
Abstract
Abstract
Background:
Since 2005, we have been conducting prospective surgical site infection (SSI) surveillance and infection control according to the U.S. Centers for Disease Control and Prevention guidelines for patients who undergo gastrointestinal surgery at our institution. Surgical site infection occurs with greater frequency in emergency than in elective surgery because of factors such as ill-conceived preoperative preparation and “dirty” operations. A large number of studies have been reported on risk factors for SSI in elective colorectal surgery; however, there are few papers on such factors in emergency colorectal surgery. The aim of this study was to identify risk factors for incisional SSI in emergency colorectal surgery.
Methods:
Using our SSI surveillance database, we analyzed retrospectively 78 patients who underwent emergency colorectal surgery between 2005 and 2010. Univariable and multivariable analyses were used to identify risk factors for incisional SSI. Moreover, we subclassified dirty-infected operations (class IV) by the extent of contamination according to our own definition to study the incidence of incisional SSI at each degree.
Results:
The incidence of incisional SSI was 32.1% (25/78 patients). By univariable analysis, seven parameters correlated with a higher risk of incisional SSI: Surgical incision class III–IV, obesity (body mass index ≥25 kg/m2), American Society of Anesthesiologists score 3 or 4 points, chronic kidney disease (serum creatinine concentration >1.2 mg/dL), blood loss ≥200 mL, blood transfusion, and ventilator support. Multivariable analyses showed that surgical incision class III–IV (odds ratio [OR] 5.9; 95% confidence interval [CI] 1.7, 25.2) and obesity (OR 11.9; 95% CI 2.1, 87.8) were independent risk factors for incisional SSI. The incidence of incisional SSI in colon perforation with generalized contamination was statistically higher than that in prepared colon perforation and colon perforation with localized contamination (82.4% vs. 25.0%; p<0.001).
Conclusions:
The risk factors for incisional SSI in emergency colorectal surgery were incision contamination and obesity. Moreover, the incidence of incisional SSI among the incision class IV operations increased significantly with increasing extents of contamination. As a tactic for management of dirty abdominal wounds, we suggest that primary skin closure is suitable in cases of perforation of a prepared colon or colon perforation with localized contamination. On the other hand, in cases of colon perforation with generalized contamination, delayed primary skin closure or leaving an incision open to heal by secondary intention should be considered.
T
We focused on emergency colorectal operations. We performed a retrospective statistical analysis to identify risk factors for incisional SSI in such surgery. In addition, we subclassified dirty-infected operations (incision class IV) into three groups by extent of contamination according to our own definition to study the incidence of incisional SSI at each level.
Patients and Methods
Surveillance
Since 2005, we have been conducting prospective SSI surveillance and infection control according to the CDC guidelines [7] for all patients who undergo gastroenterologic surgery at the Institute of Gastroenterology (several types of gastrointestinal surgeons, including colorectal surgeons), Nippon Medical School Musashikosugi Hospital (branch hospital in a university setting). In the present retrospective study, attending physicians or nurses observed all operative sites at least once a day until patient discharge from the hospital. Post-discharge SSI surveillance was carried out in the outpatient clinic, and all patients were followed up for 30 d postoperatively. The diagnosis of SSI was made after discussion among attending physicians, nurses, and a dedicated infection control physician.
Using our SSI surveillance database from July 2005 to May 2010, a single-institutional retrospective statistical analysis was performed. The study included patients who underwent emergency colorectal operations that included at least one of the following procedures: Large bowel resection, anastomosis, colostomy creation, or simple closure of the colorectal region. Patients who underwent simple appendectomy, hernia incarceration relief, or ileus operation without manipulation of the colon or rectum were excluded. The abdominal incisions were closed primarily in all patients. Emergency operations were defined by the anesthesiologist (described in the anesthesia record). On-call operations that were not urgent were excluded from the analysis.
Standard protocol for dirty operations
As a matter of institutional policy, we followed a standard protocol for dirty-infected operations as follows: Peritoneal lavage was performed using >10 L of warm saline, a closed suction drain was placed in the abdominal cavity, the fascia was closed with knotted absorbable suture, gloves were exchanged, and the incision was irrigated with 500 mL of warm saline. The subcutaneous tissues were not approximated, and the incisions were closed with skin staples or “loosely” by suture. The use of a site protector and placement of a subcutaneous drain were not necessarily required. Because the management of all dirty-infected operations was by by this standard protocol, there was no open site management during the research period.
