
Abstract

To the Editor:

Magnetic resonance imaging of the thoraco-lumbar spine at admission.
Initially, cefazolin and gentamicin were prescribed. A computed tomography (CT)-guided biopsy of the T6 vertebral body was performed through the right pedicle of T6 on the day after the patient's admission. Pathology examinations confirmed a chronic inflammatory reaction. Serial cultures of blood, urine, sputum, and biopsy tissues revealed no growth. Because of persistent fever and back pain, the patient was treated empirically with oxacillin 1.5 g q6h beginning on day four after her admission.
The patient experienced persistent fever and weakness in her left leg, and more severe destructive osteomyelitis with epidural extension and cord compression were found on the MR images of her thoraco-lumbar spine (Fig. 2A). Decompression surgery, consisting of posterior laminectomies of T5 and T6 and a transpedicular biopsy, were done on day 18 of hospitalization. Tissue culture revealed no growth. The patient's antibiotic therapy was then changed to ceftriaxone 2 g q12 h.
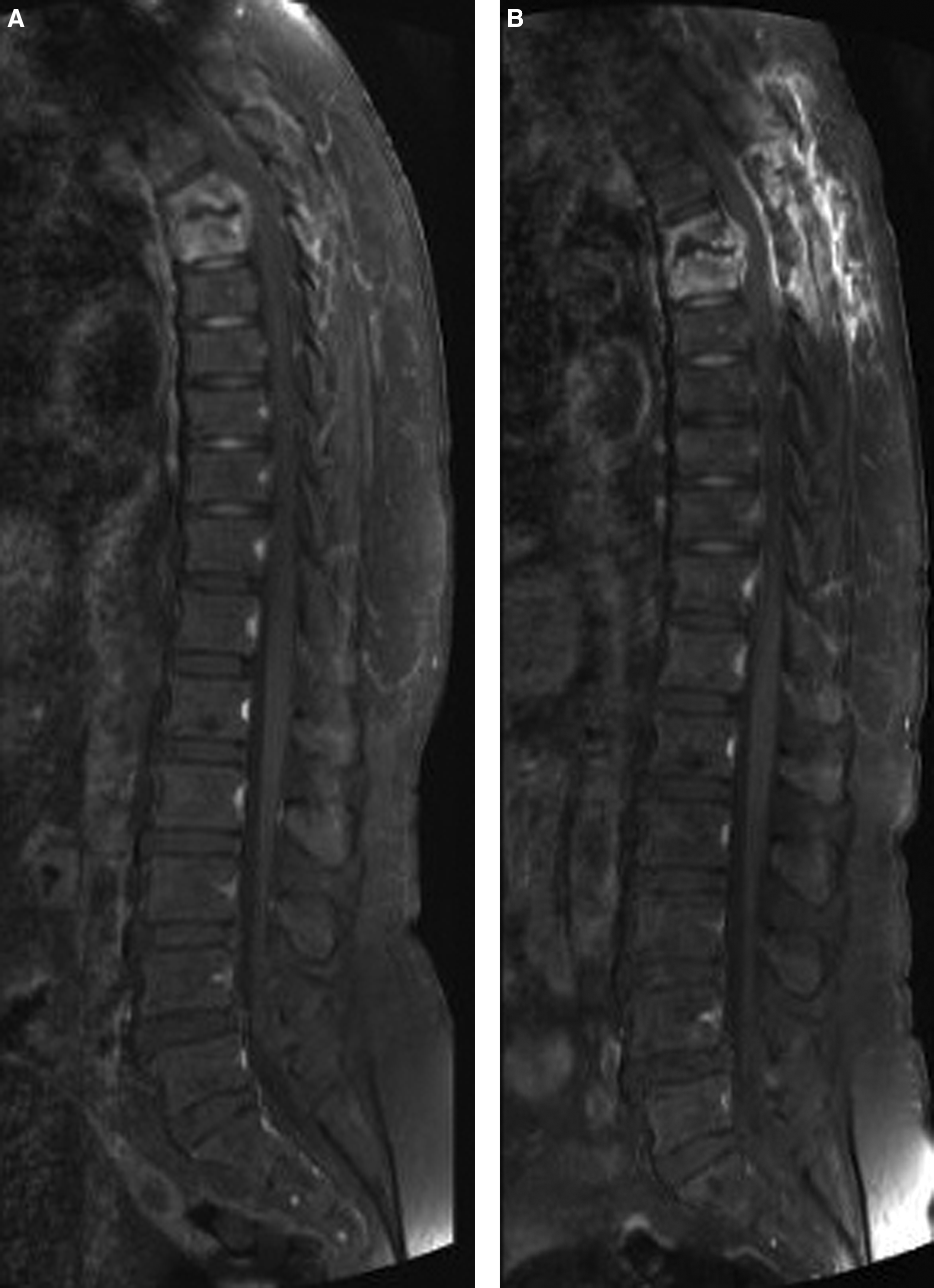
Sagittal views of T1-weighted magnetic resonance images after administration of gadolinium contrast revealed strongly enhancing vertebral osteomyelitis with epidural extension and compression of the spinal cord before the first
However, progressive bilateral weakness of the patient's lower limbs, and urinary retention were noted. Progressive extension of the epidural abscess, together with collapse of the T5–T6 vertebral bodies (which compressed the spinal cord) were demonstrated in MR images (Fig. 2B). The patient then underwent transthoracic corpectomies at T5 and T6, with internal fixation of an autologous bone graft (from the iliac crest) on day 36 after her first operation. Tissue culture confirmed Burkholderia cepacia infection. After antibiotic susceptibility tests showed the infecting organism to be sensitive to ceftazidime, meropenem, trimethoprim-sulfamethoxazole, and levofloxacin, the patient's antibiotic therapy was changed again, to levofloxacin 250 mg q8h. However, her pulmonary compliance and function were poor after open chest surgery, and she succumbed about 2 wk after her second operation from septic shock and respiratory failure.
Burkholderia cepacia, a gram-negative bacillus, is an important pathogen that infects patients particularly with cystic fibrosis (CF) and chronic granulomatous diseases, and immunocompromised patients [1,2]. This bacterium is found commonly in moist environments in association with soil, water, and plant roots [3]. The types of infection caused most commonly by B. cepacia are bacteremia, urinary tract infection, surgical site infection, septic