
Abstract
Abstract
Background:
Ventilator-associated pneumonia (VAP) accounts for almost 90% of infections in mechanically ventilated patients and more than one-quarter of all patients requiring intubation, with associated mortality rates as high as 70%. The rise in methicillin resistance within the community has led to a national increase in methicillin-resistant Staphylococcus aureus (MRSA) rates in early VAP and associated healthcare expenditure.
Methods:
Trauma patients identified via an institutional VAP database were stratified by gender, age, severity of shock (24-h transfusions), and severity of injury. The primary outcome measure was evaluation of the incidence and trend of early MRSA VAP over a 6-y period. Secondary outcomes examined the adequacy of our current empiric antibiotic regimen as it pertained to outcome variables, including mortality.
Results:
A total of 997 episodes of VAP were identified in 727 patients. Linear regression showed that the incidence of early Staphylococcus aureus (SA) VAP was stable over the 6-y period (slope=−0.911; p=0.490). Over the same 6 y, however, the percentage of MRSA in early SA VAP (slope=3.95; p=0.0154) and the incidence of early MRSA VAP increased. No difference in mortality was detected between early methicillin-susceptible SA and early MRSA VAP. After adjustment for age, ISS, and 24-h transfusion requirements, early MRSA was not an independent predictor of mortality (odds ratio [OR], 0.815; p=0.59).
Conclusions:
Although the incidence of early SA VAP with methicillin resistance increased significantly within the first 7 d of admission, this study showed no difference in mortality and resource utilization between early VAP from MRSA and other causative organisms, despite lack of empiric MRSA coverage.
V
The development of VAP and the causative pathogen is variable and dependent on length of hospital stay. Early-onset VAP is associated with less-resistant pathogens and a shorter length of stay (LOS) [6]. Historically, early VAP attributed to Staphylococcus aureus (SA) as the causative pathogen comprised relatively higher percentages of methicillin-sensitive SA (MSSA) versus methicillin-resistant SA (MRSA) in trauma patients [7,12]. However, documented increases in community-acquired MRSA (CA-MRSA) over the last decade has resulted in increasing methicillin resistance rates within community-acquired pneumonia (CAP) [13]. The increase in methicillin resistance within the community has led to a national increase in MRSA rates in early VAP and associated healthcare expenditures [14,15]. The purpose of this study was to evaluate the incidence and trend of early MRSA VAP over a 6-y period in our Level 1 trauma center and to examine the adequacy of our current empiric antibiotic regimen.
Materials and Methods
Identification of patients and demographics
Trauma patients eligible for this study were admitted to the Presley Regional Trauma Center in Memphis, TN from January 1, 2004, through December 31, 2009. Patients were identified via an institutional VAP database. Demographic and additional patient information was obtained from the trauma registry (NTRACS 3.5, Digital Innovations, Inc., Forest Hill, MD). Patients were stratified by gender, age, severity of shock (24-h transfusions), and severity of injury (admission Glasgow Coma Scale score [GCS], Injury Severity Score [ISS], and chest Abbreviated Injury Score [AIS]).
Diagnosis and management of VAP
Ventilator-associated pneumonia was suspected if a patient had been mechanically ventilated ≥48 h; evidence existed of new or changing infiltrate on chest radiograph; and met at least two other criteria: 1) temperature >38°C or <36°C; 2) white blood cell count (>10,000 cells/mm3,<4,000 cells/mm3, or 10% immature bands); or 3) macroscopically purulent sputum [16,17]. Patients with suspected VAP underwent bronchoscopy in a uniform manner with bronchoalveolar lavage (BAL) as described previously [9,17–19].
Empiric anti-microbial therapy in our trauma unit is standardized via a VAP pathway that has been well validated [7,9,19–25]. Briefly, empiric antimicrobial selection was based on days from admission. Immediately after bronchoscopy, patients with suspected early VAP (onset ≤7 d from admission) were started on ampicillin-sulbactam 3 g intravenous (IV) q 6 h in absence of a beta-lactam allergy. In the absence of allergy, patients with suspected late VAP (onset >7 d from admission) were started on vancomycin 20 mg/kg IV q 12 h plus cefepime 2g IV q 8 h. Beta-lactam allergic patients were started on moxifloxacin 400 mg IV q 24 h or ciprofloxacin 400 mg IV q 8 h plus vancomycin 20 mg/kg IV q 12 h for early VAP and late VAP, respectively. Antibiotics were adjusted to renal function. Vancomycin doses were adjusted to achieve steady-state peak plasma concentrations between 35–45 mg/L and trough concentrations between 15 to 20 mg/L.
