
Abstract
Abstract
Background:
The ideal antimicrobial treatment for intra-abdominal infections (IAIs) in the setting of fast-paced emergency departments (EDs) should be effective, convenient, and of limited resource utilization. Antibiotic monotherapy is a feasible option for this. We conducted a study in which we compared two regimens for antibiotic monotherapy recommended by published guidelines in ED patients with community-acquired, complicated IAIs (cIAIs).
Methods:
The study was a prospective, randomized, study of ampicillin-sulbactam versus moxifloxacin for cIAIs. After the diagnosis of cIAI was established, patients were assigned randomly to receive either moxifloxacin 400 mg intravenously (IV) qd followed by moxifloxacin 400 mg orally (PO) qd, or ampicillin-sulbactam 1.5 g IV qid followed by ampicillin-sulbactam 750 mg PO q12h. Source control procedures were used for all patients and all had complete follow-up. The primary efficacy variable for the study was the clinical response at the test-of-cure visit.
Results:
A total of 116 patients were enrolled for prospective evaluation and randomized assignment to treatment with ampicillin-sulbactam (n=55) or moxifloxacin (n=61). At the test-of-cure evaluation, the overall clinical failure rate was 13.8%. The clinical failure rates in the ampicillin-sulbactam and moxifloxacin groups were 16.4% (9/55) and 11.5% (7/61), respectively (p=0.446). With regard to infection site, the clinical failure rate in cIAIs consisting of lower gastrointestinal (GI) tract infection was significantly lower in the moxifloxacin than in the ampicillin-sulbactam group (4.3% vs. 19.6%; p=0.024). According to multivariable analysis, independent risk factors for treatment failure were the time to ED presentation >24 h (odds ratio [OR] 6.8; 95% CI 1.3-36.2; p=0.024) and ampicillin-sulbactam therapy (OR 9.5; 95% CI 1.1–76.6; p=0.033).
Conclusions:
A significant difference existed in the clinical responses of the two groups. As compared with ampicillin-sulbactam, moxifloxacin was more effective for the treatment of community-acquired cIAIs of the lower GI tract. A higher risk of treatment failure for antibiotic therapy was found for patients presenting to the ED with symptoms of cIAIs lasting >24 h. Alternative antimicrobial agents should be considered for treating these patients.
The ideal antibiotic regimen for proper and timely treatment of IAIs in fast-paced EDs should be effective and convenient, and have limited resource utilization. From the viewpoint of clinicians in the ED, antibiotic monotherapy is a convenient and feasible option for meeting these criteria. We therefore conducted a study focused on patients with community-acquired IAIs in which we compared two regimens for antibiotic monotherapy of complicated IAIs (cIAIs) (ampicillin-sulbactam vs. moxifloxacin) recommended in older published guidelines for treating these patients [4,6]. To determine the clinical efficacy of these two monotherapeutic regimens and to identify potential risk factors influencing the treatment outcome, we conducted our study as a prospective, randomized, study of ampicillin-sulbactam versus moxifloxacin for the treatment of cIAIs.
Methods
Study design
This prospective, comparative, randomized, single-blind study was conducted at a 1,200-bed tertiary care hospital in south Taiwan. Annually, approximately 85,000 patients visit the ED of the hospital and are managed in three different services (internal medicine, surgical emergency/trauma service, and pediatric emergency medicine) in accordance with their chief complaints. During the 19-mo period from March 2009 to September 2010, all patients 18 years of age or older were presented to our ED with acute abdomen-related symptomatology were potentially eligible for the present study. The study was approved by the institutional review board of our hospital and registered at clinical trials.gov under the identification code ID: NCT00952796.
