
Abstract
Abstract
Background:
Registration of complications of treatment is an important instrument for measuring the quality of health care. Reliable registration depends on definitions, the case-finding method that is used, and the registration method itself. We conducted a comparative study of two different methods of registration for the surveillance of surgical site infections (SSIs) in a single hospital.
Methods:
The study included all patients in both the surgical database and the microbiology and infection-prevention database of the hospital who underwent surgery on the abdominal aorta or peripheral vascular procedures from March 1, 2009 to March 1, 2010. The surgical database included positive scores for SSI in cases of positive wound swabs, the need for incision drainage, or the need for antibiotic treatment. The microbiology and infection-prevention database used criteria from the U.S. Centers for Disease Control and Prevention (CDC), and based positive scores on redness, heat, swelling, or pain in the area of a surgical incision within 30 d after a procedure, and on a positive swab, drainage from an incision, or the presence of pus following a diagnostic puncture.
Results:
The surgical complication database included 218 patients, of whom 20 (9.2%) had a SSI. The microbiology and infection-prevention database included 236 patients, of whom 33 (14%) had a SSI. The databases were merged and all infections were ascertained by an expert team. The surgical database had a sensitivity of 57% for SSIs, whereas the microbiology and infection-prevention database had a sensitivity of 93% (p<0.05).
Conclusion:
Physicians provided less reliable scores for SSI than did trained infection-control practitioners. This raises questions about the comparability of rates of SSI in different institutions as a means for judging the quality of hospital care.
Patients and Methods
All patients who underwent elective or urgent vascular surgery, either aortic surgery or surgery on a lower limb, between March 1, 2009 and March 1, 2010 were included in both the surgical and the microbiology and infection-prevention databases. The surgeon or resident was responsible for registration of the patient in the surgical database. Surgical site infection was scored in cases in which there were clinical manifestations of infection (areas of redness, heat, swelling, or pain around the incision), in cases of the need for wound drainage, or when antibiotics were needed. Complications in patients undergoing vascular surgery were registered on a new form, on which different types of complications could be scored prospectively. All patients admitted to the hospital for vascular surgery were included in this registration. Surgical site infections were registered for both the patient's period of hospitalization and in the outpatient clinic, according to the setting in which they occurred, and were documented in the patient's file and later entered in an electronic database (Microsoft Access; Microsoft, Redmond, WA).
The database in the department of microbiology and infection prevention scored SSIs according to the criteria established by the U.S. Centers for Disease Control and Prevention [6]. The main criteria among these are the presence of redness, heat, swelling, or pain around a surgical incision within 30 d after an initial procedure, and the presence of a positive culture, incision drainage, or pus after a diagnostic puncture. The inclusion of patients in the study was based on the planning list of the hospital's operating theater, and the patients in the study were followed prospectively for the development of an SSI. The patients' medical records were searched for the presence of the criteria named above. Post-discharge surveillance was continued until 30 d after each patient's surgical procedure. The microbiology and infection-prevention department documented complications in a database compiled with SPSS software (SPSS, Chicago, IL). Patients who met the inclusion criteria for the study were selected from both the surgical and the microbiology and infection-prevention data bases on the basis of the codes for the types of their surgeries and date of operation.
The patients were matched and their data were merged into a single aggregated database. All patients with a discordant score in the two databases were reviewed by an expert team consisting of a surgeon and medical microbiologist who had not been involved in the initial assessment. They used the CDC criteria named above for defining SSI.
Statistical analysis of the study data was done with SPSS version 19.0. The Fisher exact test was used to calculate statistical significance. A value of p<0.05 was considered statistically significant.
Results
The surgical database contained a total of 218 patients, of whom 20 (9.2%) had a SSI (Table 1). Seven SSIs followed aortic surgery (n=127), and 13 SSIs followed after peripheral vascular surgery (n=91).
The microbiology and infection-prevention database included 236 patients, of whom 33 (14%) had positive scores for SSI (Table 1). The surgical registration data base included 14 SSIs after aortic surgery (n=133) and 19 SSIs after peripheral vascular surgery (n=103). Because of the discordant number of patients in the two databases, we merged the two databases into one, thus analyzing only the data for patients who were present in both databases. No infection was scored for the 28 patients present in the surgical database but absent from the microbiology and infection-prevention database. The latter database contained 45 patients who were not included in the surgical database, and two SSIs were present in this population. After merger of the two databases, 191 matching patients were found, in 155 of whom no infection was scored. An infection was documented in both databases in 15 patients.
