This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of the American College of Surgeons and the Surgical Infection Society. The American College of Surgeons is accredited by the ACCME to provide continuing medical education for physicians.
AMA PRA Category 1 Credits™
The American College of Surgeons designates this live activity for a maximum of 22 AMA PRA Category 1 Credits™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
American College of Surgeons
Inspiring Quality:
Highest Standards, Better Outcomes
Disclosure Information
In compliance with ACCME Accreditation Criteria, the American College of Surgeons, as the accredited provider of this activity, must ensure that anyone in a position to control the content of the educational activity has disclosed all relevant financial relationships with any commercial interest. All reported conflicts are managed by a designated official to ensure a bias-free presentation. Please see the insert to this program for the complete disclosure list.
Program
Wednesday, April 18, 2012
12:00–13:00
Executive Council Luncheon (By invitation)
Fairway Ranch
13:00–17:00
Executive Council Meeting (By invitation)
Fairway Ranch
17:00–18:00
Nominating Committee (By invitation)
Fairway Ranch
19:00–21:30
Presidential Dinner (By invitation)
Byron's
Thursday, April 19, 2012
07:30–10:15
ANNUAL UPDATE SYMPOSIUM:
Prevention of Surgical Site Infection: A Systematic Review of the Evidence
Four Seasons Ballroom
Welcome and Introduction
Sandra Berrios-Torres, MD and E. Patchen Dellinger, MD
Evidence-based update to the CDC/HICPAC guideline for prevention of surgical site infection: Developmental process
Sandra Berrios-Torres, MD
Surgical site infection prevention: Antibiotic prophylaxis and the evidence
Kamal M. F. Itani, MD
Antimicrobial bowel preparation and systemic antibiotics in elective colon surgery
Donald E. Fry, MD
Glycemic control and prevention of surgical site infection
Lillian Kao, MD
Staphylococcus aureus: Screening and decolonization
Charles E. Edmiston, MD
Prevention of surgical site infection in joint replacement surgery
Elie Berbari, MD
Teamwork and collaboration for prevention of surgical site infection
E. Patchen Dellinger, MD
Panel discussion
Sandra Berrios-Torres, MD, E. Patchen Dellinger, MD, and Arvind Nana, MD
10:15-10:30
Break
10:30–12:00
Tribute Symposium in Memory of Doctor Stephen F. Lowry
Four Seasons Ballroom
Remembrance
Philip S. Barie, MD, MBA
Stephen Lowry 1986-1991: Five years that defined sepsis research for the next century
Lyle L. Moldawer, PhD
The human endotoxin model: A brief review and some dose-response considerations
Steven E. Calvano, PhD
Imaging for microbes
Yuman Fong, MD
Defining and measuring surgical quality
Carla C. Braxton, MD, MBA
12:00–13:30
Lunch
Pavilion
13:30–16:50
PLENARY SESSION
Four Seasons Ballroom
The Art and Science of Surgical Infections (Papers 1–9)Moderators: Pamela A. Lipsett, MD, MHPE and Robert Sawyer, MD
O1.Regulation of sepsis-induced mitochondrial respiration/biogenesis by a nitric oxide, carbon monoxide pathway. Sean Whelan, (resident) presenting. University of Pittsburgh.Discussant: Michael West, MD, PhD
O2.Infectious complications following exploratory laparotomy for trauma: The case for improved antibiotic prophylaxis. Kareem Husain, (new member) presenting. Washington University.Discussant: Jeffrey Claridge, MD
O3.Synthesis and efficacy of a novel phosphate-rich PEG compound (Phospho-PEG) with anti-virulence activity against multiple-antibiotic-resistant pathogens. Alexander Zaborin, presenting. University of Chicago.Discussant: Donald E. Fry, MD
O4.Can surgical site infection after joint arthroplasty be reduced? Mayank Taneja, presenting. Rothman Institute, Thomas Jefferson University.Discussant: E. Patchen Dellinger, MD
O5.Endothelial TLR4 signaling is responsible for intestinal ischemia in the pathogenesis of necrotizing enterocolitis via its effect on the expression of microvascular tone regulators: eNOS and endothelin-1. Ibrahim Yazji (resident), presenting. University of Pittsburgh.Discussant: Henri R. Ford, MD, MHA
O6.Chest x-ray report language is incongruous with quantitative culture results in ventilator-associated pneumonia. Heather Evans, presenting. University of Washington.Discussant: Addison K. May, MD
O7.Bacterial and mitochondrial DNA assays distinguish sepsis from SIRS in primates. Carl Hauser, presenting. Beth Israel Deaconess Hospital/Harvard Medical School.Discussant: Philip S. Barie, MD, MBA
O8.Multi-drug resistance does not influence mortality in critically ill patients with Acinetobacter infections. Claire Murphy, presenting. The Ohio State University.Discussant: Nicholas Namias, MD, MBA
O9.Remote ischemic preconditioning prevents lung and liver injury following hemorrhagic shock/resuscitation. Chung Ho Leung, presenting. St. Michaels-Toronto.Discussant: Timothy R. Billiar, MD
Committee Meetings (Attendance mandatory for committee members)
Pavilion
08:00–09:45
PARALLEL SESSION I
Amphitheater
Fundamental Mechanisms of Surgical Infection (Papers 10–15)Moderators: William G. Cheadle, MD and Ori D. Rotstein, MD
O10.Cues present at anastomotic leak sites induce a stable mexT mutation in Pseudomonas aeruginosa causing enhanced tissue-destroying capacity. Benjamin Shoga (resident), presenting. University of Chicago.Discussant: Brian Zuckerbraun, MD
O11.Interleukin (IL)-25 improves innate and acquired immunity during parenteral nutrition. Aaron Heneghan, presenting. University of Wisconsin-Madison.Discussant: Jared Huston, MD
O12.Oncostatin M (OSM) receptor deficiency provides a survival advantage in a septic shock model. Pang Young (resident), presenting. University of Alberta.Discussant: John C. Marshall, MD
O13.Neurotransmitters modulate expression and release of cold-inducible RNA-binding protein (CIRP), a proinflammatory mediator in macrophages. Weng-Lang Yang (new member), presenting. Hofstra North Shore-LIJ School of Medicine.Discussant: William G. Cheadle, MD
O14.Age and autophagy in sepsis-induced acute kidney injury: A role for the calcium/calmodulin-dependent protein kinases. Gina Howell (resident), presenting. University of Pittsburgh.Discussant: Rachel Khadaroo, MD, PhD
O15.The ApoE4 isoform is associated with an increased inflammatory response in humans after in vivo endotoxin challenge. Stephen Gale, presenting. Robert Wood Johnson Medical School-University of Medicine and Dentistry of New Jersey.Discussant: Alfred Ayala, PhD
08:00–10:30
PARALLEL SESSION II
Four Seasons Ballroom
Clinical Investigations in Surgical Infection (Papers 16–21)Moderators: John C. Marshall, MD and Mark Malangoni, MD
O16.The burden of unnecessary empiric antibiotic therapy in suspected ventilator-associated pneumonia. Jeremy Thompson, presenting. Vanderbilt University.Discussant: Charles Adams, MD
O17.Re-defining the clinical pulmonary infection score (CPIS) for trauma patients. George DeBusk (resident), presenting. Brown University.Discussant: Lillian Kao, MD
O18.Do narcotics have an impact on the presence of Pseudomonas infections in the ICU? Sandra Swoboda, presenting. The Johns Hopkins University.Discussant: Soumitra R. Eachempati, MD
O19.Acute kidney injury (AKI) is associated with early cytokine dysregulation after trauma. Azra Bihorac (new member), presenting. University of Florida and University of Washington.Discussant: David Efron, MD
O20.Procalcitonin concentration (PCT) is associated with severity of sepsis in critically ill surgical patients (CrISPs). Vanessa Ho (resident), presenting. Weill Cornell Medical College.Discussant: Therese Duane, MD
O21.Diagnosis of infection after trauma splenectomy: It's about the lack of platelets and not the white blood cell count. Aman Banerjee (resident), presenting. MetroHealth Medical Center/Case Western Reserve University.Discussant: David Blake, MD
10:00–10:15
Break-Visit the Exhibits
10:15-11:15
William A. Altemeier Memorial Lecture
Four Seasons Ballroom
Colon Cancer: Do Alpha-Bugs Lead the Charge?Cynthia L. Sears, MD
11:15-12:15
Surgical Infection Society Presidential Address
Four Seasons Ballroom
I am Not a ScientistRobert G. Sawyer, MD
12:00–13:30
LUNCHEON SYMPOSIUM
Pavilion
(Industry-sponsored; not part of scientific program)
13:30–15:45
PARALLEL SESSION III
Amphitheater
Understanding the Host Response to Surgical Infection (Papers 22–29)Moderators: Nicholas Namias, MD and Alfred Ayala, PhD
O22.Neuregulin-4 protects intestinal cells from NEC-inducing bacteria by reduced apoptosis without promotion of cell restitution. Shannon Castle (new member, resident), presenting. Children's Hospital, Los Angeles.Discussant: Jose M. Prince, MD
O23.Dysregulation of miR-142-3p, -146, -299, and-200c downregulates HMGB1 and induces microbial tolerance in a novel model of chronic peritonitis. Ziad Kanaan (resident), presenting. University of Louisville.Discussant: Michael A. West, MD, PhD
O24.Commensal bacteria play a protective role in mediating mortality from pneumonia-induced sepsis. Benyam (Ben) Yoseph, presenting. Emory University.Discussant: John C. Alverdy, MD
O25.A dampened inflammatory response in critically ill geriatric patients is essential to survival.Mary Ottinger (resident), presenting. Brown University.Discussant: John A. Mannick, MD
O26.Changes in leukocyte expression of Ecrg4 following burns: An immunosurveillance marker? Nicole Lopez (new member, resident), presenting. University of California, San Diego.Discussant: Marc Jeschke, MD
O27.The role of T regulatory cells in mesenchymal stromal cell (MSC)-mediated wound healing. Kristin Cook (resident), presenting. University of Medicine and Dentistry of New Jersey-New Jersey Medical School.Discussant: Joanne Lomas-Neira, PhD
