
Abstract
Abstract
Background:
Descending necrotizing mediastinitis (DNM) is a highly morbid infectious process. This uncommon disease process has carried historically a substantial burden of morbidity and mortality. In this study we hypothesized that application of a prospective modified management algorithm would decrease the morbidity and mortality from this highly destructive process.
Methods:
We developed a systematic approach for managing DNM, focusing on serial debridement guided by imaging, in conjunction with the use of broad-spectrum antibiotics and modern principles of critical care. We reviewed all patients admitted with this disease process from 2007–2012. Data collected included demographic information, co-morbidities, laboratory data including culture results, operative details, imaging frequency and findings, complications, and survival. Continuous variables were reported as median values and ranges.
Results:
From 2007–2010, we treated eight patients with DNM. The median age of the patients was 33 y (range 28–63 y), and 63% were male. In accordance with our algorithm, the patients underwent serial imaging at regular intervals following operative debridement. The median number of imaging studies was 11 (range 4–19). The patients required a median of five operative debridements (range 1–15). In five patients, drainage was necessary through a cervical exploration. A thoracic approach was required in six patients (two thoracoscopic, four via thoracotomy). Additional procedures included thymectomy (n=2), anterior mediastinotomy, carotid sheath exploration and resections of the clavicle, first rib, manubrium, pectoralis major muscle, and sternocleidomastoid muscle. The most common etiologic agents were Peptostreptococcus spp. and Streptococcus anginosus. Study patients received a median of six different antibiotics (range 2–10) for a total of 42 d (range 34–55 d). These patients were hospitalized for a median of 29 days (range 16–56 d), with 15 d (range 7–48 d) spent in the intensive care unit. Remarkably, the rate of survival was 100% (median follow-up of 33 mo). The patients developed no major complications, required no re-admissions, and had no re-infections.
Conclusions:
We applied an algorithmic approach to the treatment of DNM, consisting of aggressive operative debridement and enhanced by equally aggressive imaging. Our patients had excellent outcomes despite the widely known lethality of DNM. An aggressive approach may decrease complications and improve survival in this devastating disease process. Furthermore, our prospective experience with DNM suggests that this algorithm used in the present study should be the standard for managing patients with this challenging condition.
D
Such infectious processes achieve rapid spread from the neck into the thoracic cavity as a result of three cervical fascial planes that serve as a conduit into the mediastinum. The most common space in which infecting organisms in DNM enter the chest is the retrovisceral space, connecting the retropharyngeal space with the posterior mediastinum. The other two portals of entry include the viscerovascular space, which descends along the carotid sheath, and the pretracheal space, which is involved most commonly with post-operative infections following operations involving the thyroid or cervical trachea (Fig. 1). The pathogens responsible for DNM spread by direct extension into the chest, expedited by gravity as well as negative intrathoracic pressure generated by normal respiratory excursion.
