
Abstract
Abstract
Background:
Postoperative peritonitis (PP) is associated with a high rate of multi-drug-resistant micro-organisms. The role of Pseudomonas aeruginosa in this condition has never been assessed. We evaluated the risk factors and prognosis for PP caused by P. aeruginosa.
Methods:
Patients hospitalized in the intensive care unit (ICU) after re-operation for PP were identified prospectively. Analyses were performed retrospectively. Specific risk factors were investigated by comparing P. aeruginosa PP with PP having other causes. The main outcome endpoint was death in the hospital.
Results:
We found 55 P. aeruginosa PP among the 349 cases of PP (16%) in the ICU over 14 years. Factors associated with the presence of P. aeruginosa in peritoneal fluid culture were Acute Physiology and Chronic Health Evaluation (APACHE) II score (odds ratio [OR] 1.1; 95% confidence interval [CI] 1.02–1.09; p=0.004) and respiratory failure (OR 2.3; 95% CI 1.26–4.16; p=0.006). These criteria performed poorly in predicting P. aeruginosa PP. Such infections were associated with a higher hospital mortality rate, but not after adjustment for the severity score. Adequate antibiotic therapy comprising two antibiotics effective against P. aeruginosa was associated with a lower mortality rate for P. aeruginosa PP in the ICU.
Conclusion:
The prevalence of P. aeruginosa PP is not high. Risk factors do not allow accurate prediction of the infection. Our data suggest two drugs effective against P. aeruginosa should be considered for treating these infections.
Previous investigators have reported that Pseudomonas spp. represent between 10% and 13% of total isolates retrieved in culture of PP [4,5]. The recent papers by Seguin et al. and Riché et al. reported that Pseudomonas aeruginosa was isolated in 7%–17% of cases of PP [6,7].
Pseudomonas species raise specific concerns in other settings, as they are associated with a particularly poor prognosis in ventilator-associated pneumonia (VAP) or blood stream infections [8,9]. Pseudomonas infections are difficult to treat and are associated with high rates of relapse. It has been recommended that P. aeruginosa pneumonia and blood stream infections be treated with long-term combination anti-microbial therapy to increase the treatment success rate and improve the patient's prognosis [9–12]. However, the specific morbidity associated with P. aeruginosa PP has not been evaluated, and the need to target P. aeruginosa specifically in PP has not been investigated. Therefore, no specific guidelines addressing the impact and significance of P. aeruginosa in PP and the optimal anti-microbial management have been established. These considerations justify a study focusing on PP caused by P. aeruginosa. Identification of risk factors and clinical characteristics of P. aeruginosa PP could allow optimization of global management, especially regarding EA.
The primary objective of this study, designed to evaluate the role of this bacterial species in intra-abdominal infections, was to assess factors associated with the presence of P. aeruginosa in culture of PP and its specific prognosis. Secondary objectives were to assess the time course of the prevalence of PP involving P. aeruginosa over a period of several years, and, in the specific subpopulation of P. aeruginosa PP, to identify factors associated with better outcomes, especially the hypothetical benefit of dual drug therapy compared with monotherapy.
Patients and Methods
Study population
From January 1994 through December 2007, all adult patients with PP requiring admission to a surgical intensive care unit (ICU) were included prospectively in a database, and their medical charts were reviewed retrospectively. Postoperative peritonitis was defined as peritoneal infection after abdominal surgery, confirmed by macroscopic findings and peritoneal fluid culture on re-operation yielding at least one colony. Post-operative peritonitis involving P. aeruginosa was identified by isolation of at least one P. aeruginosa colony from peritoneal fluid culture. Patients with PP and pure fungal infection were excluded. In accordance with French law, because this observational study did not modify the physicians' laboratory or clinical practices, the patients or relatives were simply informed about this study; informed consent was not required. The Paris North Hospitals, Paris 7 University, AP-HP Institutional Review Board (IRB), reviewed and approved the study.
