
Abstract
Abstract
Background:
Multiple organ dysfunction syndrome (MODS) is the leading cause of death in intensive care units throughout the world. Several composite clinical scores, such as the Multiple Organ Dysfunction (MOD) score and Sequential Organ Failure Assessment (SOFA) score, have been developed to assess the severity of critical illness and predict mortality. Survival in fully manifest MODS is nearly unprecedented.
Methods:
Case report and review of the relevant literature.
Case Report:
A 55-year-old male was admitted to the neurologic intensive care unit with left lateral medullary syndrome, and access for permanent enteral feeding was indicated. On day 7 of the patient's hospitalization an attempt was made to place a gastrostomy tube in the patient, but the procedure was aborted after unexplained intra-operative hemodynamic instability. Eight days later the patient developed florid MODS of unclear etiology. His daily MOD and SOFA scores peaked at 16 and 20, respectively, and his cumulative MOD and SOFA scores peaked at 19 and 22, respectively, portending 100% mortality. Over the next 6 wks the patient gradually recovered nearly all organ function, until both his MOD and SOFA scores decreased to 1. He was discharged to a sub-acute rehabilitation facility.
Conclusions:
This patient is the oldest patient reported to have survived fully manifest MODS. Whereas scoring systems such as the MOD and SOFA systems can be useful tools, they have several limitations and their results must be interpreted with caution.
M
It is estimated that 14% of all patients admitted to intensive care units (ICUs) develop MODS during their stay, and the syndrome is responsible for up to 80% of all deaths in the ICU [7,8]. Despite an ever-increasing understanding of the pathophysiology of MODS and some modest improvements in survival in the syndrome, it continues to be the leading cause of death in ICUs worldwide, especially for surgical patients [9].
Several clinical assessment systems have been developed to assist clinicians in assessing the severity of critical illness and predicting morbidity and mortality. Two of the most widely used such systems are the Multiple Organ Dysfunction (MOD) scoring system and the Sequential Organ Failure Assessment (SOFA) [10,11]. Both assign points (0 to 4) for increasing levels of dysfunction of the six organ systems that are most frequently affected in MODS, with a maximum score in both systems of 24 points. These systems are the cardiovascular, pulmonary, hepatic, renal, coagulation, and neurologic systems. When the total SOFA score >15, mortality is approximately 90%, and with a MOD score >20 the mortality is reported to be 100% [10,12]. The MOD and SOFA systems represent an improvement over earlier risk-stratification systems because, unlike earlier systems with scores that were designed to be calculated only on the day of admission, the MOD and SOFA scores may be re-calculated on a daily basis, and a practitioner can use the initial, aggregate, and trended scores in both systems to obtain more accurate predictions of mortality [13]. The SOFA score offers the putative advantage of taking into account support measures such as vasopressors, inotropic agents, and renal replacement therapy when calculating it, whereas the MOD score is based only on objective clinical parameters such as laboratory values and vital signs [14]. We here report the case of a patient who experienced a catastrophic intra-operative event that resulted in fully manifested MODS but who survived despite having a predicted mortality of nearly 100% on the basis of both his MOD and SOFA scores.
Case Report
A 55-year-old male was admitted to the neurologic ICU with left lateral medullary syndrome caused by acute occlusion of his left vertebral artery. He presented to the emergency department with dizziness of sudden onset, blurry vision, dysphagia, dysarthria, truncal ataxia, and loss of pain and temperature sensation in his right upper and lower extremities. His medical history included a prior transient ischemic attack, hypertension, type II diabetes mellitus, and multiple prior abdominal operations (diaphragmatic hernia repair, laparoscopic cholecystectomy, and two umbilical hernioplasties treated with mesh reinforcement. After 7 d of anti-platelet therapy his neurologic symptoms resolved, except for persistent dysphagia that made oral intake unsafe for the patient. A general surgery consultation was requested for enteral feeding access. It was noted that the patient's family reported a “bad reaction” following general anesthesia for his first operation, which resulted in a nine-day hospitalization, but further detail about this episode was unavailable.
