
Abstract
Abstract
Background:
Primary echinococcosis, and especially primary alveolar echinococcosis (AE) is rare among adrenal lesions.
Methods:
We report a case of primary AE in a 28-year-old male with low backache and occasional upper limb pain lasting for six months, and review the pertinent but sparse literature on this disorder.
Results:
Evaluation of the patient revealed an abdominal mass as right adrenal AE. The adrenal gland is a rare extrahepatic site of occurrence of echinococcosis, and particularly of AE. Patients with adrenal echinococcosis usually have nonspecific clinical symptoms. Imaging examinations revealed clearly the features of AE and its surrounding pathology. Alveolar echinococcosis was seen as an inhomogeneous pseudotumor with irregular boundaries, an irregular central pseudocystic appearance, and infiltration into surrounding structures. On contrast-enhanced computed tomography, the periphery of the mass in AE may be enhanced and multicentric vesicles may be seen. Magnetic resonance imaging may show the multivesicular morphology of lesions. The definitive diagnosis of AE should be confirmed by pathologic or serologic examination. Radical surgical resection of the removable parasitic lesion, followed by anti-infective therapy with benzimidazoles, is the primary method for treating AE.
Conclusion:
Although primary adrenal AE is rare, it should be included in the differential diagnosis of adrenal masses, especially in regions where AE is endemic.
Case Report
A 28-year-old male was referred to the department of urologic surgery for evaluation of a low backache and occasional upper limb pain that had lasted for 6 mo and had worsened 1 mo before the patient's admission. The patient had no associated urologic symptoms, and neither he nor any members of his family had experienced such symptoms in the past. Physical examination yielded normal findings and the results of a complete blood cell (CBC) count, electrolyte assays, a serum biochemistry profile, and urinalysis were within normal limits. However, the patient had a low plasma norepinephrine concentration of 200 ng/L (normal range 272–559 ng/L) and low plasma epinephrine concentration of 45 ng/L (normal range 54–122 ng/L).
