
Abstract

I am reminded of a casual conversation I had with Doctor Kevin Tracey, a brilliant neurosurgeon and scientist, nearly 10 years ago at one of the national meetings. We were reminiscing about the glory days of our residency in the Department of Surgery at New York Hospital–Cornell Medical College (now New York Presbyterian Hospital of Weill Cornell Medical College), when Kevin explained to me that he had reached a point in life where he had shifted his focus from the pursuit of excellence to the quest for significance. This rather thought-provoking theme resonated well with me because all of my life, my overarching desire has been to make the greatest difference possible in my community and in the lives of others. Well, January 12, 2010, became a defining moment in my personal quest for significance—in my overarching desire to make the biggest difference possible.
To put this experience in the proper context, I need to give you some background on Haiti. Prior to the earthquake, Haiti was considered the poorest country in the Western Hemisphere. Nearly 75% of the population earned less than $2 per day, and 50% actually lived on less than $1 per day [1,2]. The unemployment rate was estimated to be around 70%, which is not surprising given the fact that the average gross domestic product (GDP)—the measure of the wealth of an economy—had been negative for most of the past two decades. Approximately 50% of the population was less than 18 years old, the illiteracy rate exceeded 50%, and the average life expectancy was 61 years. According to the World Health Organization, the maternal mortality ratio was 670/100,000 in 2005–2006, making it the second leading cause of death behind human immunodeficiency virus/acquired immunodeficiency syndrome [1–3]. Thus, prior to January 12, 2010, Haiti was already a country “in extremis,” in desperate need of life support. Unfortunately, the earthquake that struck Haiti at 4:53 PM on January 12, 2010, left the country in “full cardiac arrest.” This catastrophic event created an opportunity for many of us to make a big difference.
As President-Elect of SIS, I was extremely proud that many SIS members responded to this crisis in person. Furthermore, members who could not go to Haiti found other ways to contribute to the medical relief effort. Indeed, to a large extent, SIS directly or indirectly helped prepare many of the responders, and particularly your President-Elect, to intervene “… for such a time as this.” For the next few minutes, I want to share with you my personal, life-transforming experience in responding to the call to action following the earthquake.
In the book of Esther, Chapter 4, in the Holy Bible, we find Mordecai, a Jewish aide in the court of the Persian King, Xerxes, who had raised his orphan little cousin, Esther, to become the Queen of Persia. Both Mordecai and Esther had managed to conceal their Jewish identity. When the King passed an edict to exterminate all Jews from Persia on the 13th day of the 12th month (in roughly 11 months), Mordecai challenged Esther to go to the King to try to reverse the decree and prevent the carnage by saying: “…And who knows but that you have come to (your) royal position for such a time as this?” [4]. On January 13, 2010, the day after the quake, as I reflected on my personal journey and where I found myself in contemporary American medicine, I couldn't help feeling that I had spent the first 51 years of my life preparing “for such a time as this,” and SIS played a pivotal role in this preparation.
I emigrated from Haiti to Brooklyn, NY, a few weeks before my fourteenth birthday. After graduating from John Jay High School, I was blessed to be able to attend two of the finest institutions of higher learning in the U.S., Princeton University and Harvard Medical School. From there, I was most fortunate to go to the New York Hospital–Cornell Medical Center for general surgery residency training, where I encountered numerous role models and mentors who figure prominently in the hall of fame of the SIS. These include the late Doctor G. Tom Shires, one of the most revered members of American surgery: A pioneering trauma surgeon who built an amazing department of surgery; Doctor Peter Dineen, one of the founding members of SIS; Doctor Roger Yurt, Past-President of SIS (1991); Doctor Steve Lowry, Past-President of SIS (2008); Doctor Phil Barie, Past-President of SIS (2004); and Doctor John Davis, a permanent fixture in the leadership of SIS. These individuals nurtured me during residency and helped forge the path I was to follow.
