibiotics, although improvements were noted following intensive perioperative SSI prevention efforts. The growing incidence of multi-drug resistant isolates mandates routine culture of SSI to allow for appropriate antimicrobial therapy. Preoperative screening for MRSA colonization should be considered to identify patients at risk for MRSA + SSI.
SchulmanCarl IMD, MSPHKuchkarianFernandaMPHWithumKellyBSDuncanRobertPhD
Univ of Miami Miller School of Medicine
Antimicrobial Fabric Technology Reduces Bacterial Contamination: A Novel Infection Control Approach
Background: Healthcare-associated infections account for an estimated 1.7 million infections and 99,000 associated deaths each year in American hospitals (CDC). Recent studies have shown that textiles, specifically clothing worn in healthcare settings, may contribute to the build up and spread of bacteria. We hypothesized that scrubs treated with antimicrobial technology would decrease the amount of bacterial contamination in an ICU setting.
Methods: A prospective, observational study was conducted to test the effectiveness and durability of scrubs made with antimicrobial fabric in reducing bacterial colonization. The fabric was treated with hindered amine technology that can be durably bound to a textile substrate and charged with EPA-registered chlorine bleach, allowing it to act as a reservoir of chlorinated amines available for continuous antimicrobial activity. A four week trial was conducted at a Level 1 Trauma Center. Eighty-six scrubs were worn by 39 trauma intensive care unit nurses. The scrubs were constructed with treated fabric on one side (i.e. left or right) and untreated (control) fabric on the other side. The side of treatment was randomized and blinded to the nurses, the on-site study team and the microbiological team. The fabric was subjected to different wash frequencies (1, 25 and 50) in order to test the durability of its antimicrobial activity. After being worn by the nurses during a 12 hour shift, scrub patches were sampled from both the treatment and control sides and were sent for microbiological analyses. Three sites were sampled on each side of the front of the scrub tops (chest, waist, lower pocket) and two sites on each side of the scrub bottoms (thigh, knee). Repeated measures two-way Analysis of Variance (ANOVA) was used with two grouping factors (week number and side of treatment) and with two repeating factors (treated/ untreated and the scrub sample position).
Results: The total aerobic bacteria CFU (SE) for treated versus untreated scrub shirts were 6.57 (0.14) and 6.96 (0.13) respectively (p = 0.023). For the scrub pants, treated versus untreated total aerobic bacteria CFU (SE) counts were 5.06 (0.17) and 5.49 (0.14) (p = 0.0018). There was a reduction in bacterial load on the treated versus untreated sides throughout the different weeks (p = 0.001), however, the effectiveness of the fabric decreases with the number of washes (week 1, 1 commercial wash, p = 0.045; week 2, 25 washes, p = 0.034; week 3, 50 washes, p = 0.12).
Conclusion: The use of hindered amine technology in scrubs worn in the ICU was effective at decreasing bacterial colonization. This suggests a potential benefit in the area of infection control and highlights the need for a larger-scale effectiveness study. Applying antimicrobial fabric technology to hospital textiles would be a cost-effective and minimally disruptive intervention.
HoffmanMarcus KMDDarwicheSophie SMDKohutLauryn KMABilliarTimothy RMD
Univeristy of Pittsburgh
Mice Subjected to Severe Peripheral Trauma are Resistant to Pseudomonas Pneumonia at 24 Hours
Introduction: Nosocomial infections following trauma are a major source of morbidity and mortality. Research in serum cytokine levels has revealed a pro-inflammatory state following trauma and sterile injury. In a model of sterile trauma simulating bilateral femur fractures, our lab has previously shown serum levels of inflammatory cytokine interleukin-6 being elevated at 24 hours following injury. There has been little in vivo research investigating resistance to infection following trauma. We hypothesized that during this pro-inflammatory state, mice would be more resistant to death following pneumonia and sepsis.
Methods: Utilizing a trauma model of pseudofracture, anesthetized C57BL/6 mice were subjected to soft tissue crush injury followed by injection of bone solutions to bilateral hind limbs. At 24 hours following injury, mice were anesthetized before receiving intratracheal inoculation of Pseudomonas aeruginosa strain M57-15, approximately 1.7 × 107 colony forming units (CFU) per inoculation. Intratracheal inoculation was achieved by sterile incision and blunt dissection, followed by injection with 29-gauge syringe of 35μl of bacteria grown to log phase, pelleted and resuspended in 0.9% normal saline. Mice were randomized to inoculation (n = 12), pseudofracture followed by inoculation (n = 12), or pseudofracture alone (n = 8). Mortality was defined as death in the first 48 hours following Pseudomonas inoculation. At 48 hours after inoculation, mice were sacrificed. Blood, bronchoalveolar lavage (BAL), and right lung were collected and cultured.
Results: Mice subjected to pseudofracture alone had no mortality. The group of mice subjected to Pseudomonas inoculation alone had a mortality of 87.5%. Mice that underwent Pseudomonas inoculation 24 hours after injury by pseudofracture had a mortality of 50%. Interestingly, mice subjected to pseudofracture followed by inoculation that survived to time of sacrifice had an average of 2.2 × 105 CFU/mL of Pseudomonas in their blood while surviving non-pseudofractured inoculated mice had no positive blood cultures. Similarly, pseudofractured mice inoculated had BAL of 2.7 × 105 CFU and right lung had 1.3 × 107 CFU on average whereas non-pseudofractured inoculated mice had means of 170 CFU per BAL and 6.6 × 103 CFU per lung.
Conclusion: In our model of sterile traumatic injury, there appears to be a trend toward a survival benefit in mice exposed to a highly lethal inoculation of Pseudomonas aeruginosa at 24 hours post-injury. Surviving mice in this model of injury and infection appear to tolerate higher bacterial loads in blood and lung as compared to mice that underwent Pseudomonas inoculation alone.
RodriguezNoe AMDFinnertyCeleste CPhDLeeJong OMDHegdeSachin DMDHerndonDavid NMD
Department of Surgery, The University of Texas Medical Branch and The Shriners Hospitals for Children, Galveston
ICU-Acquired Pseudomonas Aeruginosa and Acinetobacter Baumannii are Independent Predictors of Mortality Post Burn
Introduction: The objective of this study was to determine the impact of Pseudomonas aeruginosa (PA) and Acinetobacter baumannii (AB) on survival of pediatric burned patients. The effect of these infectious agents on post-burn mortality has been inconclusive. We hypothesized that acquisition of PA or AB, during the acute period post-burn, is associated with higher in-hospital mortality.