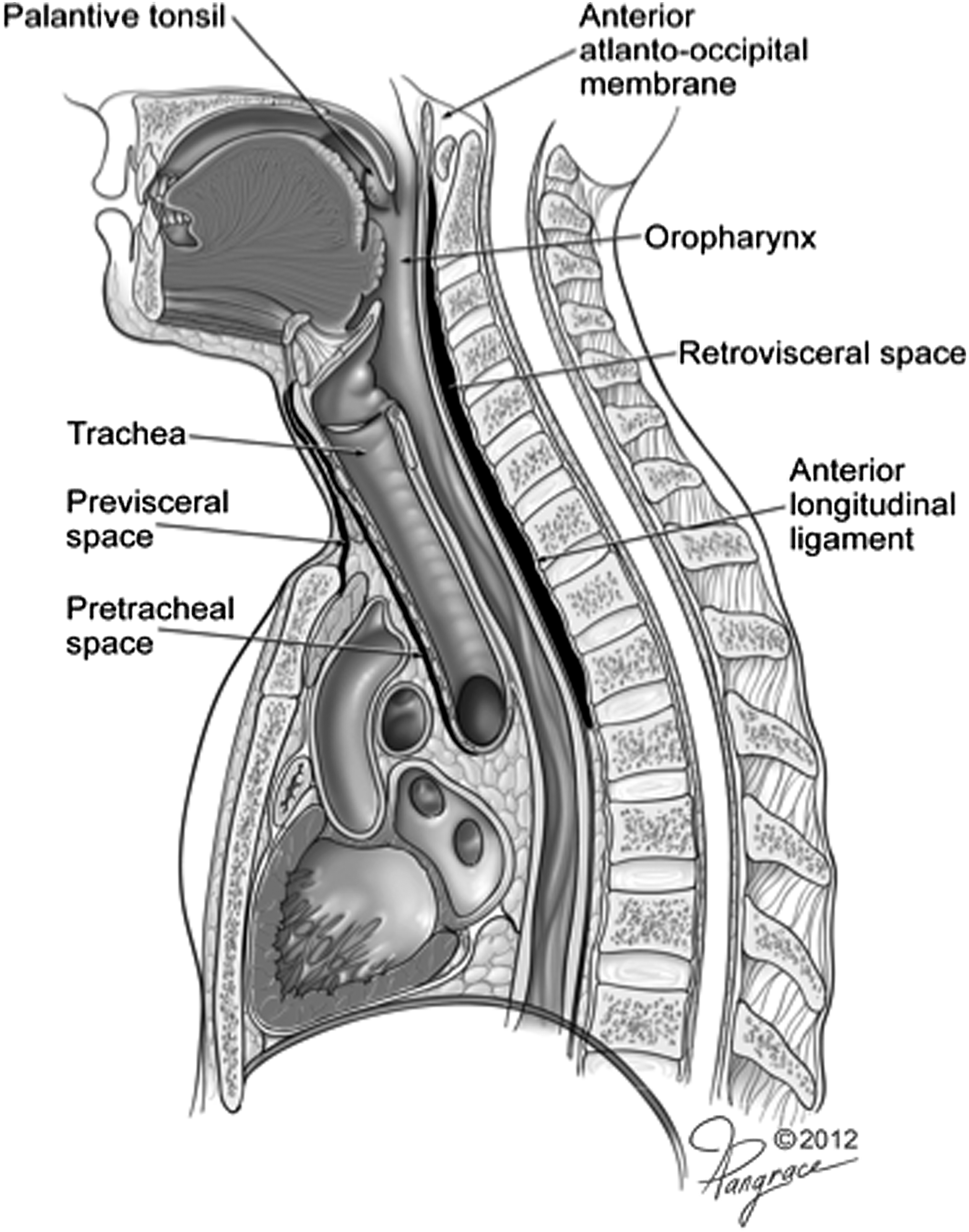
Fascial layers important in necrotizing mediastinitis. This diagram illustrates the three fascial layers—superficial, visceral and prevertebral—and the potential routes of spread from the cervical tissues into the mediastinum.
Until 10 y ago, mortality rates in DNM remained high despite the advent of novel imaging tactics and the introduction of modern tenets of critical care. Mortality rates in retrospective studies of DNM have varied between zero and 83% [1,2]. Freeman et al. first described the use of an algorithmic approach to manage DNM [1]. They advocated a wide, multi-disciplinary approach with aggressive drainage, including cervical and thoracic debridement, followed by serial cross-sectional imaging to direct future debridements. Over a period of 18 y, Freeman et al. treated 10 patients with DNM without any mortality, although they did report marked morbidities [1].
The optimal managment for patients with DNM remains controversial [2]. Our group has prospectively implemented a modified algorithm [1] for managing patients with DNM. This modified approach involves a greater multidisciplinary input and aggressively implements follow-up imaging every 24–72 h, with serial debridements based on imaging findings. Herein we present the results of our prospective application of this modified algorithm, with which there has been no mortality to date (Fig. 2).