The next stop along the journey was the University of Pittsburgh School of Medicine, where I encountered another outstanding role model and teacher who introduced me formally to SIS by asking me to put together the slides for his Presidential address in 1988: Doctor Richard Simmons, one of the foremost authorities on surgical infections. In addition, I met Doctor Tim Billiar, my friend, research partner, mentor, and subsequent Chairman of the Department of Surgery at the University of Pittsburgh and also Past-President of SIS (2006); Doctor Andy Peitzman, an outstanding role model, a long-time member of and contributor to SIS; and finally, Doctor Marc Rowe, my training director, teacher, and colleague at Children's Hospital of Pittsburgh, who had a passion for surgical infections and was a regular contributor to SIS. These role models, whose names are engraved in the annals of SIS, are largely responsible for whatever stature I had achieved in American surgery when the earthquake struck on January 12, with the epicenter situated just a few miles from where I grew up. I was a Haitian-American pediatric surgeon with expertise in trauma and surgical infections who had risen to some modest level of prominence as a member of the Executive Committee of the American College of Surgeons (ACS) Board of Governors, a member of the Executive Committee of the ACS Committee on Trauma, and President-Elect of both the SIS and the Society of Black Academic Surgeons. Thus, when bricks were falling on and hurting little children in Haiti, I realized that I was uniquely qualified to intervene “for such a time as this.”
I left my house on January 9, 2010, to attend the Annual Retreat of the American Board of Surgery in Napa Valley, CA. From there, I traveled to Raleigh-Durham, NC, on January 12 for a visiting professorship at Duke University. I was meeting with one of the residents, Dr. Lindsay Talbot, just before dinner when I received a flurry of text messages, e-mails, and phone calls informing me that a 7.0 earthquake had struck Haiti. My family was concerned because we had not been able to contact my sister and her husband, who live in Port-au-Prince, the capital of Haiti. On returning to the hotel room, I became glued to the television, seeking to learn the extent of the devastation. By the time the images started to circulate on Cable News Network (CNN) and other networks, it was clear that the situation in Haiti was dire: A country that was already on life support had now developed a full-blown cardiac arrest. When we finally heard from my sister the afternoon of the thirteenth, she described the situation simply as “apocalyptic.” By now, it was clear to me that I needed to go to Haiti to help in the medical relief effort. However, I knew it wasn't safe, and I wondered how my wife and children would react when I told them I wanted to go to Haiti.
From Duke, I was scheduled to go to the American College of Surgeons (ACS) offices in Chicago for a meeting of the Executive Committee of the ACS Committee on Trauma. I called home from the airport. The first words from my wife were: “You NEED to go to Haiti.” This wasn't a mere suggestion; it was a simple declarative statement from the Chief Executive Officer (CEO) of the Ford household, Donna, my wife of more than 25 years, and my pillar who has made me the person that I am today. Therefore, even if I had any ambivalence about going to Haiti, I had no choice but to go. Our children, Arielle and Alex, understood the seriousness of the situation, yet they were also very supportive. In fact, the night before I left for Haiti, my daughter's only instruction to me was: “make sure you take a picture with Sanjay Gupta when you meet him.” I laughed and retorted that I was going to provide medical assistance and therefore, there was no way that I was going to meet this famous CNN news correspondent, who had been reporting on the devastation and the grim medical situation in Port-au-Prince. Little did I know that this would turn out to be a prophetic statement. My family clearly helped me get ready “for such a time as this.”