Perioperative antibiotic use
Preoperative oral antibiotics were not possible because these were emergency operations. For all class II (clean-contaminated) operations, prophylactic administration of a second-generation cephalosporin was started 30 min before skin incision in all cases. The dose was repeated every 3 h during surgery and stopped within 3 d after the operation. For class III (contaminated) and IV (dirty-infected) operations, various types and durations of third- or fourth-generation cephalosporin or carbapenem antibiotics were used, and de-escalation of antibiotics was performed according to the results of gram staining and bacterial culture.
Dependent variable
The dependent variable of this study was incisional SSI, which included both superficial and deep infections as defined by the CDC criteria. Specifically, incisional SSI was defined as an infection that occurred at the incision site within 30 d after surgery and was characterized by at least one of the following: Purulent drainage from the incision; an organism isolated from a culture of fluid from the incision; incisional pain, tenderness, localized swelling, redness, or heat with opening of the incision; and diagnosis by the surgeon or attending physician [7]. Superficial incisional SSI involves only the skin or subcutaneous tissue of the incision, whereas deep incisional SSI involves the deep soft tissues (e.g., fascial and muscle layers) [7].
Independent variables
The independent variables of the analysis were various patient characteristics, the preoperative data, and the operative variables such as gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, diabetes mellitus, smoking, preoperative serum albumin concentration, chronic kidney disease (preoperative creatinine concentration), surgical incision classification, duration of the operation, colostomy creation, blood loss, blood transfusion, and postoperative ventilator support. The anesthesiologist calculated the ASA score preoperatively. Body mass index was calculated from the patient's height and weight (kg/m2). The incision classification was based on the CDC definition as follows: Class I (clean), class II (clean-contaminated), class III (contaminated), or class IV (dirty-infected). All continuous and ordered variables were converted to categorical variables by setting cutoff values: age (< or ≥70 years), BMI (<25, ≥25), ASA score (≤2, ≥3 points), albumin concentration (≥3.0, <3.0 g/dL), creatinine concentration (≤1.2, >1.2 mg/dL), incision class (II, III–IV), duration of operation (≤75th percentile, >75th percentile), and total blood loss (<200, ≥200 mL). We subclassified dirty-infected operations (class IV) into three groups by degree of contamination according to our own definition to study the incidence of incisional SSI at each level. The definitions were as follows: Class IV-1 (prepared colon with perforation), class IV-2 (colon perforation with localized contamination), and class IV-3 (colon perforation with generalized contamination). Prepared colon perforation refers to the perforation of colon that had been prepared mechanically for colonoscopy. Our definition of colon perforation with localized contamination was cases without widespread contamination of the intraperitoneal cavity, such as those of encapsulated colon perforation or penetration (but not a free perforation).
Statistical analysis
Statistical analysis was performed using JMP software V. 10.0.0 (SAS Institute Inc., Cary, NC). The univariable relation between each independent variable and incisional SSI was evaluated using the Pearson χ2 test for all categorical variables. Independent variables with a p value<0.05 in the univariable analysis were used in the multivariable analysis by a stepwise logistic regression model. P values<0.05 were considered to be statistically significant. Calibration and discrimination of the regression model performance were assessed by the coefficient of determination (Nagelkerke generalized R2) and the area under the receiver-operating characteristic (ROC) curve.
Results
A total of 82 patients who underwent emergency colorectal surgery were enrolled in SSI surveillance, with 78 patients accepted for the final analysis. Three patients were withdrawn because they died or underwent reoperation <30 days after surgery and did not develop SSI during the study period. In addition, one patient with a colon diverticulum perforation was in a poor general condition, so we could perform only simple closure of the perforated site, stoma creation, and drainage. The intraperitoneal infection continued in this patient, and an incisional SSI developed. Because we could not determine whether the infection was an incisional or organ/space SSI, we excluded this patient from the analysis.
