
Abstract
Abstract
Background:
Pasteurella multocida is a commensal organism present in the oral cavities of many animals. It can cause various infections including soft tissue, joint, and respiratory infections in human beings, but intra-abdominal infection by P. multocida is rare. We report our experience with a case of acute cholecystitis with bacteremia caused by P. multocida.
Case Report:
The patient was a 39-year-old female who underwent emergency laparoscopic cholecystectomy for acute cholecystitis. The patient's blood and bile cultures were positive for P. multocida. She kept a dog and a cat as pets, but denied having had any bites or major scratches. Our investigation did not find that she had any sign of other potential sources of infection.
Conclusion:
Acute cholecystitis can be a primary source of Pasteurella bacteremia in a previously healthy, young patient.
P
Case Report
A 39-year-old female presented to the emergency department of our hospital with a chief complaint of acute, severe epigastric pain and fever. She had a history of right hypochondrial pain after meals for several years. Because her attacks of such pain had increased in frequency, she had been scheduled for elective laparoscopic cholecystectomy.
The patient was admitted to the medical service with a diagnosis of acute cholecystitis, and because her symptoms did not resolve after the administration of ampicillin-sulbactam, she was referred to the surgical department 2 d after admission. She had a temperature of 37.7 °C and was distressed by severe colicky pain. She had tenderness of the right upper quadrant and a positive Murphy sign. Peritoneal irritation was absent. Laboratory examination revealed a leukocyte count of 21,200 cells/mcL, C-reactive protein concentration of 12 mg/dL, and normal hepatobiliary enzyme activity.
Ultrasound examination revealed a markedly distended gallbladder (119×38 mm) with moderate wall thickening. A gallstone was lodged in the neck of the gallbladder (Fig. 1). Computed tomography (CT) demonstrated features similar to those on ultrasonography, and abscess formation was ruled out. We diagnosed acute cholecystitis and performed a laparoscopic cholecystectomy on the same day, and the patient had an uncomplicated post-operative course.
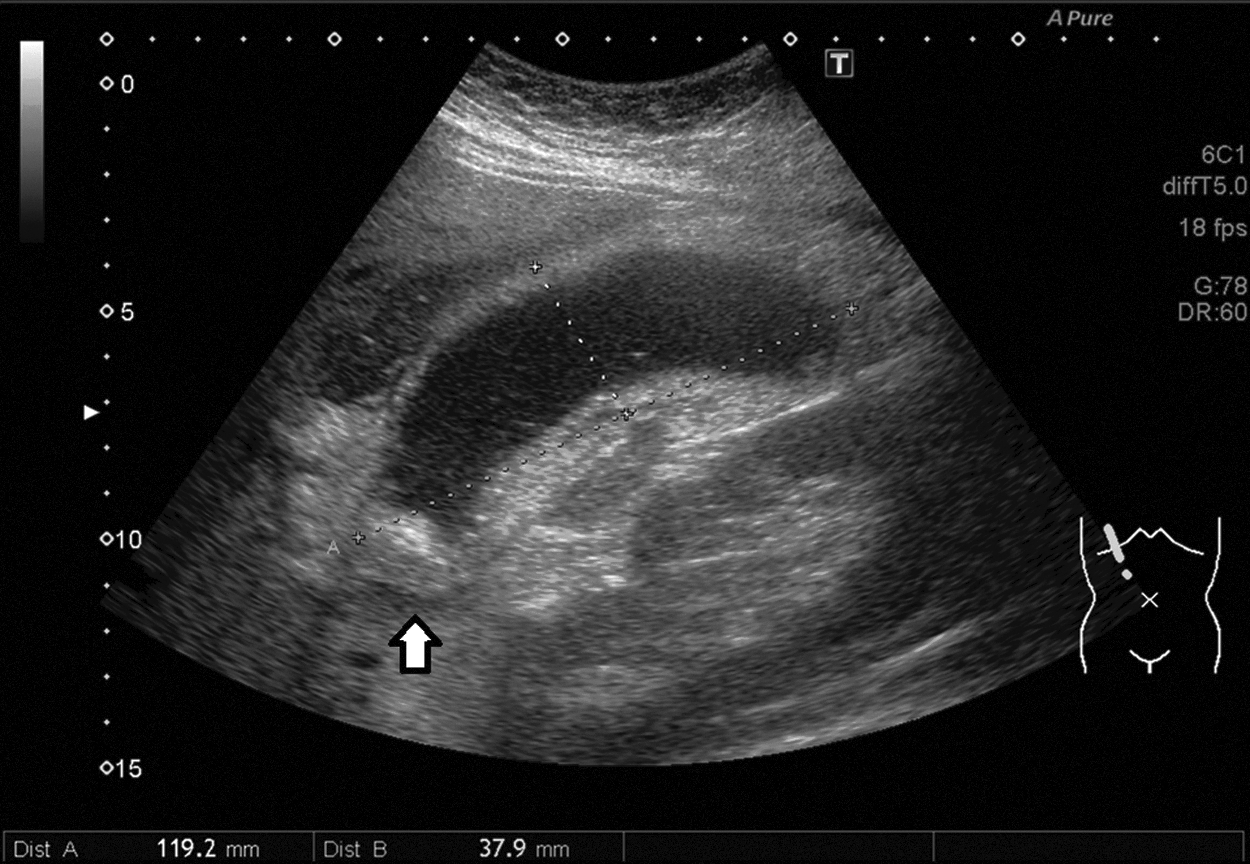
Ultrasound image showing marked gallbladder distension. The arrow shows a gallstone lodged in the gallbladder neck.