Pre-operatively the patient's temperature was 36.8° C, his heart rate was 95 beats/min, his blood pressure (BP) was 129/86 mm Hg, and his SaO2 was 99% (FIO2 0.21). He was conscious and alert, demonstrated 5/5 strength of all four extremities, had decreased pinprick sensation on his left face and right body, and had left cerebellar ataxia and slight rotatory nystagmus. Cardiopulmonary examination yielded normal findings. The patient's abdomen was soft, non-tender, and non-distended with no organomegaly, and he had multiple well-healed surgical incisions (“chevron” incision, peri-umbilical midline incision, and four laparoscopic port incisions). His preoperative laboratory results were notable for a white blood cell count (WBC) of 11,200/mm3, hematocrit of 33.9%, platelet count of 245,000/ mm3, and serum creatinine concentration of 1.0 mg/dL. The remainder of the patient's comprehensive metabolic panel and coagulation profile was normal (Table 1).
During renal replacement therapy.
Cr=creatinine; GCS=Glasgow Coma Scale; HCT=hematocrit; MOD=multiple oprgan dysfunction; NR=not recorded; POD=post-operative day; SOFA=Sequential Organ Failure Assessment; T bili=total bilirubin; WBC=white blood cells.
On day 7 of his hospitalization the patient underwent an attempted Stamm gastrostomy under general endotracheal anesthesia (percutaneous endoscopic gastrostomy was contraindicated because of the patient's multiple prior upper abdominal operations). The patient's vital signs at the start of the procedure were notable for sinus tachycardia with a heart rate of 112 beats/min, a BP of 155/80 mm Hg, and an SaO2 of 100% (FIO2 1.0). A vertical upper-midline incision encountered dense left upper quadrant adhesions. After 20 min of adhesiolysis, the patient's BP decreased rapidly to 60/40 mm Hg with a heart rate of 100 beats/min, and his SaO2 decreased to 86% (FIO2 1.0). Infusions of norepinephrine, phenylephrine, and epinephrine were initiated but resulted in an increase in BP to only 95/55 mm Hg. The patient was ventilated manually for approximately 10 min until his SaO2 returned to 98%. A chest radiograph confirmed proper endotracheal tube placement and the absence of pneumothorax; intra-operative fiberoptic bronchoscopy (FOB) revealed only scant thin secretions without airway obstruction. Intra-operative laboratory values were normal and essentially unchanged from previous values. An electrocardiogram (ECG) revealed non-specific ST-wave abnormalities; serial cardiac enzyme determinations yielded normal results. The patient was then transferred to the surgical intensive care unit (SICU) in critical condition approximately 90 min after his hemodynamic instability began. He maintained a pulse throughout this event, and chest compressions and defibrillation were therefore not administered.
Upon admission to the SICU the patient required the administration of three vasopressor agents to maintain his mean arterial pressure (MAP) above 60 mm Hg, but his oxygenation and ventilation were normal and his urine output was adequate. On post-operative day (POD) 2 his hematocrit decreased from 38% to 20%. A non-contrast-enhanced computed tomography (CT) scan of the patient's abdomen and pelvis revealed a 10x14x14-cm epigastric intra-abdominal hematoma believed to be the result of the adhesiolysis. Eight units of packed red blood cell concentrates (PRBC), eight units of fresh-frozen plasma (FFP), and two units of platelets were transfused over the next 24 h. On that same day the diagnosis was made of an acute left popliteal venous thrombus (DVT), and an inferior vena cava filter was placed. By POD 3 the patient was weaned from vasopressors but remained ventilator-dependent, with a Glascow Coma Scale (GCS) score of three points off of sedation and analgesia.