Color Doppler ultrasonography (USG) of the patient's upper abdomen, and contrast-enhanced abdominal computed tomography (CT), were done. The adrenal gland was abnormal on USG, and an elliptical mass measuring 8×6 cm was seen in the right adrenal region. The internal echogenicity of the mass appeared inhomogeneous. The mass had a peripheral solid component of uneven thickness with a ragged inner boundary, and showed localized large and uneven echogenic dots (Fig. 1A). No obvious blood flow signals were observed either in the periphery or interior of the mass (Fig. 1B). Part of the mass had no distinct boundary separating it from the right posterior liver, the upper pole of the right kidney, and the inferior vena cava (IVC). Doppler USG showed that the IVC was compressed, with a decreased rate of blood flow but without abnormal filling (Fig. 1C).

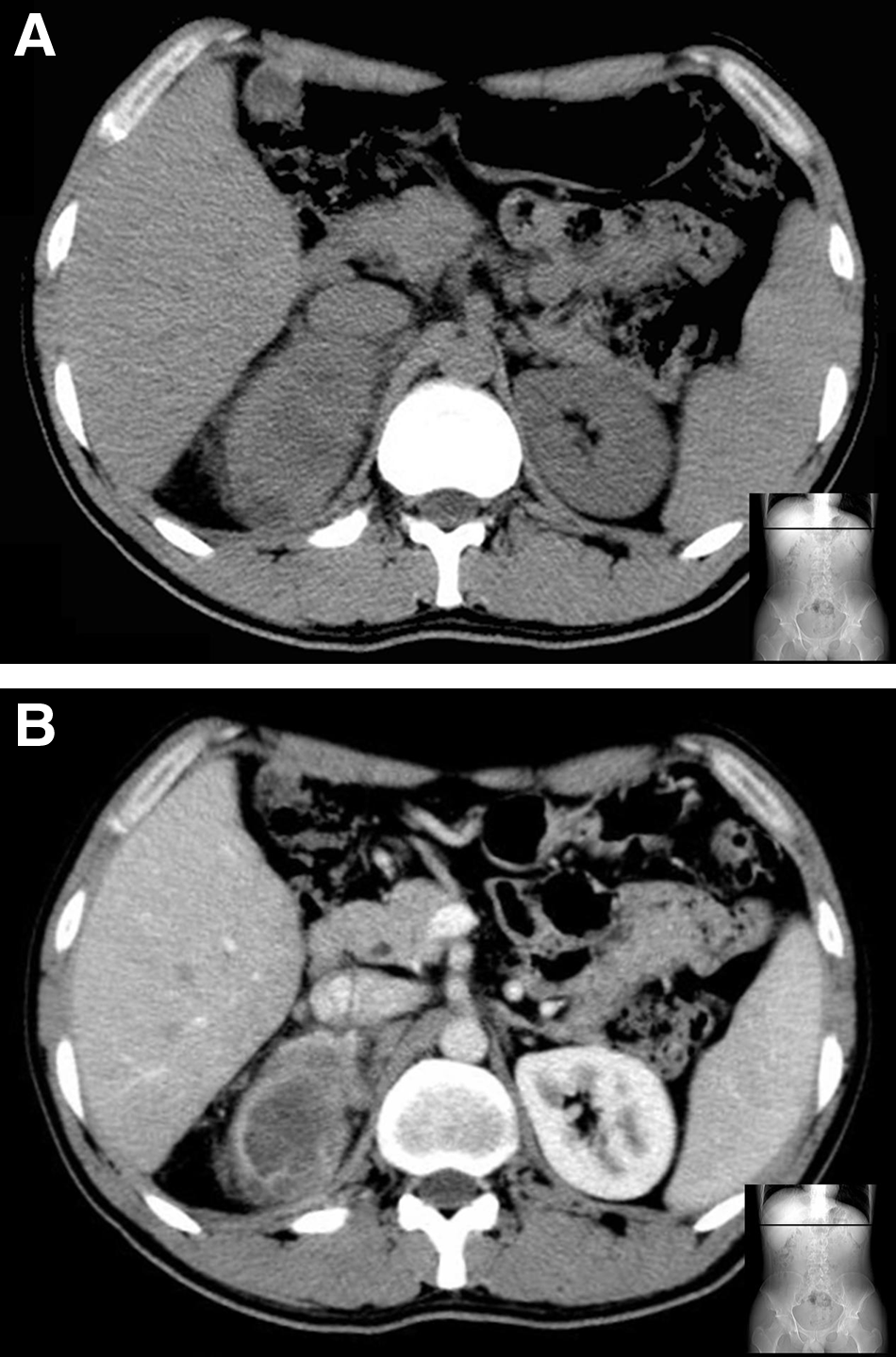
A plain CT scan demonstrated an inhomogeneous soft-tissue mass in the right adrenal region, with an irregular low-density area (CT value: 11 Houndsfield units) without clear boundaries (Fig. 2A). A plaque-like high-density region with punctate calcification was seen in the solid area of the lesion. On contrast-enhanced CT, the boundary and intervals of the lesion were slightly enhanced and its contour was visible clearly. A few small, cystic, low-density foci without contrast enhancement were seen in the peripheral solid area of the mass (Fig. 2B). The boundaries between the mass and the liver and the upper pole of the right kidney were unclear, suggesting infiltration. No other masses were found in the abdomen or thorax, although several enlarged lymph nodes were detected around the adrenal mass and IVC.
The adrenal mass and the surrounding enlarged lymph nodes were excised radically because it was difficult to exclude other pathologic conditions in the region of the mass. The operation revealed the adrenal mass to be irregular and tightly adherent to Glisson capsule, Gerota fascia, and the wall of the IVC. The lesion was excised completely. The excised specimen was irregular and grayish white, measuring 8×7×6 cm. When dissected the specimen yielded a dull yellowish viscous fluid. Histologic examination revealed many small cysts of varying diameters in the solid component of the specimen (Fig. 3). The cyst wall was composed of multiple layers, with a lamellar eosinophilic structure. No definite scolex was found in the small cysts. The diagnosis of adrenal AE was confirmed through pathologic examination. The enlarged lymph nodes around the mass showed reactive hyperplasia.
