
Abstract
Abstract
Background:
The incidence of infected femoral artery pseudoaneurysms is likely to increase with increasing numbers of femoral artery interventions.
Methods:
Case report and review of literature.
Results:
We present a case of dehiscence of a vein patch repair of an infected femoral pseutoaneurysm treated with ligation of vessels and coverage by rectus abdominis muscle flap.
Conclusion:
We consider the use of this flap as a good second line option for the coverage of exposed femoral vessels, in the presence of sepsis, particularly when the external iliac artery has been ligated.
Case Report
A 50-year-old patient had an elective open resection of a right atrial angiosarcoma and a single right coronary artery bypass graft done with a long section of saphenous vein from the right groin. Intra-operatively he required an intra-aortic balloon pump, which was inserted through the left groin with a percutaneous technique. Because of bleeding at the insertion site, a cutdown was done and polyprolylene sutures were placed to achieve hemostasis.
Two weeks after the initial operation, the patient developed a 2.8-cm pseudoaneursym in his left groin following removal of the sheath from his left common femoral artery. This was diagnosed on ultrasonography and treated with an ultrasound-guided injection of thrombin.
However, the thrombin injection was unsuccessful and was repeated. Over the next 5 d, cellulitis developed in the patient's left groin, in association with edema of the left lower limb extending proximally into the pelvis. A computerized tomographic angiogram (CTA) revealed that the pseudoaneurysm was 4.2 cm in diameter and in close apposition to the skin (Fig 1).

Three-dimensional reconstructed computed tomographic angiogram demonstrating a 4-cm pseudoaneurysm communicating with the distal left common femoral artery.
The psuedoaneurysm was primarily repaired emergently with a vein patch of long saphenous vein from the contralateral groin. Skin preparation at surgery was done with an alcoholic solution of povidone-iodine and vancomycin 1 g IV given at induction. Proximal vascular control of the left external iliac artery was achieved through a left Rutherford Morison (oblique, left iliac fossa) incision. Coverage of the repaired artery was achieved by mobilizing the left sartorius muscle medially from the anterior superior iliac spine.
The wound was left open and a topical negative-pressure dressing was applied the next day. An intraoperative tissue culture specimen and blood cultures grew Klebsiella pneumoniae, which was sensitive to ertapenem, and the patient was treated with this antibiotic. His clinical signs of sepsis then diminished.
Six days post-operatively the patient's repair dehisced. At surgery, the common and superficial femoral arteries and profunda femoris artery were ligated because of clinical evidence of frank infection. The sartorius muscle had necrosed in its proximal region. The Rutherford-Morison incision was opened to reveal frank pus, which was drained. Prophylactic four-compartment fasciotomies were performed and the leg was found to be ischemic as compared with the contralateral leg but was deemed viable.
Coverage of the over-sewn vessel stumps necessitated the raising of a rectus abdominis flap. This was achieved with the existing Rutherford Morison incision (Fig. 2A). The left-sided anterior rectus sheath was opened longitudinally in its midline. The pedicle of the inferior epigastric artery was identified medial to the spermatic cord (see Fig. 2A).

The pedicle of the inferior epigastric artery was skeletonized, providing the pivot point for rotation of the flap. The rectus abdominis muscle was dissected below the arcuate line from the transversus abdominis fascia and above the arcuate line from the posterior rectus sheath. An appropriate length of rectus abdominis muscle was measured and the muscle was divided superiorly and transposed to the recipient defect via a tunnel created beneath the inguinal ligament (Fig. 2F). With care taken to avoid twisting or stretching of the inferior epigastric vessels, several absorbable sutures were loosely placed into adjacent muscles in the groin. The Rutherford-Morison incision was drained with a 30-gauge Robinson drain and closed in layers, and the groin wound was drained with two closed vacuum drains, packed, and covered with an occlusive dressing.
The wound was inspected on the day following this procedure and the muscle was found to be healthy and was dressed with a topical negative-therapy dressing. The infected arterial segment was sent for culture and grew K. pneumoniae. The patient made a good post-operative recovery with a warm foot and no pain at rest. The vascularity of the patient's left leg was maintained via collateralization, and no immediate re-vascularization was required. Motor and sensory neurologic function were preserved. Drains were removed and fasciotomies closed on the fourth post-operative day.
Discussion
Sartorius, rectus femoris, and rectus abdominis muscle flaps (Fig. 3) have been described for coverage of vascular suture lines across femoral vessels in the settings of actual or potential infection [1–4]. The sartorius muscle flap is often used as a first-line option because of its ease of use and good outcome [5–11].