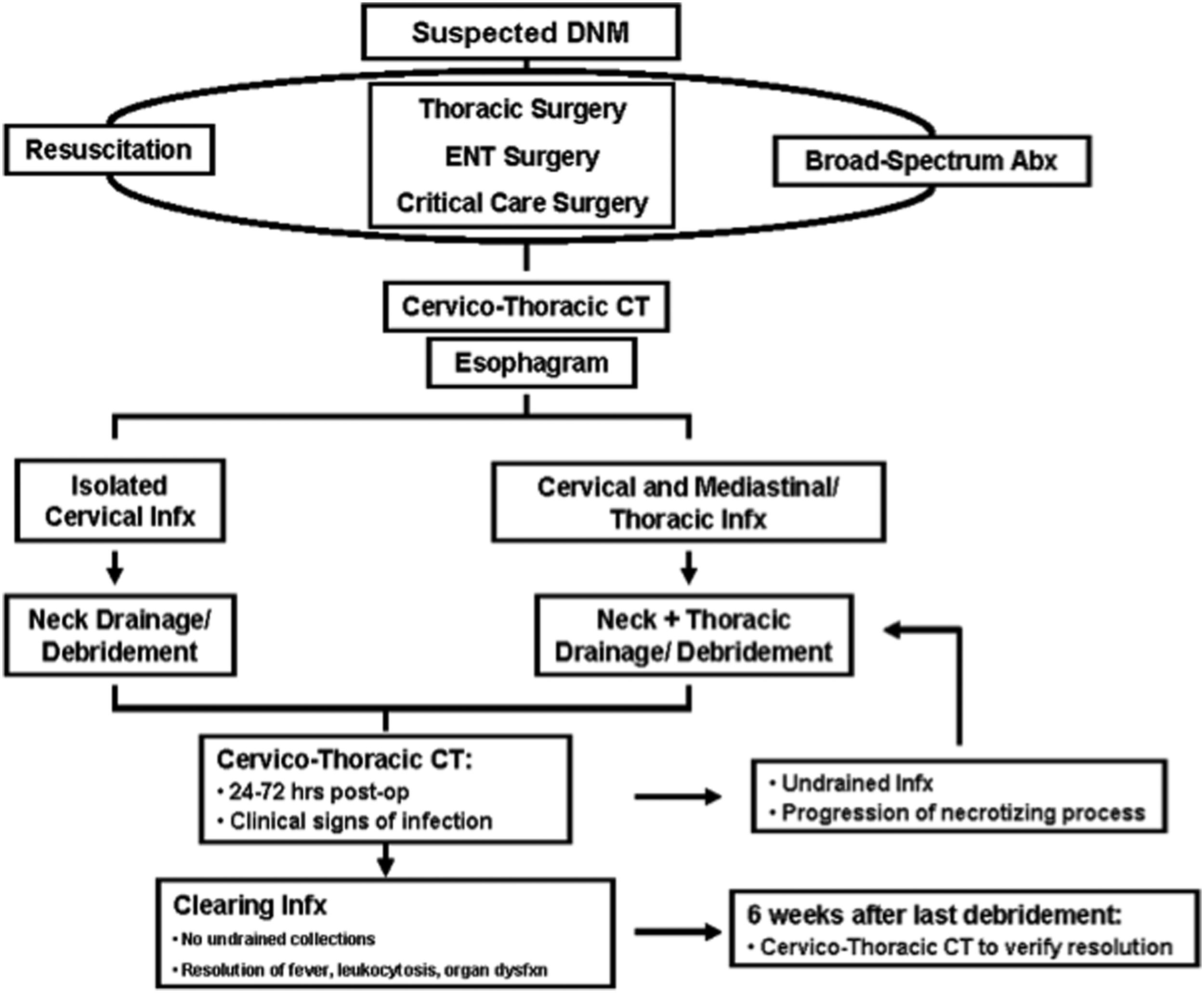
The DNM management algorithm. The key elements that define our algorithm include cervico-thoracic CT imaging at 24–72 h intervals, and return to the operating room for undrained infection or evidence of progressive disease.
