
Abstract
Abstract
Background:
A nosocomial outbreak of multi-drug-resistant Acinetobacter calcoaceticus–A. baumannii (MDR-ACB) complex infection occurred in a newly constructed building at a 2,500-bed tertiary medical center in Taiwan.
Methods:
An investigation was carried out by molecular approaches to trace the bacteria. Antimicrobial susceptibilities, risk factors, and the occurrence of nosocomial MDR-ACB infections were investigated. From January to December 2009, 53 patients were infected with MDR-ACB, and 23 environmental surveys were performed in two surgical intensive care units (ICUs) within the new building. Forty-two clinical isolates were obtained from patients and 22 samples from nine environmental surveys.
Results:
Forty clinical isolates (95.2%) and 18 environmental samples (81.8%) were positive for MDR-ACB of type A, the predominant outbreak strain. This strain was identical to that isolated in an outbreak in the old hospital in 2006, as proved by repetitive extragenic palindromic-based polymerase chain reaction and pulsed-field gel electrophoresis. Although the outbreak isolates contained blaOXA-23-like and blaOXA-51-like genes, analysis of the antimicrobial susceptibilities demonstrated increases in resistance to cefepime and imipenem-cilastatin in MDR-ACB isolated in the later outbreak.
Conclusions:
Not only patients or healthcare workers, but also medical equipment, might have carried the predominant outbreak strain from the old district to the new building. Therefore, even in a new environment, infection control programs must be enforced continually, and healthcare providers must be educated repeatedly to prevent recurrent outbreaks of MDR-ACB infection in the hospital setting.
Multi-drug-resistant ACB (MDR-ACB) complex is an increasing threat to hospitalized patients, particularly those in intensive care units (ICUs); and it imposes therapeutic challenges [6,7]. Carbapenems, including imipenem-cilastatin and meropenem, are the treatments used most commonly; however, an increase in the number of prescriptions for carbapenems has led to an increase in the number of resistant Acinetobacter strains [8,9]. Among Acinetobacter isolates, class D β–lactamase (OXA-23-, OXA-24-, and OXA-58-type carbapenemase) has been reported as the most prevalent mechanism of resistance [10].
Hospitalized patients can acquire MDR-ACB infections by various modes of transmission, including cross-transmission among patients, transmission by healthcare workers, invasive procedures, and contamination of the surrounding environment [11–14]. Comprehensive infection control programs can prevent an outbreak of MDR-ACB in hospitals [11,15]; thus, control of sporadic outbreaks of MDR-ACB infection is a critical policy issue for medical centers.
Throughout 2006, sporadic outbreaks of Acinetobacter spp. infection occurred in China Medical University Hospital, a 2,500-bed university hospital in central Taiwan [14]. In October 2008, a newly constructed building was opened more than 500 m from the older district hospital. However, beginning in February 2009, gradual increases in the number of MDR-ACB isolates were found in two surgical ICUs in the new building. The aim of this study was to investigate the antimicrobial susceptibilities and molecular epidemiology of the MDR-ACB isolates in the new building and to determine whether there was a predominant strain in both the new and old districts. The relation of risk factors such as invasive medical procedures to the occurrence of MDR-ACB infections also was investigated.
Patients and Methods
Study design and epidemiologic surveillance in surgical ICUs
Retrospectively, we collected all isolates of MDR-ACB from the trauma and surgery intensive care unit (ICU-A) and the neurosurgical intensive care unit (ICU-B) from January 1, 2009 to December 31, 2009. These two ICUs are located on consecutive floors in the newly constructed hospital building. In addition to positive cultures of MDR-ACB, all patients had clinical infection signs, including fever >38°C, pyuria for urinary tract infection, purulent sputum for pneumonia, pus discharge from a surgical site, or erythema over central vascular catheter insertion sites. Demographic and clinical data were collected by medical chart review for each patient with a positive MDR-ACB culture. The patient-days for the resident patients with MDR-ACB infection were the time before acquisition of isolates. Cultures were obtained of the hands of the in-charge healthcare workers after washing to evaluate the efficacy of hand-washing procedures.