Methods: Data collection was performed on all admissions to a single pediatric burn ICU from December 1999 to December 2009. Samples were taken three times per week. If microbial growth was recognized at any point during the in-hospital stay, a Siemens MicroScan Gram Negative MIC/Combo panel was used for identification and susceptibility of PA and AB. Patients with positive cultures were compared to those with negative cultures during the study period. Primary outcome was in-hospital mortality. Multivariate logistic regression was performed to determine the odds ratio of AB and PA associated deaths. Statistical significance was set at a P value of < 0.05.
Results: There were 1317 patients included in the study. 389 patients were found to have positive cultures for PA, 224 patients were positive for AB. The unadjusted mortality rate for patients with AB was 10.3% and 2.3% for those without. AB was a predictor of in-hospital mortality (odds ratio, 3.2; 95% CI, 1.7-6.0; P < 0.001). PA does seem to be an important independent predictor of mortality when controlling for AB (odds ratio, 3.3; 95% CI, 1.7-6.2, P < 0.001). Additionally, 34 patients were found to have AB positive cultures of blood and catheter tips, their in-hospital mortality rate was 29%.
Conclusion: During the acute period of severe burns, acquiring PA or AB is independently associated with increased in-hospital mortality. The role of PA and AB as causative factors or rather markers of severe illness remains uncertain.
AsgharJavariah IMD, MPHIyeghaUroghupatei PMDStatzCatherine LRN, MPHGloverJames JBScChipmanJeffrey GMDBeilmanGregory JMD
University of Minnesota Dept of Surgery
Institutional Surgical Site Infection Programs are Complementary to American College of Surgeons National Quality Improvement Program for Monitoring Epidemiologic Changes in Surgical Site Infections
Background: The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) is among the first national, validated, multi-specialty programs for assessing risk-adjusted surgical outcomes and improving 30-day morbidity and mortality associated with surgical outcomes, including surgical site infections (SSIs). At present, ACS NSQIP lacks data to bridge the gap between process measures and surgical outcomes. Our goal was to compare relevant SSI surveillance measures between data collected for our institutional SSI surveillance program and that collected for ACS NSQIP at the same institution.
Methods: Using both ACS NSQIP methodology and our long-standing SSI surveillance program, we conducted a prospective, cohort study of general and vascular surgery procedures conducted at the University of Minnesota, Fairview (UMMC-F) in 2009 associated with known SSI. All patients were followed for 30-days post-operatively or one year in case of an implant. Our hospital program assessed SSIs in inpatients and outpatients based on microbiology reports, physician surveys, SafetySurveillor®, referral calls from area hospitals, and International Classification of Diseases-9 (ICD-9) codes reported by the hospital. ACS NSQIP data collection included chart review and patient phone calls. SSIs were compared using the two methodologies.
Results: 3252 patients were followed through UMMC-F surveillance program, while ACS NSQIP evaluated 1765 patients during the same time-period. ACS NSQIP identified a higher percentage of SSIs. More diabetic patients and fewer smokers were identified with facility-led data. While continuous data were collected through the hospital surveillance program and were available monthly, risk-adjusted data from ACS NSQIP lagged by 10 months.
Characteristics of ACS NSQIP and UMMC-F Facility-led Program on SSIs in 2009
ACS NSQIP
UMMC-F
N = 1765
N = 3252
SSI 152 (8.6%)
SSI 156 (4.8%)
SIP %
DIP %
OSI %
SIP %
DIP %
OSI %
SSI
3.7
2
2.8
1.9
0.6
2.2
Age (y)
51.2
52
53.8
51.3
58.3
53.1
BMI (kg/m2)
29.8
29.9
29.5
30.2
27.7
28.7
Smoker
37.3
42.9
28
24
35
24.6
Diabetic
16.4
11.4
16
22
30
39.7
Wound Culture
No record
Recorded
Lag time
10-months
1-month
SIP: superficial incisional primary infection.
DIP: deep incisional primary infection.
OSI: organ space infection.
Conclusions: ACS NSQIP captures a higher percentage of SSIs. However, a significant lag-time currently precludes utilization of ACS NSQIP for rapid program improvement for SSIs. Complementary use of both programs permits comprehensive and rapid evaluation of evolving epidemiologic changes in SSIs.
CastleShannon LMDBernardJessica KBSWilliamsMonicaBSGrishinAnatoly VPhDFordHenri RMD, MHAFreyMark RPhD
Childrens Hospital Los Angeles
ERBB4 is Upregulated in a Mouse Model of Necrotizing Enterocolitis
Introduction: ErbB4 is a recently described member of the receptor tyrosine kinase family that includes the epidermal growth factor (EGF) receptor. EGF administration has been shown to decrease the incidence of NEC in a rat model. However, the expression and function of the ErbB4 family of receptors in NEC is not known. We have previously demonstrated that ErbB4 is upregulated in an adult model of mouse colitis and protects against apoptosis in vitro. We hypothesized that ErbB4 may be upregulated in experimental NEC.
Methods: Enterobacter sakazakii (ES), a pathogen that has been associated with clinical outbreaks of NEC, was used to induce NEC in neonatal mice. Wild-type FVB newborn mice were administered 107 cfu ES or equivalent volume of saline at 12 hours of age and allowed to nurse with their mothers. Animals were euthanized upon development of signs of NEC (abdominal distension, profuse bleeding or diarrhea, cyanosis, lethargy), and control litters at the same time point. Pathology specimens were scored from 0 (normal) to 4 (severe) based on epithelial sloughing, ulceration, neutrophil infiltration, and presence or absence of gross perforation. ErbB4 expression was quantified by immunofluorescence microscopy and by Western blot analysis of terminal ileum.
Results: 7/15 of the mice developed severe clinical and morphological evidence of severe NEC by day of life 1 (Pathology scores 3.5 + /-0.5). None of the control animal developed signs of illness. Immunofluorescent analysis of intestinal sections showed increased ErbB4 levels in the intestinal epithelium of mice that developed NEC after treatment with ES. Quantitative Western blot analysis of ileal homogenates demonstrated a 4-fold increase (p < 0.001) in ErbB4 protein levels with ES infection.
Conclusion: ErbB4 is upregulated in the intestinal epithelium in a mouse model of NEC. As in the adult colitis model, this could be a compensatory mechanism to attenuate the inflammatory response and the degree of epithelial injury in NEC. Thus, ErB4 may represent a possible therapeutic target to prevent or attenuate the development of NEC.