Protocol management
Patients underwent abdominal surgery in our hospital or another institution and, if necessary, were transferred for management of postoperative infection. They received prophylactic or curative antibiotic therapy in the presence of abdominal infection according to the institution's protocols. All patients had been admitted to the ICU because of organ dysfunction, and all had received standard intensive care management.
Susceptibility testing and empirical anti-microbial therapy
Peritoneal fluid samples were collected systematically during re-operation and sent immediately to the bacteriology laboratory. Gram staining and cultures were performed with identification and susceptibility testing for gram-positive and -negative bacteria. Antibiotic susceptibility was determined by the disk diffusion method, according to the criteria of the Antibiotic Susceptibility Testing Committee of the Société Française de Microbiologie [13]. In vitro susceptibility to various antibiotics was recorded for all bacteria, with a focus on beta-lactams (piperacillin-tazobactam [pip/taz], imipenem-cilastatin, ceftazidime), fluoroquinolones, and aminoglycosides effective against P. aeruginosa. Results were expressed as proportions of strains of P. aeruginosa susceptible to each antibiotic. Parenteral EA was started at the time of re-operation according to the recommendations of our institutional protocol. This protocol is based on a broad-spectrum beta-lactam antibiotic pip/taz or imipenem-cilastatin. Imipenem-cilastatin is selected for patients with severe peritonitis or previous antimicrobial therapy. The use of amikacin for broadening of spectrum and synergistic combination is optional [3].
Risk factors and morbidity associated with P. aeruginosa post-operative peritonitis
Patients with PP involving P. aeruginosa (P. aeruginosa PP) were compared with patients with PP caused by other bacteria (other PP) to determine risk factors for P. aeruginosa PP. Only the first episode of PP was considered for analysis. For comparison, the following information on each patient was collected after admission to the ICU: Age; gender, severity of the underlying medical condition (stratified, according to the criteria of McCabe and Jackson, as “rapidly fatal,” “ultimately fatal,” or “not fatal”) [14]; immune status [15]; previous reoperation; characteristics of initial operation. Its type, route, and incision class [16]; use of interval antbiotic therapy (IA) and broad-spectrum IA; Acute Physiology And Chronic Health Evaluation (APACHE II) score [15]; organ dysfunction as defined by Knaus et al. [17]; time to re-operation; presence of bacteremia; identification of pathogens in peritoneal fluid; and results of anti-microbial susceptibility tests.
Definitions
Interval antibiotics were defined as any antibiotic prescribed between initial surgery and re-operation for PP [3]. Broad-spectrum IA was defined as IA including at least one of the following antibiotics: pip/taz, imipenem-cilastatin, or a fluoroquinolone. Empiric antibiotic therapy for PP was prescribed at re-operation while waiting for the results of culture and antibiotic susceptibility testing [3], and was considered adequate when, according to susceptibility testing, all bacteria isolated were susceptible to at least one of the drugs administered [3]. In a specific analysis focusing on management of P. aeruginosa PP, two definitions of adequate EA were used. Adequate EA therapy was defined initially as any antibiotic therapy targeting P. aeruginosa PP, but subsequently considered to be adequate only when combination therapy comprising administration of a beta-lactam plus an aminoglycoside or a fluoroquinolone was prescribed for P. aeruginosa PP [11].
Multi-drug-resistant (MDR) bacteria were defined as MRSA, coagulase-negative staphylococci, beta-lactam-resistant enterococci, or Enterobacteriaceae producing extended-spectrum beta-lactamase or cephalosporinase [3]. Pseudomonas aeruginosa was defined as MDR in the presence of resistance to at least two of the following groups of antibiotics: beta-lactams (except carbapenems), aminoglycosides, carbapenems, or fluoroquinolones.