Study participants
Patients who had signs and symptoms of IAI were initially evaluated by members of the ED staff. Patients were enrolled in the study if they met all of the following inclusion criteria: Suspected or confirmed cIAI; expected duration of in-hospital treatment with intravenous (IV) antibiotics ≥3 full days but not >14 d; ability to provide written informed consent for participation in the study. A confirmed diagnosis of IAI required a surgical procedure (laparotomy or laparoscopy) or percutaneous procedure that revealed intra-operative evidence relevant to IAIs, such as overt peritoneal inflammation with purulent exudates, intra-abdominal abscess, or macroscopic bowel perforation with diffuse peritonitis. In cases of suspected IAI, radiologic evidence and clinical symptoms had to be compatible with an IAI, and a surgical procedure had to be scheduled. Patients with known hypersensitivity to the drugs used in the study or with healthcare-associated infections, including those with a history of any hospitalization in the 30 d before the ED diagnosis of IAI, were excluded from the study.
Treatment and data collection
Randomization was done through the use of sealed envelopes upon the patient's arrival in the ED. All participating patients provided informed written consent. After the diagnosis of cIAI was established, patients were assigned randomly to receive either moxifloxacin 400 mg IV qd followed by moxifloxacin 400 mg PO qd or ampicillin-sulbactam 1.5 g IV qid followed by ampicillin-sulbactam 750 mg PO q12h. The physician in charge had to evaluate the patient's clinical condition and toleration of oral intake to decide whether to convert from IV to PO administration of a drug used in the study. The duration of combined IV/PO treatment was 5–14 d. Source-control procedures, including abdominal surgery or computed tomography (CT)-guided percutaneous drainage, were used for all patients. Samples for microbiologic testing were collected either as intra-operative specimens or from drainage fluids.
Patients were visited during the follow-up period to collect all pertinent data, which were recorded on a standard data-collection form. The following characteristics were recorded by a single trained data abstractor: Gender; age; height; body weight; body mass index (BMI); shock index (defined as the ratio of heart rate to systolic blood pressure) measured on arrival in the ED; fever (temperature >37.5°C); intensity of abdominal pain assessed on a visual analogue scale (score 0–10); time interval between onset of symptoms and arrival in the ED (time-to-ED) ≤24 h or >24 h; presence of high-risk co-morbidities such as a medical history of diabetes mellitus, liver cirrhosis, chronic kidney disease, or malignant disease; relevant laboratory data obtained in the ED; infection site (dichotomized as upper or lower gastrointestinal tract [UGI/LGI]); source control procedure; duration of treatment; adverse drug reactions; and survival or death.
The primary efficacy variable for the study was the clinical response at the test-of-cure visit (10–14 d after the end of treatment). Test therapy was considered successful if fever and clinical signs of infection resolved without a change in the patient's initial antibiotic therapy. Contrarily, the persistence or exacerbation of clinical signs or symptoms relevant to cIAIs or an early shift to other antibiotics than those used initially because of poor improvement was considered as clinical failure. To ensure consistency, adverse effects were recorded in the case-report form and judged to be related or unrelated to the study drugs by two principal investigators (C.-W.C. and J.-Y.W.). Post-discharge surveillance was based on scheduled visits to the surgeon in charge. All patients were followed until completely well.
Statistical analysis
On the basis of local epidemiologic data and the results of previous studies, we assumed that a reduction of >10% in the rate of clinical failure was clinically relevant as compared with the rate of such failure with standard therapy, and we therefore chose this limit as the parameter by which to calculate the statistical power of the results of the study. For a non-inferiority margin of 10%, with a 5% level of significance and 80% statistical power, it would be necessary to have a sample size of 49 evaluable patients randomized into each treatment arm of the study. This implied a total of ≥98 patients for the study. A two-sided 95% confidence interval (CI) was constructed for the difference in clinical response in the two study treatment groups for evaluating the hypothesis of noninferiority of moxifloxacin. Data were analyzed with SPSS version 14.0 (SPSS, Chicago, IL, USA). Data on the characteristics of patients in the two study treatment groups were compared with the χ2 test and Fisher exact test for categorical variables, and with the Student t-test for continuous variables. Because the primary outcome was binary, both the relative risk and risk difference were reported in all randomized and clinically evaluable populations. If the difference in treatments was concluded to show non-inferiority, the superiority test was declared as having been done. For each category of potential risk factors for treatment failure, the incidence of success as well as of failure was calculated by dividing the number of events by the number of patients in that category. Odds ratios (OR) and their 95% CIs were calculated. Multiple logistic regression analysis was used to identify variables that were related significantly to the likelihood of clinical failure of antibiotic treatment. Regression models were controlled for the effects of confounding variables. Results of the logistic regression analysis are reported as adjusted ORs with 95% CIs. All tests of significance were two tailed; values of p<0.05 were considered to indicate statistical significance.