O28.Increased elderly T cell co-inhibitory receptor expression & SHP-1 activation depress T cells, increasing infections. Gautam Bandyopadhyay (new member), presenting. University of Rochester.Discussant: Ori D. Rotstein, MD
O29.Evolutionary dynamics of anastomotic leak: Investigation of virulent phenotype switching in Pseudomonas aeruginosa with an agent-based model. Jordan Stern (resident), presenting. The University of Chicago.Discussant: Daithi Heffernan, MD
13:30–16:00
PARALLEL SESSION IV
Four Seasons Ballroom
Outcomes Studies in Surgical Infection (Papers 30–37)Moderators: Lena M. Napolitano, MD and Addison K. May, MD
O30.Reduction in Acinetobacter infections associated with reduction of environmental contamination of a trauma/burn intensive care unit (ICU). L. Sylvia Munoz-Price, presenting. University of Miami.Discussant: Heather L. Evans, MD
O31.Burn-induced inflammatory response in adipose tissue. Celeste Finnerty (new member), presenting. University of Texas Medical Branch/Shriners Hospitals for Children.Discussant: Basil A. Pruitt Jr., MD
O32.Admission serum procalcitonin concentration (PCT) diagnoses sepsis accurately in a surgical intensive care unit (SICU) patient population. Peter McWhorter (resident), presenting. Weill Cornell Medical College.Discussant: Donald E. Fry, MD
O33.Examination of the bacterial microbiome in bronchoalveolar lavage samples from trauma patients utilizing next-generation sequencing technology. Ryan Huebinger (new member), presenting. University of Texas-Southwestern.Discussant: Gary An, MD
O34.Mortality associated with ventilator-associated pneumonia (VAP) has decreased over time. Laura Rosenberger (resident), presenting. University of Virginia.Discussant: Martin Croce, MD
O35.The differing microbiologic profile of ventilator-associated pneumonia (VAP) in geriatric versus young trauma patients. Andrew Stephan (new member), presenting. Brown University.Discussant: Lewis Kaplan, MD
O36.Does negative pressure therapy reduce surgical site infections following contaminated ventral hernia repair? David Krpata (resident), presenting. Case Western Reserve University.Discussant: Kamal Itani, MD
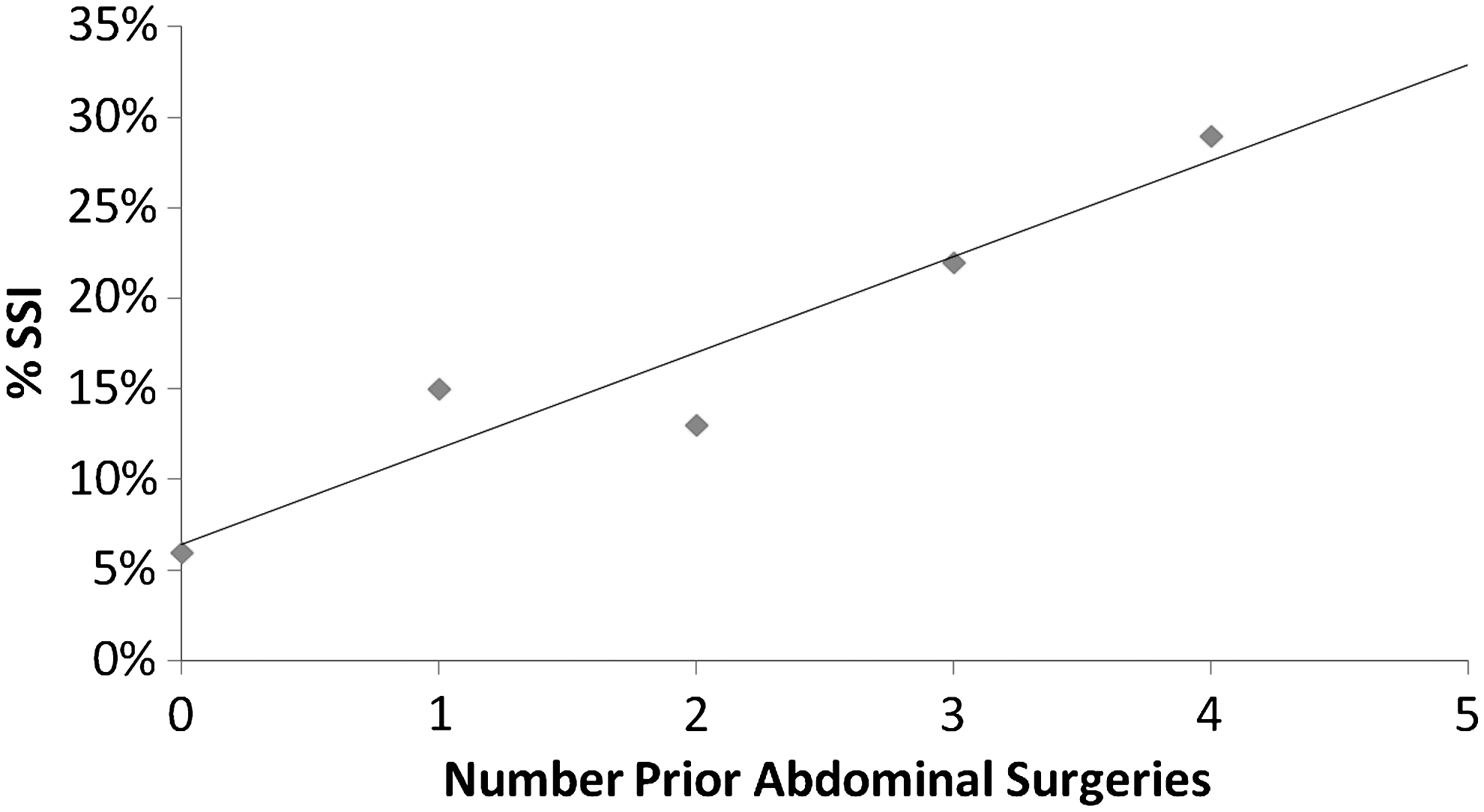
O37.Outcomes and predictors of surgical site infection (SSI) in stoma reversal. Jennifer Moffett (resident), presenting. Baylor College of Medicine/Rice University.Discussant: Jose Prince, MD
16:00–17:20
POSTER SESSION (Posters 1–58)
Basic and Clinical Studies in Surgical Infection
Section 1:
Microbiology, Biochemistry, and Antibiotic Use (Posters 1–4, 7,10–13)
Co-moderators: Matthew Rosengart, MD, Gautam Bandyopadhyay, PhD, Kelly Hogan, PharmD
Section 2:
Surgical and Other Therapies (Posters 15–24)
Co-Moderators: Greg Beilman, MD, Samir Awad, MD, Jose Prince, MD
Section 3:
Surgical Site and Skin/Soft Tissue Infections (Posters 25–28, 30–33, 35, 37, 40)
Co-Moderators: Kamal M. F. Itani, MD, Lewis Kaplan, MD, Jeffrey Bailey, MD
Section 4:
Other Infections (Posters 42–49)
Co-Moderators: Philip S. Barie, MD, MBA, Heather L. Evans, MD, Alicia Mohr, MD
Section 5:
Outcome and Risk Factor Analyses (Posters 50–58)
Co-Moderators: Lillian Kao, MD, Thomas Z. Hayward, III, MD, Sandra Swoboda, MS
17:30–18:30
Annual Business Meeting Presiding: Pamela A. Lipsett, MD, MHPE (Members only)
Amphitheater
19:30–20:00
Reception
Foyer
20:00–22:00
Awards Banquet
Four Seasons Ballroom
SATURDAY, April 21, 2012
07:00–08:00
Executive Council Meeting(By invitation)
TBA
08:00–09:00
SPECIAL CLINICAL SYMPOSIUM:
Unique Infections in the Military Operational EnvironmentCo-Moderators: COL Greg Beilman, MD and COL David Blake, MD
Prevention and treatment of combat-related infections
CDR Carlos Rodriguez, MD
Infection control in a deployed setting
COL Duane Hospenthal, MD
Utilizing a trauma systems approach to prevent infectious complications in combat casualty care
COL Jeffrey Bailey, MD
Panel discussion
09:00–11:00
COMBINED SESSION I
Four Seasons Ballroom
Mechanistic Insights into the Development of Surgical Infection (Papers 38–44)Moderators: John C. Alverdy, MD and Edwin A. Deitch, MD
O38.Cholinergic signaling in the gut: A novel mechanism in barrier protection through activation of enteric glial cells. Gerald Cheadle, presenting. University of California, San Diego.Discussant: Jared Huston, MD
O39.Sepsis-induced cardiac mitochondrial deficiency involves altered mitochondrial localization of tyrosine kinase cSrc and tyrosine phosphotase Shp2. Qun Zang, presenting. University of Texas-Southwestern.Discussant: Carl Hauser, MD
O40.Investigating the dynamics of bacterial virulence in necrotizing enterocolitis with a multi-scale agent-based model. Moses Kim, presenting. The University of Chicago.Discussant: Matthew Rosengart, MD
O41.Bacterial diversity in formula-fed vs. breast-fed rats and its possible role in susceptibility to necrotizing enterocolitis (NEC). Brandon Bell, presenting. Children's Hospital, Los Angeles.Discussant: John Alverdy, MD
O42.Addition of proanthocyanidins to intra-gastric elemental nutrition stimulates intestinal goblet cell size and function. Joseph Pierre, presenting. University of Wisconsin, Madison.Discussant: John Mazuski MD, PhD
O43.Shock/sepsis-induced neutrophil infiltration and mortality is mediated by ngiopoietin (Ang)-2. Joanne Lomas-Neira, presenting. Brown University.Discussant: Philip Efron, MD
O44.Hepatic apoptosis and liver dysfunction post-burn is mediated by c-Jun N-terminal kinase-2. Alexandra Smith, presenting. Sunnybrook Health Science Center.Discussant: Jeffrey Upperman, MD
11:00–11:15
Break–Visit the Exhibits
11:15-11:30
FELLOWSHIP AWARD RECIPIENT PRESENTATIONSModerator: Philip S. Barie, MD, MBA
Four Seasons Ballroom
The role of CaMK in the regulation of autophagy and sepsisGina Howell, MD, University of Pittsburgh. Mentor: Matthew Rosengart, MD, MPH
Mediators of endothelial cell dysfunction in the development of shock-induced acute lung injuryJoanne Lomas-Neira, MS, PhD, Brown University.
11:30–13:30
COMBINED SESSION II
Four Seasons Ballroom
Basic Science and Clinical Investigations (Papers 45–52)Moderators: Jeffrey Claridge, MD and Ping Wang, MD
O45.Surgeons don't listen: Evaluation of compliance with antimicrobial stewardship program (ASP) recommendations. Therese M. Duane, presenting. Virginia Commonwealth University.Discussant: Joseph Solomkin, MD
O46.Anti-inflammatory drug discovery in vivo: Use of the zebrafish to screen compounds for their ability to inhibit neutrophil infiltration. Filip Miscevic, presenting. St. Michael's Hospital, Toronto.Discussant: John Davis, MD
O47.The use of e-test minimum inhibitory concentration (MIC) values to determine vancomycin treatment failures in a surgical ICU population. Jonathon Pouliot, presenting. Vanderbilt University.Discussant: Greg Beilman, MD
O48.The invariant natural killer T-cell (iNKT) response is enhanced in critically ill septic geriatric patients. Daithi Heffernan, presenting. Brown University.Discussant: Carol Miller-Graziano, PhD
O49.Intravenous immunoglobulin (IVIG) does not confer protective immunity against infections in deceased donor kidney recipients. Avinash Agarwal, presenting. University of Virginia.Discussant: Ping Wang, MD
O50.The intestinal mucus layer is a critical but unrecognized component of the gut barrier. Jordan Fishman, presenting. University of Medicine and Dentistry of New Jersey-New Jersey Medical School.Discussant: Olga Zaborina, PhD
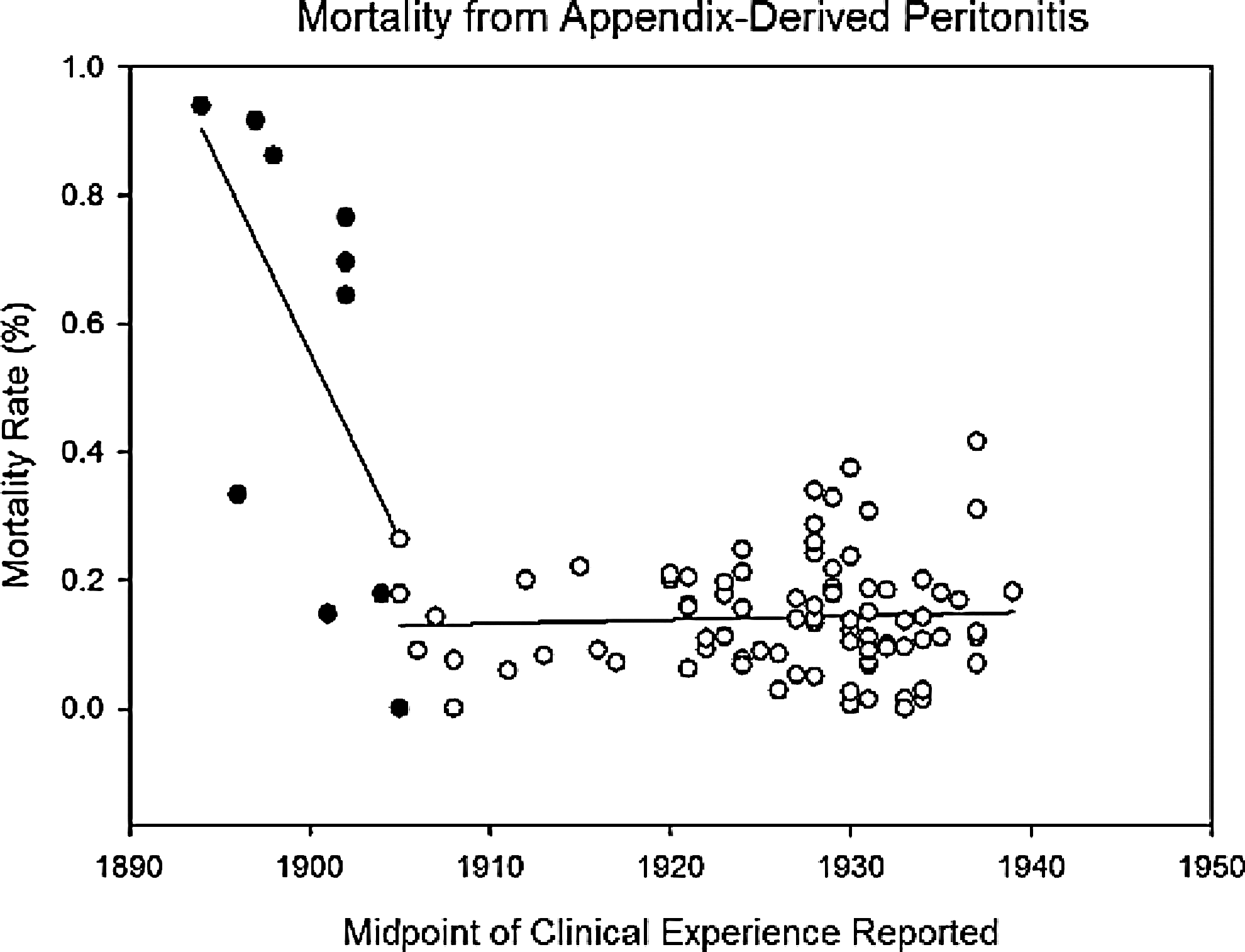
O51.How much do antibiotics help? A meta-analysis of outcome from appendix-derived peritonitis (PAP) before antibiotics. Xiuwen Wu, presenting. Nanjing University.Discussant: Lena M. Napolitano, MD
O52.TNF-α Nco1 polymorphism and sepsis susceptibility in surgical patients. Kavita Baghel (new member, resident), presenting. Chatrapatti Sahuji Maharaj Medical University, Lucknow, India.Discussant: Joseph P. Minei, MD
13:30
ADJOURNMENT
Oral Presentation Abstracts
WhelanSeanCarchmanEvieZuckerbraunBrian
University of Pittsburgh
REGULATION OF SEPSIS-INDUCED MITOCHONDRIAL RESPIRATION/BIOGENESIS BY A NITRIC OXIDE, CARBON MONOXIDE PATHWAY
Background: Organ injury and dysfunction in sepsis accounts for significant morbidity and mortality. Adaptive cellular responses in the setting of sepsis prevent irreversible injury and allow for organ recovery. Others and we have shown that part of the adaptive response includes regulation of respiration and maintenance of a healthy mitochondrial population.
Hypothesis: The purpose of these investigations were to test the hypothesis that regulation of mitochondrial respiration and homeostasis is regulated by inducible nitric oxide synthase (iNOS)/NO signaling. Furthermore, NO signaling is dependent on upregulation of heme oxygenase-1 (HO-1) and carbon monoxide (CO) signaling.
Methods: Experimental sepsis was induced using a cecal ligation and puncture model in iNOS knockout (ko) or wild type (C57BL/6) mice. Some mice were randomized to treatment with CO-releasing molecule (CORM 10mg/kg), the NO scavenger 1400W, or vehicle controls. Additionally, some mice were treated with scramble or HO-1 specific siRNA via tail vein injection. Primary mouse hepatocytes were utilized from these mice. Lipopolysaccharide was utilized in vitro at a dose of 100 ng/mL. Oxygen consumption and extracellular acidification rates were analyzed by Seahorse Analyzer. Western blotting, immunohistochemistry, and rtPCR was performed for analysis of HO-1, iNOS, markers of autophagy, and markers of mitochondrial biogenesis.