Patients and Methods
Clinical management
For all patients with suspected DNM, early and appropriate resuscitation was initiated along with the introduction of broad-spectrum antibiotic therapy. Importantly, prompt consultations were obtained with surgical intensive care specialists, thoracic surgeons, and otolaryngologists. Imaging studies were obtained, including contrast studies of the esophagus, and computed tomography (CT). The patients were then taken to the operating room for cervical debridement, with or without thoracic debridement, as directed by findings on imaging. For the thoracic approach, we explored the chests of patients via thoracotomy or video-assisted thoracoscopic surgery (VATS). The mediastinal compartment was opened and debrided aggressively. Wide drainage was achieved with thoracostomy tubes.
Post-operatively, the patients were transferred to the surgical intensive care unit (SICU), where resuscitation was continued. Central venous and arterial catheters were placed, and resuscitation was directed at achieving a central venous pressure of 10–12 mm Hg with the addition of vasopressor agents to maintain a mean arterial pressure of 60 mm Hg. The patients were supported with mechanical ventilation, using properties of lung protective ventilation when appropriate. Early enteral nutrition and moderate glucose control were standard. Broad-spectrum antibiotics were initiated at the time of patients' admissions and adjusted on the basis of culture results and clinical progression. All patients were given prophylaxis against stress-related gastric incisal hemorrhage and deep venous thrombosis (DVT). Consideration was given to maintaining patients in a euvolemic state and preventing contrast-induced nephropathy, because of the frequency with which patients underwent CT imaging requiring the intravenous contrast administration. The patient management algorithm is seen in Fig. 2.
Data collection
Following approval by the appropriate institutional review board, we searched our prospectively collected clinical data base for all patients admitted with the diagnosis of mediastinitis from 2007–2012. Each patient chart was reviewed retrospectively for patient demographics, co-morbidities, Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, clinical features at admission, and initial vital signs. We captured additionally details pertaining to operative procedures, antibiotic use, laboratory tests including culture results, and imaging studies. Continuous variables are reported as medians and ranges, and categorical variables are reported as n and percent.
Results
Patient demographics
Eight patients met the inclusion criteria for the study. The median age was 33 y and 63% were male. Co-morbidities included rheumatoid arthritis in one patient (12.5%) requiring immunosuppressive therapy, and diagnoses of hypertension and hyperlipidemia in two patients (25%).
The etiologies of the patients' infections were as follows: three (37.5%) originated as pharyngitis, two (25%) began as a sternoclavicular infection, one (12.5%) originated as a peritonsillar abscess, and one (12.5%) began as a pharyngeal injury. The etiology was unknown in one patient, in whom it was presumed to be oropharyngeal.
Clinical course
On admission, the patients' median temperature was 37.3°C (range 36.9–39.6°C), and three (37.5%) patients were febrile. The patients' median heart rate was 109 beats/min (range 60–136). One patient (12.5%) was hypotensive, with a blood pressure on admission of 90/50 mm Hg (mean arterial pressure 63 mm Hg). The patients' median white blood cell count (WBC) was 12.2×103/mcL (range 8.4×103–20.4×103/mcL), and five (62.5%) patients had an elevated WBC at admission. One patient had acute kidney injury at initial presentation. The median APACHE II score for our patient population was 10 (range 5–16).
Imaging studies were performed routinely at admission. The images shown in Figure 3 represent slices from the CT scan of a typical patient with DNM. The presence of gas and fluid in the mediastinal tissues was highly suggestive of a necrotizing process.