The mean age of the patients was 60.8±15.7 years with a range of 26–94 years, and 57.7% of the patients were male. Tables 1 and 2 summarize the operation causes, procedures, and the incisional SSI rates for each cause and procedure. Only one patient was scheduled for operation via a laparoscopic approach, and this operation was converted to laparotomy. Therefore, all the operations were performed via an open approach. The colon perforations in 33 patients were all class IV, and there were no patients with class III incisions.
These patients were believed to have acute appendicitis before their operation and underwent ileocecal resection.
SSI=surgical site infection.
NS=not significant.
The overall incidence of incisional SSI was 32.1% (25/78 patients). By univariable analyses, seven parameters correlated with a higher risk of incisional SSI: incision class III–IV, obesity (BMI ≥25 kg/m2), ASA score 3–4 points, chronic kidney disease (serum creatinine concentration >1.2 mg/dL), blood loss of ≥200 mL, blood transfusion, and ventilator support (Table 3). Multivariable analyses showed that surgical incision class III–IV and obesity were independent risk factors for incisional SSI (Table 4). Figure 1 indicates the relation between the subclass of class IV surgical incisions and incisional SSI rates. Thus, the SSI rates in class IV-1, IV-2, and IV-3 incisions were 0, 33.3%, and 82.4%, respectively. There was a significant difference in the incisional SSI rate of class IV-3 sites (82.4%) compared with that of class IV-1 and -2 incisions (25.0%) (p<0.001).
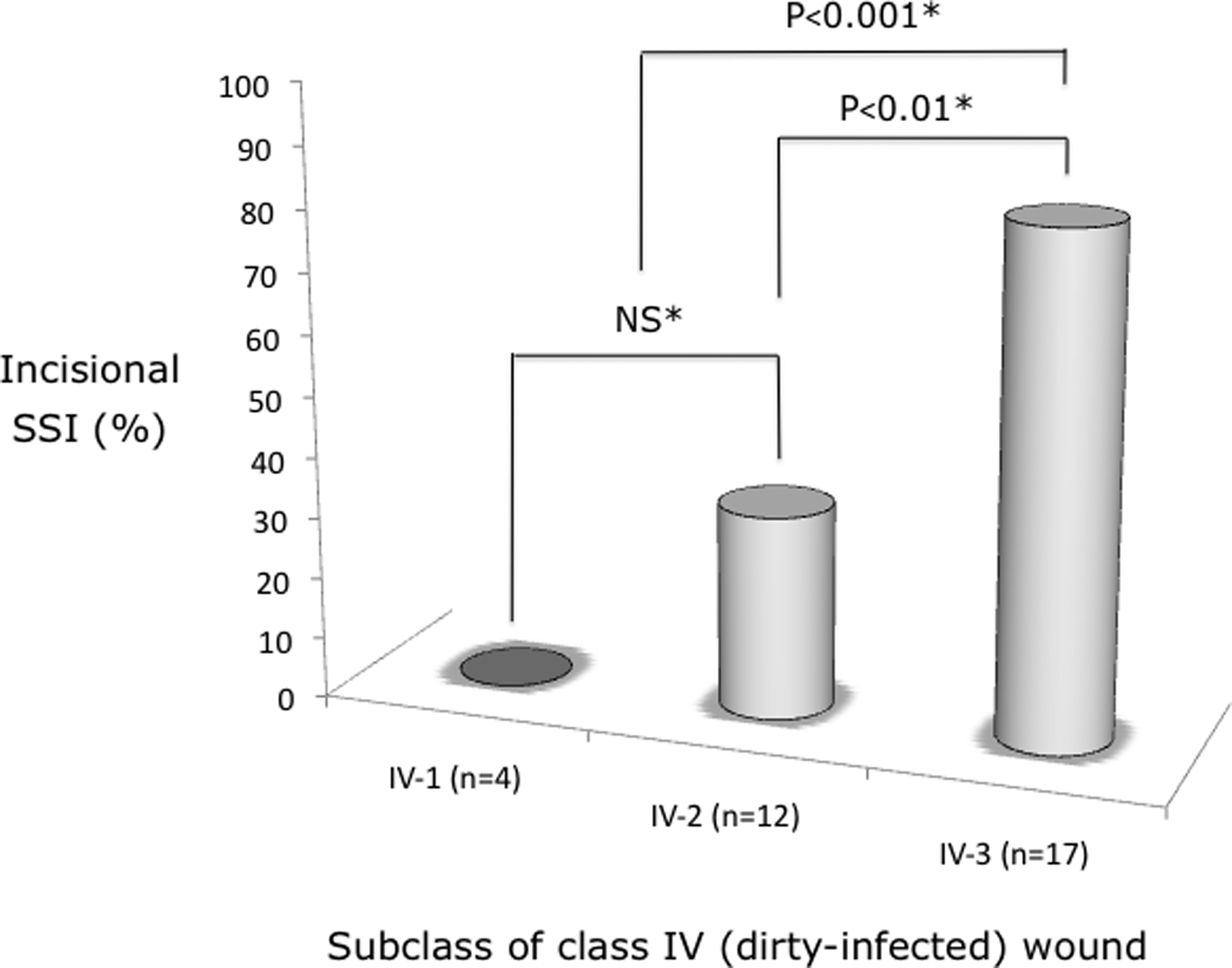
Incisional surgical site infection rates and subclass of class IV (dirty-infected) incisions (IV-1=prepared-colon perforation; IV-2=colon perforation with localized contamination; IV-3=colon perforation with generalized contamination). *Pearson χ2 test.