Bacterial culture and antimicrobial susceptibility testing
All isolates from patients (except blood cultures, which were processed initially with a Bactec 9000 system [Becton Dickinson, Sparks, MD]) or environmental samples were streaked across Trypticase soy agar with 5% sheep blood (TSA II)/Levine EMB agar (Becton Dickinson) and incubated at 37°C. Bacterial isolates were identified as ACB complex, and the antibiotic susceptibilities of the isolates were determined using a BD Phoenix™ Automated Microbiology System (Becton Dickinson), as described previously [14]. Antimicrobial susceptibility was confirmed by disk diffusion following the guidelines and criteria of the Clinical Laboratory Standards Institute [16]. The definition of multi-drug resistance was resistance to three or more classes of the following antimicrobial agents: Anti-pseudomonal cephalosporins, anti-pseudomonal carbapenems, β-lactam/β-lactamase inhibitor combinations, anti-pseudomonal fluoroquinolones, and aminoglycosides [9,17].
Molecular fingerprinting by repetitive extragenic palindromic-based polymerase chain reaction (REP-PCR)
The Acinetobacter isolates were prepared for extraction of genomic DNA as described previously [14]. Consensus primers for the REP sequences found in many bacterial chromosomes, including those of Acinetobacter spp., were used in the REP-PCR [18–20]. To prepare genomic DNA, the bacterial pellets were resuspended in 600 mcL of lysis buffer (20 mM Tris Cl, pH 7.5; 10 mM ethylene diamine tetraacetic acid, 40 mM NaCl, 0.2% sodium dodecyl sulfate, and protease K 200 mcg/mL) and incubated at 50°C for 45 min. The DNA was extracted with 1:1 phenol:chloroform solution. The paired primers REP-1 (5′-IIIGCGCCGICATCAGGC-3′) and REP-2 (5′-ACGTCTTATCAGGCCTAC-3′) were used to amplify putative REP-like elements in the bacterial DNA [19]. The procedures for amplification by REP-PCR and interpretation of fingerprint profiles were as described previously [19]. A negative control containing everything except the DNA extract, which was replaced with 5 mcL of sterile distilled H2O, was included in each PCR run to rule out reagent contamination. Gel electrophoresis was used to separate the REP-PCR amplification products, which were compared with molecular weight standards. A standard strain of A. baumannii (ATCC 19606; American Type Culture Collection, Manassas, VA) was compared with isolated strains from patients and environmental samples. Each isolate was run in duplicate, and fingerprint profiles were interpreted by researchers who were blinded to the clinical data. For detection of genes encoding blaOXA-23-like and blaOXA-51-like, a multiplex PCR assay was performed as described previously [21].
Genotyping by pulsed-field gel electrophoresis (PFGE)
Bacterial isolates from patients and the environment were genotyped using pulsed-field gel electrophoresis (PFGE) according to a manual protocol (Bio-Rad, Hercules, CA). The PFGE analysis was carried out as described previously [22]. The bacterial genomic DNA was prepared and digested with ApaI (New England BioLabs, Ipswich, MA). The digested fragments were subjected to PFGE, which was conducted with 6 V/cm gradient at 14°C and with 3–8-s pulse intervals for 10.5 h followed by 12–20-s pulse intervals for 10.5 h. The gel was stained and analyzed using BioNumerics software (Applied Maths, Austin, TX). Pulsotypes were assigned to clusters with >80% similarity from the dendrograms.
Statistical analysis
Comparisons between patient groups were analyzed by χ2 tests for categorical variables or paired t-tests for continuous variables. A p value<0.05 was considered statistically significant.