BantonKaysie LMDStatzCatherine LRN, PHN, MPHChipmanJeffrey GMDGloverJames JBSBeilmanGregory JMD
University of Minnesota
Antiseptic Wound Care Policy Contributes to Reduction of SSI's And Increased Transplant Survival
Introduction: Improvement in surgical patient morbidity and mortality is now a measure of hospital quality of care. Reduction and even elimination of surgical site infections (SSI's) is now connected with healthcare reimbursement by CMS and addressed by the SCIP guidelines. Not only does lowering rates of wound infections translate into improved patient outcomes, as a secondary benefit, rates of drug-resistant bacterial infections result in fewer serious infections and a reduction in the spread of nosocomial infections to our non-surgical patients.
Background: Several factors contribute to wound infections including bacterial inoculums, host defenses and extent of wounding/tissue damage. Some of our most serious infections arise in the background of iatrogenic immunosuppression of transplant surgery. In 1995, our Transplant surgeons implemented an Antiseptic Wound Care policy which includes a strict antiseptic pre-procedure shower protocol. This was followed by a structured study in pancreas transplant patients (1997) and finally adopted as a hospital-wide policy in 2001. Our null hypothesis is that a strictly followed Antiseptic Wound Care Policy with a pre-operative shower will have minimal impact on the microbiological make up of our wound infections, morbidity or mortality.
Methods: Prospective collection of wound infection surveillance data and patient mortality rates at one year of 6,334 transplant cases from January 1, 1993 to December 31, 2008. We compare initial microbial isolates from 534 SSI's during this period to the isolates reported by NHSN from Transplant SSI's.
Results: During the course of data collection, our overall organ transplant wound infection rate was 8.4% as compared to CDC report of 7.2% over the same time period. We did observe a 71% drop in transplant first year mortality as the wound infection rates dropped from 22% to 6.5% during the first 3 years after our Antiseptic Wound Care Policy was enacted. The rate of VRE wound infections in transplant patients as reported by NHSN over the approximate same period is 10% although unpublished reports find over 25% VRE wound infections in this population. Our rates of VRE were 0% pre-Antiseptic Wound Care Policy and 5.5% post implementation which corresponds to the emergence of VRE nationally. Our rate of MRSA during this study period was 1.6% and was statistically similar to our pre-policy rate. The other microbial make up of our multi-organism deep wound infections did not change. We also did not observe the emergence of ESBL wound infections during the course of the study period.
Conclusion: Careful adoption of an Antiseptic Wound Care protocol especially in immunosuppressed patients can result in a dramatic decrease in SSI incidence, pathogen resistance, morbidity and 1 year mortality. Strict adherence to antiseptic showering and wound cares can effectively improve our surgical patient outcomes and nosocomial infection rates.
DarwicheSophie SMDHoffmanMarcus KMDPribisJohn PBScZhuXinmeiPhDOchoaJuan BMDBilliarTimothy RMD
University of Pittsburgh
Pseudofracture: A Model for Late Post-Traumatic Immunosuppression
Introduction: Severe injury can lead to immunodepression rendering trauma patients more susceptible to infections. This immunodepression is manifested by a suppression of T cell function and is most often measured by in vitro assays on cells isolated from injured animals in the experimental setting. We previously developed a model of severe peripheral tissue trauma referred to as the pseudofracture (PF) model. In this model anesthetized mice are subjected to muscle crush followed by the injection of crushed syngeneic bone to simulate femur fracture. We have shown that this results in depressed splenocyte responses to mitogens in vitro. To characterize T cell responses in vivo we assessed the host response to Listeria Monocytogenes (LM) infection following PF. LM infection in cleared through mechanisms known to require T cells.
Methods: Male C57BL/6 mice, age 8–12 weeks, underwent the pseudofracture trauma model (PF = bone solution injection and crush injury to the thigh musculature bilaterally) or no experimental manipulation (C = control). One hour later all mice received an inoculation of 5 × 105 CFU of Listeria Monocytogenes by intraperitoneal injection. At 72hrs spleen and liver were harvested for evaluation of bacterial loads. Experimental groups had a sample size of n = 6. Statistical significance (p < 0.05) was assessed by Student's t-test.
Results: At 72hrs there was a statistically significant increase in bacterial loads in the liver from mice that underwent pseudofracture in comparison to control mice (PF = 5.29 ± 1.30 log10CFU/liver vs. C = 3.05 ± 0.66 log10CFU/liver). A similar statistically significant increase was found in the spleens of PF in comparison with the spleens from the control mice (PF: 5.68 ± 0.60 log10CFU/spleen vs. C: 3.83 ± 0.47 log10CFU/spleen). No mortality was seen in the group of control mice, however, in comparison there was a 33% mortality rate in the PF mice at 72hrs.
Conclusion: Significantly increased rates of Listeria Monocytogenes infection following pseudofracture trauma demonstrate an increased susceptibility to infection in vivo following trauma which corresponds with previously identified cellular dysfunction in this model.
GyangElsieShiehLisaMD, PhDForseyLynnRN, PhDMaggioPaulMD, MBA
Stanford University
A Simple Screening Tool for the Early Identification of Sepsis in a Non-ICU Setting
Introduction: Despite advances in the management of septic patients, the mortality from septic shock remains > 50%. Timely implementation of goal-directed therapy has been associated with improved patient outcomes and decreased sepsis-related mortality, highlighting the importance of early sepsis recognition. While the majority of studies have focused on screening tools for early sepsis in the critically ill patient population, less has been reported in the non-ICU setting. We hypothesized that a simple sepsis-screening tool performed by nursing staff could accurately identify early sepsis in both surgical and medical patients in a non-ICU setting. A pilot study was initiated to investigate the accuracy of a simple three-tiered screening tool. We examined the tool's sensitivity and specificity in a non-ICU environment and characterized its performance in both surgical and medical patient populations.
Methods: Patients admitted to a medical/surgery unit were screened with a three-tiered sepsis-screening tool every 8 hours by our nursing staff. In preparation, nursing staff were provided additional training to identify new infection and assess for organ dysfunction. The initial screen identified the (SIRS) systematic inflammatory response parameters (HR, temperature, WBC, and RR). If there were > 2 SIRS, the nurse would assess for suggestion of new infection. If the patient had both > 2 SIRS and new infection, the nurse would identify and record any evidence of organ dysfunction. If the patient screened positive for sepsis (>2 SIRS and new infection) or severe sepsis (sepsis with end organ dysfunction), the primary treatment team was notified and their action recorded. All patients with ICD-9 codes for sepsis, severe sepsis and septic shock were identified during this one-month time period. In addition, all screened patients underwent a chart review.