Results: LPS treatment inhibited aerobic respiration in vivo in wild type but not iNOS knockout cells. Experimental sepsis in vivo or LPS in vitro induced iNOS and HO-1 protein levels; however, induction of HO-1 was dependent on iNOS expression. Furthermore, experimental sepsis or LPS-induced hepatic autophagy/mitophagy and biogenesis, and this was significantly attenuated in iNOS ko mice or cells, with NO scavenging, or with knockdown of HO-1. Moreover, these responses in iNOS-deficient mice or with HO-1 knockdown could be restored via delivery of CO both in vivo and in vitro. Additionally, CO treatment minimized cell injury and death.
Conclusions: These data suggest that regulation of respiration and mitochondrial responses are dependent at least in part on a NO, CO signaling pathway. Further investigations are required to elucidate the regulatory mechanisms and relative contributions of these endogenous gaseous molecules in preventing organ injury in sepsis.
HusainKareemKeuneJasonSatoBryanJarmanSteveYanYanCarrollWilliamBochicchioGrantSchuererDouglasMazuskiJohn
Washington University
INFECTIOUS COMPLICATIONS FOLLOWING EXPLORATORY LAPAROTOMY FOR TRAUMA: THE CASE FOR IMPROVED ANTIBIOTIC PROPHYLAXIS
Background: Patients who undergo exploratory laparotomy for trauma are at high risk for intra-abdominal and surgical site infection (SSI). Much focus has been directed at appropriate type and timing of prophylactic antibiotics, but little attention has been paid to antibiotic re-dosing when there is large blood loss or lengthy operation, or antibiotic use in patients undergoing delayed fascial closure.
Hypothesis: Ideal administration of perioperative antibiotics decreases postoperative infections in patients undergoing exploratory laparotomy for trauma.
Methods: All surviving patients undergoing exploratory laparotomy for trauma at a level one trauma center from November 2009–June 2011 were analyzed, including patients whose fascia was not closed at the initial operation. Prophylactic antibiotic administration was graded as ideal if antibiotics were given within one hour of incision, re-dosed when two antibiotic half-lives had passed, re-dosed intraoperatively if greater than one blood volume had been lost, and if the antibioitc covered anaerobes when a bowel injury was present. Patients were characterized as having no infection, a minor SSI only, an infection related to laparotomy, or an unrelated infection such as pneumonia.
Results: A total of 119 patients underwent exploratory laparotomy for trauma during the time period. Of these patients, 50.4% suffered a postoperative infection, while 49.6% did not; 31% had infections directly related to laparotomy (25% major related infection, 6% minor SSI), and 19% had unrelated infections. Only 53 patients (45%) met criteria for ideal prophylactic antibiotic administration; infections were significantly less common in these patients (see Table). Infections were also more common in the 24 patients (20%) who underwent delayed fascial closure, with 54% developing a related infection (p<0.001) and 83% developing any infection (p<0.001).
Prophylactic Antibiotics and Infections Following Trauma Laparotomy
Related Infection
Unrelated Infection
Ideal Prophylactic Antibiotic Administration:
Yes
No
p Value
Yes
No
p Value
Met Criteria
10
43
<0.001
20
33
<0.001
Didn't Meet Criteria
27
39
40
26
Conclusions: Ideal administration of prophylactic antibiotics is associated with decreased infectious complications following exploratory laparotomy for trauma. Development of protocols ensuring such administration could potentially benefit future trauma patients.
ZaborinAlexanderPolozovAlexanderFirestoneMillicentZaborinaOlgaAlverdyJohn
The University of Chicago
SYNTHESIS AND EFFICACY OF A NOVEL PHOSPHATE-RICH PEG COMPOUND (PHOSPHO-PEG) WITH ANTI-VIRULENCE ACTIVITY AGAINST MULTIPLE-ANTIBIOTIC-RESISTANT PATHOGENS
Background: We have previously demonstrated that hospital pathogens that cause lethal gut-derived sepsis are triggered to express a lethal phenotype when they sense local phosphate (Pi) depletion. However, maintaining local phosphate in the distal gut will require a special phosphate delivery vehicle.
Hypothesis: The aims of the present study were to synthesize and test the efficacy of a novel phosphorylated polyethelene glycol co-polymer (Pi-PEG15–20) to prevent lethal gut-derived sepsis against a broad range of antibiotic-resistant pathogens.
Methods: Terminal phosphorylation of PEG15–20 was performed with phosphorus oxychloride, and Pi-PEG15–20 was tested for prevention of microbial virulence/lethal phenotype in multiple pathogens using C. elegans as a surrogate host. Transmission electron microscopy (TEM) of C. elegans intestinal tube examined microbial adhesion.
Results: Pi-PEG15–20 significantly protected against C. elegans mortality due to highly aggressive pathogens including C. albicans, P. aeruginosa, Serratia marcescens, K. oxytoca and E. faecalis (n=75/group, p<0.001). Microscopic analysis demonstrated that Pi-PEG15–20 prevented accumulation of microbes in the worm intestine, attenuated intestinal distension, and maintained a protective mucus layer between intestinal tube microvili and bacteria (see Figure). Importantly, Pi-PEG did not affect microbial growth but highly suppressed virulence expression as judged by its effect on phosphate signaling protein PstS, pyocyanin, and pyoverdin production (n=3, p<0.001).
TEM of intestinal tube of C. elegans feeding on P. aeruginosa (P.a.) without (A) or with (B) 5%Pi-PEG15–20. In the presence of Pi-PEG, ordered and intact microvili are seen with preservation of a protective layer (glycocalyx) distancing bacteria from microvili.
Conclusions: Exploiting phosphate signaling mechanisms in pathogens relevant to the surgical patient with Pi-PEG may be a non-microbicidal, anti-virulence strategy to prevent gut-derived sepsis without altering the intestinal microbiota.
TanejaMayankPurtillJamesRothmanRichardAustinMattParviziJavad
Rothman Institute at Thomas Jefferson University Hospital
CAN SURGICAL SITE INFECTION AFTER JOINT ARTHROPLASTY BE REDUCED?
Background: Surgical site infection (SSI) following total joint arthroplasty (TJA) is a devastating complication with immense psychological and economic burden for the patient and the healthcare provider. Due to the presence of foreign material (prosthesis), eradication of SSI in this patient population is challenging and numerous strategies have been adopted to prevent this complication.
Hypothesis: We hypothesize that a majority of contaminations of the surgical site, leading to subsequent infection, occur during draping, and that repeat skin antisepsis prior to application of incise draping will reduce the incidence of SSI.
Methods: This randomized, single-blind, prospective study recruited 600 patients undergoing TJA between March 2010 and November 2011 at a single center. 537 subjects qualified for analysis by completing the first postoperative visit. The control group had standard preparation of skin with chlorhexidine (preoperative shower), alcohol and povidone-iodine (intraoperative skin preparation). Incise draping (Ioban™) was applied once the skin was dry. The experimental group had the same skin preparation but after draping and prior to application of the incise drape, a combination of iodine povacrylex (iodophor)/alcohol (DuraPrep™) was applied to the skin. All variables such as perioperative antibiotics, operating room environment, and postoperative wound management were the same in both groups.
Results: The use of an additional skin preparation prior to application of incise draping significantly reduced the incidence of SSI in patients undergoing TJA. The cumulative incidence of superficial incisional SSI at 0.7% (2/269) in the experimental group was significantly lower than the incidence of superficial incisional SSI at 3.3% (9/268) in the control group (p<0.036; relative risk, 0.21; 95% confidence interval, 0.02 to 1.05). Additionally, the observed incidence of skin blistering was lower in the experimental group at 3.3% (9/269) versus 5.9% (16/268) in the control group (p=0.15).
Conclusions: It appears that repeat skin antisepsis after draping and prior to application of incise draping does lead to a significant (nearly five-fold) reduction in superficial incisional SSI. We believe the beneficial effect of repeat skin antisepsis results in removing contaminating organisms that gain access to the surgical site during draping. The reduction in skin blistering that was observed could also be the result of a reduction of contaminating organisms remaining on the skin after draping.
YazjiIbrahimChhinderSodhiAfraziAminGoodMistyNealMatthewJiaHongpengLinJoyceBrancaMariaGrantZacharyMaCongrongPrindleThomasHackamDavid
University of Pittsburgh
ENDOTHELIAL TLR4 SIGNALING IS RESPONSIBLE FOR INTESTINAL ISCHEMIA IN THE PATHOGENESIS OF NECROTIZING ENTEROCOLITIS VIA ITS EFFECT ON THE EXPRESSION OF MICROVASCULAR TONE REGULATORS: eNOS AND ENDOTHELIN-1
Background: Necrotizing enterocolitis (NEC) is the leading cause of GI-related death in premature infants; its etiology remains unexplained. Our lab has shown that TLR4 signaling is fundamental to the pathogenesis of NEC. Previous research has focused on epithelial TLR4 signaling; however, NEC is a disease of early ischemia and tissue necrosis.
Hypothesis: We now hypothesize that TLR4 signaling in intestinal microvascular endothelial cells is responsible for gut ischemia associated with NEC and is a necessary component in the pathogenesis of this deadly disease.
Methods: NEC was induced in newborn wild-type (WT), and endothelial-TLR4-deficient mice (endo-TLR4-/-) through a combination of formula gavage and hypoxia, and the extent of NEC development was assessed via histology, mucosal cytokines, and enterocyte apoptosis. To study intestinal blood flow, mice received intra-cardiac injections of fluorescent Tomato Lectin 5 minutes prior to death and 3D-blood flow remodeling was performed. Expression of microvascular-tone regulatory genes: eNOS, which produces NO, as well as the potent vasoconstrictor endothelin-1 (ET1), were also assessed.
Results: Endo-TLR4-/- mice were protected from NEC. There was little change in iNOS expression of endo-TLR4-/- mice compared to a several-fold increase in WT NEC animals. This correlated with a 75% decrease in intestinal villus perfusion of WT NEC vs. insignificant change in perfusion of the endo-TLR4-/- animals subjected to the same stress. In addition, there was a significant increase in intestinal apoptosis and decrease in proliferation of the WT NEC group, both of which were absent in the endo-TLR4-/- group. Induction of TLR4 signaling via IP LPS injections in both newborns and adults replicated to a large extent the results of the NEC experiment. Intestinal ischemia of the WT NEC group was associated with 40% decrease in eNOS expression and 27% increase in ET1 expression, contributing to the ischemic conditions associated with NEC. Endo-TLR4-/- animals challenged with NEC-type stress or LPS-TLR4 stimulation did not change expression of eNOS and ET1 expression.
Conclusions: This work demonstrates a novel role for TLR4 signaling in regulating microvascular tone. Endothelial TLR4 signaling in the gut downregulates eNOS and upregulates ET1, leading to intestinal ischemia as seen in NEC.
EvansHeatherYetisgen-YildizMelihaBejanCosminWarnerKeirBlackRobertMaierRonaldWurfelMark
University of Washington
CHEST X-RAY REPORT LANGUAGE IS INCONGRUOUS WITH QUANTITATIVE CULTURE RESULTS IN VENTILATOR-ASSOCIATED PNEUMONIA
Background: The chest X-ray is a key element of the definition of ventilator-associated pneumonia (VAP). As part of the development of a natural language processing (NLP) classifier, we aimed to determine the value of information from chest X-ray reports (CXRR), distinct from the chest X-ray itself.
Hypothesis: Manual annotation will uncover the association between CXRR language and bronchoalveolar lavage (BAL) culture results in a group of patients with clinical suspicion for VAP.
Methods: Using a dataset derived from all trauma patients ventilated for >48 hours in a level 1 trauma center between 2007–2010, we extracted CXRR from the day prior, day of, and day after BAL from the electronic medical records of those patients who underwent BAL for the purpose of VAP diagnosis. We defined a coding guideline using the chest X-ray element of the clinical pulmonary infection score (no infiltrate, diffuse infiltrate or atelectasis, focal infiltrate) and a three-point scale for suspicion of pneumonia (no suspicion, suspicion, probable pneumonia). Baseline characteristics and outcomes of the patients were compared by BAL result with univariate analysis. CXRR content was compared by BAL outcome.
Results: A total of 828 CXRR, derived from 344 patients, were annotated, 409 (49.4%) from 199 patients diagnosed with VAP on the basis of positive BAL culture (pBAL). VAP and non-VAP patients were similar in injury severity, hospital stay, and mortality, except men had a higher rate of pBAL than negative BAL (169 [84.9%] vs. 110 [75.9%], p=0.03). CXRR with content revealing any suspicion of pneumonia were more often associated with pBAL than negative BAL (191 [46.7%] vs. 160 [38.2%], p=0.0139). Though not significant, “localized infiltrate” was more common in CXRR from pBAL than negative BAL patients (56 [13.7%] vs. 36 [8.6%]); “no infiltrate” was less often described (46 [11.2%] vs. 54 [12.9%]), as was “diffuse infiltrate or atelectasis” (307 [75.1%] vs. 329 [78.5%] p=0.06). “No infiltrate” was noted concurrently with “no suspicion” without exception. Despite pBAL results, 218 CXRR contained no phraseology suggestive of pneumonia.
Conclusions: We discovered an association with CXRR language and VAP diagnosis, but also found clinicians opted for BAL testing in patients without evidence of VAP suspicion or infiltrate on CXRR. We intend to use NLP to further assess the predictive value of CXRR data in a comprehensive algorithm for risk assessment of VAP.
