
Abstract

To the Editor:
Meningitis is an uncommon complication in neurosurgery, regardless of the frequency of dural tears, with an average infection rate of 0.40% (0.28% after craniotomy and 1.2% after ventriculostomy or ventriculoperitoneal shunt insertion), but the overall mortality rate is as high as 34% [1]. Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, Klebsiella spp., and Enterococcus faecalis are the pathogens isolated most frequently from meningitis after neurosurgery [2]. However, to the best of our knowledge, Acinetobacter baumannii meningitis has not been reported in the English-language literature as a secondary event in neurosurgery performed via an endoscopic transnasal approach. We describe A. baumannii meningitis after trans-sphenoidal pituitary tumor excision.
A 45-year-old female presented to our emergency department with fever, chills, severe headache, and vomiting for 1 d. She had undergone trans-sphenoidal pituitary tumor excision 3 weeks prior to her visit to our department. She was mentally clear initially, but her level of consciousness decreased within a few hours. Physical examination showed neck stiffness with meningismus. A complete blood count revealed mild leukocytosis (10,970 cells/mm3) with a left shift (neutrophils 87.8%). The neuro-imaging studies disclosed no evidence of an intracranial lesion (Fig. 1). Analysis of cerebrospinal fluid (CSF) showed mild opening pressure elevation (200 mm H2O) and white, turbid fluid with pleocytosis and neutrophil predominance (white blood cell count 25,620 cells/mm3, neutrophils 99%), elevated protein (741 mg/dL), and a low glucose concentration (<2 mg/dL). Thus, bacterial meningoencephalitis was diagnosed, and empiric ceftriaxone and vancomycin were prescribed immediately. Transnasal endoscopic inspection of the surgical site revealed no evidence of CSF leakage. Three days later, the microorganism isolated from the CSF culture was identified as A. baumannii, and antibiotics were switched to imipenem-cilastatin according to the susceptibility results. The patient recovered without obvious sequelae after 14 d of antibiotic treatment.
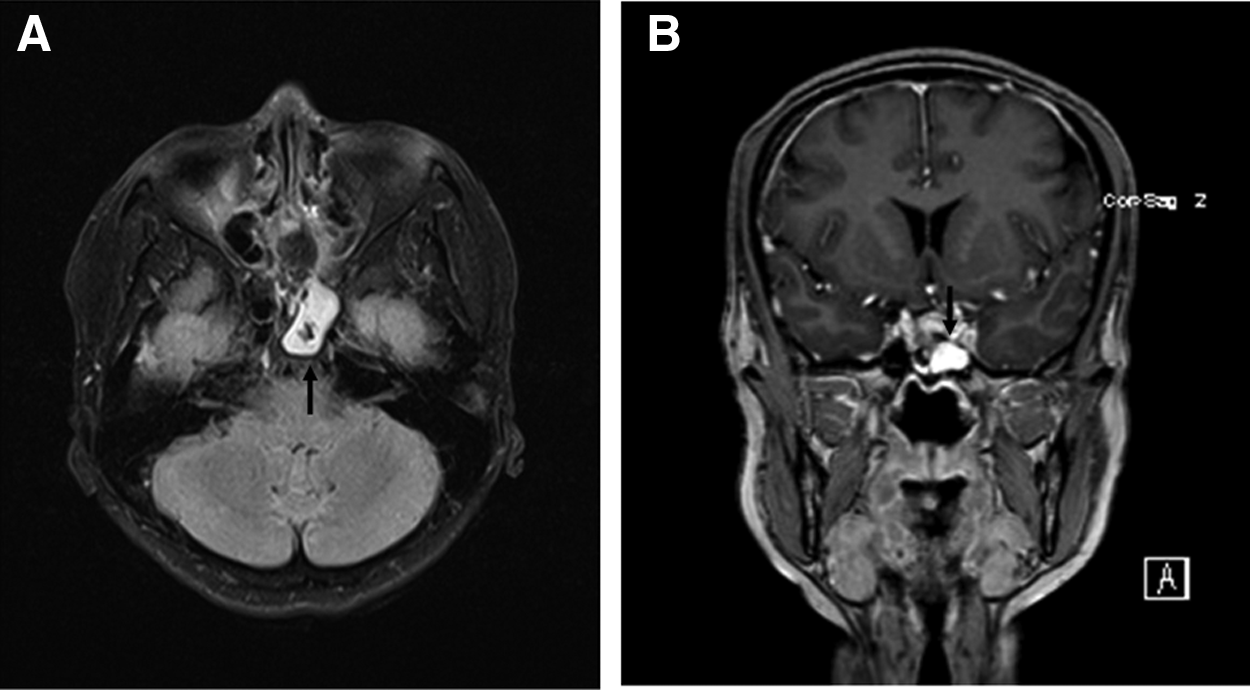
Postoperative brain magnetic resonance images with gadolinium enhancement. (
Bacterial meningitis is a medical and neurologic emergency that requires immediate and timely treatment. Immediate antibiotic therapy is paramount, but recommendations for antimicrobial therapy change over time as a result of antimicrobial resistance. Nosocomial bacterial meningitis may result from invasive procedures (e.g., craniotomy, placement of a ventricular catheter, lumbar puncture, intrathecal infusion of medication, or spinal anesthesia), complicated traumatic brain injury, or metastatic infection in patients with hospital-acquired bacteremia. The causative microorganisms have a different spectrum than is characteristic in cases acquired in the community setting. Therefore, the treatment regimen should be broad in spectrum and cover multi-drug-resistant pathogens.