Outcome
Patient outcome was recorded as the number of re-operations following admission to the ICU, duration of mechanical ventilation, ICU length of stay (LOS) for survivors, and ICU and in-hospital death. The prognosis was assessed by taking into account the presence or absence of P. aeruginosa, adequacy of EA as defined above, and, finally, in the subpopulation of P. aeruginosa PP, the number of antibiotics active against P. aeruginosa in EA and definitive antibiotic therapy. Kaplan-Meier curves were used to compare mortality rates over time in the ICU in the two groups.
Statistical analysis
Results are expressed as mean±standard deviation (SD) and as percentages for categorical variables. All analyses were performed using the Statview software package (version 5.0; SAS Institute, Inc., Cary, NC) and MedCalc software (version 7.3.0.1, Mariakerke, Belgium). Univariable analysis was performed using the Student t-test or the Mann-Whitney u-test, as appropriate for continuous variables, and the χ2 or Fisher exact test for categorical variables. All variables with a p value<0.10 by univariable analysis of factors associated with the presence of P. aeruginosa PP and of in-hospital death were entered in a multivariable logistic regression analysis. Odds ratio (ORs) and 95% confidence intervals (CIs) were calculated. Statistical significance was defined as p<0.05.
Results
During the study period, 349 patients with PP were admitted to the ICU. One hundred thirty-one patients (38%) died in the ICU, and 145 patients (42%) died in the hospital. For 55 (16%) of the 349 patients, peritoneal fluid culture yielded one P. aeruginosa strain. Epidemiologic, clinical, and microbiologic characteristics and outcomes of patients with P. aeruginosa PP and other PP are reported in Table 1. The P. aeruginosa PP rate remained stable over the years, with no outbreaks (Fig. 1). The susceptibility rates of the 55 P. aeruginosa strains were 82% for pip/taz, 89% for imipenem-cilastatin, 89% for ceftazidime, 73% for ciprofloxacin, and 89% for amikacin.