HauserCarlSursalTolhaItagakiKiyoshiKurosawaShinichiroStearns-KurosawaDebby
Beth Israel Deaconess Medical Center/Harvard Medical School
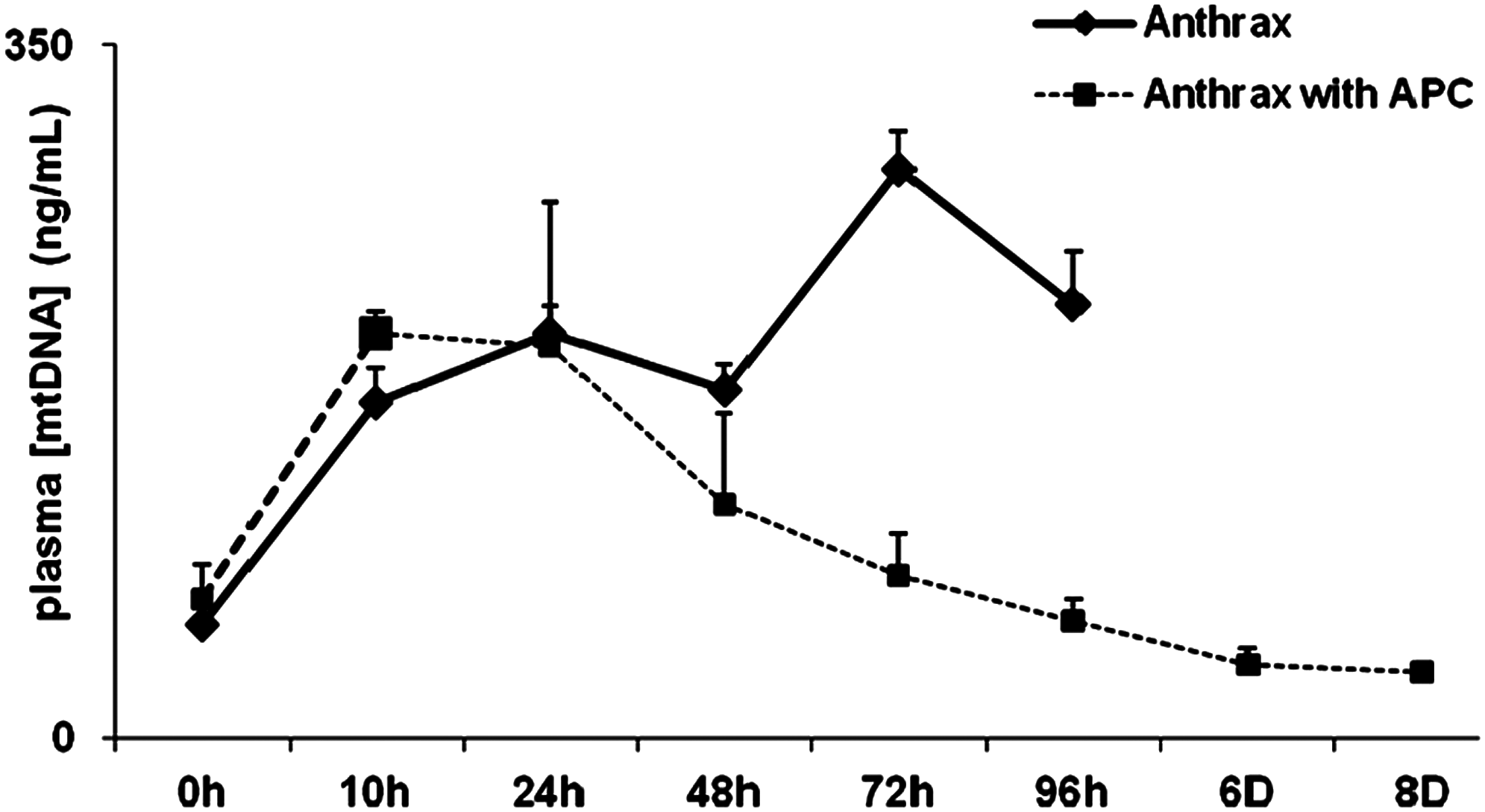
BACTERIAL AND MITOCHONDRIAL DNA ASSAYS DISTINGUISH SEPSIS FROM SYSTEMIC INFLAMMATORY RESPONSE SYNDROME (SIRS) IN PRIMATES
Background: Differentiation of sepsis from SIRS is difficult in clinical practice. No current test differentiates SIRS due to sterile tissue injury from sepsis completely.
Hypothesis: Plasma mitochondrial DNA (mtDNA) reflects cell damage, appearing in plasma after injury and activating innate immunity. Bacterial 16sDNA (bDNA) reflects infection by pathogens and also activates innate immunity. Measurements of damage- and pathogen-associated molecular patterns (DAMPs, PAMPs) may allow categorization of inflammatory syndromes according to origin.
Methods: Baboons were given 1) Shiga Toxin-1 (ST1) to create lethal, sterile injury (n=3); 2) sublethal E. coli infusion (EC) to model infection (n=3); and 3) infusion of non-toxigenic anthrax (ATX) followed by ciprofloxacin (ABX) to model lethal sepsis. Group 3 was pre-treated with activated Protein C (aPC, n=4) or vehicle (n=4) to assess the role of innate immunity. Quantitative plasma bDNA, mtDNA, blood cultures (BC) and multiple organ failure (MOF) markers were assessed serially.
Results: With ATX infusion, BC and bDNA peaked, becoming negative after ABX. bDNA was detected longer. After non-lethal EC infusion, bDNA and mtDNA fall immediately. ST1 toxicity causes increasing mtDNA up to death without bDNA detection. After ATX without aPC, mtDNA increases until death. With aPC rescue, mtDNA decays after bacteremia and animals survive. MOF markers are related to mtDNA rather than bDNA concentration.
Conclusions: mtDNA and bDNA biomarkers detect bacteremia and distinguish sterile from infective tissue injury in primates. The data support a global classification of innate immune "DANGER" responses into 1) sterile responses to endogenous DAMPs (SIRS); 2) responses to pathogens without self-perpetuating associated tissue injury (INFECTION); and 3) responses to pathogens with tissue injury that sustains SIRS (SEPSIS). In treated sepsis the endogenous SIRS response rather than the initial septic insult likely drives MOF and determines outcome.
Plasma mtDNA demonstrates cell damage due to bacteremia. After bacteremia, tissue injury persists without rescue by aPC, showing its dependence on innate immunity.
MurphyClaireHaJoo HyunCookCharlesStevensonKurt
The Ohio State University
MULTI-DRUG RESISTANCE DOES NOT INFLUENCE MORTALITY IN CRITICALLY ILL PATIENTS WITH ACINETOBACTER INFECTIONS
Background: Acinetobacter has emerged as a leading cause of infection among critically ill patients. The incidence of multi-drug resistance (MDR) has also increased, limiting treatment options. This retrospective study aimed to identify predictors of mortality in critically ill patients with Acinetobacter infections.
Hypothesis: MDR Acinetobacter is associated with an increased risk of mortality.
Methods: Patients admitted to an intensive care unit (ICU) between January 2006 and December 2009 were eligible for evaluation. Patients with an Acinetobacter positive culture and associated clinical symptoms were included. A multivariable logistic regression analysis was performed to identify independent predictors of mortality.
Results: One hundred fifty six patients were evaluated with a mortality rate of 34.6%. Baseline characteristics including age and history of MDR organisms were similar between survivors and non-survivors. Non-survivors had higher APACHE II scores (22.3 vs. 19.5, p=0.02), and were more likely to be surgical patients (50 vs. 33.3%, p=0.04) and immunosuppressed (33.3 vs. 16.7%, p=0.02). MDR Acinetobacter rates were similar between survivors and non-survivors (63.7 vs. 70.4%, p=0.404). Non-survivors had a higher incidence of Acinetobacter bacteremia compared to survivors (38.9 vs. 5.9%, p<0.001). Although there were no differences in rates of adequate empiric coverage, survivors were more likely to receive a carbapenem as empiric therapy (33.3 vs. 16.7%, p=0.027). In the multivariable analysis (Table), predictors of mortality included immunosuppression, higher APACHE II score, and bacteremia. Use of a carbapenem for empiric therapy exhibited a survival benefit.
Adjusted Odds Ratio (95% Confidence Interval)
p-value
Immunosuppressed state
2.76 (1.05–7.27)
0.04
APACHE II
1.1 (1.04–1.17)
0.002
Bacteremia
14.1 (4.34–45.82)
<0.001
Carbapenem as empiric therapy
0.29 (0.11–0.76)
0.012
SICU admission was included but had a p-value>0.05.
Hosmer and Lemeshow Goodness-of-fit test p=0.906.
Conclusions: Although multi-drug resistance is presumed to delay appropriate therapy and increase mortality, this study found no correlation between resistance and mortality. Predictors of mortality included immunosuppression, higher severity of illness, and bacteremia. Use of a carbapenem for empiric therapy should be considered in ICU patients thought to be at risk for Acinetobacter.
LeungChung HoWangFengAilenbergMenachemVadaszBrianLilesConradCaldaroneChristopherRotsteinOri
Hospital for Sick Children, Toronto
REMOTE ISCHEMIC PRECONDITIONING PREVENTS LUNG AND LIVER INJURY FOLLOWING HEMORRHAGIC SHOCK/RESUSCITATION
Background: Hemorrhagic shock and resuscitation (S/R) contributes to the development of organ dysfunction including liver injury and lung edema. Previous studies have demonstrated that antecedent remote ischemic preconditioning (RIPC) prevents ischemia/reperfusion injury in a number of organ-specific models.
Hypothesis: We hypothesized that RIPC could exert multi-organ protection in a model of global ischemia/reperfusion.
Methods: RIPC was accomplished by subjecting male C57BL/6 mice to occlusion of the right femoral artery for 10 min and reperfusion for 10 min. Sham mice underwent groin dissection but without femoral artery occlusion. Shock was initiated by blood withdrawal from the left carotid artery and maintained at a systolic BP of 35 mm Hg for one hour followed by resuscitation with normal saline infusion. Liver injury was assessed by serum alanine aminotransferase (ALT) and tumor necrosis factor (TNF)α levels, and histological analysis. Lung injury was assessed by alveolar protein leakage from the bronchoalveolar lavage fluid (BALF). Alveolar macrophage phenotype in the lung was identified by flow cytometry using CD206 as a marker of anti-inflammatory M2 macrophages in the BALF.
Results: S/R markedly increased serum ALT and TNFα levels in sham mice; however, these increases were substantially prevented in RIPC mice. Furthermore, hepatocyte ballooning and hemorrhage in the liver was significantly reduced in RIPC mice compared with sham mice. In the lung, RIPC prevented the increase in alveolar protein that was observed in sham mice. S/R markedly reduced the anti-inflammatory M2 macrophage population in the lung—an effect that persisted for 2 hours after resuscitation in sham mice. However, the M2 macrophages returned to the initial levels prior to shock in RIPC mice.
Conclusions: RIPC exerts a potent protective effect on multi-organ dysfunction in a model of S/R injury. Protection correlates with the reduction of inflammation in the liver, and the preservation of the M2 macrophage phenotype in the lung. RIPC represents a potential clinical intervention to prevent S/R-associated organ injury in the surgical setting.
The data represent the mean and SEM of 3–4 mice/group at t=1 hour of resuscitation for ALT and TNFα, and at t=2 hour for BALF. *p<0.05 vs. S/R.
ShoganBenjaminOlivasAndreaTrimbleWilliamGilbertJackZaborinaOlgaAlverdyJohn
The University of Chicago
CUES PRESENT AT ANASTOMOTIC LEAK SITES INDUCE A STABLE mexT MUTATION IN PSEUDOMONAS AERUGINOSA CAUSING ENHANCED TISSUE DESTROYING CAPACITY
Background: Intestinal anastomotic leak is a feared complication. We have shown that rats subjected to preoperative radiation followed by a colon resection develop high anastomotic leak rates (>70%) only when colonized by P. aeruginosa. We also have shown that P. aeruginosa recovered from a leaking anastomosis undergo in vivo transformation to a stable tissue-disrupting phenotype capable of collagen breakdown and destruction of epithelial cells.
Hypothesis: In this study we performed deep sequencing of the inoculating and transformed strains to better understand the genetic basis of this virulent transformation.
Methods: Rats received pelvic radiation, a 1 cm distal colon resection, anastomosis, and cecal inoculation with stock strain P. aeruginosa (P1). On postoperative day 6, the rats were euthanized and the anastomosis was excised. Transformed P. aeruginosa (P2) was isolated from anastomotic tissue by culture on selective media. Both strains were phenotyped for pyocyanin production, swarming, and collagenase activity. Genomic DNA was isolated, sequenced, and complete reconstruction was performed.
Results: Compared to the inoculating strain P1, the P2 strain demonstrated significantly increased production of pyocyanin, enhanced collagenase activity, and extreme flagella-mediated swarming motility. The P1 and P2 strains demonstrated identical genomes with the exception of a single nucleotide mutation in the transcription factor mexT (C→A, 2807731 NC002516 genome). P1 mexT is predicted to encode a full-length 304-aa MexT protein, whereas the mutation in P2 leads to a stop codon limiting the protein product to a presumed 44-aa non-functional truncated protein. As MexT is a known antibiotic efflux pump activator, we confirmed these findings by showing that resistance to chloramphenicol was >20-fold higher in P1 compared to P2 (p<0.05). Next, we replaced mexT in the P2 strain with mexT from the P1 strain. The mexT-replaced P2 strain lost its ability to swarm, was attenuated in collagen destruction, and expressed pyocyanin production similar to P1, confirming the role of mutated MexT in the observed hypervirulent phenotype transformation.
Conclusions: P. aeruginosa found at leaking anastomotic sites expresses a genetic mutation in MexT that encodes a phenotype capable of extreme intestinal tissue destruction. This may have important implications in the pathogenesis of anastomotic leak.
HeneghanAaronPierreJosephKudskKenneth
University of Wisconsin, Madison
INTERLEUKIN (IL)-25 IMPROVES INNATE AND ACQUIRED IMMUNITY DURING PARENTERAL NUTRITION
Background: Parenteral nutrition (PN) increases infections in critically injured patients. PN impairs acquired immunity by reducing secretory IgA (sIgA) production and transport. Recently, PN was found to reduce a Paneth cell antimicrobial molecule, secretory phospholipase A2 (sPLA2), and the goblet cell glycoprotein MUC-2 in intestinal secretions, causing depression of innate mucosal immunity. IL-4 regulates sIgA while the Th2 cytokines IL-4 and IL-13 regulate sPLA2 and MUC-2 through the IL-13 receptor.