Results
A total of 130 patients were enrolled initially for prospective evaluation. Sixty-five patients were randomized to receive moxifloxacin and the other 65 were assigned to receive ampicillin-sulbactam. Fourteen patients without complete study data or with an incomplete follow-up were excluded, and the remaining 116 patients were analyzed further (Fig. 1). The patients' mean age was 52.3 years (range 19–92 years), and 70 (60.3%) of the patients were male. There was no significant difference in the background characteristics of the treatment groups except that patients with co-morbidities were more common in the moxifloxacin than in the ampicillin-sulbactam group (23% vs. 7.3%, respectively; p=0.02). Detailed characteristics of all participants in the study are displayed in Table 1.
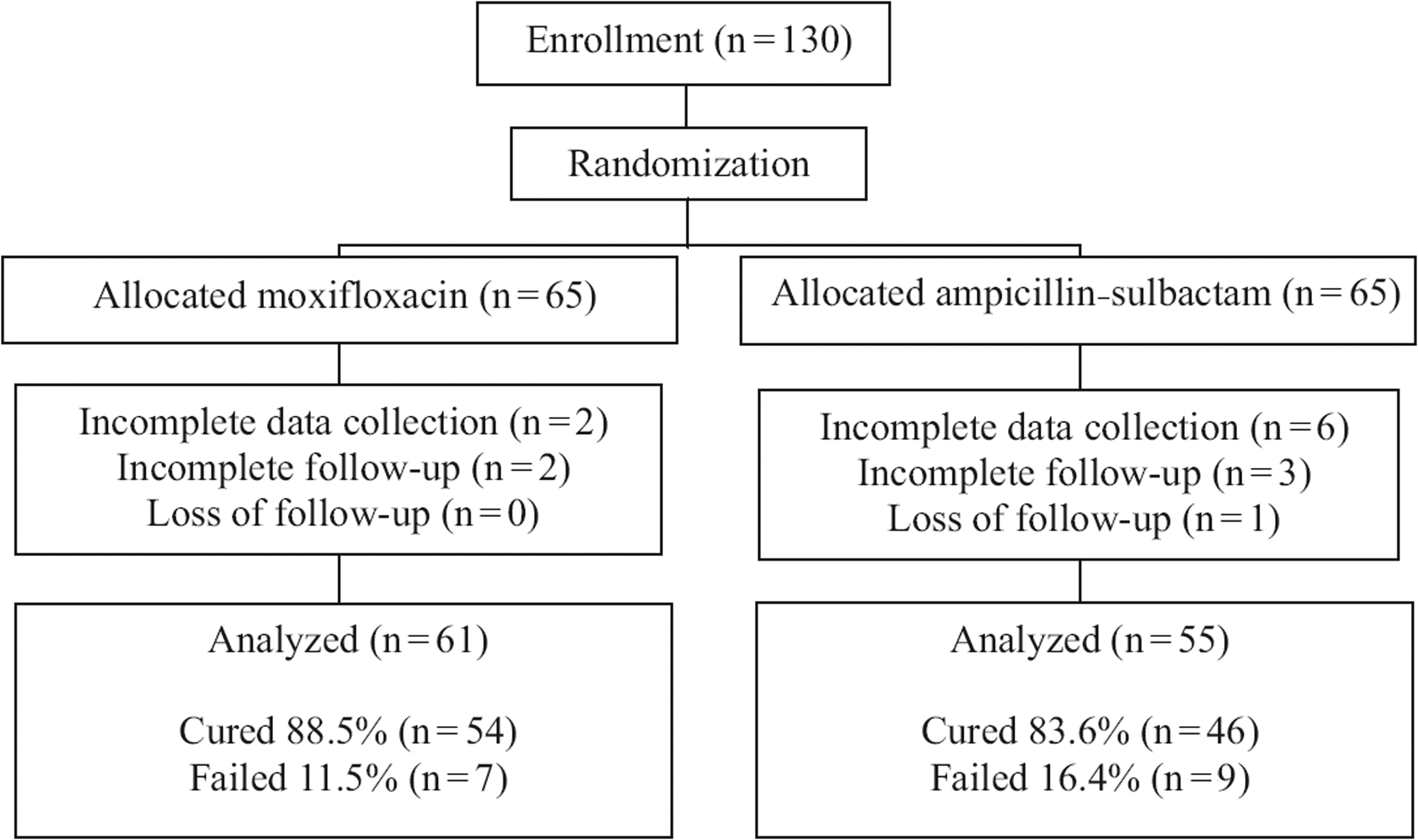
Patient disposition in study.