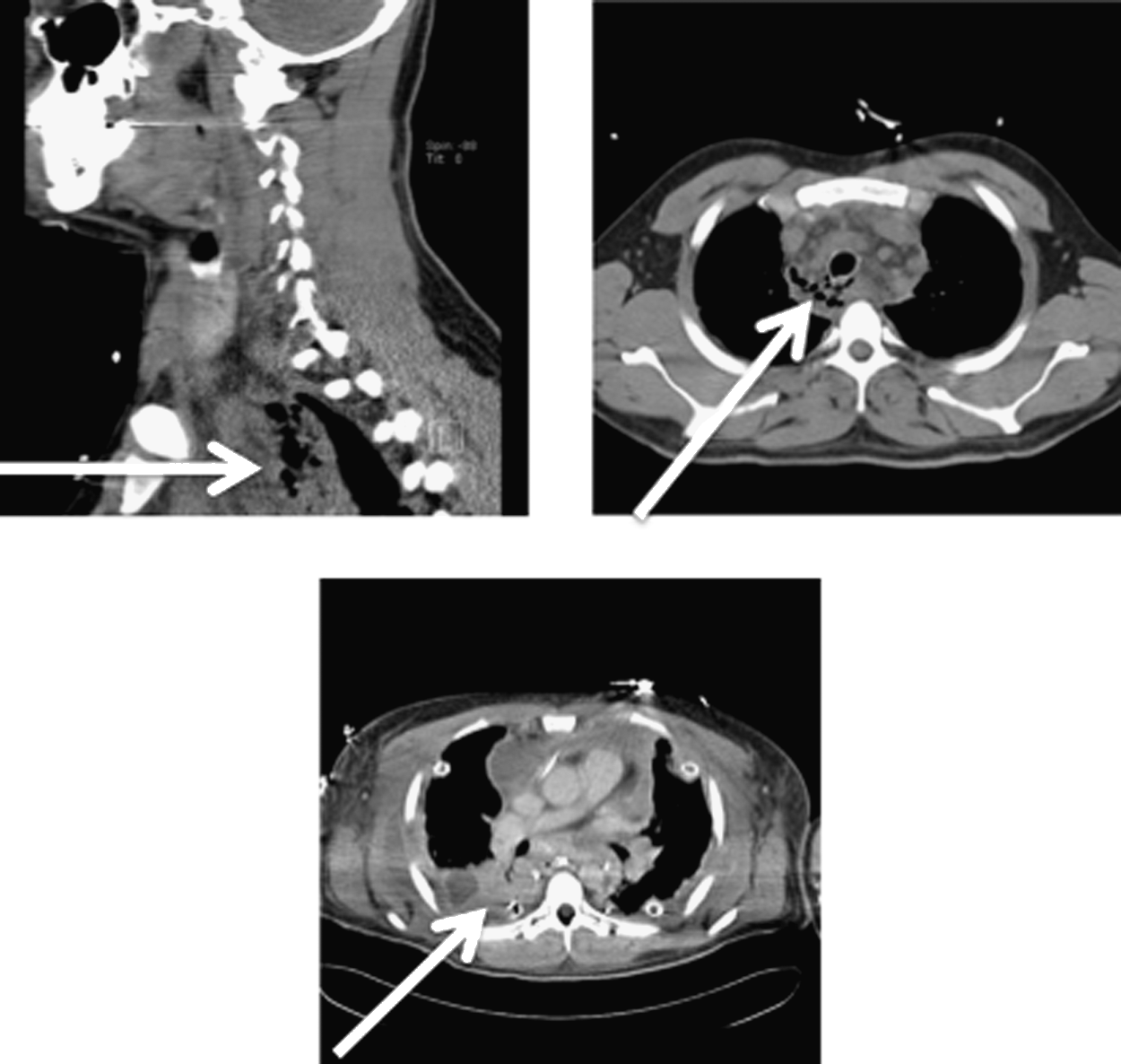
Representative computed tomography (CT) imaging leading to additional surgical drainage, revealing persistent fluid collections in the mediastinum in a 28 year-old male with DNM. Arrows demonstrate concerning areas that prompted surgical intervention.
The patients required a median of five operative debridements (range 1–15), with a median interval between operations of 3 d (range 1–10 d). In six (75%) patients, drainage was necessary through a neck exploration. A thoracic approach was required in six (75%) patients (two thoracoscopic, four via thoracotomy). Additional procedures included thymectomy; anterior mediastinotomy; and carotid sheath exploration; and resections of the clavicle, first rib, manubrium, pectoralis muscle, and sternocleidomastoid muscle (Table 1).