Hypothesis: Since IL-4 and IL-13 are mediated by IL-25 and since PN reduces luminal sPLA2, MUC-2, and sIgA, we hypothesized that IL-25+PN would restore luminal acquired and innate immunity.
Methods: 2 days after IV cannulation, randomized male ICR mice received chow (n=12), PN (n=9), or PN+0.7 mcg of exogenous IL-25 (n=11) daily for 5 days. Small intestine wash fluid (SIWF) was collected for analysis of sPLA2 activity, MUC-2 relative density, sIgA, and luminal levels of IL-4 and IL-13. Changes to the intestinal goblet and Paneth cells were analyzed using histology.
Results: PN reduced luminal sPLA2 compared with chow (p<0.0001). IL-25 increased sPLA2 to chow levels (p<0.0001). PN reduced luminal MUC-2 compared to chow (p<0.002). IL-25 increased MUC-2 levels (p<0.02) compared to PN. Luminal cytokine levels decreased with PN compared to chow (IL-4: p<0.0001) (IL-13: p<0.002). IL-25 increased both cytokines compared to PN (IL-4: p<0.03) (IL-13: p<0.02).
Conclusions: PN impairs innate mucosal immunity by suppressing luminal sPLA2 activity compared to chow, but exogenous IL-25 reverses this dysfunction. PN decreases the density of MUC-2 in the lumen compared to chow, which is also reversible with IL-25. Hypertrophy of goblet and Paneth cells occurred following IL-25 stimulation, consistent with increased sPLA2 and MUC-2. PN decreases adaptive mucosal immunity via sIgA compared to chow, while IL-25 improves sIgA but not to chow levels. These data show PN with lack of enteral feeding impairs multiple aspects of innate and adaptive mucosal immunity, which is reversed by exogenous IL-25.
Chow
PN
PN+IL-25
Intestinal sPLA2 (FL/μL/min)
7811±466
1895±418A
5955±825
Luminal IL-4 (pg/mL)
183.1±11.9
119.3±8.1A
146.4±8.7B
Luminal IL-13 (pg/mL)
15.3±1.8
8.1±1.1A
13.9±1.6
Luminal MUC-2 (relative density)
75912±6182
50366±4059A
65448±4626
Luminal slgA (pg/mL)
398.1±39.5
163.4±24.2A
281.4±29.7B
A, p<0.05 vs. chow and PN+IL-25; B, p<0.05 vs. chow.
YoungPangPedryczBarbaraLucykxValerieCompstonCatharineLukowskiChrisMuellerThomasKhadarooRachel
University of Alberta
ONCOSTATIN M (OSM) RECEPTOR DEFICIENCY PROVIDES A SURVIVAL ADVANTAGE IN A SEPTIC SHOCK MODEL
Background: Sepsis is a significant contributor to mortality and morbidity in inpatient populations worldwide. There is a significant cost associated with the potential complications associated with sepsis. Despite improvements in goal-direct therapy of sepsis and septic shock, there remains a high mortality rate (17–42%). The morbidity and mortality associated with sepsis is related to progression from local injury to multiple organ dysfunction. Elucidating the pathophysiology of sepsis is critical to developing new diagnostic and therapeutic modalities. OSM is a 28 kDa glycoprotein that is part of the IL-6 family of cytokines. Activation of the OSM receptor (OSMR) results primarily in activation of the JAK/STAT pathway. The primary biological functions of OSM/OSMR are in regulation of inflammation. Levels of OSM have been previously shown to increase in septic patients. However, the role and mechanism of OSM/OSMR in sepsis has been poorly elucidated.
Hypothesis: Signaling through the OSM/OSMR is critical in mediating local and distant inflammation in sepsis.
Methods: This study examined wild-type (WT) and OSMR knockout (OSMR-/-) C57BL/6 in a cecal ligation and puncture (CLP) model of sepsis. The experiment used a standardized protocol with CLP using 18- and 25-gauge needles. Mice were observed for 24 hours prior to collection of serum and tissue samples. Serum cytokine levels were measured using a multiplex detection system. Further tissue analysis was conducted with PCR, ELISA, Western blots, and histologic analysis.
Results: WT and OSMR-/- were examined using a CLP model of sepsis. Measurement of OSMR by PCR showed increased expression in lung, heart, and kidney, in proportion to the size of cecal puncture, and correlating with the degree of sepsis. Mortality was significantly higher in WT mice (42%) compared to OSMR-/- (0%) at 24 hours post-CLP. Serum cytokine levels were measured, which demonstrated that in OSMR-/- mice, there was a significant suppression of IL-6 (41,355 pg/mL vs. 790 pg/mL) and IL-10 levels (4,791 pg/mL vs. 1,293 pg/mL).
Conclusions: Activation of the OSM/OSMR axis is important to stimulation of local and systemic inflammation in a CLP model of sepsis. Deficiency of OSMR is protective in our CLP model of sepsis in mice. This can potentially influence future therapeutics models for sepsis, by targeting the OSM/OSMR axis.
YangWeng-LangQiangXialoingMatsuoShingoDongWeifengNicastroJeffreyCoppaGeneWangPing
Hofstra North Shore-LIJ School of Medicine
NEUROTRANSMITTERS MODULATE EXPRESSION AND RELEASE OF COLD-INDUCIBLE RNA-BINDING PROTEIN (CIRP), A PRO-INFLAMMATORY MEDIATOR, IN MACROPHAGES
Background: Accumulated evidence indicates a cross-talk between autonomic nervous system (ANS) and the immune system in controlling inflammation. ANS is subdivided into the sympathetic (SNS) and parasympathetic nervous system (PNS). During infection, SNS is activated to release mainly norepinephrine (NE) for binding adrenergic receptors. Meanwhile, PNS activity is inhibited, resulting in a decrease of acetylcholine (ACh) to activate nicotinic cholinergic receptors (nAChR). We have identified that extracellular CIRP stimulates proi-nflammatory responses. CIRP is a nuclear protein and functions as an RNA chaperone to facilitate translation.
Hypothesis: Neurotransmitters NE and ACh have direct activity in controlling CIRP expression and release in macrophages.
Methods: Rats were subjected to sepsis by cecal ligation and puncture (CLP). Blood and liver tissue were collected after CLP. Primary peritoneal macrophages from rats were treated with LPS (10 ng/mL), NE (20 nM), and nicotine (100 μM) for 6 or 24 h. RAW 264.7 macrophages were transfected with green fluorescence protein (GFP)-CIRP plasmid and monitored under fluorescent microscopy. CIRP protein and mRNA levels were measured by Western blotting and real time PCR, respectively. Cell viability was determined by MTS assay.
Results: In rat serum, CIRP protein levels increased 3.4-fold at 20 h after CLP. The levels of CIRP mRNA and protein in the liver were increased by 4.0- and 2.4-fold, respectively. LPS and NE increased CIRP mRNA levels at 6 h by 5.9- and 10.1-fold, respectively, and intracellular CIRP protein levels at 24 h by 2.1- and 2.0-fold, respectively, in peritoneal macrophages. CIRP was detected in cultured media of LPS- and NE-treated macrophages at 6 h. In contrast, nicotine, a nAChR agonist, inhibited LPS-induced CIRP expression and release. LPS, NE, and nicotine did not affect cell viability, indicating that CIRP release was not through passive necrosis. Green fluorescence was only observed in the nucleus of RAW cells transfected with GFP-CIRP, while it could be detected in both nucleus and cytoplasm after exposure to LPS.
Conclusions: CIRP levels increase in serum and the liver of septic rats. Expression and release of CIRP regulated by neurotransmitters in macrophages shows a novel route of the influence of the nervous system on inflammatory responses.
HowellGinaCollageRichardLoughranPatriciaZhangXianghongRosengartMatthew
University of Pittsburgh
AGE AND AUTOPHAGY IN SEPSIS-INDUCED ACUTE KIDNEY INJURY: A ROLE FOR THE CALCIUM/CALMODULIN-DEPENDENT PROTEIN KINASES
Background: Sepsis is a leading cause of acute kidney injury (AKI), and advanced age increases both the risk of AKI, as well as the likelihood of non-recovery. Autophagy is a critical adaptive response to sepsis and may be cytoprotective in the context of AKI. Induction of autophagy is in part a calcium-dependent process; we have demonstrated that calcium signaling via the calcium/calmodulin-dependent protein kinases (CaMKs) is fundamental for autophagy in immune cells. However, both autophagy and CaMK expression are attenuated with age.
Hypothesis: We hypothesize that age-related decline in CaMK signaling contributes to the reduction in autophagy, and thus, worsened renal recovery in response to sepsis.
Methods: Aged (>45 weeks) or young (8–10 weeks) mice were subjected to LPS (1.5 mg/kg IP) or saline injection. After 48 hours, blood and organs were harvested. Autophagy was assessed by immunoblot and immunofluorescence utilizing anti-LC3B antibody. Morphological differences in the appearance of mitochondria and autophagic structures was detected with electron microscopy (EM). CaMKIV expression was assessed by immunoblot against anti-CaMKIV antibody. Renal function was quantified by assaying serum blood urea nitrogen (BUN) and cystatin.
Results: Aged mice exhibited less autophagy in the kidney in response to LPS as evidenced by less LC3B expression and visualization of fewer autophagic structures by EM. Furthermore, aged mice demonstrated evidence of decreased CaMKIV expression and worsened mitochondrial damage as compared to young mice after LPS administration. This attenuation in autophagy and CaMKIV expression, along with worsened mitochondrial damage, correlated with persistently elevated BUN (124 vs. 27 mg/dL, p<0.001) and cystatin (1,188 vs. 529, p=0.003) concentrations in the aged versus the young mice.
Conclusions: These results support the notion that the loss of CaMK expression with age may contribute to the attenuation of autophagy observed in older individuals, thus inhibiting renal recovery in response to a septic insult. The mechanisms will become increasingly important to characterize as the population ages and the incidence of septic AKI continues to rise.
GaleStephenCoyleSusetteCalvanoStevenCorbettSiobhanLowryStephen F.
Robert Wood Johnson Medical School/University of Medicine and Dentistry of New Jersey
THE APOLIPOPROTEIN E (ApoE) 4 ISOFORM IS ASSOCIATED WITH AN INCREASED INFLAMMATORY RESPONSE IN HUMANS AFTER IN VIVO ENDOTOXIN CHALLENGE
Background: After injury or infection, most patients experience self-limited inflammation; yet others develop hyperinflammation (SIRS/sepsis), worsening morbidity and mortality. Efforts increasingly focus on identifying genetic polymorphisms that may help predict these discrepant outcomes. ApoE, a multifunctional protein with metabolic and immunomodulatory activity, exists as 3 isoforms (ApoE2, E3, or E4) in humans based on allelic inheritance. ApoE3 is most common and has anti-inflammatory properties. The less common ApoE4 is associated with certain inflammatory conditions including Alzheimer disease and cardiovascular disease. Also, animal and human observational studies suggest that ApoE4 is associated with hyperinflammation.
Hypothesis: Healthy human volunteers possessing the ApoE4 allele will demonstrate a greater inflammatory response after in vivo endotoxin challenge than subjects with other isoforms.
Methods: Thirty-six otherwise healthy volunteers were given intravenous endotoxin (2ng/kg) to induce moderate systemic inflammation. Vital signs and blood samples were obtained at various times post-challenge. Plasma TNFα concentrations were assessed by sandwich ELISA. DNA was extracted from the leukocytes at baseline and ApoE isoforms were determined by direct sequencing. Results were analyzed using unpaired t-test.
Results: Of 36 volunteer samples examined, 8 expressed the ApoE4 allele (ApoE4+). Compared to ApoE4- subjects, those ApoE4+ experienced a greater rise in TNFα (p<0.01) and in body temperature (p<0.02) after endotoxin challenge. From the same cohort, 19 subjects were homozygous for the ApoE3 allele (ApoE3/ApoE3); 17 had other allele combinations. The ApoE3 homozygotes had lower TNFα levels (p<0.02) and a lower temperature curve (p<0.02) after endotoxin challenge than all other (AO) subjects either homozygous or heterozygous for ApoE2 or ApoE4.
Conclusions: The ApoE4 allele is associated with a greater inflammatory response after in vivo endotoxin challenge. Subjects homozygous for ApoE3 experienced a less robust inflammatory response after endotoxin challenge when compared to those who are homozygous or heterozygous for ApoE2 or ApoE4. ApoE polymorphism may contribute to differing responses to injury or infection. Genetic testing for ApoE isoforms may help predict which patients will develop hyperinflammation and progress to SIRS or sepsis after injury or infection.
ThompsonJeremyEckertMatthewDortchMarcusPouliotJonathonNorrisPatrickBoczkoErikMayAddison
Vanderbilt University
THE BURDEN OF UNNECESSARY EMPIRIC ANTIBIOTIC THERAPY IN SUSPECTED VENTILATOR-ASSOCIATED PNEUMONIA
Background: Empiric broad-spectrum antibiotics (AB) for suspected ventilator-associated pneumonia (VAP), with aggressive de-escalation based upon quantitative cultures, has been shown to reduce VAP morbidity and mortality. However, AB exposure is associated with an increased risk of subsequent infection and infection with resistant pathogens. This unnecessary exposure has not been well quantified.
Hypothesis: Empiric AB regimens designed to cover common VAP pathogens result in unnecessary AB exposure while inadequately covering some pathogens until standard culture and sensitivity data returns.
Methods: To assess appropriate AB coverage and quantify unnecessary exposure, retrospective review was performed of all mechanically surgical ICU patients from 2005 to 2010 who underwent bronchoscopy-directed bronchoalveolar lavage (BAL) for suspected VAP. Quantitative cultures were considered positive if ≥10,000 cfu/mL. Appropriateness of empiric AB therapy was defined as pathogen sensitivity to at least 1 empiric agent based on final cultures. Unnecessary exposure was defined as exposure to AB not required for therapy and quantified as the sum of AB days for each agent.