Visual analogue scale (score 0–10).
Diabetes mellitus, liver disease, chronic kidney disease, or malignant disease.
Values of p are for comparisons between two groups of clinically evaluable patients.
One patient lost to follow-up was assumed to be free of adverse events and mortality.
CRP=C-reactive protein; ED=emergency department; GI=gastrointestinal; NA=not analyzed due to incomplete data collection; GI=gastrointestinal.
Complicated intra-abdominal infections of the UGI tract were diagnosed in 24 patients, most of whom had perforated duodenal ulcer disease (22/24; Table 2). Ninety-two patients had cIAIs originating from the LGI tract; these included 77 patients with complicated appendicitis. Microorganisms were isolated in 50 cases (43.1%). Table 3 shows the distribution of isolated organisms. The most commonly isolated pathogen in both treatment groups was Escherichia coli, followed by Klebsiella spp. and Bacteroides spp. Extended-spectrum β-lactamase (ESBL)-producing E. coli were responsible for one clinical failure in the ampicillin-sulbactam group. Extended-spectrum β-lactamase-producing Klebsiella spp. were isolated in one patient who was cured with moxifloxacin. Pseudomonas aeruginosa infections were found in five patients. All five of these patients, including one treated with moxifloxacin, recovered uneventfully without clinical failure.
Including cholangitis and cholecystitis.
Appendicitis with purulent exudates, gangrene, perforation, or focal abscess.
GI-gastrointestinal.
Data are presented as numbers of cases.
Two cases treated with moxifloxacin.
Treated with ampicillin-sulbactam.
Treated with moxifloxacin.
ESBL=extended-spectrum beta-lactamase.
Treatment was successful in 84.6% (110/130) and 86.2% (100/116), respectively, of all randomized and clinically evaluable patients (Table 4). According to the test-of-cure evaluation for all randomized patients, the clinical cure rate in the moxifloxacin group was 88.5% (54/61) versus 83.6% (46/55) in the ampicillin-sulbactam group (risk difference of 6%; 95% CI −7% to 12%). The outcome analysis for clinically evaluable patients yielded similar results (risk difference of 5%; 95% CI −8% to 18%), which were consistent with a non-inferiority conclusion. With regard to infection site, in an intention-to-treat analysis in which patients who were lost to follow-up were considered not to have responded to treatment, the clinical success rate in treating cIAIs caused by LGI infection was significantly higher in the moxifloxacin group than in the ampicillin-sulbactam group (95.7% vs. 80.46%; risk difference of 14%; 95% CI 0.5%–27%, p=0.038). For clinically evaluable patients, moxifloxacin was again superior to ampicillin-sulbactam, with a difference in the two treatments' success rate of 15% (95% CI, 17%–29%, p=0.024). On the basis of these findings, we further focused on LGI infections for a risk-stratification analysis. Table 5 shows the correlation of potentially confounding risk factors in clinically evaluable patients in the study groups in which treatment was successful clinically and in which it failed. By univariate analysis, we found that time to ED and choice of antibiotic treatment were statistically significantly different in patients in whom treatment was successful and those in whom it failed. After adjustment for all covariates, a time to ED >24 h (OR 6.8; 95% CI 1.3–36.2; p=0.024) and ampicillin-sulbactam therapy (OR 9.5; 95% CI 1.1–76.6; p=0.033) remained independent risk factors for treatment failure.