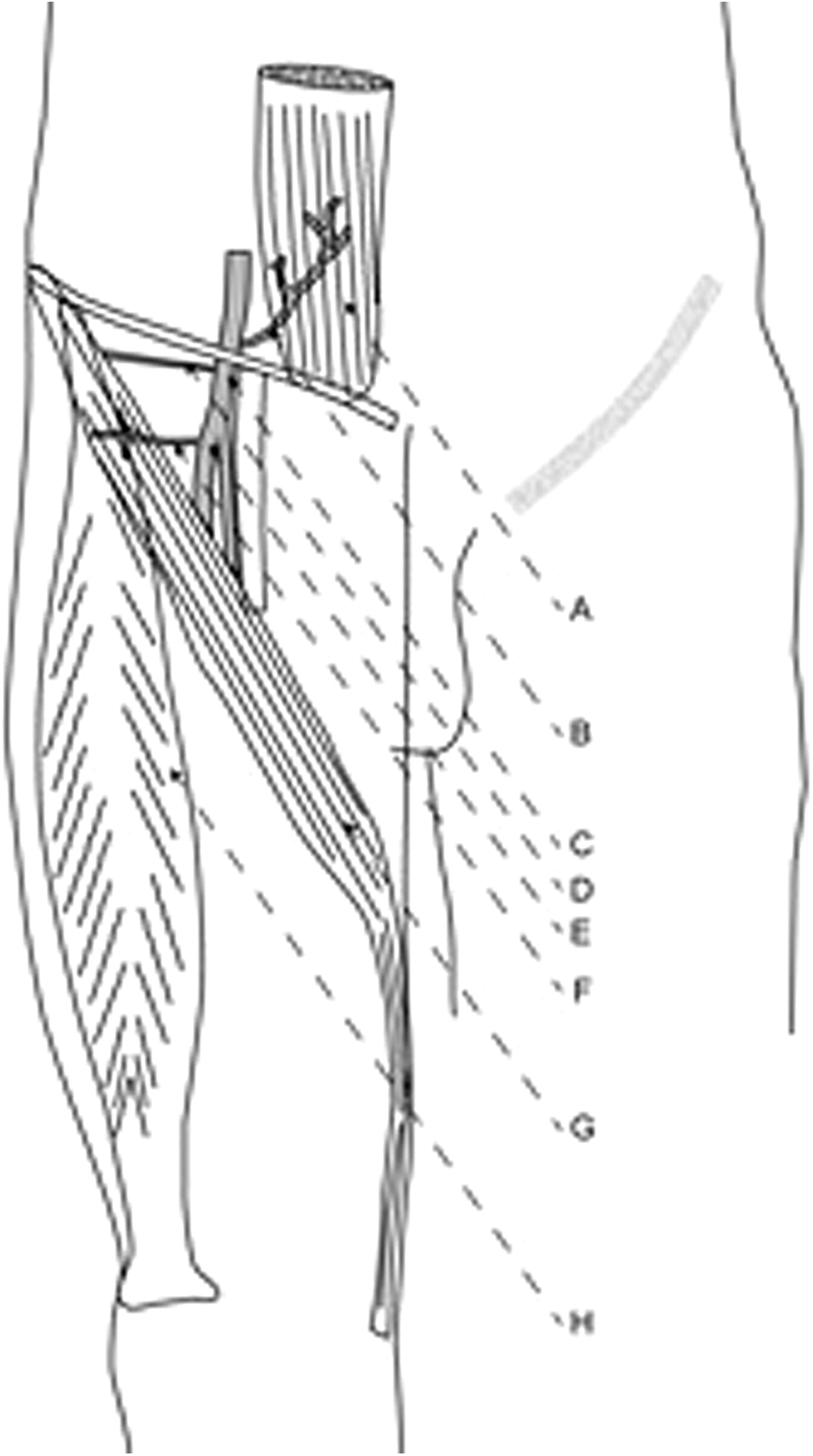
Diagram representing the arterial supply and location of the rectus abdominis and sartorius muscles in relation to the femoral artery.
The proximal blood supply of the sartorius muscle flap is provided by the superficial circumflex branch of the common femoral artery and the lateral circumflex branch of the profunda femoris artery [12]. Its viability may be enhanced by preserving its proximal, medially based blood supply [13,14]. The blood supply to the rectus femoris muscle is also largely from the profunda femoris artery [15]. Ligation of the superficial femoral artery (SFA) may not affect the viability of the sartorius muscle flap, but this possibility may not extend to cases in which both the SFA and the profunda femoris arteries have been ligated [16].
However, the rectus abdominis muscle flap relies for its blood supply on the inferior epigastric artery, which is a division of the external iliac artery before the latter passes beneath the inguinal ligament. Hence, its vascularity will not be compromised by arterial ligation in the groin done because of complications of the repair of an infected psudoaneurym. Furthermore, it has been shown that flaps dependent upon the inferior epigastric artery flaps do not increase morbidity of the abdominal wall [17–19]. This complication in the case described here was due to a deep incisional surgical site infection, which is likely to have been inoculated at the time of initial femoral artery puncture for cardiac intervention. With the increased number of such procedures being performed, it is imperative that appropriate care is taken to ensure aseptic technique for preventing such problems.
The inferiorly based flap of the rectus abdominis can be used to cover complex vascular groin wounds. It is particularly useful following injury to the femoral vessels with resulting compromise of the major vascular pedicles of the commonly used thigh muscular flaps. We consider the use of this flap as a good second-line option for the coverage of exposed femoral anastomoses, particularly in the presence of infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.