Results: 64% of 435 BAL results were negative. Of the 140 positive BALs with available susceptibility data, 86% (121) had all identified pathogens treated appropriately; 2 patients were thought to have inadequate suspicion of VAP and did not receive empiric AB; in 17 patients (12% of patients receiving empiric therapy), the AB did not cover all pathogens. The majority of uncovered infections (11 of 17) were due to pan-resistant Acinetobacter. Of the 279 negative BAL cultures, 56 % (156) received empiric AB at the time of BAL, while the remaining 44% were receiving three-agent therapy for another infection prior to the BAL. The 156 patients who began empiric coverage at the time of the (negative) BAL received 8.6 AB days/patient of unnecessary AB, totaling 1,342 unnecessary AB days.
Conclusions: Broad-spectrum empiric AB coverage for VAP results in significant unnecessary exposure while still inadequately covering some patients. In this patient population, 1,342 unnecessary AB days was provided yet 12% of pathogens remained uncovered. The current strategies contribute significant unnecessary costs and likely contribute to AB resistance. These data strongly support the development of tools that can more rapidly identify pathogens in VAP.
DeBuskGeorgeStephenAndrewMonaghanSeanConnollyMichaelGreggSheaAdamsCharlesCioffiWilliamHeffernanDaithi
Brown University
RE-DEFINING THE CLINICAL PULMONARY INFECTION SCORE (CPIS) FOR TRAUMA PATIENTS
Background: The CPIS is often used either as the definitive test, or as a trigger to obtaining microbiological samples for definitive diagnosis of ventilator-associated pneumonia (VAP) in trauma patients. Many features of the CPIS are common to both worsening infection as well as progression of the traumatic injury. Indeed, CPIS has been considered futile in trauma patients given the heavy reliance upon progressive radiographic findings and the subjective findings of quality of secretions. We therefore undertook an analysis of the individual components of the CPIS score in trauma patients with and without microbiologically proved VAP.
Hypothesis: Oxygenation, as denoted by PaO2:FiO2 ratio, will be most useful in distinguishing progression of critical illness versus pneumonia.
Methods: A retrospective review of all trauma patients who developed VAP over a 3-year period. A CPIS score of ≥5 was used as a trigger to consider undertaking bronchoalveolar lavage (BAL). Pneumonia was diagnosed if the BAL yielded a growth of >10,000cfu/mL (BALpos). If the growth was <10,000cfu/mL then patients were deemed BALneg. Charts were reviewed to assess each feature of the CPIS. Each component of the CPIS was compared between BALpos and BALneg patients.
Results: 138 patients underwent BAL. 117 (84%) were BALpos. All patients had a CPIS score ≥5. There was no difference between BALpos and BALneg patients with respect to mean age (44.9 vs. 44.3 yrs; p=0.85), male gender (78% vs. 81%; p=0.70), average CPIS (7.17 vs. 6.86; p=0.5), or purulent secretions (27% vs. 36%; p=0.80). BALneg patients had no difference in localized pattern on chest X-ray (CXR) (55% vs. 41%; p=0.25) but were more likely to have progression of CXR findings (77% vs. 47%; p=0.037). All patients had either fever or leukocytosis. BALneg patients were less likely to be febrile (64% vs. 84%; p=0.039) and significantly less likely to have an abnormal PaO2:FiO2 (64% vs. 94%; p=0.0004).
Conclusions: The CPIS score remains a much-utilized tool to guide clinical consideration of VAP. However, many features remain common to intubated trauma patients with and without VAP. The PaO2:FiO2 was markedly different between BALpos and BALneg patients. We propose re-defining the application of CPIS. Greater caution must be applied to progressive radiographic findings or a normal PaO2:FiO2 when utilizing CPIS to diagnose VAP in trauma patients.
SwobodaSandraLipsettPamela
The Johns Hopkins University
DO NARCOTICS HAVE AN IMPACT ON THE IRESENCE OF PSEUDOMONAS INFECTIONS IN THE SURGICAL INTENSIVE CARE UNIT (SICU)?
Background: Morphine is a known immunosuppressant whose activity is associated with impaired bacterial clearance and enhanced susceptibility to infectious organisms. The virulence of enteric Pseudomonas aeuriginosa (PSAE) has been influenced by morphine in vitro by transforming the phenotype to one with mucus suppression, barrier disruption, and lethality. Clinical use of morphine has been linked to increased susceptibility and morbidity in burn patients. Little is known regarding critically ill patients (SICU) receiving narcotics.
Hypothesis: To examine the effect of narcotic administration and the development of virulent PSAE intra-abdominal infections in SICU patients.
Methods: This was a retrospective case-control study. From 2004–2007 SICU patients with an intra-abdominal infection with PSAE were identified. Patients were matched 1:1 with non-PSAE infected controls (CON) for every case (PSAE) as follows: Calendar year, age (within 10 years), ICU time to culture, gender, source. Narcotic doses were converted to fentanyl equivalents. Analysis included chi-square, t-test and MLR as appropriate. Data are presented as mean (SD), or median (IQR 25%−75%, p<0.05).
Results: Patients were well matched: Median age was 56 (range 20–86), APACHE II was 26 points (7,11) with no significant differences in gender, race, diseases such as hypertension, cirrhosis, diabetes, dialysis, immunosuppression, transplantation, malignant disease or in ICU days to positive culture. Case patients were in the hospital longer (but not the ICU) prior to positive culture, with mean hospital days to culture 27 vs. 13 (p=0.01). In the PSAE group the median cumulative dose of narcotic pre-culture was 5,792 mcg (510, 40,568) vs. 1,275 mcg (0, 13,375) (p=.007). The median number of days of narcotic exposure pre-infection was significant (PSAE 12 days (5–31) vs. CON 2 (0–8) days) (p=0.01). There were no differences in hospital or SICU mortality, or antibiotic days pre-culture (p=0.47). All patients received multiple anti-infective agents.
Conclusions: Through careful matching, our study examines patients who develop post-operative peritoneal infections (PSAE vs. non-PSAE) and the role of narcotic exposure on the presence of PSAE infections. Due to low power in this cohort, we are uncertain of the specific impact of the narcotic; whether it is the time of exposure, total amount of narcotic, or a combination of both. Further, it is unclear if the class of narcotic has a role in PSAE infections in SICU patients.
BihoracAzraBaslantiTezcan OzrazgatCuencaAlexEfronPhilipMaierRonaldMoldawerLyle
University of Florida
ACUTE KIDNEY INJURY (AKI) IS ASSOCIATED WITH EARLY CYTOKINE DYSREGULATION AFTER TRAUMA
Background: Nosocomial infections (NCI) are a common and costly complication after trauma. AKI occurs in 26% of trauma patients and is associated with increased mortality. Previous studies have suggested that patients with AKI have an exaggerated pro-inflammatory response as measured by circulating cytokine levels.
Hypothesis: AKI patients who develop NCI will exhibit cytokine dysregulation compared to AKI patients who do not develop NCI.
Methods: A secondary analysis of the “Inflammation and the Host Response to Injury” database was explored to include adult blunt trauma patients who had available plasma cytokine analyses. AKI was defined by the RIFLE classification, which requires a 50% increase in serum creatinine concentrations. Association between AKI, NCI, and plasma cytokines was analyzed using a mixed model analysis.
Results: Among 147 patients, NCI occurred in 72% and 51% for patients with and without AKI, respectively. Patients with AKI had significantly higher plasma concentration of pro-inflammatory cytokines (IL-1ra, IL-6, IL-8, and MCP-1) compared to patients without AKI, as measured in the first 12 hours of injury. However, patients with AKI who developed NCI demonstrated a trend toward lower pro-inflammatory cytokines IL-1ra and IL-6 and higher anti-inflammatory IL-4 and IL-10 at 12, 24, and 48–120 hour time periods after injury. This change in response was most prominent among patients with AKI and NCI who died, as compared to those who survived. In a mixed model analysis adjusted for age, gender, race, and ISS scores, AKI, NCI, and initial (<12 hours) cytokine concentrations were independently associated with a change in cytokine levels over time.
Conclusions: Post-traumatic AKI may be associated with increased risk of NCI and death after trauma, which may be secondary to an altered early inflammatory response.
Longitudinal changes in median cytokine concentration in AKI patients.
HoVanessaMcWhorterPeterJohnsonJeffreyEachempatiSoumitraShouJianBariePhilip S.
Weill Cornell Medical College
PROCALCITONIN CONCENTRATION (PCT) IS ASSOCIATED WITH SEVERITY OF SEPSIS IN CRITICALLY ILL SURGICAL PATIENTS (CRISPS)
Background: Procalcitonin (PCT) is a biochemical marker that has stimulated interest for its potential ability to differentiate sepsis from non-infectious causes of systemic inflammatory response syndrome. It is unknown whether PCT can differentiate severity of sepsis in a population of CrISPs.
Hypothesis: PCT correlates with severity of sepsis in CrISPs, and the degree of PCT elevation varies by source of sepsis. Secondarily, PCT on admission to the surgical intensive care unit (SICU) would have prognostic value and be associated with mortality.
Methods: 244 consecutive SICU patient admissions were studied. Age, diagnosis, presence/severity of sepsis upon admission, source of infection, and in-hospital mortality were collected; PCT was drawn upon admission. Sepsis severity was stratified as sepsis (SEP), severe sepsis (SVS), and septic shock (SSH). Source of infection was grouped as blood stream, intra-abdominal, respiratory, skin/soft tissue, or urologic. Nonparametric rank-sum tests assessed differences between groups, α=0.05.
Results: Of 244 patients admitted, 45 had sepsis (1 with SEP, 35 with SVS, 9 with SSH); of these, 23 patients had intra-abdominal infection. 213 had PCT drawn; the 1 patient with SEP did not. PCT (mean±SD) (Table) was significantly different for varying severity of sepsis: 0.64±2.40 for patients without sepsis, 11.93±19.19 for SVS, and 18.20±13.62 for SSH, p=0.001. PCT was not different between groups based on sepsis source (p=0.79). Mean PCT for survivors was 2.83±9.58, vs. 7.06±12.45 for non-survivors, p=0.007.
By Kruskal-Wallis equality of populations rank test. bBy two-sample Wilcoxon rank-sum test.
Conclusions: In CrISPs, PCT correlates with severity of sepsis and mortality. This rapid diagnostic test can be a useful aid for early diagnosis, treatment, and prognostication of surgical patients with sepsis.
BanerjeeAmanKellyKatherineZhouHannahDixonShanteriaClaridgeJeffrey
Case Western Reserve University
DIAGNOSIS OF INFECTION AFTER TRAUMA SPLENECTOMY: IT'S ABOUT THE LACK OF PLATELETS AND NOT THE WHITE BLOOD CELL COUNT
Background: There is a lack of evidence-based criteria to assist with diagnosing infection in patients s/p trauma splenectomy (TS). The literature suggests that white blood cell count (WBC) is associated with infection in TS patients.
Hypothesis: There exist key differences in laboratory and clinical parameters that can help diagnose infection s/p TS.
Methods: All consecutive trauma patients s/p TS at a Level 1 trauma center from 2005 to 2011 were evaluated for the development of infection. Demographic, laboratory, and clinical parameters on odd postoperative days (POD) 1 through 15 were compared between infected and non-infected patients. Backward stepwise logistic regression was used to identify significant independent predictors of infection.
Results: 127 patients had a TS; 25 patients died within 48 hours leaving 102 cases for analysis. The mean day for the first infectious episode in the 41 patients who developed an infection was POD 7 (range 4–14). In the 41 patients who developed infection, the three most common infections were pneumonia (51%), urinary tract infection (24%) and bacteremia (20%). An evaluation of laboratory and clinical parameters demonstrated no differences in WBC between groups at any time. The table below summarizes some key significant differences. Over the 15 days analyzed, POD 5 was most strongly associated with different laboratory and clinical differences between infected and non-infected patients. Independent predictors of infection were platelet count on POD 5 (OR=0.99; 95% CI=0.989–0.999, p=0.029) and maximal temperature on POD 5 (OR=4.1; 95% CI=1.44–11.85, p=0.008). The C statistic was 0.83.
Conclusions: The most significant parameters for prediction of infection after TS are Tmax on POD 5 and a platelet count that rises at approximately one-half the rate of non-infected patients. WBC and Injury Severity Score were not predictive. Serial clinical and laboratory data over time may allow for improved diagnosis of infection.
Clinical Parameter
Non-infected (n=61)
Infected (n=41)
p-value
Injury Severity Score (ISS)
23
33
0.000
Platelet Count POD3
245
154
0.000
Platelet Count POD5
349
224
0.003
Platelet Count POD7
607
317
0.000
Platelet: WBC Ratio POD5
22.0
14.9
0.005
Maximum Temperature (Tmax) POD5
37.5
38.3
0.000
Peak Heart Rate POD5
103
116
0.001
Maximum Systolic POD5
139
154
0.007
CastleShannonWangLarryGrishinAnatolyFordHenriFreyMark
Children's Hospital Los Angeles
NEUREGULIN-4 PROTECTS INTESTINAL CELLS FROM NEC-INDUCING BACTERIA BY REDUCED APOPTOSIS WITHOUT PROMOTION OF CELL RESTITUTION
Background: In human and murine colitis models, expression of the ErbB4 receptor tyrosine kinase is elevated. Furthermore, ErbB4 expression inhibits cytokine-induced apoptosis in cultured colon epithelial cells, suggesting a protective role in the intestine. However, the role of ErbB4 in NEC is unknown.
Hypothesis: In this study we used in vitro and in vivo models to test the hypothesis that ErbB4 activation protects against experimental NEC and to elucidate the mechanism by which ErbB4 protects against bacteria-induced intestinal damage.