On POD 10 the patient suddenly became hypotensive, tachycardic, hypoxemic, and oliguric. Administration of voluminous crystalloid produced no improvement in his condition, and treatment with two vasopressors was resumed. A comprehensive investigation revealed evidence on FOB of pulmonary aspiration of gastric contents, and bronchoalveolar lavage (BAL) fluid culture grew >104 colony-forming units (CFU)/mL of multi-drug-resistant (MDR) Escherichia coli. The patient's laboratory data on POD 11 were notable for a white blood cell count of 17,300/mm3, hematocrit of 28%, platelet count of 264,000/mm3, serum creatinine concentration of 3.0 mg/dL, and serum total bilirubin concentration of 1.4 mg/dL (Table 1). He developed acute respiratory distress syndrome requiring positive end-expiratory pressure (PEEP) at a maximum of 30 mm Hg during airway pressure release ventilation (APRV). Maximum doses of three vasopressors and dobutamine were required for circulatory support. The patient also developed a prolonged ileus, and a total bilirubin concentration that peaked at 10.3 mg/dL and aspartate aminotransferase (AST) concentration that peaked at 23,000 IU/L, which is consistent with “shock liver.” Anuria with a peak serum creatinine concentration of 3.53 mg/dL was treated with continuous venous–venous hemodialysis (CVVHD). A nadir platelet count of 26,000 mm3 occurred despite multiple platelet transfusions. Frequent periods of freedom from sedation revealed neurologic unresponsiveness except for brain stem reflexes. The patient's daily MOD score peaked at 16 points on POD 12 and his cumulative MOD score was 19, indicating a 90% risk of mortality (Fig. 1) [10]; his daily SOFA score peaked at 20 points on POD 13 and his cumulative SOFA score was 22, indicating a 100% likelihood of mortality (Fig. 1) [11,15].
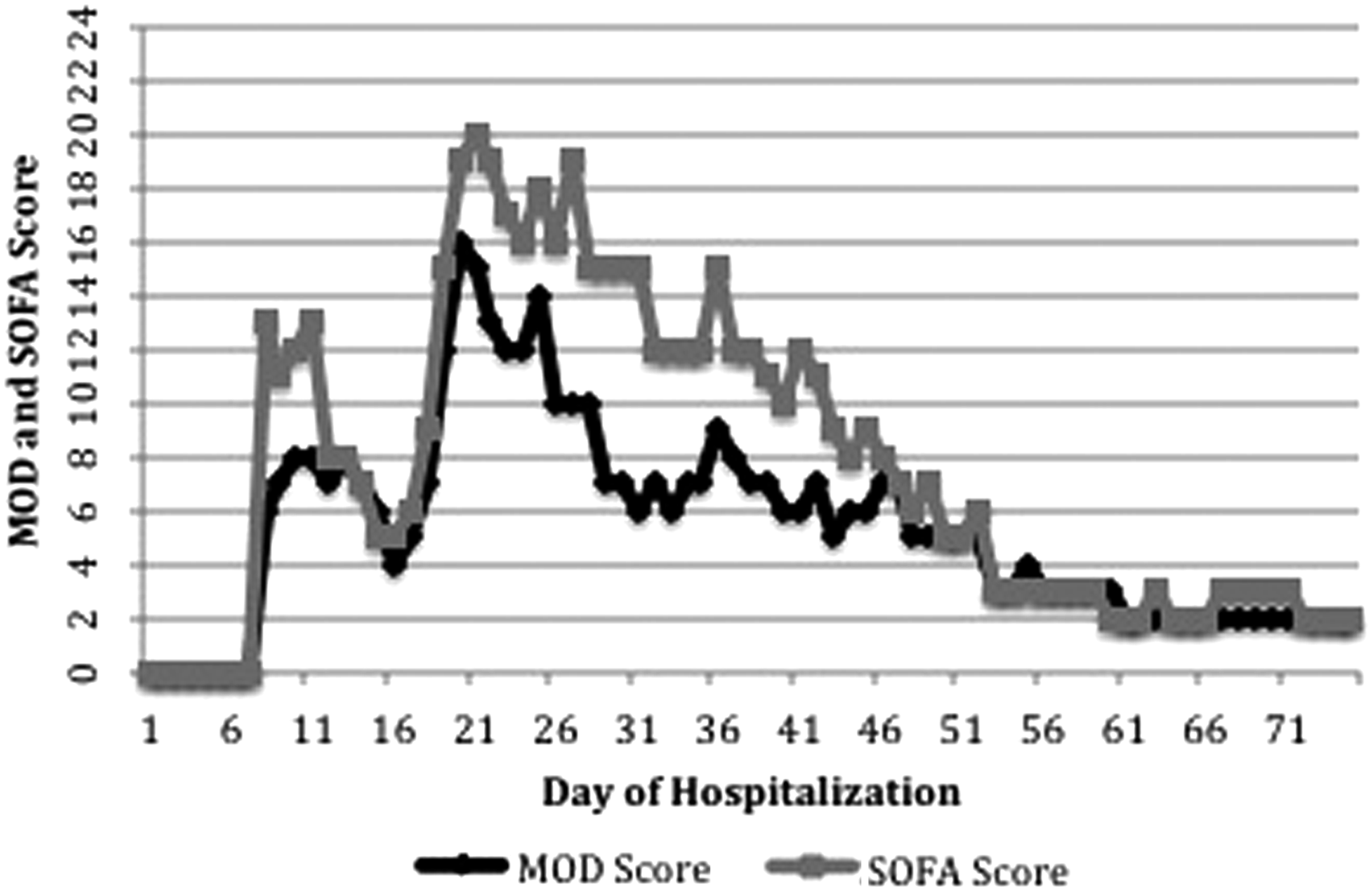
Daily Calculated Multiple Organ Dysfunction and Sequential Organ Failure Assessment scores.
The patient's florid MODS continued for 11 d with minimal improvement. He completed 8 d of broad-spectrum antibiotic treatment for his E. coli pneumonia, and empiric therapy for septic shock according to guidelines of the Surviving Sepsis Campaign [16], except that drotrecogin alfa (activated), still available at the time, was contraindicated in his case. During the next 4 wks gradual signs of improvement were observed in all of the patient's organ systems (Table 1). Findings on electromyography and nerve conduction studies were consistent with severe