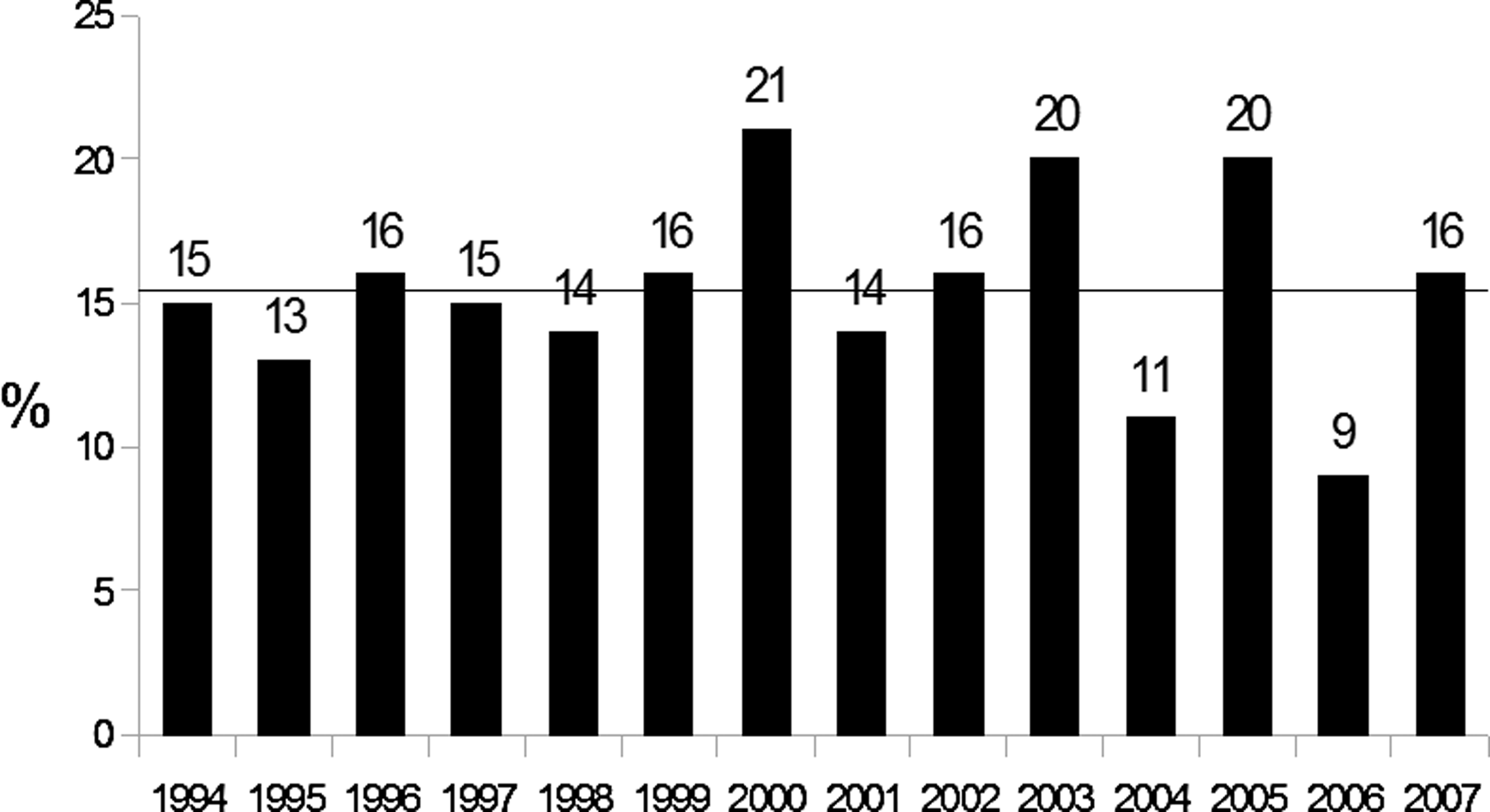
Time course of Pseudomonas aeruginosa post-operative peritonitis rates with trend line demonstrating stable prevalence.
APACHE=Acute Physiology and Chronic Health Evaluation; ICU=intensive care unit; IS=initial surgery; LOS=length of stay; OSF=organ system failure; SAPS=Simplified Acute Physiology Score; SD=standard deviation; PP=post-operative peritonitis; WBCs=white blood cells.
Favorable outcome=discharge from ICU without further re-operation.
Multi-drug-resistant P. aeruginosa was found in eight cases (15%). Micro-organisms also found in cultures of the 55 cases of P. aeruginosa PP compared with those found in other cases of PP are shown in Table 2. Multi-resistant bacteria were isolated in 27 of the 55 cases (49%) of P. aeruginosa PP (Table 2): Escherichia coli in seven cases; Enterobacter aerogenes in two; E. cloacae in one; Klebsiella pneumoniae in one; Enterococcus faecium in nine; coagulase-negative staphylococci in seven; and MRSA in four. Only two of the 13 cases of bacteremia observed in the P. aeruginosa PP group were related to P. aeruginosa strains.
Risk factors for P. aeruginosa PP
Factors associated with P. aeruginosa PP according to univariable analysis (p≤0.1) were a higher APACHE II score, respiratory dysfunction, previous re-operation, and prescription of broad-spectrum IA (see Table 1). These variables were entered in multi-variable logistic regression analysis, and only two variables were associated with Pseudomonas aeruginosa PP: APACHE II score (OR 1.1; 95% CI 1.02–1.09; p=0.004) and respiratory dysfunction (OR 2.3; 95% CO 1.26–4.16; p=0.006). A previous re-operation was not associated with P. aeruginosa PP on multi-variable analysis (OR 1.72; 95% CI 0.92–3.2; p=0.09). The percentages of P. aeruginosa PP according to the presence or absence of respiratory dysfunction or APACHE II score≥22 points are shown in Figure 2A. The optimal cutoff point provided by the receiver operating characteristic curve was obtained for an APACHE II score of 22 (Fig. 2B).