Ventilator-associated pneumonia was diagnosed when BAL culture results contained at least one species demonstrating growth of ≥100,000 colony-forming units/mL (CFU/mL) (18,26–28). Preliminary culture results were used only when ≥24 h had elapsed after the initial BAL (23,24). Anti-microbial therapies were narrowed or expanded based on the resulted culture sensitivities and the trauma pathway for definitive therapy was followed.
Outcomes
The primary outcome measure was evaluation of the incidence and trend of early MRSA VAP over a 6-y period. Secondary outcomes were intended to examine the adequacy of our current empiric antibiotic regimen. Outcome variables included ventilator days, intensive care unit length of stay (ICU LOS), hospital LOS, and mortality.
Statistics
Differences were compared using chi-square and the Fisher exact test for categorical variables and the Student t-test for continuous variables. Linear regression was used to examine the relationship between VAP rates over the study period. A multi-variable model was constructed to identify if early MRSA VAP was an independent predictor of mortality. All statistical analysis was performed using JMP version 8 and SAS version 9.2 (SAS Institute, Cary, NC). A p value of less than 0.05 was considered significant. The Institutional Review Boards at the Regional Medical Center at Memphis and the University of Tennessee Health Science Center approved this study.
Results
A total of 997 episodes of VAP were identified in 727 patients (1.4 episodes per patient) during the 72 mo period. Early VAP (512 episodes) represented 51.4% of episodes of VAP. The majority of patients were male (81%) with a mean age, ISS, and admission GCS of 41, 31 and 9, respectively. Overall mortality was 19% for the entire cohort. There was no difference in demographics between patients with early MRSA VAP and all other causes of early VAP. Injury severity was equivalent between the groups as measured by ISS, chest