arthritis, peritonitis, soft-tissue infection, endocarditis, and respiratory tract infection [4,5]. Several predisposing factors, including CF, chronic granulomatous diseases, indwelling intravascular catheters, assisted ventilation, and intravenous drug abuse increase the risk of infection with B. cepacia [1,6]. Contaminated fluids, such as tap water and nebulizer, irrigation, and dialysis fluids, have also been reported as sources of B. cepacia infection [1,7,8].
Vertebral osteomyelitis caused by B. cepacia is described rarely, with only three cases, consisting of two cases of cervical and one case of lumbar osteomyelitis, reported in the literature [3,6,8]. The diagnosis of B. cepacia infection in these three cases was confirmed by CT-guided biopsy or open surgery. All of the patients recovered gradually after the prescription of suitable antibiotics, possibly aided by decompressive surgery. The sources of the patients' infections were probably intravenous drug abuse, previous rhinoplasty with contaminated fluid, and an unnoticed external wound that occurred either during a fall on an icy road or from intramuscular stimulation therapy. Antimicrobial resistance of B. cepacia has been considered a great challenge in treating infection caused by the organism [1]. To the best of our knowledge, B. cepacia infection involving the thoracic spine in a healthy adult, as in our case, has not been reported previously in the literature.
In the case of our patient, no intravenous drug abuse or recent major surgery was revealed. The source of the patient's B. cepacia infection may have been her occupational environment of soil, water, and plants. However, even though tissue cultures were done in three invasive procedures, including a CT-guided biopsy and open spine surgery, the patient's vertebral B. cepacia osteomyelitis was confirmed only on day 54 of hospitalization. This may have been due to the sizes of the specimens used for culture and the concentration of bacteria in them. Among advanced techniques in medical microbiology, 16s ribosomal ribonucleic acid (RNA) gene sequencing is a rapid and accurate alternative to the phenotypic method of bacterial identification [9]. In future cases of possible B. cepacia infection, this tool may be considered for diagnosis, as in the case described by Yang et al. [8].
In conclusion, this is the first case of thoracic vertebral osteomyelitis caused by B. cepacia infection in an immunocompetent adult. Our case demonstrated this rare pathogen in pyogenic vertebral osteomyelitis. The optimal treatment of such disease is based on the early detection of B. cepacia, which is inherently resistant to drugs commonly used empirically for the treatment of vertebral osteomyelitis.