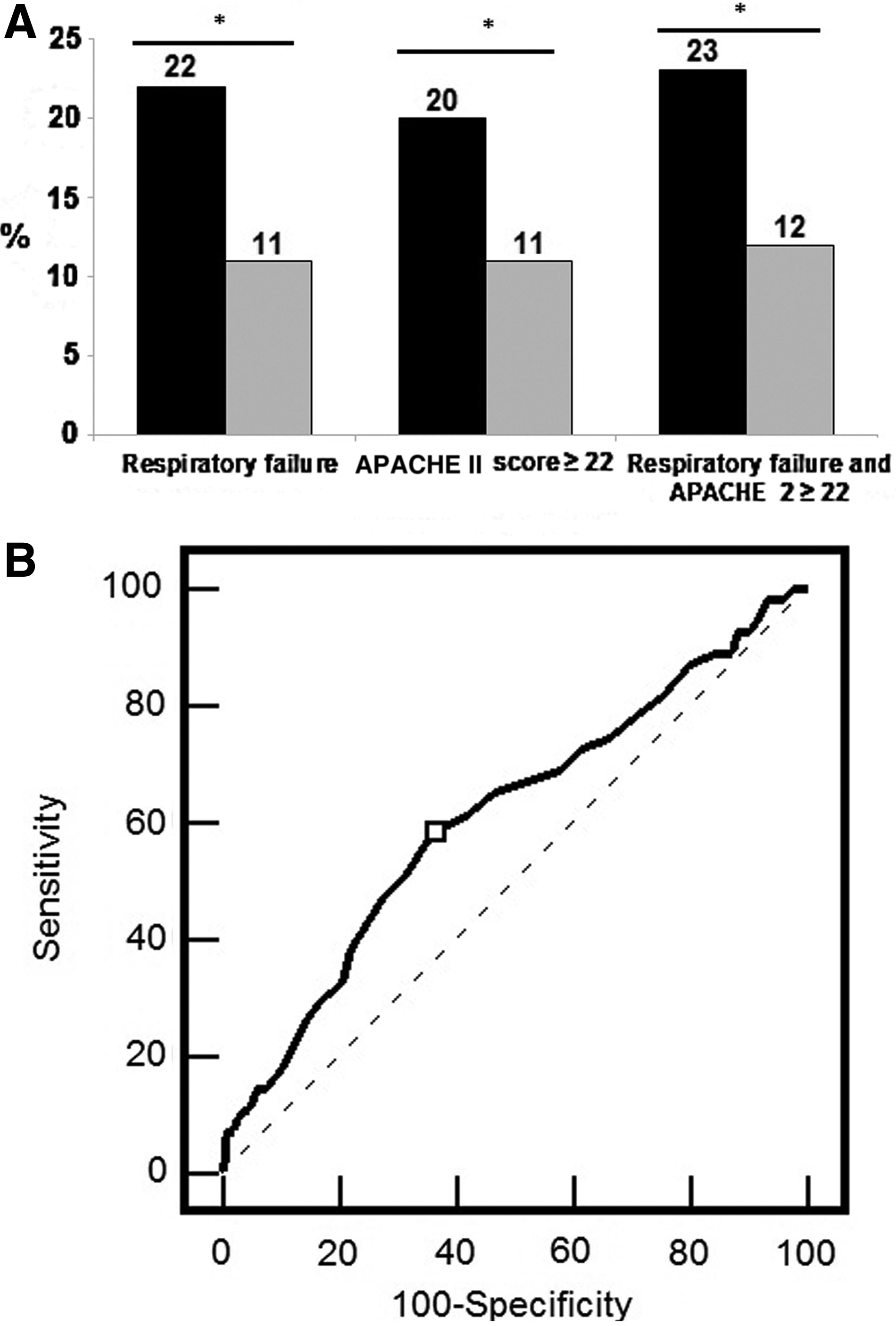
Disease severity measures. (
Risk factors for death in the 349 patients with PP and outcome of P. aeruginosa post-operative peritonitis
Outcome of Patients with P. aeruginosa post-operative peritonitis
Peritonitis was associated with a higher hospital mortality rate according to univariable analysis (56% vs. 39%; p=0.012; see Table 1). This higher rate was seen mainly during the first few days in the ICU, as assessed by Kaplan-Meier curves (Fig. 3). Apart from in-hospital death, no outcome difference was observed between patients with P. aeruginosa PP and other patients (Table 1).