Results: Over a one-month period 2,143 screens were completed in 245 patients (169 surgical, 76 medical). The prevalence of sepsis was 8.6% in the pilot unit during the same time period. Overall, the screening tool yielded a sensitivity of 95%, and a specificity of 92%. In the medical patient population the sensitivity was 100% and the specificity 95%. In the surgical patient population the screening tool yielded a sensitivity of 93% and a specificity of 90%.
Conclusion: A simple screening tool performed by nursing staff can accurately identify early sepsis in both medical and surgical patients in a non-ICU setting. We identified a trend towards a higher sensitivity and specificity for our screening tool in the medical population compared to the surgical population, although these findings need to be validated in a larger study. Our data suggest that a simple screening tool for sepsis may provide a means to successfully identify early sepsis in a non-ICU setting.
MaishGeorge OMDWoodChrisPharmDBeeTiffanyMDZarzaurBenjaminMDMagnottiLouis JMDSchroeppelThomasMDMinardGayleMDCroceMartin A.MDFabianTimothy CMD
University of Tennessee Health Science Center, Memphis
Linezolid Insensitivity in Bacterial Isolates from Trauma Patients: An Uncommon Occurrence?
Introduction: Drug-resistant microorganisms are a significant cause of infections, resulting in increased length of ICU stay, increased hospital days, and death for patients. Gram positive organisms, particularly methicillin resistant Staphylococcus aureus (MRSA) and vancomycin resistant enterococcus are becoming more problematic, since treatment options are limited. Linezolid is an oxazolidinone antimicrobial that is used to treat such Gram positive infections. It was approved by the FDA in 2000. There has been concern that there would be a rapid rise in linezolid resistance with its use because of its bacteriostatic rather than bacteriocidal action.
Methods: A retrospective analysis of sensitivity data from the microbiology lab of a large safety net hospital from 2003–2010 was performed. Those isolates that were tested for sensitivity to linezolid were analyzed. The trauma intensive care unit (TICU) and post-trauma unit (TRAUMA) were compared to the hospital as a whole (HOSP). TRAUMA practices a strict restrictive antibiotic policy regarding empiric and therapeutic antibiotic use.
Results: 1308 isolates in 457 patients were tested for linezolid sensitivity for TRAUMA (2.9 isolates per patient) compared to 6197 isolates in 2445 patients (2.5 isolates per patient). Of the 1308 isolates, only 8 were either intermediate or resistant to linezolid: 5 were Enterococcus faecium (3 from blood and 2 from pleural fluid; all had intermediate sensitivities) and 3 were Staphylococcus epidermidis (2 from central venous catheters and 1 from pleural fluid; all were resistant). The rate of linezolid insensitivity in TRAUMA was 0.6%. For HOSP, the rate of linezolid insensitivity was 2.3% (143 of 6197 isolates; p < 0.0001 vs. TRAUMA). There were 83 linezolid-resistant isolates and 60 intermediate isolates in HOSP. 96 of the isolates were enterococcus (36 resistant), 46 were Staphylococcus epidermidis (46 resistant) and one was Staphylococcus aureus (resistant).
Conclusion: A restrictive, regimented algorithm for antibiotic usage (TRAUMA) results in a low rate of linezolid insensitivity when compared to HOSP. Antibiotic stewardship is crucial for maintenance of linezolid sensitivity.
AhmedNasimMDFACSKuoYen-HongPhDKuoYen-LiangMDDavisJohn M.MD, FACS
Jersey Shore University Medical Center
Risk Factors for Mortality in Patients Admitted with the Primary Diagnosis of Clostridium Difficile Colitis: A Retrospective Cohort Study using Nationwide Inpatient Sample (NIS) Database
Introduction: Clostridium difficile colitis (CDC) is one of the most common enterocolitis in hospitalized patients. Community acquired CDC is on surge as well. Risk factors associated with the disease are old age, prior hospitalization, use of antibiotics. The purpose of this study was to assess the risk factors for mortality in patients who were admitted with the primary diagnosis of CDC using Nationwide Inpatient Sample (NIS) database.
Methods: A retrospective cohort study was conducted to evaluate the mortality risk associated in adult (≥18 years) patients in whom the primary admitting diagnosis was CDC and admitted through emergency room. The ICD-9 code 008.45 was used to retrieve data from the 2006 NIS database. Patients were excluded from this study if the variables of interested were missing. Multiple logistic regression models were used to assess the association between mortality and comorbidity while controlling for potential confounding factors.
Results: A total of 12,610 patients were included in this study. Among them, 442 patients (3.5%) expired. The characteristics are shown in the Table. The expired patients were older, but there was no difference with regard to gender, diabetes status, obesity,or the treating hospital's teaching status. From a multivariable logistic regression in which the age, gender, and major comorbidities were controlled, the following comorbidities significantly associated with the increases of mortality: fluid and electrolyte disorders (odds ratio [OR] = 1.8, 95% confidence interval [CI]: [1.4, 2.4], P < 0.001); congestive heart failure (OR = 1.4, 95% CI: [1.1, 1.7], P = 0.004); chronic pulmonary disease (OR = 1.5, 95% CI: [1.2, 1.9], P < 0.001); renal failure (OR = 2.1, 95% CI: [1.7, 2.6], P < 0.001); weight loss (OR = 2.0, 95% CI: [1.6, 2.5], P < 0.001); Peripheral vascular disorders (OR = 1.4, 95% CI:[1.0, 1.9], P = 0.04); metastatic cancer (OR = 3.5, 95% CI:[2.2, 5.3], P < 0.001).
CHARACTERISTICS n (%)
DISCHARGE ALIVE (n = 12168, 96.5%)
DEATH (n = 442, 3.5%)
P-Value
Age, mean (SD)
70.1 (17.1)
80.8 (10.2)
<0.001
Female
7942 (65)
277 (63)
0.28
Median Household income quartiles
0.002
$1 - $35,999
2715 (22)
94 (21)
$36,000 - 44,999
3034 (25)
87 (20)
$45,000 - 58,999
3170 (26)
109 (25)
$59,000 or more.
3249 (27)
152 (34)
Teaching Hospital
5326 (44)
199 (45)
0.64
Fluid and electrolyte disorders
8182 (67)
366 (83)
<0.001
Congestive heart failure
2289 (19)
158 (36)
<0.001
Conclusion: Major co-morbidities including congestive heart failure, chronic pulmonary disease, renal failure and metastatic malignancies are associated with CDC mortality. Early diagnosis and prompt treatment of CDC may reduce the mortality in this patient population.