Having received the green light from the CEO of the Ford household to go to Haiti, the next question was how to enter the country, given the fact that the airport was closed. I contacted my friends at the State Department and at the Department of Health and Human Services (HHS). They informed me that the “Feds could use my help” because of my background. However, as I am not a federal employee, it was difficult to arrange transportation for me in an expedited fashion because of logistical challenges. Therefore, I contacted a non-governmental organization based at the University of Miami, Project Medishare, and they offered me a seat on their chartered plane to Port-au-Prince for Saturday, January 16. I informed the CEO of Children's Hospital Los Angeles, Mr. Richard Cordova, and the Dean of the Keck School of Medicine of the University of Southern California, Doctor Carmen Puliafito, of my intention to go to Haiti, and both offered me incredible support for this journey. In fact, Dean Puliafito recruited a team of health care professionals to send to Haiti within fewer than 48 h. Meanwhile, at the ACS offices, I was able to work closely with the new Executive Director, Doctor David Hoyt; the Chairman of the Board of Regents, Doctor Brent Eastman; the Chair of the Board of Governors, Doctor Michael Zinner; and the leaderships of the Committee on Trauma and the American Association for the Surgery of Trauma to issue an immediate call to action to mobilize qualified ACS Fellows to go to Haiti to help in the medical relief effort. I flew from Chicago to Los Angeles to pack and then flew to Miami early on January 16 to board a Project Medishare charter flight to Haiti. When I landed in Miami, I received notification that the Department of HHS wanted me to report to the U.S. Embassy on arrival in Port-au-Prince to work with the Disaster Medical Assistance Team (DMAT) and Immediate Medical Surgical Response Team (IMSuRT) that had been deployed.
First Hours
I went to work within hours after my arrival at the U.S. Embassy, when a six-year-old boy with a distended abdomen and lethargy who had had a ceiling collapse on his lower abdomen presented to our make-shift clinic, a waiting room that had been converted into an infirmary to care for earthquake victims. He had not voided since the earthquake and was unable to walk because of a pelvic fracture. His abdomen was tender with peritoneal signs. He needed an urgent laparotomy, but we were ill-equipped to perform it in the closet that had been converted into an operating room solely for the purpose of doing life-saving amputations. Therefore, the decision was made to transfer the patient via helicopter to the naval aircraft carrier, USS Carl Vinson, which was docked in the Bay of Port-au-Prince. My heart nearly stopped when I was informed that I had to accompany the patient to the aircraft carrier to perform the operation because there was no pediatric surgeon on board. Furthermore, the ship's surgeon had been operating virtually all night on other earthquake victims. I had always said that the only way I would fly on a helicopter is if I were unconscious. However, seeing this child in desperate need of an urgent laparotomy, I was able to garner sufficient courage to overcome my personal fears and fly on the helicopter. Assisted by an outstanding surgical team led by the Vinson's surgeon, Doctor Behrndt, we performed an urgent laparotomy, which revealed close to 3 L of urine in the child's abdomen stemming from a bladder neck injury, as well as signs of peritonitis. We managed the injuries successfully, and he looked quite good postoperatively. The ship's Chief Medical Officer then informed me that he would like me to spend the night on the carrier so that I could assist in the surgical management of other pediatric earthquake victims who were already on board. One of these patients was a twelve-year-old girl who had had a ceiling collapse on her head. She had an infected open scalp laceration, and at the center of the wound, there was a piece of brick impaled or embedded in her skull. She was febrile despite receiving appropriate antibiotics; she needed to have the foreign body removed. We were able to break up the piece of brick into multiple fragments to facilitate removal. We retrieved most of the fragments. However, there was one that was simply inaccessible to us without a craniectomy. I felt ill-prepared to perform such a procedure given my limited neurosurgical experience. Doctor Behrndt had the brilliant idea to contact a certain reporter who had arrived on the island shortly after the earthquake and who claimed to be a practicing neurosurgeon, to see if he would be willing to assist us. Therefore, we contacted Sanjay Gupta from CNN, and he graciously agreed to come aboard the aircraft carrier to assist us. He proved to be a competent neurosurgeon. He performed a craniectomy and retrieved two additional fragments of brick that were pressing on the dura. Of course, one of the principal tasks I had to fulfill was to obey my daughter's previous request: “Make sure you take a picture with Sanjay Gupta when you meet him” (Fig. 1). Once we had completed the operation, it was time to board the helicopter for a pleasant ride back to the island, now that my fear of flying on a helicopter had vanished!

Henri Ford and Sanjay Gupta just before operating on earthquake victim.