Percentages are based on number of patients reporting outcome for each treatment arm.
For superiority test.
cIAIs=complicated intra-abdominal infections; CI=confidence interval.
Each risk factor was adjusted for all other risk factors listed in the table.
Statistically significant at p<0.05.
BMI=body mass index; BT=body temperature; ED=emergency department.
A detailed analysis of the clinically evaluable treatment failures in the study is presented in Table 6. Of five patients who underwent second source control procedures, one patient with buccal cancer ultimately expired from abdominal sepsis. Microorganisms were isolated from 43% (7/16) of the patients in whom treatment failed. The most commonly isolated pathogen was P. aeruginosa (3/7), followed by Clostridium perfringens (2/7). Sixteen potentially adverse drug related events were reported, of which four events that might have been associated with IAIs or related source control procedures were excluded. The incidence of adverse events related to drugs investigated in the study was roughly similar in the moxifloxacin (11.5%) and ampicillin-sulbactam (9.1%) groups (p=0.674). All 12 adverse events were of mild severity. The most frequently reported drug-related adverse event was diarrhea (6/12), followed by nausea (4/12). Skin rash was reported in one patient treated with moxifloxacin. Another patient experienced cyclic abdominal pain accompanying the IV administration of ampicillin-sulbactam. No serious adverse event was reported in either treatment group.
Ultimately expired from multiple organ failure.
Discussion
Early diagnosis, adequate source control, and proper antibiotic treatment are the basic elements of management for cIAI [7]. Our analysis shows that the affected site is another important factor in the outcome of treatment for such infection. Previous similar studies focusing on a variety of community-acquired cIAIs showed that moxifloxacin was as effective as comparator drugs for their treatment [8–10]. In the present study, although both ampicillin-sulbactam and moxifloxacin appeared equivalent in terms of the clinical response of cIAIs generally, moxifloxacin was more efficacious for treating cIAIs of the LGI tract. Furthermore, when potential risk factors were taken into account, treatment with ampicillin-sulbactam was associated with an approximately 9.5-fold greater risk of treatment failure than was moxifloxacin in patients with community-acquired cIAIs.
As compared with the UGI tract, the LGI tract contains more complex bacterial species and warrants greater consideration of drug resistance. Because ampicillin-sulbactam has a good safety profile and provides coverage of a wide spectrum of bacterial pathogens, including aerobic gram-positive and gram-negative bacteria as well as anaerobic organisms, some physicians regard it as an option for the treatment of cIAIs without considering emerging drug resistance among E. coli [11–13]. In our institution, the proportion of E. coli strains that were nonsusceptible to ampicillin-sulbactam increased from 35% in 2001 to 41% in 2011. The considerable clinical failure of ampicillin-sulbactam therapy in community-acquired IAIs is consistent with recent findings [11,12,14]. Simple regimens, such as monotherapy, that provide an adequate spectrum of coverage with easy administration, are a desirable option for clinicians. As compared with ampicillin-sulbactam, moxifloxacin seems a better and more efficacious choice of antibiotic monotherapy for patients with mild-to-moderate community-acquired cIAIs of the LGI tract.