CarvalhoCarla MMDBesseyPalmer QMD, MSYurtRoger WMD
Weill Cornell Medical Center
Hyperglycemiaa Early Post Burn has Little Effect on the Risk of Infection and Death
Introduction: Hyperglycemia early after mechanical injury has been identified as a risk factor for infection, death and other adverse complications. Clinical outcome for burn patients has been related to patient age, total burn size (TBSAB), and the presence or absence of inhalation injury (IHI), but the further impact of early hyperglycemia following burn has not been characterized.
Methods: The records of all patients 18 years and older admitted within 24 hours of burn over a two year period were reviewed. Both the first glucose value determined in the laboratory (G1) and the highest glucose value in the first 24 hours of admission (GMax) were recorded. These values in addition to age, TBSAB and IHI were related to death, length of stay (LOS), and the development of at least one infection by logistic and linear regression.
Results: There were 600 patients admitted during the study period. Ages ranged from 18 to 95 (43.5 ± 0.72, Mean ± SEM) and burn size from 0 to 95 % TBSA (6.7 ± 0.5). There were 66 patients with IHI; 85 developed at least one infection; and 26 died. Although 104 patients had an initial glucose > 150 mg/dl, only 57 had a known prior history of diabetes. Age, burn size, and IHI were strongly related to LOS, infection, and death (P < 0.0001), with IHI having the greatest effect (Odds ratio for death 7.32, 95% confidence interval 2.25 – 23.86, P = 0.001). Surviving patients who developed at least one infection had higher initial and maximum glucose values than those who did not (G1 156 ± 8 vs 120 ± 2 mg/dl, P = < 0.0001 and GMax 186 ± 9 vs 131 ± 3, P < 0.0001), and they had a longer LOS (49 ± 5 vs 11 ± 1 days, P < 0.0001). Both G1 and GMax were also related to age and burn size (P < 0.0001), so that their effect on infection may not be independent. Although the highest glucose value within the first 24 hours of admission tended to show a small adverse influence on survival, this did not reach statistical significance (odds ratio for death 1.01, 1.00 – 1.02, P = 0.071).
Conclusion: The major predictors of infection and death after burn in this sample of burn patients were age, TBSAB, and IHI. Hyperglycemia early after burn appeared to have a negligible influence on these clinical outcomes.
FinnertyCeleste CPhDJuHyunsuPhDSprattHeidiPhDVictorSundarJeschkeMarc GMD, PhDHegdeSachinMDBhavnaniSuresh KPhDLuxonBruce APhDBrasierAllan RMDHerndonDavid NMD
University of Texas Medical Branch/Shriners Hospital for Children
Can Proteomics Improve the Prediction of Burns Mortality? Results from Regression Spline Modeling
Introduction: Reliable prediction of mortality in severely burned patients remains elusive. Clinical covariates or plasma protein abundance have been used with varying degrees of success; however, despite the application of many wellness scores to predict burn patient outcome, the triad of burn size, inhalation injury, and age remain the most reliable predictors. Here, we investigated the effect of combining proteomics variables (i.e., serum analyte abundance measured at the time of admission) with these three clinical covariates on the early identification of burn patients who will die.
Methods: Three hundred thirty-two children with total burn surface area (TBSA) exceeding 25%, were admitted and consented to an institutional review board-approved experimental protocol between 1997 and 2008, and required at least one surgical intervention. Serum hormones, acute phase proteins, and cytokines were measured at the time of admission. Mathematical models were used to determine the association of each analyte with patient analyte.
Results: Principal component analysis demonstrated that serum protein abundance and the clinical covariates each provided independent information regarding patient survival. Because analyses using data-driven generalized additive models demonstrated that the relationships between analytes and mortality were not linear, we performed non-linear modeling using multivariate adaptive regression splines (MARS). Combining serum analytes with clinical assessments in MARS-based modeling increased overall outcome prediction accuracy from 52% to 81% and increased area under the receiver operating characteristic curve from 0.82 to 0.95.
Conclusion: These results show that the accuracy of the MARS classifier can be substantially improved by combining protein abundance information with clinical covariates. Future studies will be necessary to validate these findings and overcome the limitations of the current study, which are discussed.
DavisJohn MMDKuoYen-HongPhDAhmedNasimMDKuoYen-LiangMD
Jersey Shore University Medical Center
Surgical Site Infections in Elective Colectomies and CABG: Comparing Age and Hospital Teaching Status using NIS Data 2001-2006
Background: An increase in the surgical site infection (SSI) rate in elective colectomies was reported from studying the Nationwide Inpatient Sample (NIS) database. However, the SSI from coronary artery bypass graph (CABG) during the same period of time was not assessed. The purpose of this study was to assess the SSI from CABG patients and to evaluate the impact of patients' age and hospital teaching status on SSI.
Methods: The National Inpatient Sample database was used to evaluate infections in adult patients (age ≥ 18 years old) for elective colectomies (n = 90,596) and elective CABG (144,642) from the years 2001 through 2006. Annual infection rates were determined for each of the operations.
Results: For CABG, the SSI did not change overtime for both the younger (age < 65 years, P = 0.60) and older (age ≥ 65 years, P = 0.06) at the 0.05 level of significance. When further stratified by the hospital teaching status, there was a trend of SSI increase in the teaching hospital (P = 0.03) for the older group, but not for the younger group (P = 0.89). For the non-teaching hospitals, the SSI did not increase over time (P = 0.65 for older group; P = 0.22 for younger group). For the patients who had colectomy, the SSI increased over time for both age groups and teaching statuses. When comparing the teaching status impact on SSI, there was a difference in the CABG (P = 0.04) and colectomy (P < 0.001) in the older group in 2006. For the younger group, teaching status did not impact SSI in patients having CABG, but teaching status differences were found in colectomy patients in 2001, 2003, 2004 and 2005.
Conclusion: This study identifies differences in the SSI rates among procedure, teaching status and age groups.
RutkoskiJohn DMDGainesBarbara AMD
Childrens Hospital of Pittsburgh, University of Pittsburgh
Ertapenem for the Treatment of Perforated Appendicitis in Children
Introduction: Ertapenem is a frequently used carbapenem in the treatment of adults with mild-to-moderate community acquired intra-abdominal infections. Several randomized-controlled trials have demonstrated the clinical effectiveness of this agent. Its use in children has been less well characterized. We hypothesize that ertapenem will effectively treat the most common intra-abdominal infection in children, perforated appendicitis.