polyneuropathy of critical illness. The patient demonstrated a slow return of motor function, moving his eyes and facial muscles initially, and then his shoulders, and after this his extremities (upper before lower). His treatment with vasopressors was stopped on POD 24. His liver enzymes and bilirubin returned to normal by POD 30, and his ventilator support was minimized by POD 42. His renal function returned gradually and his renal replacement therapy was discontinued on POD 44. By POD 53 the patient's daily MOD and SOFA scores had decreased to 2 points each, awarded for a persistent GCS of 11 (Fig. 1).
After a nearly complete recovery from the critical phase of his MODS, the patient experienced several additional complications that led to his having an additional 4-mo stay in the SICU. These included two episodes of lower gastrointestinal hemorrhage (of an obscure source) that resolved with non-operative management, “urosepsis” from an E. coli infection of the urinary tract, a multi-drug-resistant Pseudomonas aeruginosa pneumonia, copious airway secretions, and paroxysmal supraventricular tachycardia. The patient was eventually weaned completely from the ventilator, was awake and alert, able to follow commands briskly and to sit upright unaided, regained 1/5 strength in his right upper and lower extremities, and vocalized short, incomprehensible sounds. On POD 181 he was discharged to a neurologic rehabilitation facility. His MOD and SOFA scores on discharge were both 1, earning a single point for a GCS of 13.
Discussion
The case described here is remarkable for at least two reasons. First, to our knowledge, it is only the third reported case in the literature of survival in fully-manifest MODS and involves the oldest patient to survive such a florid presentation of MODS, with all of these cases occurring at our center [17]. Several independent studies have demonstrated a 100% mortality of patients with a MOD or SOFA score >20 [15,18–21]. Furthermore, several studies have shown that trends in both the MOD and SOFA scores throughout the period of a patient's stay in the ICU are as useful for prognostication as are calculations of these scores on admission or at a particular time during the ICU stay. As shown in Figure 1, both the MOD and SOFA scores of the patient whose case is described in this report, for the 7 d before his aborted operation, were 0, and his two major episodes of deterioration, on days 9 and 20 of his hospitalization, were associated with increases in both scores.