Acinetobacter baumannii is a non-motile, non-fermentative, aerobic, gram-negative coccobacillus that can persist for a long period in various environments. It is part of the normal flora of the human skin and can be isolated from the rectum, nose, and thorax. This pathogen is characterized by its great resistance to the environment, enabling it to spread rapidly and develop resistance to conventional antimicrobial agents. Infections caused by A. baumannii were uncommon before the 1970s, but have been increasing since then, in recent years accounting for 1%–3% of all nosocomial infections, including bacteremia, pneumonia, urinary tract infection, and surgical site infection [2]. However, meningitis caused by Acinetobacter spp. is still rare. To date, only seven cases of community-acquired Acinetobacter meningitis in adults have been reported in the English-language literature [3]. The causative organisms were most likely Acinetobacter lwoffii, Acinetobacter johnsonii, and Acinetobacter junii [4]. Furthermore, surgery-related Acinetobacter meningitis is responsible for fewer than 5% of meningitis cases associated with craniotomies, ventriculostomy tubes, and traumatic brain injuries and has a high mortality rate: 25%–34% [1,2,5,6].
Fever and progressive consciousness disturbance were the most common clinical manifestations, as they are in patients with bacterial meningitis caused by other pathogens. Guidelines for treatment of post-neurosurgical meningitis from the Infectious Diseases Society of America recommend either ceftazidime or cefepime [3]. Nevertheless, pharmacodynamic assessment of these antimicrobial agents in CSF suggests the recommended dose will target fewer than 10% of contemporary Acinetobacter isolates [3]. Carbapenems are the mainstay of treatment nowadays in susceptible isolates. Treatment with imipenem-cilastatin led to recovery of 11 of 13 patients (84.6%) [3]. Meanwhile, colistin, a polymyxin abandoned previously because of nephrotoxicity, was reported to retain good in vitro activity and in many cases represents the only therapeutic option in multi-drug-resistant Acinetobacter meningitis. Its role in therapy is limited by its poor CSF penetration, but in an isolated meningitis case, where it was used intraventricularly and intrathecally, a greater than 90% cure rate was observed [7]. Unlike the strains found in nosocomial infections, the strain of Acinetobacter in community-acquired meningitis rarely shows a multiple antibiotic resistance phenotype.
According to the review of Siegman-Igra et al., the median time to the development of Acinetobacter meningitis after a neurosurgical procedure is 12 d (range 1–40 d) [8]. Based on our patient's clinical history and the fact that further transnasal endoscopic inspection showed no obvious skull base lesion, the route of A. baumannii infection was considered to be via surgery, as the organism may have been inoculated into the sphenoid sinus at the time of surgery. Even though meningitis is a well-known complication of neurosurgery and any pathogen can be responsible, the disease is rarely caused by A. baumannii, and such a case has never been reported as a complication of trans-sphenoidal pituitary tumor excision. Because of its high mortality rate, early diagnosis and prompt use of appropriate antibiotics according to epidemiologic trends and in vitro susceptibility testing are essential to maximize the potential for survival.