AIS, GCS, and transfusions. There were also no differences in outcomes, including ventilator days, ICU LOS, hospital LOS, and mortality (Table 1). To examine the potential severity of inadequate empiric antibiotic therapy (IEAT) with MRSA VAP, we compared mortality between early MSSA and early MRSA VAP. No difference was detected between these two cohorts (25.4% vs. 17.5%, p=0.283). Multi-variable logistic regression was then performed to see if MRSA was an independent risk factor for mortality. After adjustment for age, ISS, and 24-h transfusion requirements, regression failed to show early MRSA as an independent predictor of mortality (odds ratio [OR], 0.815; p=0.59).
Values expressed as means or percentages.
ISS=Injury Severity Score; GCS=Glasgow Coma Scale Score (on admission); AIS=Abbreviated Injury Score; ICU=intensive care unit; LOS=length of stay.
Figure 1 depicts the total number of early VAP, early MSSA VAP, and early MRSA VAP episodes over time. Linear regression shows that the incidence of early SA VAP was stable over the 6-y period (slope=−0.911; p=0.490). The actual percentage of early VAP caused by SA did not differ. Over the same 6 y, however, the percentage of MRSA in early SA VAP (slope=3.95; p=0.0154) and the incidence of early MRSA VAP increased (slope=1.35; p=0.0028; (Fig. 2).
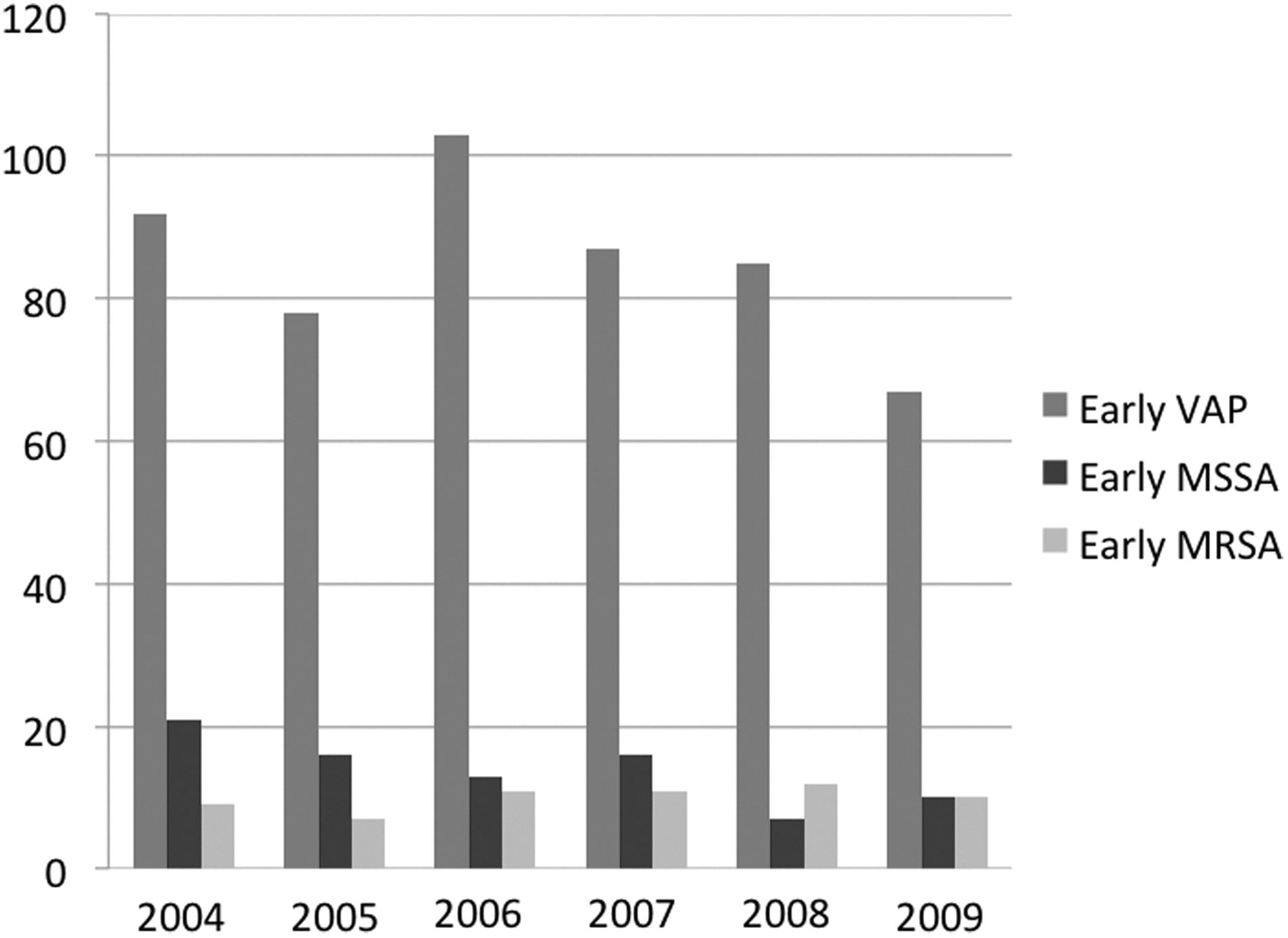
Total number of early ventilator-associated pneumonia (VAP), early methicillin-sensitive Staphylococcus aureus VAP, and early methicillin-resistant S. aureus VAP.
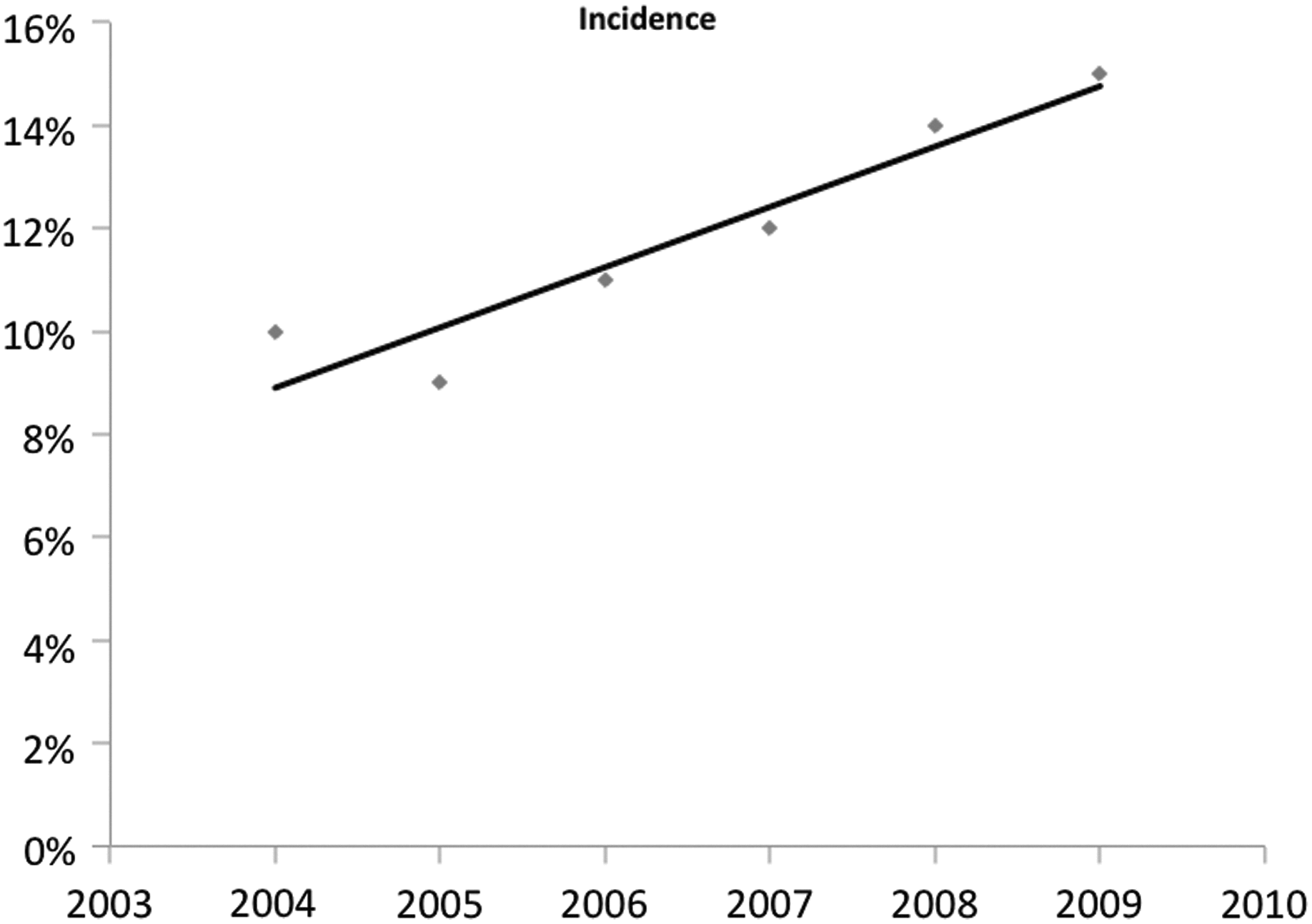
Linear regression of methicillin-resistant Staphylococcus aureus incidence in early ventilator-associated pneumonia.
There were a total of 29 species isolated as causative pathogens for early VAP during the study period. Some of the more common pathogens were SA, Haemophilus spp., Streptococcus pneumoniae, Pseudomonas aeruginosa, Enterobacter spp., Escherichia coli, and Klebsiella spp. Gram-negative pathogens were more common than gram-positive pathogens in early VAP (55.3% versus 44.7%). The cumulative incidence of the most common early VAP pathogens (SA, Haemophilus spp., and S. pneumoniae) was 67.3%.