For physicians in the ED, both the identification of potential risk factors and selection of proper antibiotic therapy within a limited time frame are important issues. Although the role of a microbiologic workup of infected body fluid in the treatment of IAIs has in recent years been debated, results of culture of blood or tissue specimens are usually unavailable during patients' ED stay. It is usually recommended that antibiotic treatment be initiated as soon as possible after the diagnosis of IAI [15,16]. Appropriate risk stratification and selection of antibiotics is especially pivotal. Rapid risk triage based on concise information obtained from initial interviews with patients is a convenient and feasible solution to meeting these pivotal needs. Physiologic disturbance, advanced age, co-morbidities, malnutrition, and malignant diseases have been proposed as influential factors in treatment failure [3,16–19]. According to the results of our study, treatment delay (time-to-ED >24 hours), and the choice of antimicrobial therapy, were important risk factors. The association between delay in antibiotic treatment and an unfavorable outcome has been demonstrated previously [18,20,21]. With an additional survey regarding processing time in the ED, we found that the mean treatment delay (from arrival in the ED to the initiation of adequate source control) was 5.9±9.9 h for all of the patients randomized in our study. We also constructed receiver operating characteristic (ROC) curves to investigate the most accurate cutoff value for time to ED in predicting treatment failure. The best cutoff value for this was 59 h, with an area under the curve (AUC) of 0.658 (sensitivity, 69%; specificity, 75%; data not shown). However, even with the better performance of a sensitivity of 75%, we still arbitrarily dichotomized the time to ED into the two categories of (≤24 h or >24 h) so as to facilitate the process of risk stratification in the ED and to minimize the potential recall error and statistical disturbances caused by outlying values. Emergency physicians may obtain time-to-ED information in encountering ED patients, but may still fail to appreciate the time-to-treatment interval in fast-paced and crowded settings. The need for complete recording of a patient's history, incorporating accurate identification of potential treatment delays, should be emphasized. Second-line antibiotics for cIAIs including imipenem-cilastatin, meropenem, doripenem, piperacillin-tazobactam, cefepime, ceftazidime, ciprofloxacin, or levofloxacin, each in combination with metronidazole, might be considered in advance for patients with a time to ED >24 h [16,17].
Among patients with UGI infections, substantially more of those assigned to the moxifloxacin group were aged >65 years (77.8% vs. 22.2%), and the moxifloxacin-treated patients had more co-morbidities than those in the ampicillin-sulbactam group (66.7% vs. 33.3%, respectively). However, the limited number of study participants with cIAIs of the UGI tract restrained our further exploration. Although previous studies have shown moxifloxacin to be efficacious for the treatment of infections of the UGI tract, further large-scale studies focusing on this issue, with adequate control of confounders, are still needed to provide convincing conclusions [9]. On the other hand, our study presents some compelling information. We excluded healthcare-associated cIAIs and particularly highlighted infections of the LGI tract, and merely compared the efficacy of first-line antimicrobial monotherapies against community-acquired cIAIs. The simplicity of focused objectives and treatment protocols would clarify our findings relevant to straightforward conclusions.
Conversely, our study had some weaknesses. First, the quality of interventional procedures for source control was not standardized. The preference of celiotomy or percutaneous drainage differed among physicians in charge, which might result in inadequate source control with subsequent treatment failure. Second, the generalizability of the findings in the study is limited by its having been a single-institution study with local epidemiology. The results of our study should be tempered by the individual features of every particular treatment facility and local bacterial surveillance reports. Third, the selection of ampicillin-sulbactam as a comparator drug in treating cAIAs is controversial because newly updated guidelines no longer include it for consideration in the treatment of some cIAIs [17]. However, these newer guidelines were issued during or after the period of our study; at the time the study was begun, ampicillin-sulbactam was still considered a valuable option for treating cAIAs. Our study adhered to recommendations in the previous versions of the guidelines of the Surgical Infection Society, Infectious Diseases Society of America, and regional infectious disease societies in the United States [4,6].
No significant difference existed between the antibiotic treatment groups in our study when the data for the primary outcome were analyzed. As compared with ampicillin-sulbactam, moxifloxacin is more effective for the treatment of community-acquired cIAIs of the LGI tract. For patients presenting to the ED with symptoms that have lasted >24 h, antibiotic therapy has a high risk of treatment failure. Second-line antimicrobial agents may be considered for these patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.