ASA=American Society of Anesthesiologists.
ASA=American Society of Anesthesiologists; BMI=body mass index; CI=confidence interval.
Nagelkerke's generalized R2 and the area under the ROC curve of the logistic regression model were 0.50 and 0.86, respectively. These findings of calibration and discrimination indicate that the regression model is relatively well fit.
Discussion
Surgical site infection occurs with greater frequency in emergency than elective gastrointestinal surgery because of factors such as ill-conceived preoperative preparation and dirty operations [6]. A large number of studies on risk factors for SSI in elective colorectal surgery have been reported [e.g., 8,9]; however, there are few papers on such risk factors in emergency colorectal surgery [5,10]. Therefore, we believe that SSI measures in emergency colorectal surgery have not been determined sufficiently. The CDC guidelines note that knowledge of risk factors for SSI before certain operations allows targeted preventive measures [7]. Thus, we have come to believe that analyzing risk factors for incisional SSI in emergency colorectal operations may suggest preventive tools.
This study indicates that incision contamination is a powerful independent risk factor for incisional SSI in emergency colorectal surgery. The following intraoperative SSI measures have been reported in dirty operations: subcutaneous tissue irrigation [11,12], peritoneal lavage [13], wound protection [11,14], subcutaneous drainage [10], antimicrobial sutures [15], and delayed primary closure [5]. There is no doubt that irrigation of the subcutaneous tissue and peritoneal lavage are effective in preventing incisional SSI; however, with what the incision should be irrigated is not yet clear [11–13]. A recently published meta-analysis of 24 randomized controlled trials (RCTs) encompassing 5,004 patients who underwent intraoperative lavage showed that povidone–iodine application significantly decreased the SSI rate [16]. Thus, the use of povidone–iodine is being discussed for highly contaminated operations [17].
Incision protection significantly reduced incisional SSI in elective open colorectal surgery in two RCTs [14,18]. Moreover, a protector that sticks to an incisional margin can press evenly in a circle and is considered to keep tissue moist and prevent tissue damage at incision sites, which may contribute to the prevention of incisional SSI [19]. Given these facts, site protectors are considered in theory to be effective for dirty wounds.
The present study has revealed that obesity (BMI ≥25 kg/m2) also is an independent risk factor for incisional SSI in emergency colorectal operations. Because obesity is a predictable preoperative risk factor for incisional SSI, some prospective RCTs have been reported on the usefulness of subcutaneous drains in obese patients [20,21]. Allaire et al. reported that the use of closed suction drainage in the subcutaneous space might reduce the incidence of postoperative site complications (including incisional SSI) in obese women who have at least 2 cm of subcutaneous fat and undergo cesarean delivery [20]. On the other hand, the use of subcutaneous drains in obese patients undergoing elective cholecystectomy, although it reduces seroma formation, does not affect incisional SSI [21]. It was recently reported that the incidence of incisional SSI in 79 patients at high risk for such infections who underwent colorectal resection, including obese patients (subcutaneous fat tissue thickness >20 mm) and those who underwent emergency operations with or without a subcutaneous drain, was 14.3% and 38.6%, respectively [10]. These results suggest that subcutaneous drains are effective for preventing incisional SSI, even in emergency operations and obese patients. This suggestion also is supported by our results that the independent risk factors for incisional SSI in emergency colorectal operation are the degrees of wound contamination and obesity.