Methods: After obtaining IRB approval, the medical records of all children who underwent an appendectomy and received ertapenem over a two year period at a single tertiary care pediatric institution were examined. During this time, a standard treatment protocol was utilized; primary source control was obtained by laparoscopic or open appendectomy, followed by at least five days of intravenous ertapenem therapy, until patients were afebrile for 24hrs, had return of bowel function, and a normal white blood cell count. Ertapenem was administered according to patient's weight in kilograms and age. Children over 12 years of age received a single daily dose; younger children were dosed twice a day. Standard demographic data was abstracted. Descriptive statistics, student's t-test, a chi square analysis were performed as indicated.
Results: A total of 144 patients met entry criteria. Average age was 9 years, with a range of 2 to 18. 55% were male. Infectious complications included intra-abdominal abscess in 35 (24%) and wound infection in 5 (3.5%).
Conclusion: In this cohort, infectious complications from perforated appendicitis in children appear to be higher than quoted in the literature (13–20%). These findings suggest that caution should be exercised when extrapolating the findings from the adult studies to children. Obvious limitations of this study include its retrospective nature and the lack of microbial specimens from the initial operation. Further studies are needed to evaluate the role of ertapenem in the management of pediatric perforated appendicitis.
KuoYen-HongPhDKuoYen-LiangMDAhmedNasimMDDavisJohn MMD
Jersey Shore University Medical Center
Factors Associated with Postoperative Pneumonia in Patients with Open Lung Resection: A Retrospective Cohort Study using 2006 Nationwide Inpatient Sample
Background: Pneumonia is associated with prolonged length of hospital stay, high mortality, and the increased costs of health care. Identifying the risk factors associated with pneumonia will improve patient care. The purpose of this study was to assess the factors which associated with the risk of developing postoperative pneumonia in patients with open lung resection.
Methods: A retrospective cohort study was conducted by using the 2006 Nationwide Inpatient Sample. Adult patients (≥18 years of age) had elective open lung resection (ICD-9-CM codes: primary diagnosis 162.2 to 162.9, primary procedure 32.3, 32.39, 32.4, 32.49, 32.5 and 32.59) on the day of admission were included in this study. Postoperative pneumonia is the primary outcome (ICD-9-CM codes: 480.x, 481, 482.xx, 483.x, 484.x, 485, 486, 997.31, and 997.39). Multiple logistic regression models were used to assess the association between risk factors with postoperative pneumonia while controlling for confounding factors.
Results: A total of 5,269 patients were included for this study. The postoperative pneumonia rate was 7.5%. A lower proportion of female had pneumonia (Table). There was no difference among the median household income quartiles or the hospital teaching status. From a multiple logistic regression model in which age, gender, and other comorbidities were controlled, the following comorbidities significantly associated with the increased risk of postoperative pneumonia: weight loss (odds ratio [OR] = 4.0, 95% confidence interval [CI]: [2.4, 6.4], P < 0.0001), chronic pulmonary disease (OR = 2.4, 95% CI: [1.9, 3.0], P < 0.0001), coagulopathy (OR = 2.4, 95% CI: [1.3, 4.4], P = 0.007), fluid and electrolyte disorders (OR = 2.3, 95% CI:[1.8, 3.0], P < 0.001) and congestive heart failure (OR = 1.7, 95% CI: [1.1, 2.4], P = 0.01).
CHARACTERISTICS n (%)
No Pneumonia (n = 4874, 92.5%)
Pneumonia (n = 395, 7.5%)
P-Value
Age, mean (SD)
66.8 (10.2)
68.1 (9.5)
0.05
Female
2537 (52)
178 (45)
0.007
Median Household income quartiles
0.94
$1 - $35,999
1135 (24)
90 (23)
$36,000 - 44,999
1244 (26)
100 (26)
$45,000 - 58,999
1209 (25)
104 (27)
$59,000 or more.
1170 (25)
94 (24)
Teaching Hospital
2833 (58)
231 (58)
0.89
Chronic pulmonary disease
2404 (49)
285 (72)
<0.0001
Hypertension
2586 (53)
171 (43)
0.0002
Fluid and electrolyte disorders
581 (12)
115 (29)
<0.0001
Metastatic cancer
1038 (21)
90 (23)
0.49
Diabetes (uncomplicated)
675 (14)
56 (14)
0.86
Deficiency anemias
410 (8)
45 (11)
0.04
Congestive heart failure
208 (4)
38 (10)
<0.0001
Weight loss
61 (1)
29 (7)
<0.0001
Solid tumor without metastasis
133 (3)
18 (5)
0.04
Peripheral vascular disorders
315 (6)
18 (5)
0.13
Hypothyroidism
385 (8)
17 (4)
0.01
Renal failure
141 (3)
15 (4)
0.31
Coagulopathy
53 (1)
16 (4)
<0.0001
Obese
219 (4)
16 (4)
0.68
Conclusion: This study identified major comorbidities which associated with increased risk of postoperative pneumonia. Strategy on managing patients with those conditions can reduce the costs of health care.
MasoodMuhammad FMDParkPaulineMDNapolitanoLena MMD
University of Michigan
Critical Care Resource Utilization in Severe ARDS Patients with 2009 Influenza a (H1N1)
Background: The 2009 Influenza A (H1N1) virus caused severe pneumonia in young adults, with a worldwide pandemic. Some patients developed severe acute respiratory distress syndrome (ARDS) and were transferred to our surgical ICU (SICU) for evaluation for possible extracorporeal membrane oxygenation (ECMO). We examined critical care resource utilization in these critically ill patients with severe viral pneumonia.
Methods: Prospective observational cohort study (2009- 2010) of all patients confirmed with severe ARDS (defined as PaO2/FIO2 ratio < 100) due to 2009 Influenza A (H1N1) viral pneumonia. Critical care resource utilization, including ICU length of stay (LOS), ventilator days, ECMO days, high frequency oscillatory ventilation (HFOV) days, vasopressor use days and continuous renal replacement therapy (CRRT) days.