Methods: Newborn rat pups were formula-fed (FF), FF with the ErbB4-specific ligand neuregulin-4 (NRG4), or breast-fed (BF). FF and NRG4 groups were gavage-fed and stressed with hypoxia and hypothermia, with or without 100 ng/pup NRG4 per feed. Animals were euthanized upon the development of severe disease and ileum was collected. IEC-6 rat ileal epithelial cells were treated with 108 cfu/mL Cronobacter sakazakii (CS) and 100 ng/mL of ErbB4 ligands heregulin-1 or NRG4, with or without treatment with the Src-kinase inhibitor PP2 (2.5 μM). Apoptosis was assessed by luminescent caspase activity assay and by Western blot of cell lysates for cleaved caspase levels. Cellular restitution was assayed by creating standard wounds on confluent cell monolayers and measuring wound size 8 hours after treatment with CS and ErbB ligands.
Results: Immunofluorescence analysis showed increased ErbB4 expression with experimental NEC in rats. Development of NEC was delayed in pups treated with NRG4, with 89% surviving to 36 hours, compared to 55% of the FF group. Kaplan-Meier analysis showed a significant survival advantage (p=0.039) for NRG4-treated animals. In vitro, the ErbB4 ligands heregulin and NRG4 reduced bacteria-induced apoptosis by 31+/-1.0% and 45+/-5.6%, respectively (p=<0.001). Src inhibition by PP2 reduced NRG4 protection (p=0.03). Cell restitution in the presence of NRG4 was not significant compared to wound healing in control groups.
Conclusions: NRG4, a ligand specific for ErbB4, is protective against early development of NEC in a neonatal rat model and against bacteria-induced apoptosis in vitro. Src kinase inhibition reverses the protective effect of NRG4 in vitro and thus is a possible signaling pathway by which ErbB4 activation protects against NEC. ErbB4, then, may represent a highly selective therapeutic target to prevent or attenuate human NEC.
KanaanZiadBarnettRebeccaGardnerSarahPeytonJimCheadleWilliam
University of Louisville
DYSREGULATION OF miR-142-3p, -146, -299, AND-200c DOWNREGULATES HMGB1 AND INDUCES MICROBIAL TOLERANCE IN A NOVEL MODEL OF CHRONIC PERITONITIS
Background: We observed persistent peritoneal bacteria despite a transient early innate immune response to intra-peritoneal (IP) Klebsiella pneumoniae. Pretreatment with lipopolysaccharide (LPS) prior to peritonitis induced microbial tolerance in our murine model of chronic peritonitis. MicroRNAs (miRNA)s are potential regulators of inflammatory cytokines/alarmins and could explain microbial tolerance.
Hypothesis: We hypothesized that miRNA dysregulation could downregulate HMGB1, a key alarmin, and induce microbial tolerance.
Methods: 24 hours after pretreatment with IP LPS (0.01 mg/g) or saline, C57BL/6 mice were given 103 colony forming units of K. pneumoniae IP. Gentamicin was given 4 hours prior to infection and BID thereafter. Peritoneal exudate cells (PEC)s were obtained through peritoneal lavage and total RNA was isolated (n=3) at 4, 24, and 48 hours following infection. TNF-α, IL-1β, IL-6, and HMGB1 levels were detected using ELISA. miRNA expression levels were detected using SA Biosciences mouse immune-pathology RT2 miRNA PCR array (MAM-104A). Messenger-RNA (mRNA) detection was done using SA Biosciences RT2 Profiler PCR array mouse Toll-like receptor signaling pathway (PAMM_018A). Data were analyzed by Ingenuity Pathway Inc. analysis (IPA). Student t-tests were used to determine significance of fold changes.
Results: When compared to the saline group, TNF-α, IL-1β, and IL-6 were down-regulated at 4, 24, and 48 hours in the LPS group. miR-142-3p, -146, -299, and -200c were up-regulated at all time points in the LPS group (p<0.05). HMGB1, a common target for all these miRNAs, was correspondingly down-regulated at both the mRNA and protein level (Table).
4 hours
24 hours
48 hours
Fold regulation of significantly dysregulated microRNAs in the LPS group at 4, 24, and 48 hours as compared to the saline group. (p<0.05)
miR-142-3p
6.0
3.3
3.2
miR-146
2.1
3.2
2.8
miR-200c
3.2
2.8
2.9
miR-299
3.2
2.8
2.9
Fold regulation of common target for all above microRNAs (p<0.05)
HMGBI mRNA
−1.5
−1.2
−1.1
Saline Pretreated Group
75±2
58±10
84±8
HMGBI protein levels (pg/mouse)
LPS Pretreated Group
52±5
51±4
57±3
Conclusions: A tolerant pattern of pro-inflammatory cytokine protein production was observed after LPS pretreatment, as evidenced by decreased levels of pro-inflammatory cytokines. miR-142-3p, −146, −299, and-200c seem to play a key role in inducing tolerance by down-regulating both mRNA and protein HMGB1 levels in the LPS- pretreated group.
YosephBenyam (ben)BreedEliseLiangZheFoxAmyO'DonnellDaveDunneMichaelMcConnellKevinCoopersmithCraig
Emory University School of Medicine
COMMENSAL BACTERIA PLAY A PROTECTIVE ROLE IN MEDIATING MORTALITY FROM PNEUMONIA-INDUCED SEPSIS
Background: The human intestine contains over 100 trillion bacteria, which are essential for health maintenance. However, their role in critical illness is relatively unknown.
Hypothesis: The aim of this study was to assess the impact of intestinal flora in sepsis by comparing germ-free (GF) mice that lack commensal bacteria with conventional (CONV) mice that have a complex indigenous intestinal flora.
Methods: C57Bl/6 GF mice received intra-tracheal P. aeruginosa (3×105 CFU or 3×106 CFU) and CONV mice received 3×106 CFU of the same bacteria. Mice were sacrificed 7 days or 24 h after injection. Gut apoptosis was quantified by both H&E and caspase-3 staining, villus length was measured by measuring depth from crypt neck to villus tip, proliferation was quantified using BrdU, and permeability was measured in vivo to FD4. Blood and BAL levels of TNF, IL-6, IL-10, IL-1β, IL-13 and IFN-γ were evaluated via ELISA.
Results: Septic GF mice had a significantly higher mortality than septic CONV mice (100% vs. 56%, p=0.001) given the same dose of P. aeruginosa. When a 10-fold dilution of bacteria was injected in GF mice, CONV and GF mice had similar mortality (63% vs. 56%, p=ns, n=15–17/group). Further analysis was performed in mice with matched survival to eliminate the confounder of differential mortality in mice given the same dose of bacteria. GF mice had significantly lower levels of TNF and IL-1β in BAL fluid, as well as a trend towards lower levels of all cytokines measured except IFN-γ. No differences were noted in blood cytokine levels. Since the intestine has been hypothesized to be the “motor” of SIRS, intestinal integrity was also assayed. GF mice had longer villi (p=0.002) and decreased intestinal epithelial apoptosis by both H&E (p=0.02) and active caspase-3 staining (p=0.04). However, there was no difference in gut proliferation or permeability.
Conclusions: Germ-free mice that lack commensal bacteria are more susceptible to sepsis than CONV mice at the same dose of P. aeruginosa pneumonia. Differences between GF and CONV mice suggest the gut microflora may play a beneficial role in sepsis via modulation of pro-inflammatory BAL cytokines and gut integrity.
OttingerMaryMonaghanSeanGravensteinStefanCioffiWilliamAyalaAlfredHeffernanDaithi
Brown University
A DAMPENED INFLAMMATORY RESPONSE IN CRITICALLY ILL GERIATRIC PATIENTS IS ESSENTIAL TO SURVIVAL
Background: A robust inflammatory response, leading to end-organ dysfunction, often drives morbidity and mortality following critical illness. Geriatric patients are particularly susceptible to the effects of profound inflammation. Geriatric patients have baseline age-related decline in the inflammatory and immune systems, and are known to display a lowered inflammatory response to many non-critical disease processes. However, there is a paucity of literature pertaining to the specific inflammatory components among critically ill geriatric patients, and how the inflammatory profile affects mortality.
Hypothesis: Critically ill geriatric patients with an inflammatory response comparable to young patients will have increased mortality compared with geriatric patients who display a dampened response.
Methods: Critically ill surgical and trauma ICU patients were prospectively enrolled. Geriatric patients were defined as those aged 65 years and older. Young patients were defined as those aged 18 to 50 years. Blood was drawn within 72 hours of presentation to the intensive care unit (ICU), to measure circulating cytokines including IL-6 (pg/mL), IL-10( pg/mL) and TNF-alpha (pg/mL). Charts were reviewed for age, gender, APACHE II score, and outcome.
Results: 21 young (mean age 38 yrs) and 32 geriatric (mean age 76 yrs) critically ill patients were recruited. Geriatric patients were comparable to young patients in male gender (56% vs, 71%; p=0.38) and age-adjusted APACHE II score (12.5 vs. 13.5; p=0.70) but did have higher mortality (44% vs. 9.5%; p=0.001). Geriatric patients who died compared with those who lived had significantly elevated IL-6 (420 vs.111; p=0.001) and IL-10 (6.2 vs 3.1; p=0.002) and decreased TNF-alpha (1.54 vs. 3.19; p=0.01) levels. IL-6 (420 vs .295; p=0.40) and IL-10 (6.2 vs. 8.2; p=0.20) levels were not significantly different between geriatric patients who died compared with young patients who lived. However, geriatric patients who lived, compared with young patients who lived, had significantly lower IL-6 (110 vs. 295; p=0.01) and IL-10 (3.0 vs. 8.2; p=0.02). There was no such relation noted with TNF-alpha.
Conclusions: The inflammatory response to critical illness often influences outcomes. Geriatric patients who exhibit an inflammatory response as robust as their younger counterparts have dramatically increased mortality. Understanding this response may help future therapy to modulate inflammation, thereby improving mortality.
LopezNicoleEliceiriBrianPotenzaBruceBairdAndrewCoimbraRaul
University of California, San Diego
CHANGES IN LEUKOCYTE EXPRESSION OF ECRG4 FOLLOWING BURNS: AN IMMUNOSURVEILLANCE MARKER?
Background: The candidate tumor suppressor gene Ecrg4 encodes a secreted precursor protein that is tethered to the cell surface but processed and released after cell activation. Moreover, the membrane-anchored form of Ecrg4 is constitutively expressed at high levels on the surface of quiescent polymorphonuclear cells (PMNs) and monocytes, suggesting that it plays a sentinel role in monitoring homeostasis. Indeed, it is rapidly processed and shed from the leukocyte cell surface upon cell activation.
Hypothesis: We hypothesized that the disruption of homeostasis that accompanies severe burn injury (>30% TBSA) in man would mimic the effects of cell activation observed in vitro and in animal models of injury, and result in a temporal changes in the cell surface expression of Ecrg4 in leukocytes.
Methods: Flow cytometry was used to detect cell surface Ecrg4 protein expression on leukocytes from healthy volunteers. This was then compared to the same analysis on burn patients with >30% TBSA. Leukocytes from burn patients were tested weekly over the course of hospitalization. Additionally, patient multi-organ dysfunction scores (MODS) were determined on each day of leukocyte analysis. Linear regression was then used to assess to the relationship between leukocyte surface Ecrg4 expression and MODS.
Results: In the analysis of leukocytes from healthy volunteers we observed robust Ecrg4 surface expression. Conversely, in burn patients with >30% TBSA, we observed a decrease in cell surface Ecrg4, which over the course of recovery was associated with a re-expression of Ecrg4. The Ecrg4 levels on PMNs were shown to correlate with clinical injury scores.
Conclusions: The abundance of cell surface Ecrg4 on leukocytes from healthy subjects combined with the close correlation of cell surface Ecrg4 with MODS in burn patients supports a proposed sentinel function for Ecrg4 in cell homeostasis and highlights its potential use to assess leukocyte recovery from burn injury.
CookKristinSifriZiadBaranskiGreggRameshwarPranelaMohrAliciaLivingstonDavid
University of Medicine and Dentistry of New Jersey-New Jersey Medical School
THE ROLE OF T REGULATORY CELLS IN MESENCHYMAL STROMAL CELL (MSC)-MEDIATED WOUND HEALING
Background: MSCs home to the site of lung injury and accelerate healing from 7 to 5 days. One possible mechanism is through up-regulation of T regulatory cells (Tregs), which have the ability to suppress inflammatory T cells, and thereby may contribute to dysregulated wound healing.
Hypothesis: We hypothesize that MSCs promote healing by recruiting Tregs to suppress inflammation in the lungs.
Methods: Male Sprague-Dawley rats were subjected to unilateral lung contusion (LC) and assigned to two groups: LC or LC+ intravenous MSCs (LC+MSC). 5×106 allogeneic MSCs were injected intravenously 5 minutes after LC. Animals were sacrificed at 24 hrs, 3, 5, and 7 days (N=3–6/group). Peripheral blood (PB) and lung tissue was analyzed by flow cytometry for Tregs. Results are expressed as %CD25+/FoxP3+ of total CD4+ cells±SD. *p<0.01 by ANOVA and Tukey-Kramer.
Results: Following LC, Tregs more than doubled in PB and homogenized lung tissue as compared to UC (Figure). The increase in Tregs peaked at day 5 but decreased toward baseline at day 7 in both lungs and PB. LC+MSC significantly increased Tregs further. Rats injected with MSCs also showed an increase in Tregs at day 5 in both PB and lungs. This 3-fold peak is significantly higher compared to LC alone.
Conclusions: At day five following LC there is a marked increase in Tregs in PB and at the site of injury, indicating that Tregs play a role in the later stages of healing. This process is enhanced following systemic injection of MSCs, which is a novel finding in traumatic wound healing. MSC-mediated enhanced up-regulation of Tregs may contribute to faster wound healing, possibly through suppression of the inflammatory response.