Results
Molecular characterization of nosocomial outbreak caused by MDR-ACB
From January 1, 2009 to December 31, 2009, there were 64 isolates of MDR-ACB from 53 patients and 23 environmental surveys in the ICU-A and ICU-B. All 64 isolates were found to be resistant to all beta-lactams (except sulbactam), fluoroquinolones, aminoglycosides (except three isolates sensitive to amikacin), and trimethoprim–sulfamethoxazole. The sites of environmental surveys were ventilator surfaces, bed rails, bedside curtains, monitors, and tables. From the 53 patients, 42 clinical isolates were available for genomic fingerprinting, with 29 from ICU-A and 13 from ICU-B. The origin sites of positive cultures in two ICUs were as follows: Four tips of central vascular catheters, three urine, five wound pus, nine sputum, 12 blood, and two body fluids from ICU-A; and two tips of central vascular catheters, two urine, two wound pus, nine sputum, two blood, and one body fluids from ICU-B. Of the 23 environmental surveys, nine yielded positive cultures (six from ICU-A and three from ICU-B), resulting in 22 samples that were suitable for genomic fingerprinting. There was no positive culture from the hands of healthcare workers.
The 64 MDR-ACB isolates subjected to fingerprinting were distributed among four PFGE patterns, pulsotypes A to D (Fig. 1). Among these types, the most frequent isolate was type A, which accounted for 58 isolates (90.6%), with 40 isolates from patient samples and 18 isolates from environmental samples. The other six samples were determined to be type B (one patient isolate from blood), type C (one patient isolate from urine and one environmental isolate), or type D (three environmental isolates). A second molecular approach, REP-PCR, was used to validate the bacterial genomic patterns and distribution of the clinical isolates [14]. The data from the REP-PCR analysis confirmed the four distinct genomic profiles and the distribution of the 64 clinical isolates among the four profiles (data not shown).
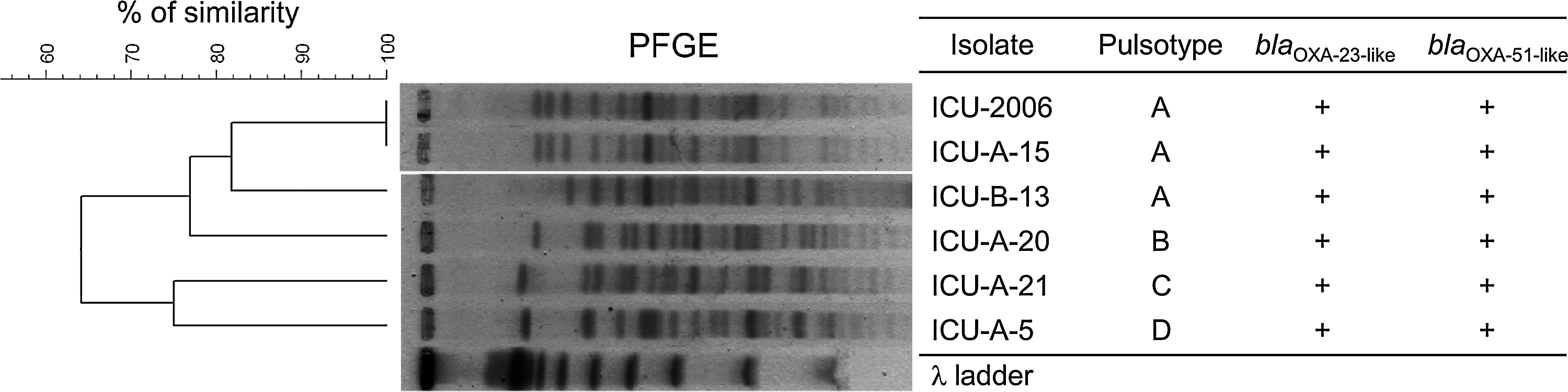
Representative pulsed-field gel electrophoresis patterns of multi-drug-resistant Acinetobacter calcoaceticus–baumannii isolates in intensive care units (ICUs) in old hospital (ICU-2006) and new building (ICU-A and ICU-B). Dendrogram was produced by BioNumerics software, showing distance calculated by the Dice similarity index of ApaI-digested DNA fragments. Degree of similarity is shown on the scale. Similarities >80% assign strains to the same cluster. Isolated locations are shown on right.