Results: 37 patients with severe influenza-associated ARDS were admitted to the SICU, 20 males (73%) and 10 females (27%). Mean age was 39.6 years (range 21–57) years. Obesity (BMI > 30) was present in 15 (40%) patients morbid obesity (BMI > 40) was present in 13 (35%) patients. All patients had severe respiratory failure despite advanced mechanical ventilatory support and severe hypoxemia with a median (IQR) PaO2/FIO2 ratio of 56 (48–63), positive end-expiratory pressure of 18 (15–20) cm H2O. Critical care treatment included antiviral and antimicrobial therapy and aggressive ICU support for multiple organ failure (respiratory, renal, cardiovascular). Patients required 705 days of mechanical ventilation (mean 19.1 days). HFOV was used in 21 patients with 115 total HFOV days (mean 5.5 days). ECMO was required in 11 patients with 191 ECMO days (mean 17.4). Refractory hypotension was common and 31 (84%) patients required continuous infusion of intravenous vasopressors with 341 total days and 11 mean vasopressor support days. Acute renal failure was common (25 patients, 68%) and due to concomitant hypotension, most patients required CRRT, with 399 total CRRT use days and 69 intermittent hemodialysis days for a total of 468 days of renal replacement therapy. All survivors but one had full renal recovery. Mean ICU LOS was 20.7 days, total 766 ICU days. Despite aggressive critical care support provided to these patients, 14 patients (38.8%) died during their index hospitalization. Autopsy results confirmed severe bilateral viral hemorrhagic pneumonia, hemorrhagic pulmonary edema, hyaline membranes, acute diffuse alveolar damage, acute hemorrhagic infarction and prominent pulmonary thrombi and hemophagocytosis.
ICU LOS (Days)
Ventilator Days
HFOV Use Days
ECMO Use Days
CRRT Use Days
Vaso-pressor Use Days
Mean (SD)
20.7 (15.7)
19.1 (13.6)
5.5 (4.3)
17.4 (16.6)
16.0 (12.3)
11.0 (10.3)
Median
15
14
4
10
13
8
Range
5–66
5–69
2–22
4–65
3–64
2–48
Conclusion: Extensive ICU resource utilization was required for treatment of these adult patients with 2009 Influenza A (H1N1) viral pneumonia and severe ARDS. These data can assist with critical care preparedness and planning for future pandemics.
RiccioLin M.MDHranjecTjasaMD, MSSawyerRobert G.MD
University of Virginia
Epidemiological Trends in Surgical Infections of the Skin
Background: Surgeons commonly treat two forms of skin infection—surgical site infections (SSI) and complicated skin and skin structure infection (cSSSI). Infections caused by resistant bacteria and healthcare associated pathogens have increased and some have presumed that they affect these two forms of skin infection similarly.
Hypothesis: Since SSI and cSSTI are both forms of skin infection, temporal changes in the epidemiology of SSI and cSSSI should closely parallel one another.
Methods: We reviewed all bacterial and fungal SSI's and cSSSI's occurring in surgical patients at our hospital from 1997 to 2009. Demographic data, comorbid conditions, and details of the hospitalization for all infections were analyzed, including isolate data for both populations and trends in numbers and percentages of gram positive cocci (GPC) and gram negative rods (GNR). Resistant GPCs were defined as methicillin-resistant S. aureus (MRSA) and vancomycin resistant enterococci (VRE). Potential healthcare-associated GNRs included Pseudomonas aeruginosa, Stenotrophomonas maltophila, Enterobacter spp., Serratia spp., Acinetobacter, and Citrobacter spp. Statistical analysis included linear regression models comparing isolate data for both SSIs and cSSSIs.
Results: There were 1756 SSI's and 764 cSSSIs. All-cause in-hospital mortality was 5.9% (N = 84) after SSI and 3.8% (N = 29) after cSSSI. 54% of SSIs (N = 952) and 51% of cSSSIs (N = 394) were diagnosed with no culture data. 1234 pathogens were isolated from SSI and 544 from cSSSI. Trends in percentage of GPCs and GNRs in SSIs and cSSSIs are shown below:
For SSI, there was a decrease in the percentage of GPC isolates, but for cSSSI the percentage of isolates that were GPCs increased. The opposite trends were seen for GNR. Regarding resistance, the percentage of isolated GPCs that were resistant increased for both SSIs and cSSSIs (y = 1.7 x + 14.6 and y = 1.5 x + 10.9 for trend lines, respectively). Simultaneously, the percentage of GNR isolates that were potentially health care associated decreased over time in both SSIs and cSSSIs (y = −0.8 x + 61.7 and y = −0.5 x + 36.8 for trend lines, respectively).
Conclusions: Contrary to our hypothesis, temporal changes in epidemiology have not been similar for SSIs and cSSSIs, at least in terms of proportions of infections caused by GPCs and GNRs. On the other hand, changes in resistance patterns for GPCs and GNRs appear to be similar for SSIs and cSSSIs. Surgeons need to understand their local pathogen epidemiology for both SSIs and cSSSIs and should not assume they are similar.
NosanovLauren BBAMaIrene TMDUppermanJeffrey SMDFordHenri RMD, MHAPierceJames RMD
Keck School of Medicine, University of Southern California
Appendicitis Perforation Rates by Year of Age
Introduction: Although numerous studies on appendicitis cite young age as a predictor for perforation, none has specifically examined perforation rates by age. We hypothesized that there may be a threshold age where the likelihood of perforation decreases. In this study, we examined the relationship of age and other accepted predictors of perforation.
Methods: Following IRB approval, we performed a single-institution retrospective analysis of all children diagnosed with appendicitis from 2004–2010. Patient demographics, pre-operative history and physical, labs, imaging, and intra-operative diagnosis were recorded. Perforation rates by age were compared. Chi-square analysis was used to confirm the threshold separating older and younger children. A multivariate logistic regression analysis was used to identify the independent pre-operative predictors of perforation, using binomial age stratified by our identified threshold.
Results: 1,386 consecutive patients were identified with appendicitis. There was non-linear variation in perforation rates by age (Figure). The threshold in perforation rates occurred between the ages of 4 and 5 years. Children under 5 had a significantly higher perforation rate than children 5 and over (p = 0.0001). There was no difference in perforation rate between children ages 5–10 years and children ages 10–15 years (p = 0.529). Multivariate analysis identified age, days of symptoms, vomiting, and tenderness on palpation as predictors of perforation. Individual perforation rate curves showed trimodal peaks, even when corrected for delay in administering antibiotics and operation, white count, and CRP.
Discussion: The data demonstrate that a threshold age exists that is associated with a higher likelihood of perforation from appendicitis. This is the first study analyzing perforation rates by year of age utilizing an appropriate, rather than an arbitrary threshold, as in previous studies. By utilizing our threshold we can appropriately take age into account when developing protocols used to determine which children should receive CT scans as well as which children should receive non-operative treatment. Our trimodal distribution of perforation by days of symptoms and age differs from a smaller previous report that identified a linear relationship. We suggest that the mechanisms involved in the development of early perforated appendicitis are likely different than those seen in later perforations.