Because an aggressive approach to post-operative imaging is a key component of our clinical approach, the patients underwent repeat imaging every 24–72 h after operative intervention, as well as upon the appearance of any signs of clinical deterioration. The median number of imaging studies done on the patients was 11 (range 4–19). Sixty-six percent of these studies resulted in subsequent operative procedures. Figure 3 shows an example of one such study, which revealed three undrained fluid collections that prompted urgent operative intervention.
Microbiology data
Each patient was treated initially with broad-spectrum antibiotics compatible with the patient's allergies and co-morbidities. The median number of anti-infective agents given to each patient was six (range 2–10) (Table 2). The median duration of antibiotic therapy was 42 d (range 34–55 d). No patient had positive results for methicillin-resistant Staphylococcus aureus (MRSA) when tested with nasal swabbing at the time of admission to the SICU. Importantly, no patients developed complications as a result of prolonged antibiotic therapy.
The most common etiologic agents of DNM were Peptostreptococcus spp. and S. anginosis. In total, eight different bacterial species were cultured among the patients in the study (Table 3). In order of descending frequency of identification they were Streptococcus spp. (16 cultures, 75% of patients); Peptostreptococcus (nine cultures, 62.5% of patients); methicillin-sensitive S. aureus (seven cultures, 12.5% of patients); coagulase-negative staphylococcus (six cultures, 37.5% of patients); Propionibacterium species (six cultures, two patients); Prevotella (four cultures, two patients); Corynebacteria (one patient); and Fusobacterium (one patient).
Outcomes
All patients required mechanical ventilation soon after their presentation. Patients remained ventilated for a median of 11 d (range 4–47 d). The median hospital length of stay (LOS) was 29 d (range 16–56 d). The median LOS in the SICU was 15 d (range 7–48 d). Seven patients were discharged to their homes and one patient was transferred to a rehabilitation unit.
The median follow-up time in the study was 1,010 days (33 mo; range 2–49 mo). A review of the outcomes of patients showed no major complications as a result of the study protocol, no re-admissions, and no re-infections. The survival in this complex patient population was 100%.
As would be expected, the patients in the study developed a number of disease-related morbidities, including respiratory failure in three (37.5%) patients, and severe acute respiratory distress syndrome (ARDS) complicating the course of treatment of one patient, who was discharged eventually to his home with supplemental oxygen, which he was no longer using at follow-up. Atrial fibrillation and supraventricular tachycardia, occurred in one patient each (two patients; 25%) (Table 4). Minor treatment-related complications occurred in two patients. One patient had bleeding after a vacuum dressing change and underwent re-operation for ligation of a small superficial vessel. Another patient developed an erosion of a drainage catheter into the esophagus, which was managed a two non-operatively.
Discussion
Necrotizing mediastinitis was reviewed first in 1938 [3]. Since that initial report, only small series and case reports of the condition can be found in the literature [2,4–12]. Pearse's review reported an estimated incidence of DNM arising from cervical or odontogenic sources as 21.7% of all mediastinal infections [3]. In his series of 110 cases, the mortality was reduced from 87% in among non-surgically treated patients to 27% with prompt surgical drainage [3].
As late at the 1980s, the utilization of proper antibiotics and the advent of imaging with CT did little to reduce the 40% mortality rate in DNM [6]. A number of clinical approaches have been taken in efforts to improve outcomes. First, imaging has become an important method for monitoring the progression of DNM. Advances in the technology of CT have been applied to evaluate clinical deterioration and to time interventions such as debridement. Modern principles of critical care are now used for all patients with DNM. Early goal-directed resuscitation, lung-protective ventilation, enteral feeding, and moderate regulation of the blood glucose concentration have each demonstrated salutary effects on mortality.