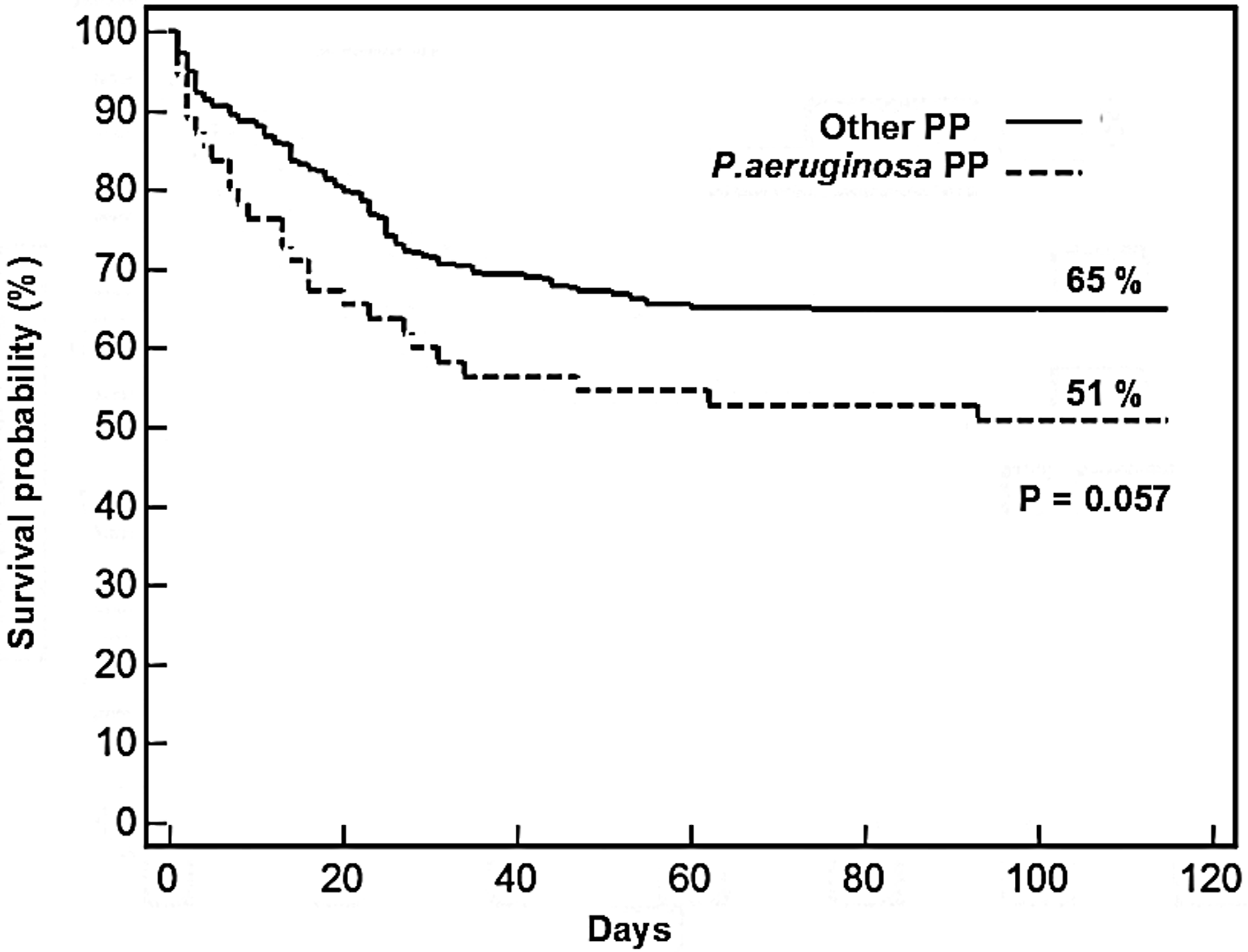
Kaplan-Meier curves for time to death in intensive care unit.