Discussion
Ventilator-associated pneumonia is responsible for a substantial number of infections in ventilated patients and has been associated with high mortality rates. Trauma patients exhibit unique pathogens and lower mortality rates compared to other patient populations. Chastre et al. reported mortality rates from VAP as high as 70% in non-trauma populations [1]. In 2010, Cook et al. showed that VAP was more common in trauma patients; however, mortality was significantly lower, when compared to non-trauma VAP [29]. Mortality in our study was comparatively low at 18%. It is clear that treatment tactics should be hospital—perhaps even units, specific and account for local pathogen virulence. As bacteria continue to evolve resistance, it is imperative to the monitor continuously effectiveness of previously established practices.
During the 6-y period that comprised this study, the pathogens isolated from positive BAL cultures remained remarkably similar to previous data from our institution. Wood et al. noted the various rates of each positive VAP culture in our trauma unit from 1998–2001. In both the previous study and this study, early VAP was more likely to be gram-negative than gram-positive (57% vs. 43% and 55% vs. 45%). In addition, the most prevalent early pathogens were also Haemophilus influenzae, Staphylococcus aureus, and Streptococcus pneumoniae and comprised 63% of the positive cultures [7]. For almost two decades, the pathogens responsible for our early VAP have remained consistent and have retained a stable sensitivity profile. This pathogen consistency and their sensitivities are attributable to our appropriate selection of empiric antibiotics, strict adherence to treatment algorithms, and prompt de-escalation of empiric antibiotics.