The charts of patients (n=21 [11%]) whose results in the surgical database and microbiology and infection-prevention database were discordant were reviewed by the research investigator, surgeon, and medical microbiologist on the expert panel conducting the assessment of registration data, who where blinded to the patient's initial scores. After revision, 161 patients among the 191 patients with matching results in the two databases were found to be without infection and 30 patients scored positively for infection (Table 2). The data flow leading to these findings is shown in Figure 1). These 30 patients were considered as being truly positive for SSIs after review by the expert panel.
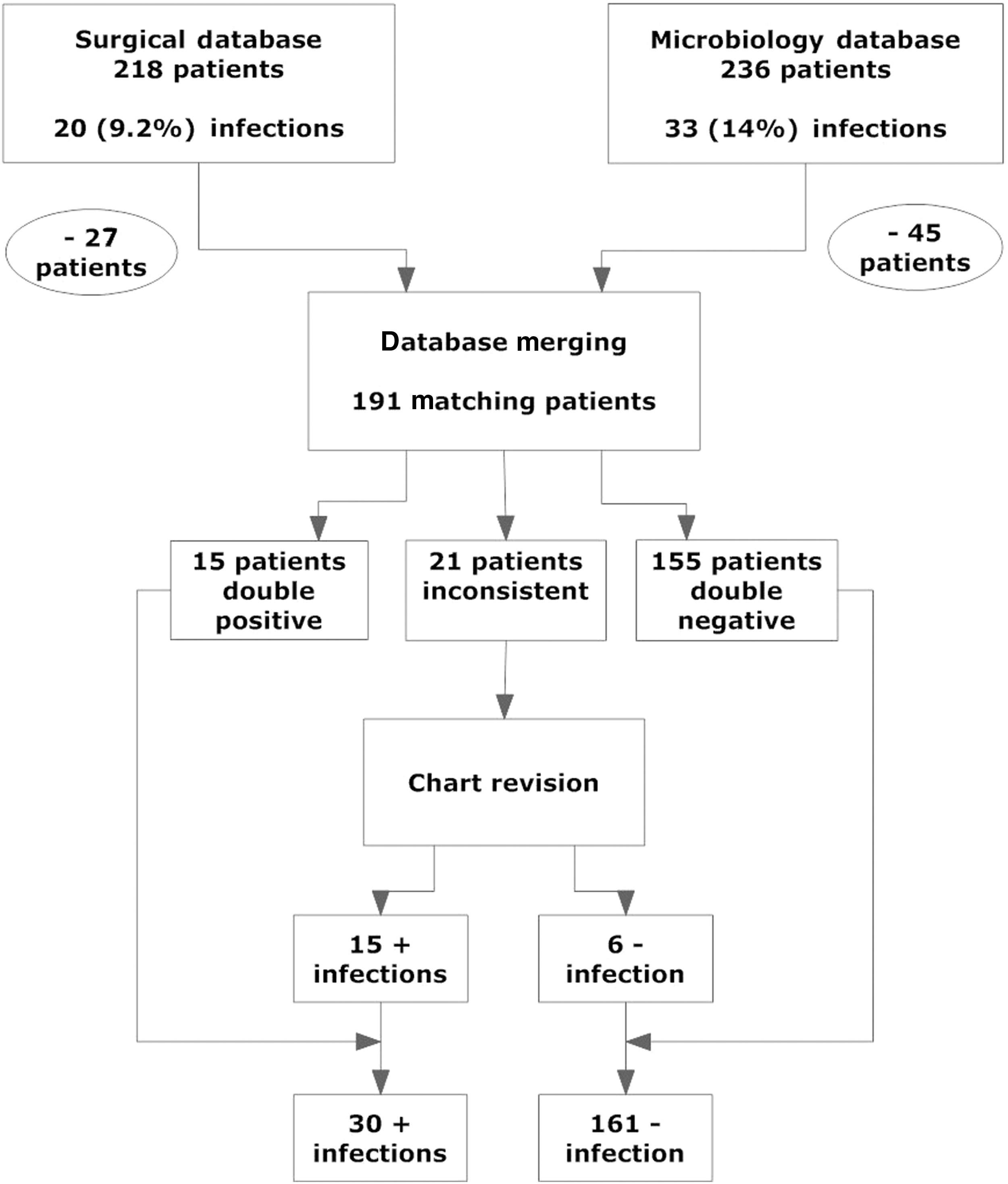
Data sources and steps in data processing leading to identification of true surgical site infections in patients undergoing abdominal aortic and peripheral vascular surgery.