ErcanUtku KBSFridmanGregPhDBrooksAri DMDJoshiSuresh GMD, PhD
Drexel University, Philadelphia
Non-Thermal Floating Electrode-DBD-PLASMA: A Novel Approach to Control Bacteria in Biofilms
Background: The non-thermal, room temperature electrical plasma discharge (also known as cold plasma) operates in open air, which is safe for treatment of fluids, and animate and inanimate surfaces (Am J Infect Control, 2010). Our floating electrode-DBD plasma (Plasma) system is constructed similarly to conventional dielectric barrier discharges, and is inherently non-thermal and able to operate at room temperature and pressure. This plasma operates under conditions where one of the electrodes is a dielectric-protected powered electrode, and the second electrode is a surface carrying organisms, in order to ignite the discharge of cold plasma. Plasma is being investigated for its applications in biology and medicine. Surface contamination by bacterial pathogens in the hospital is a major source of nosocomial infections, and existing methods alone are not sufficient to combat this. Here, we report the findings of plasma-mediated inactivation of E. coli in established biofilm forms, and significant prevention on such biofilms.
Hypothesis: Fluid-mediated plasma inactivates E. coli embedded in established biofilms and prevents such biofilms.
Experimental design: From fresh overnight culture of E. coli, aliquots of 9-, 8-, 7-, and 6-Log10 CFU/mL were prepared in trypticase soy broth (TSB) to generate killing curves. For biofilms, the overnight culture was diluted to 1:100 in TSB and allowed to established biofilms for 24h /37°C (detected by microplate/safranin assay). Phosphate-buffered saline (PBS) was exposed to plasma for various times (amount of plasma energy) and the culture aliquot or biofilm-bearing surface was then treated with it, and processed further for the demonstration of percent surviving cells. In another set, the 1:100 diluted overnight cultures was mixed with plasma-treated PBS and incubated as above.
The standard colony count assay, Safranine assay, XTT assay, and Live/Dead BacLight bacterial viability kit were used for this purpose. The Plasma generator was set to 500 Hz (Power+W/cm2) to deposit energy (J/cm2) of 0 (0 sec), 1.9 (15 sec), 3.9 (30 sec), 7.8 (60 sec), 11.7 (90 sec), 15.6 (120 sec), 23.4 (180 sec), and 39 (300 sec).
Results: Plasma (energy) dose-dependent and bacterial cell density-dependent killing responses were observed in all three conditions of E. coli. To 30 secs plasma exposure (3.9 J/cm2), planktonic forms resulted in about 60%, 89%, 97% and 100% killing of respectively 9-, 8-, 7-, and 6-Log10 cells. Biofilm-embedded E. coli were 100% killed (treatment of biofilms) in 120 sec, and were comparable to 70% ethanol-treated biofilms (for 1h). The exposure of plasma-treated PBS resulted in significant reduction (p < 0.05) in biofilm formation (prevention of biofilms). The findings of colony assay, XTT, and BacLight assay were comparable.
Conclusions: Floating-DBD Plasma is a novel technique which efficiently controls nosocomial pathogens such as E. coli even when present in established biofilms, prevents such biofilms, and has potential of surface disinfection.
O'HanleyPeterPeteMattO'HanleyKellySaboLesAllenRobertStephensJackson TJr.
Exoxemis, Inc. Little Rock, AR and Creighton University School of Medicine
Antibody Responses Not Likely to Affect Efficacy and Safety of E-101 Solution, a Novel Myeloperoxidase (MPO)-based Topical Antiseptic for Prevention of Incisional Infections
Introduction: E-101 is a topical antimicrobial, intended for application to prevent incisional surgical site infections (SSI), which will soon be in Phase 3 testing. E-101, formulated from porcine (p)-MPO and glucose oxidase (GO), has microbicidal effects against all SSI-associated microbes via p-MPO generation of hypochlorous acid and singlet oxygen. E-101 exposure has not been associated with microbial resistance or cross interference with drugs. E-101's safety profile indicates promotion of wound healing and no wound irritation or skin sensitization after administration into experimental wounds or abraded skin. This study evaluated 5 serological tests to assess whether pre-existing antibody or E-101 topical exposure might elicit an antibody response that could affect E-101's efficacy or safety.
Methods:Serological Tests. Serum GO and p-MPO neutralization and serum anti-GO and anti-p-MPO ELISAs were developed and comply with FDA and EMEA guidelines for assessing immunological effects of biologicals. Specific and sensitive (≤ 360 ng of serum antibody/mL) serum assays for assessing neutralization and binding antibodies detected by ELISA were validated using control sera. A validated ELISA test to detect human (h)-MPO antibody (Orgentec), which is the first-step in the diagnostic work-up of peri-nuclear anti-neutrophilic cytoplasmic antibody (p-ANCA)-associated vasculitis, was also employed. Serum Samples. From Phase 1 studies, 283 serum samples collected prior to topical E-101 exposure onto abraded skin, and 288 convalescent samples collected up to 10 weeks after E-101 topical exposure were assessed. A serum sample obtained from a patient with p-ANCA-associated vasculitis was used as a serologic positive for comparison with the Phase 1 samples.
Results: No pre-existing serum neutralization GO or p-MPO antibodies were detected in any Phase 1 subject, and no subjects exposed to E-101 developed serum neutralization antibodies. None of the Phase 1 subjects had detectable pre-existing serum antibodies to p-MPO or GO. E-101 exposure did not elicit any detectable serum antibodies to p-MPO or GO or to h-MPO. Also, there were no pre-existing antibodies to h-MPO among this study population (serological prevalence of antibodies to h-MPO is 0 to 17% among adult populations).
Conclusion: Exposure to topical E-101 during Phase 1 studies did not elicit anti-h-MPO antibody. This suggests that E-101 topical exposure would not be associated with a p-ANCA response (95% exact confidence interval of 0%, 1.3%). Serological data from Phase 1 subjects and the patient with documented p-ANCA-associated vasculitis suggest different binding and functional epitopes for p-MPO antibodies and h-MPO (or p-ANCA) antibodies. The absence of pre-existing neutralization antibodies to GO or p-MPO suggests that it is unlikely that immunologically-based modulation will affect the efficacy of topically applied E-101.