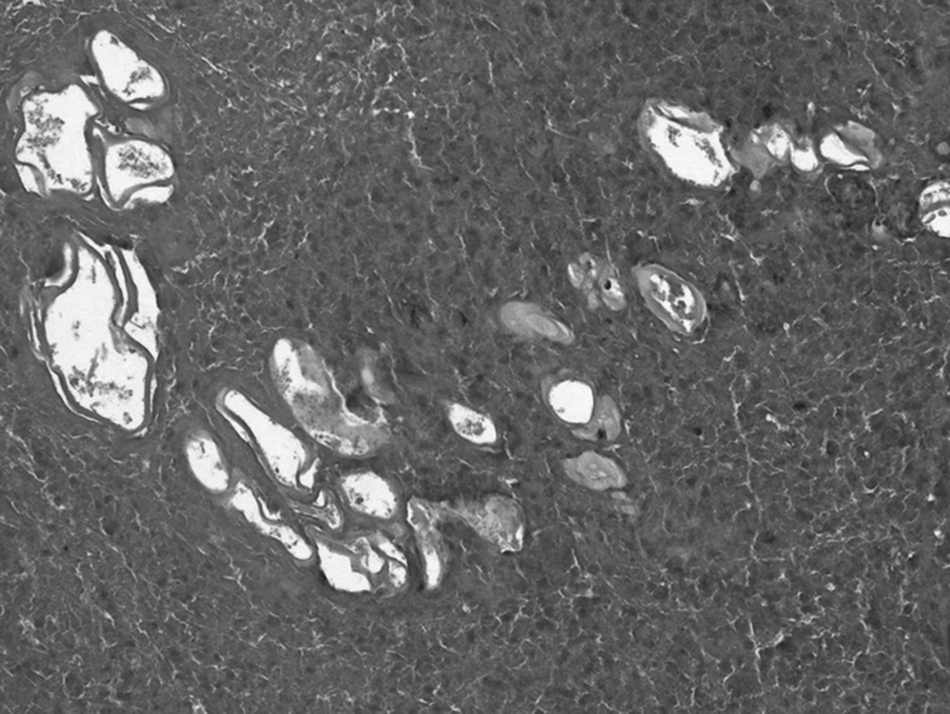
Histologic examination of the mass reveals many small cysts in its solid components. The walls of the cysts consisted of multiple layers. (Hematoxylin and eosin staining, original magnification,×200).
After excision of the adrenal mass, the patient was treated with four cycles of albendazole 400 mg BID, given with meals for 4 wks each and followed by 2-wk albendazole-free intervals. A follow-up CT at 10 mo showed no evidence of recurrence of echinococcosis.
Discussion
Echinococcosis is a common parasitic disease in rural areas, and can affect both human beings and animals. The most frequent occurrence of echinococcosis is in the liver, followed by the lungs, but it is rare in other organs [4]. Primary extrahepatic hydatid infection is more common in CE than in AE [5]. The adrenal gland is a rare extrahepatic site of echinococcosis [6,7], and particularly of AE. We are aware of only one previous case of primary AE involving the adrenal gland [8]. Although AE is benign, it shows the characteristics of a malignant tumor such as destructive tissue growth, invasion of adjacent structures, and the occurrence of metastases in distant organs [3,9,10]. In addition, an acute immunologic reaction, such as anaphylactic shock, may be caused by the rupture of a hydatid cyst in patients with CE [11], and patients with suspected echinococcosis should therefore have the condition diagnosed and treated as early as possible.
Patients with adrenal echinococcosis usually have nonspecific clinical symptoms caused by space-occupying lesions [12]. According to the literature and the case presented here, patients with adrenal CE or AE have a high frequency of ipsilateral flank pain and occasional hypertension [8]. However, these clinical symptoms do little to suggest the possibility of echinococcosis. Thus, the pre-operative diagnosis of AE depends mainly on imaging and serologic examination. Imaging studies can confirm the existence and extent of the parasitic lesion in AE, whereas serologic testing reveals antibodies or antigens specific to the disease. The diagnosis of CE must be made in close conjunction with the patients' history. It is helpful to determine whether patients come from areas in which AE is epidemic or have a history of animal contact (e.g., with sheep or cattle).