To further determine whether the 2009 MDR-ACB outbreak strain was the same as the 2006 outbreak strain that occurred in the old building of this hospital [14], a sample from the 2006 strain was analyzed using PFGE and compared with samples from the 2009 outbreak. As shown in Figure 1, the 2006 outbreak strain (pulsotype A; ICU-2006) from the old hospital district was identical to the predominant 2009 outbreak strains (pulsotype A; ICU-A-15 and ICU-B-3) from the new building. Type A MDR-ACB thus was the major causative nosocomial outbreak strain in our hospital in 2009, the same strain that was responsible for the 2006 nosocomial outbreak.
Antimicrobial susceptibilities in MDR-ACB isolates
The blaOXA-23-like and blaOXA-51-like genes were detected in MDR-ACB isolated in both the 2006 and 2009 outbreaks (Fig. 1). The antibiograms changed somewhat between the two outbreaks, in that there was a higher rate of cefepime resistance in 2009 (100%) than in 2006 (77.8%)(p<0.05) (Fig. 2) and the resistance rate to imipenem-cilastatin increased from 82.5% in 2006 to 100% in 2009 (p<0.05). Similar results were found for ampicillin-sulbactam and piperacillin-tazobactam, in that the resistance rates increased slightly from 2006 to 2009. However, all the MDR-ACB isolates remained susceptible to colistin. Changes in imipenem-cilastatin and cefepime resistance were the most notable changes in MDR-ACB susceptibilities between the two outbreaks.
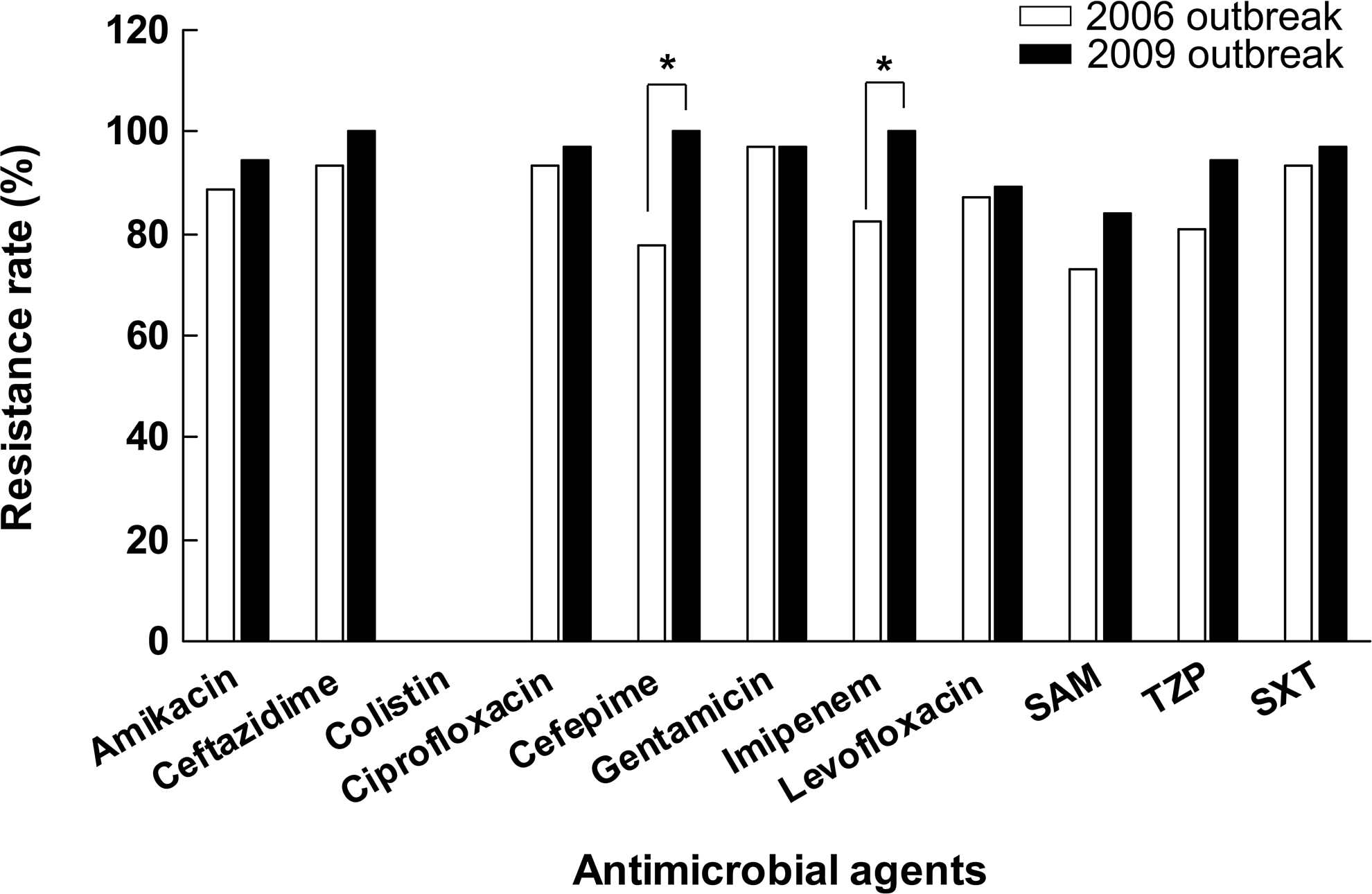
Antimicrobial resistance rates of multi-drug-resistant Acinetobacter calcoaceticus–baumannii isolated in 2006 and 2009. SAM=sulbactam-ampicillin; TZP=tazobactam-piperacillin; SXT=sulfamethoxazole–trimethoprim. *p<0.05.
Surveillance of MDR-ACB outbreaks in surgical ICUs
The timeline and spatial distribution of patients and environmental surveys with positive cultures of MDR-ACB in ICU-A and ICU-B are represented in Figure 3. There were 11 clinical isolates (six in ICU-A and five in ICU-B) that were not available for genomic fingerprinting. Those isolates are referred to as “unavailable MDR-ACB” in Figure 3. In ICU-A, there