Goals of practice should continue to include avoidance of IEAT in attempts to reduce morbidity and mortality. Studies in other institutions and our own have proved that multiple episodes of IEAT increase patients' risks of mortality; however, patients receiving only a single episode of IEAT had no difference in outcomes versus no episodes [8–10,20]. Magnotti et al. explained that the lack of difference in mortality or resource utilization from a single episode of IEAT could be due to the inherent differences associated with surgical and trauma populations [9]. Another possibility is prompt antibiotic therapy adjustment in our institution and use of preliminary BAL results at 24 h after culture attainment. Swanson et al. demonstrated that preliminary culture results at 24 h can be used safely to adjust antibiotic regimens in attempts to preserve antibiotic sensitivities and optimize patient outcomes [23]. In the rare instance that MRSA was responsible for the early VAP, the lack of difference in resource utilization or mortality could be due to the relatively short period in which patients were exposed to the single episode of IEAT.
Recently, Mera et al. analyzed 1,761,991 SA isolates reported to a national database from 1998–2007. Over the 10-y period methicillin resistance in the community increased from 33% to 54% [30]. In 2009, Vardakas et al. estimated that the overall incidence of CAP from MRSA is 0.51–0.64 cases per 100,000 population [13]. Although incidence was low, they found MRSA CAP resulted in a severe pneumonia and most often required ICU admission with mortality rates at 45%. They attributed the high mortality rate to the fact that patients were not hospitalized until 4–5 d after symptom onset, resulting in long delays before initiating appropriate antibiotics.
Not surprisingly, the increasing presence of MRSA in early VAP has mirrored the growing incidence of CA-MRSA. The mean occurrence of early MRSA VAP in the current study was 12% over the six-years with previous rates in our unit being around 4% [7]. Whereas the source of the early MRSA is unclear, we did notice that the clindamycin sensitivity in the early isolates was 72% and only 55% for the late MRSA isolates. Although not a definitive way to identify CA-MRSA, this 17% difference may be due to increasing prevalence of CA-MRSA. In the current study, empiric therapy for early MRSA VAP would have resulted in an overusage of antibiotics and placed 88% of patients at risk of developing some level of resistance or superinfection. The presence of multi-drug-resistant pathogens is correlated with days since admission, location, and prior antibiotic usage [31,32].
The retrospective design of this study has inherent limitations. True cause and effect between early MRSA VAP and the measured outcomes cannot be determined. For example, we do not know if these patients died ultimately due to the VAP or if they just died with VAP. To better identify attributable mortality risk, Bekaert et al. built a logistic regression model for the daily probability of acquiring VAP by using a weighted comparison of all types of ICU patients without VAP to those with VAP. Furthermore, using time-dependent covariates such as daily organ injury scores, the authors inferred the impact of acquiring VAP on ICU-mortality as a function of time [33]. Our analysis was obtained from an institutional database consisting of only trauma patients with the diagnosis of VAP. The database did not include daily organ function scores for the entire ICU stay. Therefore, we were unable to create a weighted comparison to patients without VAP, nor were we able to include such time-dependent covariates as daily organ function scores. Nevertheless, the objective of this study was never to demonstrate early MRSA as the true source of in-hospital mortality, but rather demonstrate its association with mortality compared to other bacterial etiologies. The association between VAP in trauma patients and mortality is well described in the literature [29]. Our multi-variable logistic regression analysis failed to identify a significant association between early MRSA and mortality after adjusting for important admission characteristics that have previously been described as predictors of mortality in trauma patients [34,35].
The study was well powered with a large sample size; however, associations within the results are not comprehensive, but subject to the few variables selected a priori. The study was designed to trend the incidence of early MRSA within the Presley Regional Trauma Center. Already mentioned, it is suggested highly that treatment pathways be designed and implemented based on local microorganism virulence and resistance. As such, caution is warranted when extrapolating these results to other intensive care settings or even other trauma units. Although there are apparent differences in toxin production and virulence between different strains of Staphylococcus aureus, our microbiological laboratory does not genotype every isolate.
It is evident that the incidence of early SA VAP with methicillin resistance is increasing, significantly, within the first seven days of admission. However, this study shows no difference in mortality and resource utilization between early VAP from MRSA and other causative organisms, despite lack of empiric MRSA coverage. Based on these findings, our current antibiotic algorithm for VAP is adequate and no changes are warranted. Even though empiric MRSA coverage did not benefit this study population as a whole, initial coverage should be considered in some patients. It is known that patients with co-morbidities, recent hospital exposure, or recent antibiotic usage are at high risk for multi-drug-resistant pathogens. These results also reinforce the necessity of continuous pathogen and resistance monitoring along with unit-specific treatment pathways.
Author Disclosure Statement
No competing financial interests exist.