Imaging examinations for echinococcosis include USG, CT, and magnetic resonance imaging (MRI) [13,14]. Ultrasonography is useful for a screening diagnosis, whereas CT and MRI are supporting examinations after USG. These examinations permit accurate understanding of the location, number, extent, and characteristics of the lesion in a patient with AE. Findings typical of CE on USG, CT, or MRI are solitary or multiple round or spherical cystic lesions with clear boundaries [10]. The findings may also include calcification and daughter cysts of visibly different sizes in the fluid. If the endocyst membrane of a hydatid cyst peels off, the pathognomonic “water-lily sign” is demonstrated [15]. Alveolar echonococcosis appears as an inhomogeneous pseudotumor with irregular boundaries, an irregular central pseudocystic appearance resulting from necrosis, and infiltration into the surrounding structures. On contrast-enhanced CT, the periphery of the mass may be enhanced and multicentric vesicles may be seen. Magnetic resonance imaging may show multi-vesicular morphology, which supports the diagnosis of AE. Calcifications in AE and CE are different, and are characteristic features of AE. In contrast to the thin, crescent- or ring-shaped calcifications found only in the cyst wall of CE, clusters of microcalcifications or plaque-like calcific foci with an irregular distribution in central or peripheral parts of the lesion are observed in AE [10]. In the present case, all of the findings on imaging of the patient's adrenal mass were consistent with those of AE. However, the CT features in this case differed from those in a previous case of adrenal AE reported by Kamishima et al. [8] because of the difference in the developmental stage of the two lesions.
The definitive diagnosis should be confirmed by pathologic or serologic examination. Puncture of cysts has not been a routine diagnostic method in suspected CE because of fear of anaphylactic reactions or secondary echinococcosis. Serologic examination for a specific antibody or core antigen is helpful when diagnosing echinococcosis. The antibody detection assay is sensitive for diagnosing hydatid cyst, whereas the antigen detection assay may be useful for assessing the efficacy of treatment [16]. To date, no single examination has proved to be the best method for diagnosing echinococcosis. Thus, multiple examinations should be used to improve diagnostic accuracy [17,18]. The indirect hemagglutination test, enzyme-linked immunosorbent assay, and latex agglutination assay have relatively high sensitivities for CE, but their specificity is limited by cross-reactions. In dubious cases of CE, confirmatory tests for the arc 5 antigen, the 8-kDa or 12-kDa subunit of antigen B, or immunoblotting for the 8-kDA subunit of antigen B (EgAgB8/1) of E. granulosus must be used [19,20]. Purified, recombinant, or in vitro-produced E. multilocularis antigens (e.g., Em2, Em2+, Em18,) have high diagnostic sensitivity and specificity for AE [19]. Most of the purified antigens can also discriminate most cases of AE from CE. Immunoblotting tests may be useful for confirming AE or as a first-line investigation if available readily.
The definitive method of treatment for CE is surgical intervention. An alternative method for some types of CE has been proposed. Puncture, aspiration, injection, and re-aspiration (PAIR), which is a minimally invasive technique used in treating cysts in the liver and other abdominal locations, has been proposed as an alternative method for treating some types of CE [21]. The exogenous ascus of AE can invade surrounding tissues and structures, which may spread the disease to other parts of the body. Therefore, the goals of treating AE are to stop invasion of the lesion into surrounding structures and to prevent dissemination. At present, the primary method for treating AE is radical surgical resection followed by anti-infective therapy with benzimidazoles [22,23]. The adrenal gland may be completely excised or partly according to the state of the adrenal AE [24]. In the case of our patient, the lesion and adrenal gland were resected radically because the adrenal mass involved surrounding structures. Treatment with albendazole was prescribed after the operation. With this approach, the patient was cured. Buttenschoen et al. [25] suggested that the resection of AE should not be restricted to the lesion but should be extended routinely to remove regional lymph nodes. This procedure reduces the risk of persistent infection from infected regional lymph nodes.
Although primary adrenal AE is rare, it should be included in the differential diagnosis of adrenal masses, particularly in the areas where echinococcosis is prevalent. Imaging examinations including USG, CT, and MRI can depict clearly the location, characteristics, and surrounding conditions of the parasitic lesion, which facilitates its diagnosis and the planning of surgical treatment.
Footnotes
Acknowledgments and Author Disclosure Statement
There was no funding for this article. All authors report no conflicts of interest relevant to this article.