In 2011, Galal and El-Hindawy reported the results of an RCT on the impact of using triclosan antimicrobial sutures on the incidence of SSI [15]. The use of antimicrobial suture led to a statistically significant decrease in the incidence of SSI in 450 patients undergoing various types of operations, including 65 cases of gastrointestinal surgery [15]. According to the results of this RCT, even in contaminated operations, antimicrobial sutures decreased the incidence of SSI (14% in the antimicrobial suture group vs. 31% in the control group) [15]. However, according to a systematic review and meta-analysis of seven RCTs encompassing 836 patients, triclosan-impregnated sutures did not decrease in the rate of SSI significantly (odds ratio 0.77) [22]. The effectiveness of the antimicrobial suture used in contaminated operations carrying a high risk of SSI is controversial, and RCTs of techniques for contaminated operations are needed.
Delayed primary closure involving only fascial suturing without primary closure reportedly is effective also for dirty abdominal wounds according to the results of another RCT (SSI rate 12%) [5]. However, the problem with this report is that incision closure was not performed when incisional SSI was suspected in the delayed primary closure group. According to the report, 26 patients were assigned to the delayed primary closure group, 12 of whom were suspected to have an infection in the open incisional site and did not undergo delayed primary closure [5]. Fourteen patients underwent delayed primary closure, three of whom developed an SSI [5]. Thus, 15 of 26 patients developed infection in the open or closed surgical site [5]. In other words, the SSI rate in these dirty operations was 57.7%, which is almost the same as the rate of 54.6% in the present study (see Table 3). Although colon perforation is defined uniformly by the CDC guidelines as leading to a class IV incision, our statistical analysis of the subclass of class IV incisions showed that there are various extents of contamination of dirty wounds and different incidences of incisional SSI depending on the extent. In the present study, there was a significant difference in the incisional SSI rate of class IV-3 sites (82.4%) compared with that of class IV-1 and 2 (25.0%)(p<0.001). The CDC guidelines recommend delayed primary skin closure or leaving an incision open to heal by secondary intention if the surgeon considers the surgical site to be heavily contaminated (e.g., class III and IV; category IB [7]. Class IV-3 incisions, as defined by us, are considered to be equivalent to heavily contaminated sites, for which the CDC guidelines recommend delayed primary skin closure. More specifically, we assume that primary skin closure can be performed for class IV-1 and 2 sites, which show an incisional SSI rate of approximately 25%, whereas the use of delayed primary skin closure or leaving an incision open to heal by secondary intention should be considered for class IV-3 sites, which show an incisional SSI rate of 80% or higher.
There are several limitations to this study. The first is the difficulty in analyzing the use of antibiotics because antibiotics were used, not only for serious underlying intra-abdominal infections, but also for a variety of concomitant indications (e.g., pneumonia and sepsis) in patients with generalized peritonitis. In such cases, the duration and type of antibiotics also differed. The second limitation is that emergency colorectal surgery, the inclusion criterion for this study, comprised both perforation and obstruction groups, which had different incidences of and risk factors for incisional SSI. The final limitation is that there were other known risk factors that were not evaluated but that could predispose a patient to SSI, including intraoperative hypothermia, differences in the use of incision protectors and preoperative steroids, and prolonged preoperative hospitalization.
Conclusions
The risk factors for incisional SSI in emergency colorectal surgery were incisional contamination and obesity. Moreover, the incidence of incisional SSI among the site class IV operations increased significantly with increasing extents of contamination. Although colon perforation, a typical indication for colorectal emergency surgery, is defined as a dirty-infected wound by the CDC guidelines, there are various extents of contamination. As a treatment strategy for dirty abdominal wounds, we assume that primary skin closure can be allowed for prepared colon perforations or colon perforations with localized contamination, even if this treatment involves a dirty operation such as that for colon perforation. On the other hand, for colon perforations with generalized contamination, the use of delayed primary skin closure or leaving an incision open to heal by secondary intention should be considered.
Footnotes
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.