Nothing could have prepared me for the magnitude of the devastation, misery, human suffering, and despair I was going to encounter when I landed on the island. The city of Port-au-Prince, where I grew up, was almost completely destroyed. It was simply unrecognizable, as if my memory bank or my brain's hard drive had been erased. The city was buried in or covered with rubble. Virtually all of the governmental buildings, churches, and schools were destroyed; even the most beautiful building in Haiti, the National Palace, was leveled. Port-au-Prince was a city in ruins (Fig. 2). Most of the streets were impassable, blocked by rubble (Fig. 3). Beneath the rubble were buried cars and countless bodies that were already decomposing, sending an unbearable stench into the air. Most people had to wear a mask or pinch their noses in order to avoid the smell. The main hospital in Haiti, the 700-bed Hôpital de l'Université d'Etat d'Haïti (HUEH), had suffered major damage, forcing it to close the inpatient wards and manage the patients on its grounds instead (Fig. 4). Three of the four medical schools were destroyed and simply non-functional. Across the street from the ruins of one of the key teaching facilities of the state medical school, I met a third-year medical student who had a look of despair painted on her face as she wondered whether she would ever be able to finish her medical studies given the magnitude of the devastation and the destruction of her school.

Pile of rubble from buildings destroyed by the earthquake.

A typical street in Port-au-Prince blocked by rubble. Cars and dead bodies are buried beneath; pedestrians are wearing face masks or pinching their noses to avoid the stench of the decomposing bodies.

Patients from the State University Hospital (Hopital de l'Universite d'Etat d'Haiti) had to be managed on the grounds of the hospital because the inpatient wards were severely damaged.
Virtually every open field in Port-au-Prince had been converted into a refugee camp or “tent city.” These tents consisted merely of four relatively frail sticks planted on the ground with a few sheets thrown around them to give a semblance of shelter. Unfortunately, any strong wind that passed blew away these sheets, exposing the refugees and their belongings. On the soccer field of Quisqueya University, adjacent to the The Haitian Group for the Study of Kaposi Sarcoma and Opportunistic Infections (GHESKIO) Clinic, where we would eventually erect a field hospital, 7,000 refugees took residence under these frail tents [5,6] (Fig. 5).

Tent city on the soccer field of Quisqueya University, adjacent to the GHESKIO clinic, that became home to 7,000 homeless refugees.
After the 82nd Airborne Division, U.S. Army, had secured the location where we were going to erect the field hospital adjacent to the GHESKIO Clinic, on the campus of Quisqueya University, the DMAT and IMSuRT teams proceeded to set up a field hospital in the span of 24 h. Once the GHESKIO field hospital became operational, armed with a megaphone, we visited various tent cities throughout the community, including the Champs de Mars and the National Palace, to inform the people that our field hospital was open to treat earthquake victims. The response was quite remarkable, as hundreds of patients presented for care on a daily basis. They came using various modes of transportation; some were carried, some came on crutches, and others via wheel barrow. The GHESKIO field hospital consisted of two adult inpatient wards, one pediatric unit, one intensive care unit, a cast room, and an operating room (Figs. 6 and 7).

Inpatient ward at the GHESKIO field hospital.

Earthquake victim undergoing placement of an external fixator in the operating room.
During the two weeks of my engagement, the GHESKIO field hospital treated close to 1,500 patients, at least 40% of whom were younger than 18 years. We also performed hundreds of operations, mostly orthopedic procedures. The most common operations were placement of external fixators, debridement of necrotizing soft tissue infections, and life-saving amputations. We also took care of numerous gunshot wounds. We had limited supplies in general, especially for managing children. For example, we did not have external fixators for children, and we did not have pediatric ventilators. This latter situation forced us to ventilate a critically ill child by hand for more than 12 h before we could transfer him to the floating naval hospital, USNS Comfort, which arrived in the bay of Port-au-Prince eight days after the earthquake. Similarly, we did not have cribs or incubators and therefore had to be creative, fashioning cribs out of boxes and using aluminum foil and the heating elements from our MREs (meals ready to eat) to keep the babies warm (Fig. 8). In some instances, we exhausted our oxygen supply. Therefore, I enlisted the help of a local Haitian physician from the GHESKIO clinic, Doctor Vanessa Rouzier, to drive me to an oxygen supply store to purchase sufficient oxygen to keep the field hospital functioning. Similarly, when we ran out of external fixators and other critical supplies, GHESKIO physicians would go to other medical facilities to obtain the necessary supplies.