The second remarkable feature of the present case is that despite an exhaustive investigation for the cause of the patient's dramatic intra-operative instability and subsequent MODS, no discrete etiology for this was ever found. The best chance of a recovery from severe MODS is achieved through identification and reversal of the underlying pathophysiology. For example, the two cases of full recovery from devastating MODS previously reported in the setting of regional enteritis were attributed to Clostridium perfringens sepsis and hemolytic-uremic syndrome for which directed medical and surgical treatments were administered promptly [17]. However, in the current case, our post-operative care was entirely supportive and the only directed therapy was for the pneumonia diagnosed on POD 11, long after the patient's initial manifestation of MODS. We speculate that the patient's initial intra-operative instability may have been caused by an anaphylactic reaction to one of the anesthetic agents given to him. As mentioned above, the patient had a history of a “bad reaction” to general anesthesia that led to a 9-d hospitalization after a simple hernia repair, which indicates that he may have been prone to unfavorable reactions to various anesthetic agents. However, the patient also underwent general anesthesia on several other occasions without incident, and the exact cause of his instability therefore remains a mystery.
After calculating the daily MOD and SOFA scores for this patient, we were somewhat surprised that his daily MOD score never exceeded 16 points and that his cumulative MOD score was only 19 points. As described in detail above, for a period of nearly seven days this patient required the available maximum ventilator assistance, the use of four vasopressor agents, renal replacement therapy, and multiple platelet transfusions for refractory severe thrombocytopenia in the setting of catastrophic bleeding. Despite this, his MOD score never reached the maximum of four points for the following organ systems: Renal (2), hepatic (3), cardiovascular (3), and hematologic (3). This highlights a weakness of the MOD score, in that it fails to account for the amount of support provided to the patient. However, the SOFA score does account for some supportive measures in its cardiovascular and renal scores, including the use of vasopressor agents and daily urine output as adjuncts to the measurement of BP and serum creatinine concentration alone [12]. This explains why the daily and cumulative SOFA scores of the patient in the present case were higher than his MOD scores during much of his hospitalization.
Another possible explanation for the patient's MOD and SOFA scores not being higher than they were is that his major post-operative deterioration occurred after he had been admitted to the SICU and was under close and continuous monitoring. Rapidly progressive instability of his condition was thus recognized and interdicted immediately and vasopressors were added to his treatment regimen before his mean arterial BP fell below 60 mm Hg for more than a few minutes. In addition, renal replacement therapy was initiated within hours of the onset of acute kidney injury, and the patient's serum creatinine concentration therefore never exceeded 3.53 mg/dL, and the uremic thrombocytopathy that was superimposed on his thrombocytopenia was eased. The MOD score incorporates the score for renal and cardiovascular dysfunction on the basis only of the serum creatinine concentration and the pressure-adjusted heart rate. Therefore, only two points were allotted to the MOD score of the patient in the present case for renal dysfunction, despite his nearly five weeks of renal replacement therapy, and only three points were awarded to his MOD score for cardiovascular dysfunction, despite his requiring three vasopressors and an inotropic agent.
This case reported here represents a dramatic presentation of fully manifest MODS in the oldest patient so far reported to survive this syndrome. Whereas scoring systems such as the MOD and SOFA systems can be useful instruments for assessing severity of illness and offering prognostic information, they have several limitations and their results must be interpreted with caution. Despite modern advances in surgery and critical care, the overall prognosis in MODS remains poor, and MODS remains the most common cause of death in ICUs throughout the world.
Footnotes
Author Disclosure Statement
No competing financial interests exist.