Although DNM has been recognized as a clinical syndrome for more than 100 y, mortality in this condition remained at as high as 83% until the past decade, when Freeman et al. reported 100% survival in a series of 10 patients [1]. Commentaries in a number of published reports have highlighted underestimation of the extent of disease as a key factor in failure to achieve adequate source control in DNM. Early reports advocated localized, transcervical drainge to control sepsis [6,13]. More recent publications have advocated a more aggressive initial approach [1,9,14]. A 1997 review by Corsten et al. found significant improvement in mortality (47% to 19%, p<0.05) with an initial debridement that included a cervical and mediastinal approach [15]. More recently, several series have demonstrated improvement, with success in 85% of patients [16]. The importance of anatomic understanding in managing the disease and the operative approach to it is illustrated by our experience and that of others [17].
Delay in treatment and failure to recognize the extent of disease can be fatal rapidly for patients with DNM. Risk factors such as glucocorticoid use prior to admission, the presence of gas on the initial CT scan, and a pharyngeal focus of fasciitis have been defined recently as independent risk factors for aggressive descending infection [18]. Delayed or inadequate therapy is likely to result in a lethal outcome of DNM, as highlighted by a report published in 1985, in which a patient with the disease refused surgical intervention upon initial evaluation [19]. Three days later, the patient presented with a compromised airway and cardiorespiratory arrest, ultimately suffering fatal anoxic encephalopathy [19]. Similarly, one of our patients refused surgery initially, which delayed his initial operation for several hours. This patient was the only individual in our cohort to develop acute respiratory distress syndrome complicating his stay in the SICU. Delay of source control probably contributed to the more severe disease course experienced by this patient.
The value of early and aggressive imaging in DNM has not been recognized uniformly in the literature. This is a major point of emphasis of our work. The first 10 published reports of DNM after the advent of CT demonstrated mortality in the range of 40%, which was essentially unchanged from that in prior reports, leading some authors to conclude that advanced imaging would not be useful in improving the outcomes of patients with DNM [7]. Although serial imaging is a key component of our algorithm for managing the disease, we are in agreement that improved use of imaging will not improve outcomes independently of other measures. In our protocol, routine serial imaging allows us to follow closely the extent of disease, providing adequate information to achieve prompt, thorough source control. Thus, our approach relies upon aggressive operative debridements guided by an equally aggressive imaging strategy.
The extent of operative debridement in DNM has been debated in the literature, with variability among individual authors as well as among the different surgical specialties that care for patients with this condition. Some authors have advocated that all mediastinal infections above the carina can be managed primarily with a cervical approach, whereas descent of infection below the carina would mandate transthoracic drainage [6,13]. Failure of management with isolated transcervical drainage in DNM has been reported at 70% [9]. With the aggressive spread of disease, other authors have called for an early, multi-disciplinary approach to debridement, regardless of the presence or absence of lower mediastinal involvement. The only previous study to achieve zero mortality reported the use of an initial debridement relying upon a combined cervical/thoracic approach [1]. In this study, 59% of patients were found on imaging to have a focus of unsuspected infection, prompting more aggressive initial surgical intervention [1]. Operative management in the care of our patients was directed uniformly by the thoracic surgery service, with initial involvement of the otolaryngology service in all cases. We recommend strongly a multi-disciplinary approach for patients who present with suspected DNM, so as to optimize source control rapidly and limit disease progression. Since our submission of this manuscript, we have managed two additional patients successfully.
Our study has shown prospectively that adopting an algorithmic, multi-disciplinary approach to the management of DNM is essential in reducing morbidity and mortality in this aggressive infectious process. Key components of the algorithm include early resuscitation and airway management, emergent operative exploration and debridement, wide drainage, serial imaging to monitor disease progression, and aggressive serial debridements to achieve optimal source control. There was minimal morbidity other than that which was disease-related, and this is a crucial feature in the management of patients with DNM, in that the application of modern tenets of critical care medicine has afforded substantial progress in treatment of the disease. In conclusion, our series of patients with DNM advances knowledge in the treatment of this rare but highly lethal condition. As demonstrated by our experience, we believe that prospective implementation of our improved algorithm should be a new standard of care for patients with this challenging disease. We strongly believe that this will allow a closer approach to achieving zero mortality in its treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.