We used a cardboard box to make a crib and aluminum foil to keep this infant warm because we didn't have cribs.
Given the delay in the initial care of injured earthquake victims and the austere conditions under which surgical procedures were being performed throughout Haiti during the first two weeks, not surprisingly, we saw a large number of surgical site infections in our daily wound clinic (Figs. 9A and 9B). Along with some members of our team, I visited the adjacent tent city on the soccer field of Quisqueya University to ensure that there were no earthquake victims who needed medical attention. We found a number of the surgical patients we had treated, as well as newborn infants we had delivered, living in deplorable conditions under the tents where there was no access to latrines or potable water (Figs. 10 and 11). There were feces and garbage all around the periphery of the tent city. The Slovaks tried to spray some insecticides to control the flies, but the agents seemed to attract even more flies, making me believe that the Haitian flies were either resistant to the insecticide or thought that the guests were spraying nutrients. In conjunction with GHESKIO field workers, members of the 82nd Airborne Division explored the possibility of digging some holes for latrines. However, because Port-au-Prince is, as is New Orleans, below sea level, it was not feasible to do so.
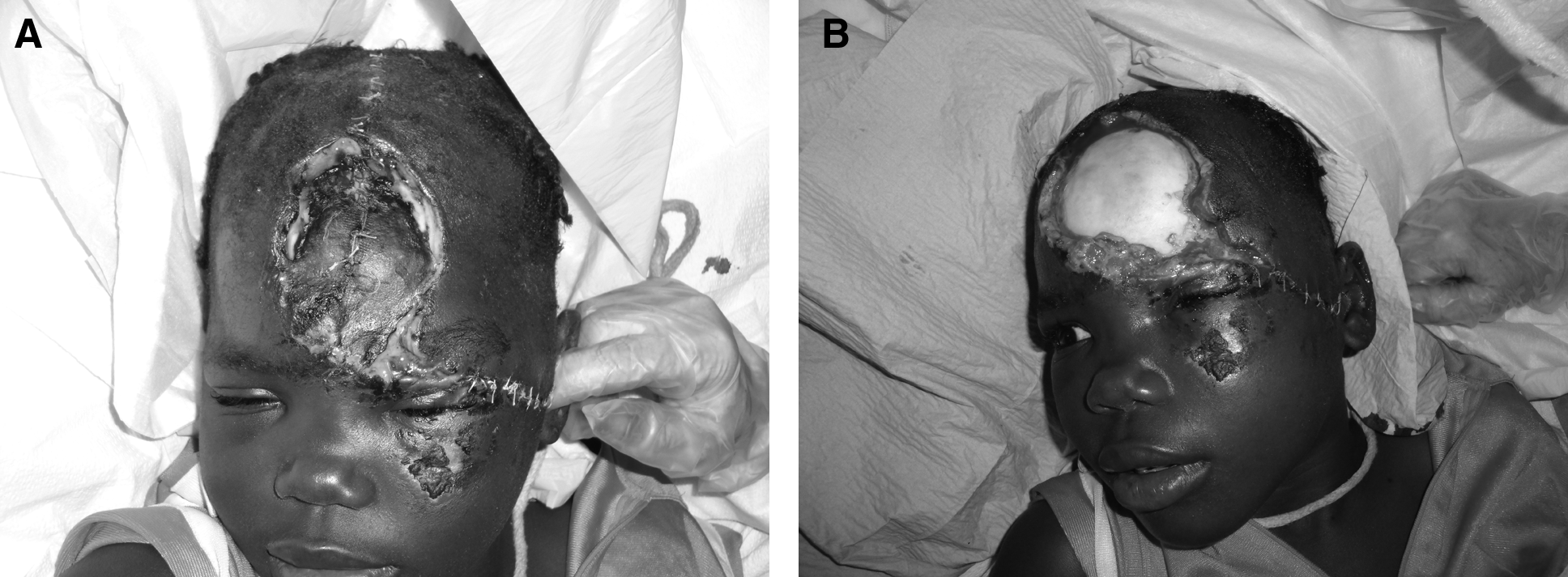
Nine-year old girl who sustained degloving scalp injury that was repaired more than 48 hours after the earthquake. There was copious amount of purulent drainage from the wound (

Living conditions in the adjacent tent city for the nine-year old girl with the scalp injury.