were only three beds (numbered 12, 13, and 19) without any MDR-ACB–infected patients in 2009 (Fig. 3A). Bed number 5 had the most cases of infection, and this bed also had a positive environmental survey. The peak in the outbreak of type A MDR-ACB infection in ICU-A occurred between October 2009 and December 2009 (Fig. 3B). In ICU-B, more than one-half of the beds had patients who acquired an infection with MDR-ACB (Fig. 3C). The genomic fingerprint for all available MDR-ACB isolates from patient and environmental samples in ICU-B was confirmed as pulsotype A. The peak of the epidemic in ICU-B occurred in October 2009 (Fig. 3D). The evidence indicates that pulsotype A MDR-ACB was the major outbreak strain in the two surgical ICUs in the newly constructed hospital building.

The spatial (
Discussion
Nosocomial infection with Acinetobacter spp. is associated with a broad range of disease, including pneumonia, bacteremia, urinary tract infections, surgical site infections, and meningitis [3–5]. Infection with MDR-ACB is believed to increase mortality rates among hospitalized patients [23,24]. Previous studies reported that in ICUs, outbreaks of infection with MDR-ACB often result from cross-transmission among patients [11,13,25]. Additionally, patients in ICUs who receive invasive procedures (central vascular catheterization, Foley catheterization, mechanical ventilation, nasogastric tube insertion, or hemodialysis) have a significantly higher risk of infection with MDR-ACB [12,14]. Molecular epidemiology methods often are used to discriminate strains of MDR-ACB during nosocomial outbreaks [14,18,26]. In the current study, the investigation took place in the clinical setting of two surgical ICUs in a new building at our hospital. The new building provides critical care for patients who may have been transferred from emergency departments at our hospital or others. It is important to note that all of the enrolled patients received critical care with invasive procedures and were hospitalized in ICUs; thus, these patients were likely at a higher risk of acquiring MDR-ACB [27].