Culture of a blood specimen obtained on the day of admission and cultures of bile were positive for P. multocida. It was revealed that the patient kept a dog and a cat as pets, but she denied having had any bites or major scratches. The patient did not have any sign of lymphadenopathy or of soft tissue, joint, or respiratory infection. Echocardiography did not show evidence of endocarditis.
The patient was treated with 1 wk of IV ampicillin-sulbactam followed by 1 wk of oral ciprofloxacin. The patient has shown no signs of recurrence of her infection.
Discussion
Pasteurella species are aerobic-to-facultatively anaerobic, non-motile, small gram-negative coccobacilli that inhabit the oral cavity and gastrointestinal tract of many animals, including cats and other felines, dogs, pigs, and a wide variety of domestic and wild animals [1]. Among Pasteurella spp., P. multocida is the most common species causing human infection, which was first described in 1930 when an infection developed after a cat bite [2].
Infection after animal bites is the most commonly reported clinical setting for Pasteurella. Approximately 15% to 20% of wounds from dog bites and more than 50% from cat bites become infected by Pasteurella spp. [3].
A substantial proportion of Pasteurella infections, develop in patients exposed to animals but without a history of bites or scratches, as in the case of our patient, or can develop in persons who have had no animal exposure or contact whatsoever [4]. Although the mode of infection in most reported cases of Pateurella infection is not clear, it is presumed to result from inadvertent direct inoculation of organisms or from colonization of the upper respiratory tract, with subsequent dissemination to the respiratory, cardiovascular, and gastrointestinal systems, the ocular or central nervous system, or the genitourinary tract [1]. Underlying respiratory tract disease, such as chronic obstructive pulmonary disease or bronchiectasis, is considered a risk factor for colonization with Pasteurella.
Unsurprisingly, the most common site of Pasteurella infection is skin and soft tissue, but such infection can as also have an uncommon presentation, such as arthritis, osteomyelitis, pneumonia, meningitis, bacteremia, or endocarditis. Reported cases of intra-abdominal infection with Pasteurella have included primary bacterial peritonitis, peritoneal dialysis-related peritonitis, intra-abdominal abscess, and appendicitis [5,6]. To our knowledge, the present case report is the second case report of acute cholecystitis caused by P. multocida [7]. The key to the diagnosis in our case was the isolation of the organism from blood and bile cultures.
Clinical experience with Pasteurella and numerous in vitro studies indicate that penicillin is the best antimicrobial agent for the treating virtually all forms of infection with the organism. Other options are cephalosporins, tetracyclines, fluoroquinolones, macrolides, and trimethoprim-sulfamethoxazole [1,8]. The strain we identified was susceptible to all of these antibiotics. Because adequate source control of the patient's infection was accomplished by surgery, we had planned to administer ampicillin-sulbactam intravenously for a total of 14 d, but there is no evidence that such prolonged therapy is needed.
Even though the perioperative management of Pasteurella cholecystitis was unremarkable, healthcare providers should be aware of the poor prognoses of patients with end-organ forms of Pasteurella infection [1]. For example, mortality in Pasteurella-induced meningitis, bacteremia, and endocarditis is approximately 25%–30% for each type of infection [9–11]. This is probably because most patients with serious infections have had predisposing diseases including liver dysfunction, cancer, chronic kidney disease, or diabetes mellitus.
Footnotes
Author Disclosure Statement
No competing financial interests exist.