Newborn infant delivered at GHESKIO field hospital living in the adjacent tent city.
Despite the devastation and human suffering caused by the earthquake, the Haitian people never lost faith or hope. Young men would assemble outside the GHESKIO field hospital with their guitars every afternoon. They did not complain about the fact that the earthquake had occurred in what was already the poorest country in the Western Hemisphere. Instead, they were singing songs of praise and hope for a new, better, and stronger Haiti. The indomitable spirit of hope, faith, and optimism that has become the fabric of the Haitian people was best exemplified by a 31-year-old Haitian street vendor who was rescued from the rubble 14 days after the earthquake. Uncertain as to what was happening when the ground started shaking, he quickly sought refuge in a building that promptly collapsed, pinning him on the ground with a broken femur. Unable to move, he was essentially entombed. Fortunately, he was facing a two-gallon jug of water. He rationed the water over the ensuing 14 days, and the day he exhausted the water supply, he was miraculously rescued. After experiencing a number of deaths and amputations at the GHESKIO field hospital, there was jubilation in our camp and I simply could not contain myself over this success (Fig. 12).

Excitement over the rescue of a street vendor who had been entombed in a collapsed building for 14 days after the earthquake.
I was fortunate that my brothers, Doctor Jean Ford, a pulmonologist and epidemiologist at Johns Hopkins, and Doctor Billy Ford, Chief of Anesthesiology at Saint Barnabas Hospital in Bronx, NY, also responded to the call to service at “such a time as this.” They were stationed at the field hospital set up by Project Medishare near the airport. I am also delighted that several SIS members participated in the medical relief effort during the first four weeks after the earthquake. They include Doctors Wes Alexander, Howard Belzberg, Eileen Bulger, Soumi Eachempati, Enrique Ginzberg, Nick Namias (SIS Treasurer), Selwyn Rogers, Tom Scalea, and Felix Lui. I should also note that many other SIS members have gone to Haiti after the first four weeks and some continue to go there on a regular basis to provide medical relief.
Missed Opportunities
Overall, the GHESKIO field hospital provided much-needed care and support for the community we served. During this acute phase of the earthquake response efforts, we met the community's critical surgical and medical needs. At the same time, there were missed opportunities that could have augmented our ability to have an even bigger impact. These are important lessons that should help us prepare better for similar disasters on American soil. They include: (1) Lack of coordination of assets; (2) lack of resources, supplies, equipment, and medications designed especially for children; (3) lack of a coordinated approach to handle the large number of displaced children and former and newly orphaned children; and (4) the limited scope of the humanitarian engagement.
Lack of Coordination of Assets
The U.S. Army (82nd Airborne Division) did not secure the location of the future field hospital until more than 36 h after the DMAT/IMSuRT teams were on site at the U.S. Embassy. Thus, we lost precious hours that could have saved additional lives and limbs and averted the resultant infections.
Lack of Resources, Supplies, Equipment, and Medication Designed Specifically for Children
Given the demographics of Haiti, we should have anticipated that there would be a large number of injured children. Not only did we have limited supplies in general, we did not, for example, have external fixators for children, pediatric ventilators, pediatric doses for medications, or cribs.
Lack of Coordinated Approach to Handling the Large Number of Displaced Children (Transfers to Other Facilities) and Formerly and Newly Orphaned Children
A large number of children became orphans as a result of the earthquake. Many children were transferred from one hospital facility to another, including the USNS Comfort, for definitive care without their parents or guardians. The electronic medical record system we were using did not keep track of patient names or other identifying factors. The lack of information regarding the location of children and adults transferred to the USNS Comfort or other facilities posed serious challenges for reunification of patients with their loved ones.