Our data indicate that the organisms involved in the MDR-ACB outbreak contained at least two genes conferring resistance to class D carbapenemas, blaOXA-23-like and blaOXA-51-like, which contributed to imipenem-cilastatin resistance. This result was similar to a previous report that both blaOXA-23-like and blaOXA-51-like genes were detected in carbapenem-resistant A. baumannii isolates in central Taiwan [28]. Notably, the carbapenem and cefepime resistance rates were increased significantly, from 82.5% and 77.8%, respectively, in 2006, to 100% for both in 2009. The deteriorating antimicrobial susceptibilities may result from both the dissemination of the major outbreak strain and the persistent selective pressure of antibiotics prescribed in our hospital.
In this study, we used molecular approaches to determine that type A (referred to as type 1 in the paper on the 2006 outbreak [14]) MDR-ACB is a predominant clonal strain in our hospital regardless of the district. Several reports have revealed that major outbreaks of Acinetobacter clones in ICUs often involve the same genotype in clinical and environmental samples [11,12]. These findings indicate that the predominant clonal strains might have higher tolerance and virulence, leading to resistance to environmental cleaning or infection control interventions and to more severe infections and poor patient outcomes, as mentioned in other papers [11,25]. The recurrence of major outbreaks of MDR-ACB clones in our hospital therefore needs to be watched for continuously and brought to the attention of healthcare workers more frequently.
Patients and healthcare workers were not exposed to the newly constructed building before it began operating in October 2008. Additionally, the new hospital district is located more than 500 m from the old district. After opening of the new building, most patients, healthcare workers, and medical equipment (including beds, monitors, ventilators, etc.) were transferred to it. There was no sharing of healthcare workers or equipment between the two ICUs except, rarely, ventilators. This may have been the main transmission route by which the same MDR-ACB strain emerged in the new district, despite attempts to disinfect the old medical equipment and the admission of new patients from emergency departments or other hospitals. Our findings are similar to the circumstances surrounding outbreaks of MDR-ACB infection in the U.S. military healthcare system [29]. Additionally, several studies have documented the spread of ACB through various modes, including contamination of medical equipment, computer devices, and the surrounding environment, or transmission by healthcare workers and during medical procedures [11–13].
Comprehensive and multifaceted infection control interventions are necessary to reduce nosocomial outbreaks of ACB infection [11–15,30]. During the outbreak in our hospital in 2006, a series of sustained infection control programs was enforced to stop the emergence of new cases [14]. The second outbreak of MDR-ACB infection might have been attributable carryover of this virulent bacterium by patients or inadequately disinfected equipment during the transfer from the old district building to the new one. Also, the attention of the medical staff to the infection control program may have been less in the new environment, which was not associated with the previous outbreak of nosocomial infections, which might have accelerated the outbreak in the new building. In May 2009 in ICU-A and in October 2009 in ICU-B, enhanced infection control procedures (other than standard universal precautions) were implemented, including repeated environmental surveys and disinfection until no further positive cultures were found and reduced use of unnecessary antibiotics. However, although one result was a decrease in case numbers, the infection potential was not eradicated. Furthermore, the number of infected ICU-A patients rose by the end of 2009, resulting in prolonged enforcement of the infection control interventions described above, combined with repeated education and monitoring of medical staff.
In conclusion, our results suggest that the same MDR-ACB strain spread from the old district to a new building, most likely through patients, healthcare workers, or medical equipment. The present study also indicates that infected patients and contaminated environment are important reservoirs for MDR-ACB. Prolonged, aggressive, comprehensive infection control interventions, combined with repeated education and surveillance of healthcare providers, are crucial for getting an outbreak of nosocomial MDR-ACB infection under control.
Footnotes
Acknowledgments and Author Disclosure Statement
This study was supported by the National Science Council of Taiwan (NSC 100-2313-B-039-003), China Medical University and Hospital (DMR98-023, 99-035 and CMU99-ASIA-21), Clinical Trial and Research Center of Excellence Funds (DOH101-TD-B-111-004) from the Taiwanese Department of Health, and Tomorrow Medical Foundation.
No conflicting financial interests exist.