Factors Associated with Death in the 349 Patients with post-operative peritonitis
According to univariable analysis, factors associated with in-hospital death were the presence of P. aeruginosa in cultures, an immunocompromised state, an underlying fatal disease, a higher APACHE II score, inappropriate EA, emergency re-operation, and more advanced age (Table 3). Multivariable analysis found that higher APACHE II score (optimal cutoff 21; OR 1.18; 95% CI 1.12–1.22; p<0.001), greater age (optimal cut off 63 years; OR 1.03; 95% CI 1.01–1.04; p=0.007), initial emergency surgery (OR 2.12; 95% CI 1.33–4.00; p=0.003), hemodynamic dysfunction (OR 2.37; 95% CI 1.42–4.06; p=0.001), and acute renal dysfunction (OR 2.37, 95% CI 1.8–5.4; p<0.0001). Interestingly, the presence of P. aeruginosa and respiratory dysfunction was not associated with a higher hospital mortality rate on multi-variable analysis.
APACHE=Acute Physiology and Chronic Health Evaluation; ICU=intensive care unit; IS=initial surgery; LOS=length of stay; OSF=organ system failure; SD=standard deviation; SAPS=Simplified Acute Physiology Score; WBC=white blood cells.
Outcome of the 55 patients with P. aeruginosa post-operative peritonitis
The specific outcome of P. aeruginosa PP according to the definition of adequacy of EA was evaluated. When adequate EA was defined only by coverage of all bacteria by at least one antibiotic effective according to antibiotic susceptibility testing, the ICU and in-hospital mortality rate and re-operation rate were not different in patients with adequate EA and those with inadequate EA. When adequate EA required the presence of two effective antibiotics against P. aeruginosa, factors associated with death in the ICU on univariable analysis were adequate EA (p=0.08), higher APACHE II score (p=0.004), hemodynamic dysfunction (p=0.06), and renal dysfunction (p=0.04). On multi-variable analysis, inadequate EA (OR 5.25; 95% CI 1.09–25.2; p=0.04) and higher APACHE II score (OR 1.13, 95% CI 1.04–1.23; p=0.006) were associated with death in the ICU.
Discussion
In this retrospective study, the prevalence of P. aeruginosa PP was 16%, which is consistent with the limited published data [6,7], and, interestingly, remained stable over the years. The IDSA guidelines recommend targeting P. aeruginosa for EA prescription but do not provide further information about the specific management of P. aeruginosa PP [2]. The data of the present study suggest that P. aeruginosa PP is associated with higher APACHE II scores and respiratory dysfunction. Nevertheless, these markers are not reliable enough to predict the presence of P. aeruginosa in peritoneal fluid culture accurately. The spectrum of antibiotic regimens proposed by the IDSA guidelines for anti-microbial management of healthcare-associated intra-abdominal infection usually covers susceptible P. aeruginosa [2]. In our population, P. aeruginosa strains demonstrated high rates of susceptibility to anti-pseudomonal antibiotics. This profile of strains cultured from nosocomial infection is in accordance with a prospective multicenter French study based on 97 cases of PP and with other studies [4,18].
As in other infectious settings, P. aeruginosa PP is associated with a higher mortality rate than other forms of PP. This higher rate is observed during the first few days of hospitalization (Fig. 3) and is related to more severe peritonitis. However, when adjusted for severity of illness score, the mortality rates of P. aeruginosa PP and other forms of PP were not significantly different. The higher hospital mortality rate cannot be attributed directly to P. aeruginosa, but rather to the more severe illness. More severely ill patients may have undergone more re-operations and IA predisposing to colonization by P. aeruginosa. These results must therefore be interpreted cautiously.