Limited Scope of the Humanitarian Engagement
Our specific charge was to provide acute medical and surgical care. However, the people in the tent cities were also suffering from poor hygiene, lack of sanitary toilets (latrines), absence of potable water, and hunger, among other problems. Our inability to address these urgent needs created some anger and disappointment among the people living in the adjacent tent city.
High Rate of Surgical Site Infections
Because of the austere conditions under which most operations were conducted, there was a high rate of surgical site infections, which approached 80%.
Challenges for the Future
There are numerous challenges or long-term issues facing Haiti. These include follow-up care for complex wounds and fractures, the need for plastic and reconstructive surgery, and the need for prostheses and rehabilitation. An equally daunting task is how to avert a public health crisis given the shortage of latrines and running water and the limited supply of food in tent cities, especially as the hurricane season approaches. Additional rebuilding challenges include rubble removal, providing housing for 1.5 million homeless refugees, and establishing an infrastructure to support education, agriculture, and reforestation. However, the principal cause that has kept me returning to Haiti on a monthly basis since the earthquake is the lack of a trauma and critical care infrastructure. According to the U.S. Agency for International Development (USAID), the January 12, 2010, earthquake is the worst natural disaster ever recorded in the Western Hemisphere in terms of human and economic impact [7]. More than 220,000 individuals were killed, more than 300,000 were injured, and more than 1.5 million were left homeless. More than 80% of the important medical facilities sustained irreparable damage, crippling what was already a limited capacity for surgical and critical care. The lack of infrastructure to provide emergency medical services undoubtedly contributed to the catastrophic number of deaths and untreated traumatic injuries that resulted in amputations or deaths. Consequently, I have been working closely in partnership with the Ministry of Health of Haiti (Ministère de la Santé Publique et de la Population), Haitian health care professionals and organizations, Project Medishare, Partners In Health, and leading universities in the US, including the University of Miami and the University of Southern California, to enhance the provision of surgical, trauma, and critical care and rehabilitation services in Haiti. This working group proposes a multi-component plan to increase Haiti's capacity to treat traumatic injuries and provide critical care by establishing a trauma system and developing a National Trauma, Critical Care, and Rehabilitation Hospital in the country.
Finally, as incoming President of SIS, let me share with you some of my priorities for the coming year. I am charging the Therapeutics and Guidelines committee of SIS to develop guidelines for optimal antibiotic prophylaxis and treatment for operations performed during disaster situations or under austere conditions such as during wars or natural disasters. I believe that SIS should provide a forum to discuss such challenges. We will renew emphasis on critical care and acute care surgery and will work closely with SIS-E, SIS–Japan, and others to develop and disseminate guidelines and work with industry to ensure that drugs and resources are available where and when they are needed. I believe that the founding members of SIS would be proud of the tremendous legacy of this great society and of the fact that SIS, through its members and innovative approaches, research, and guidelines, finds itself in the service of all nations to reduce the burden and morbidity of surgical infections. I thank you, once again, for the tremendous honor of serving as the President of this great society!
Footnotes
Acknowledgments
I want to thank the entire staff of the GHESKIO clinic, in particular Doctor Jean William (Bill) Pape, Director of the clinic, and Doctor Vanessa Rouzier for their dedication and commitment to the Haitian people and for their incredible support for the field hospital. In addition, many thanks to Doctor Jeffrey Upperman for coordinating and preparing me for the disaster relief trip to Haiti, Doctor Nadine Gracia of the Department of Health and Human Services for making it possible for me to join the DMAT and IMSuRT teams in Haiti, Doctor Susan Briggs for her strong leadership of the GHESKIO field hospital, and Amy Puliafito for coordinating the ongoing medical relief efforts in Haiti of the Keck School of Medicine of the University of Southern California.
Author Disclosure Statement
No conflicting financial interests exist.
Delivered at the Thirtieth Annual Meeting of the Surgical Infection Society, Las Vegas, Nevada, April 19, 2010.