Of all the patients who scored positively for a SSI, 13 scored positively for a SSI only scored in the microbiology database. Among these 13 patients, who were not scored positively for an SSI in the surgical database, 10 SSIs occurred after discharge. All 10 of these patients were readmitted to the hospital for proper diagnosis and treatment, indicating that their SSIs could also have been detected with the surgical registration method. The sensitivity of the surgical database for SSI was 57% and that of the microbiology and infection-prevention database was 93% (p<0.001; Table 3).
p<0.001 (Fisher exact test)
Discussion
Our study shows that SSIs are scored more reliably by infection-control nurses than by physicians. One explanation for this could be that data managers are focused on registering in an electronic database complications that are entered in a medical chart. The registration is done both for patients in the hospital and those in follow-up at an outpatient clinic. By comparison, the registration of a complication by a physician is but one of many aspects of the physician's work. Physicians recognize complications, treat them, explain them to patients, and document them in the patients' medical charts. Registration of a complication in a registry is for a patient unfortunately the least concerning part of the physician's work, and the documentation of complications, either on a printed form or in an electronic database, is easily overlooked.
Because physicians have to recognize and register not only possible SSIs but all the complications that might occur after a surgical intervention, the maintenance of a complications database is more work for them than for an infection-prevention nurse whose work consists of documenting SSIs. This might at least partly explain our results. Rates of sensitivity for the other complications registered in the surgical data base at our institution are hard to calculate because there are no other registrations with which to compare these complications, therefore making it almost impossible to calculate the true rates of SSI for the purpose of comparison.
The discordant results after combination of the surgical and microbiology and infection-prevention databases are explained partly by the way in which the registration was done. Some patients underwent multiple and different operations, but because we selected patients from our databases on the basis of surgical codes, our results were predicated on the entry of the correct code in the database. This was not always the case, with some patients being listed only with codes that differed from our surgical inclusion codes, resulting in the exclusion of these patients from one of our databases and their inclusion in the other database if their registration in it was done with the correct code. Because we needed a true value of the rate of SSI after vascular surgery, for calculating the sensitivity and specificity of identification of SSIs so as to be able to compare the results in our two databases, and because this true value was not known, we created our own reference base for true infections. After discussion at our expert panel meeting, we decided which patients had valid SSIs and which did not. This was done retrospectively on the basis of all the information registered prospectively in our surgical and microbiology and infection-prevention databases.
Almost all of the missed infections in the surgical database occurred after the patients who developed these infections had been discharged. However, every patient with a SSI that was not recorded in the surgical database was re-admitted to the hospital and received appropriate care.
The surgical registry failed to establish the number of SSIs after vascular surgery because the care team did not properly register this complication in the database. Because most of the SSIs in the surgical database occurred after the patients had been discharged, the outpatient clinic registration was particularly unreliable. A possible solution to this problem could be the assignment of a specially trained data manager to register all complications in a database.
Surgical site infection is a frequent complication after vascular surgery and is associated with increased morbidity and substantial additional cost [7–18]. Adequate registration of such infection is therefore necessary for its timely, adequate, and reliable evaluation. As more states in the United States make the reporting of healthcare-associated infections mandatory [19], the reliability of the method used for registration is becoming increasingly important. When, in a single surgical department in a single hospital, two different registration methods produce the different values for a single complication such as SSI that we found in our study, it is clear that the published results for complications are more dependent on the type of registration than on the quality of healthcare. The best results of such registration will be obtained when surgeons and the departments of microbiology and infection prevention work together in identifying and registering all SSIs.
Our center now uses a scheduled meeting with a vascular surgeon, a medical microbiologist, and a trained infection-control nurse to discuss and register every possible SSI and produce a reliable database for this complication.
However, considering the reports of SSI in the literature, with an incidence ranging from 4% to 43 % [6–17], our incidence of SSIs seems acceptable.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.