It is unclear whether P. aeruginosa is a pathogen responsible for more severe disease, or whether it only colonizes the site of infection as a marker of disease severity. The low rate of monomicrobial P. aeruginosa PP could be an argument in favor of the second hypothesis, but if P. aeruginosa were only a marker of disease severity, markers of severity associated with death in the 349 cases of PP would also have been expected to be associated with the presence of P. aeruginosa. Interestingly, cultures of fluid taken from P. aeruginosa PP found fewer Enterobacteriaceae than other PP (see Table 2). Furthermore, despite the high rate of hemodynamic dysfunction, P. aeruginosa PP was associated with a low rate of P. aeruginosa bacteremia. On the contrary, P. aeruginosa PP was associated with bacteremia caused by other microorganisms. These points may be an indication that patients with and without P. aeruginosa have some different specificities, and that severity of disease could be unrelated to the presence of P. aeruginosa. The discrepancy between the fact that hemodynamic and renal dysfunction was associated with in-hospital death but not with the presence of P. aeruginosa, and the fact that respiratory dysfunction was associated with P. aeruginosa, but not with in-hospital death, suggest that respiratory dysfunction has a specific significance in P. aeruginosa PP. However, the definition of respiratory dysfunction [17] includes many etiologies such as rapidly reversible causes such as atelectasis, often observed in peritonitis (e.g., pneumonia, sepsis-induced acute lung injury, atelectasis), which could explain the lack of association between outcome and respiratory dysfunction.
The need for combination antibiotic therapy against P. aeruginosa has been the subject of debate for many years. Several papers on Pseudomonas VAP suggest a benefit of combination therapy compared with monotherapy. In a meta-analysis based on 50 studies comparing monotherapy and combination therapy, Kumar et al. observed a lower mortality rate in septic shock or critically ill patients who received combination therapy [19]. The potential benefit of EA comprising two antibiotics effective against P. aeruginosa strains that was observed in our study is consistent with this result. In view of the relatively small sample size, this result needs to be validated by further studies. The prescription of EA comprising two antibiotics effective against P. aeruginosa should be considered in case of PP. Application of current guidelines may be not sufficient to achieve appropriate coverage of P. aeruginosa PP.
This was a single-center, retrospective study. Microbiologic features could be different in other institutions. The antibiotic resistance profile must be monitored in each institution. These results should therefore be considered with caution. Furthermore, as in most other clinical studies on this subject [20,21], the specific role of P. aeruginosa in the physiopathology of PP was not studied; only the clinical specificities of PP in which P. aeruginosa was isolated were investigated. The low prevalence of P. aeruginosa PP and the absence of any outbreak during 13 years imply that P. aeruginosa is a minor pathogen in this setting. We did not address the interesting potential synergistic effect of coinfection by P. aeruginosa and Candida albicans that has been studied in the context of pneumonia [22,23]. This issue could be the subject of further investigations. Finally, it must be kept in mind that, as in all surgical infections, the first step and the key point of management is surgery. Consequently, it may be difficult to demonstrate differential efficacy of various antibiotic regimens in this setting. This study points out issues that should be investigated in further studies.
In conclusion, P. aeruginosa was isolated in 16% of cases of PP and was associated with high mortality rates in the early course of the disease because of the more severe peritonitis. P. aeruginosa was isolated more frequently from peritoneal fluid culture in the presence of respiratory dysfunction, but this criterion is not sufficiently specific to be used in clinical practice. Even if the results should be interpreted with caution, this study suggests that optimal antimicrobial therapy for P. aeruginosa PP requires two effective antibiotics. Application of current guidelines may not be sufficient to achieve optimal management of P. aeruginosa PP.
Author Disclosure Statement
No conflicting financial interests exist.