BandyopadhyayGautamBankeyPaulMiller-GrazianoCarol
University of Rochester
INCREASED ELDERLY T CELL CO-INHIBITORY RECEPTOR EXPRESSION & SHP-1 ACTIVATION DEPRESS T CELLS, INCREASING INFECTIONS
Background: Elderly (age 65 years+) trauma patients have increased susceptibility to infections and are the majority of septic patients. Hypo-responsive T cells (Tc) are linked to immunosuppression & increased patient (Pt) infections in trauma & aging. We showed Pt post-trauma Tc depression as correlated to inhibitory receptor triggering of negative signal transduction molecules, particularly the Src homology domain containing phosphatase-1 (SHP-1).
Hypothesis: Increased inhibitory receptor (IR) expressing elderly Tc have increased SHP-1 activation resulting in decreased T cell activation to T cell receptor (TCR) stimulation, since activated SHP-1 can dephosphorylate (inactivate) the signaling molecules needed to activate NFkB (essential T cell activation).
Methods: Freshly isolated T cells from elderly & young (age<35 y), either Pts or controls (Cnt), were stimulated with anti-CD3 to assess Tc proliferation. Tc were assessed for SHP-1-inducing IRs (PD-L1, LAG-3, CD152; flow cytometry). To test if inhibition of hyper-activated SHP-1 can rescue Tc from hypo-responsiveness, control Tc were stimulated through CD47 (SHP-1 activator) in the presence/absence of a SHP-1 inhibitor to determine the effects of SHP-1 on NFkB activation & Tc proliferation.
Results: Elderly Tc from Cnt & Pts showed decreased proliferation to direct TCR stimuli & increased IR expression (CD152, PD-L1, LAG-3 (Table) compared to young Cnt & Pts respectively. Elderly Pts also had higher rates of infectious complications. Elderly Cnt Tc had increased SHP-1 activation vs. young subjects (median MFI 568 vs. 388). A SHP-1 inhibitor rescued CD47-induced Tc depression by restoring TCR-triggered proliferation & NFkB activation.
Elderly T cells from both Cnt & Trauma Pt Express Elevated Co-Inhibitory Receptors. Elderly Pts Experienced Tc Hyporesponsiveness & Higher Infection Rate
Age<35 Cnt
Age<35 Pt
Age 65+Cnt
Age 65+Pt
T cell Proliferation (Median DPM)
58263
51271
30571
18684
Infection rate
-
23%
-
50%
Median CD152
1.7%
2.6%
5.5%
7.2%
Median PD-L1
7.1%
8.2%
13.3%
16.9%
Median Lag-3 MFI
0.3
0.2
5.9
6.2
Conclusions: Increased IR expression and SHP-1 activation characterize Cnt elderly Tc defects and can contribute to increased post-trauma susceptibility to infections.
SternJordanOlivasAndreaShoganBenjaminChristleyScottZaborinaOlgaAlverdyJohnAnGary
The University of Chicago
EVOLUTIONARY DYNAMICS OF ANASTOMOTIC LEAK: INVESTIGATION OF VIRULENT PHENOTYPE SWITCHING IN PSEUDOMONAS AERUGINOSA WITH AN AGENT-BASED MODEL
Background: The pathogenesis of intestinal anastomotic leak involves host-microbe interactions at the site of surgical injury. Host factors may induce phenotypic changes in the microbiota that predispose to anastomotic failure. We have shown that P. aeruginosa can shift to an anastomosis-disrupting phenotype (P2) through mutation of the mexT transcriptional regulator when exposed to an anastomosis in irradiated bowel. This leads to expression of virulence factors on the OprN operon: Swarming and type-III secretion system (TTSS) products. Given the metabolic cost associated with virulence factors, P2 is not normally present.
Hypothesis: We hypothesize that the anastomotic milieu produces evolutionary pressures favoring the high-risk/high-reward P2 phenotype, and used an agent-based model (ABM) to investigate evolutionary dynamics and functional tradeoffs of the P2 shift.
Methods: An ABM was constructed simulating epithelial cells and P. aeruginosa in an in vitro culture. Bacteria had 2 states: P1 (mexT+) and P2 (mexT-). As the mexT locus is highly mutable, each bacterial replication event involved a probability of a switch from P1 to P2. P2 mutants manifested the effects of OprN dis-inhibition-swarming motility and activation of the TTSS, resulting in epithelial cell death, but at a higher metabolic cost. Simulations monitored P1/P2 population dynamics in conditions of non-injured and injured tissue with parameter sweeps across metabolic costs/gains from the P2 virulence functions and mexT mutation rate.
Results: The ABM accurately simulated the spatial distribution of host-microbe interactions. In the non-injured condition, P1 was favored. With injury, P2 was generally favored, but with varying stability of microbial populations depending upon the cost/gain tradeoff levels. Higher-risk/higher-reward populations were more unstable, but could be compensated by high mexT mutation rates.
Conclusions: Cell injury may favor a virulent bacterial phenotype at a healing anastomosis, despite the increased metabolic cost. Evolutionary pressure may explain the observed phenotype transformation of P. aeruginosa. The potential cost of a high-risk/high-reward strategy is reduced by having a high mutation rate, suggesting that this strategy for virulence potential is evolutionarily robust. This implicates environmental interdiction as a viable strategy for antimicrobial therapy.
Munoz-PriceL. SylviaClearyTimothyFajardo-AquinoYovanitDePascaleDenniseCoroGabrielNamiasNicholas
University of Miami
REDUCTION IN ACINETOBACTER INFECTIONS ASSOCIATED WITH REDUCTION OF ENVIRONMENTAL CONTAMINATION OF A TRAUMA/BURN INTENSIVE CARE UNIT (ICU)
Background: Acinetobacter has become one of the preeminent pathogens in ICUs worldwide. One of the peculiarities of this organism is its ability to resist desiccation, surviving in dry environments for months. Furthermore, the hospital environment is now a proven reservoir of multidrug-resistant organisms, in particular Acinetobacter.
Hypothesis: We aimed to determine the percentage of contamination with Acinetobacter of inanimate surfaces, and to correlate this rate with new acquisitions of Acinetobacter infections.
Methods: This study was performed the 25 bed Trauma/Burn ICU of a 1,500 bed hospital. The ICU was cultured weekly from 3/17/2011 to 9/13/2011. Rooms were selected by the microbiology technologist and Infection Control personnel in order to get rooms with and without Acinetobacter-positive patients. Bedrails, bedside tables, intravenous pumps, and ventilator control panels were cultured using double rayon swabs. Swabs were immediately placed on 2 mL tryptic soy broth and incubated overnight at 37C. Broths showing growth were streaked on blood and MacConkey agar. After 48 hours of incubation at 37C, any visible colonies were sub-cultured and identified by the clinical microbiology laboratory identification system. New acquisitions of Acinetobacter infections were then reviewed with respect to degree of environmental contamination.
Results: A total of 213 rooms were cultured over 15 weeks. 57 (26.7%) were found positive for Acinetobacter spp. 33 (58%) of these rooms had an Acinetobacter-positive patient, and 24 rooms (42%) did not have Acinetobacter-positive patients. Out of the 57 positive rooms, sites found to be Acinetobacter-positive included: 38 bedrails (67%), 21 intravenous pumps (37%), 6 bedside tables (11%), and 3 ventilator control panels (5%). As environmental services was informed and intensified its efforts, contamination decreased, and the number of new acquisitions of Acinetobacter decreased concomitantly from 1.40 patients per week to 0.37.
Conclusions: Acinetobacter was found in the hospital environment of 26.7% of rooms tested within a Trauma/Burn ICU among Acinetobacter-positive and -negative room occupants. A decrease in the number of acquisitions of Acinetobacter occurred as environmental cleaning efforts were focused as part of a comprehensive infection control program.
FinnertyCelesteGaoHongXiaoWenzhongPrasaiAneshJeschkeMarcGibranNicoleGamelliRichardKleinMatthewArnoldoBrettBakerHenryTompkinsRonaldHerndonDavid
University of Texas Medical Branch/Shriners Hospitals for Children
BURN-INDUCED INFLAMMATORY RESPONSE IN ADIPOSE TISSUE
Background: The response to a major burn injury is characterized by systemic inflammation, hypermetabolism, and immune suppression involving a reprioritization of energy metabolism and protein synthesis, which persists for up to 60 days post-injury.
Hypothesis: A severe burn injury induces alterations in the adipose tissue transcriptome that may be related to subsequent loss of fat tissue.
Methods: Adipose tissue samples from 109 burn patients were harvested from the time of admission until 60 days post injury, and were compared to samples from 45 non-injured control subjects. Total adipose tissue gene expression was analyzed using the Affymetrix U133 plus 2.0 GeneChip™. Clinical data detailing patient course were collected prospectively.
Results: Burn-induced alterations in adipose tissue mRNA abundance were observed in 5,914 genes (false discovery rate <0.05, fold change >1.5, burn vs. control); 2,181 genes were up-regulated while 3,176 genes were down-regulated. Surprisingly, the most significant perturbations in adipose tissue gene expression correlated with pathways central to the inflammatory response. Increased expression of cell surface receptors such as TLR and receptors for cytokines such as IL-18, IL-10, IFNγ, IL-1, and IL-6 correlated with up-regulation of down-stream signaling cascades needed to propagate the signals initiated via these receptors. Expression of genes for MYD88, IRAK, IkB, Jak/STAT, Ras, C/EBP, and MEK1/2 were significantly induced by burn injury. Apparent activation was demonstrated via up-regulation of cytokine, adipokine, and collagenase genes necessary for wound healing, immune cell recruitment, inflammation, and tissue repair.
Conclusions: We identified alterations in adipose tissue gene expression that challenge the central dogma that fat tissue is quiescent following a severe burn injury. Rather, we demonstrated that this tissue is a significant source of inflammation, and that these stimuli are massively up-regulated during the first 3 weeks post-injury. Identification of these changes provides insights into the initiation and resolution of severe burn injury, and defines possible new targets for treatment strategies that will attenuate post-burn tissue loss.
McWhorterPeterHoVanessaJohnsonJeffreyShouJianEachempatiSoumitraBariePhilip S.
Weill Cornell Medical College
ADMISSION SERUM PROCALCITONIN CONCENTRATION (PCT) DIAGNOSES SEPSIS ACCURATELY IN A SURGICAL INTENSIVE CARE UNIT (SICU) PATIENT POPULATION
Background: PCT is useful in identifying sepsis among certain patients, but sensitivity and specificity depend on the clinical setting. The value of PCT in critically ill surgical or trauma patients is debated; inflammation post-trauma (TR) or post-operative (PO) for operations other than to treat infection may affect the discrimination of PCT. This study determined sensitivity, specificity, and accuracy of PCT for sepsis diagnosis in a SICU.
Hypothesis: Primary: PCT is accurate for diagnosis of sepsis in a SICU. Secondary: Neither TR nor PO inflammatory states correlate with PCT.
Methods: Prospective, observational study of consecutive patients conducted in a tertiary-care, university SICU. PCT was assayed on admission and APACHE II scores were calculated (first 24 h). Demographics noted were: Sepsis/no sepsis, TR/no TR, PO/not PO. Pearson correlations (R) and area under the receiver-operating characteristic curve (AUC) were determined for PCT and sepsis, TR, and PO. Sensitivity analysis determined the value of PCT predictive of sepsis with the greatest accuracy (α=0.05).
Results: Among 213 patients who had PCT obtained, 42 had sepsis upon admission, 87 were TR, and 84 were PO. Among sepsis patients, PCT and APACHE II correlated weakly, R=0.07 (p=0.68). For PCT and sepsis: R=0.52 (p<0.001), AUC=0.909 (Figure). For PCT and TR: R=-0.24 (p=0.004), AUC=0.225. For PCT and PO: R=0.16 (p=0.02), AUC=0.689. Accuracy of PCT was highest at >4.60 ng/mL, with sensitivity, specificity and accuracy of 52.4%, 97.7%, and 88.7%, respectively. Lower values yielded greater sensitivity; higher concentrations yielded greater specificity.
Conclusions: PCT is reliable for diagnosing sepsis in a SICU, but greatest accuracy was observed at a higher concentration than recommended by the manufacturer or the literature (0.09–0.25 ng/mL). Neither PO nor TR correlated with PCT and should not affect the discrimination of sepsis in the SICU population.
HuebingerRyanLiuMing-MeiDowdScotRiveraFernandoBoyntonJohnCareyCurtisHawkinsKennethMinshallChristianWolfStevenMineiJosephBarberRobert
University of Texas-Southwestern
EXAMINATION OF THE BACTERIAL MICROBIOME IN BRONCHOALVEOLAR LAVAGE SAMPLES FROM TRAUMA PATIENTS UTILIZING NEXT-GENERATION SEQUENCING TECHNOLOGY
Background: Recent technological developments have allowed for more efficient detection of the bacterial microbiome. Utilization of this technology has identified a vast array of microbiological diversity, including a large number of previously unidentified bacterial species. Many patients who exhibit the clinical signs of pulmonary infection while intubated fail to demonstrate organisms utilizing traditional culture methods, or the bacteria identified are classified as “normal respiratory tract flora.”
Hypothesis: To examine the microbiome of bronchoalveolar lavage (BAL) samples using next-generation sequencing (NGS) technology, and to determine if it correlates with standard culture methods or outcomes
Methods: BAL samples were collected in the intensive care unit (SICU) as a part of standard care for intubated individuals with CPIS>6. The fluid was sequenced for the 16s region with a Roche 454 titanium FLX sequencer. Sequences were analyzed through a data analysis pipeline to identify each 16s sequence to a taxonomic phyoltype (∼species). The bacterial microbiome of each BAL was compared to the bacteria identified via standard culture methods. Correlations between microbiome taxonomic diversity and clinical outcome were examined by linear regression and Pearson correlation.
Results: Bronchoalveolar lavage samples from 12 subjects were examined by 454 pyrosequencing. Mean ventilator days on when BAL was conducted equaled 4. Number of phylotypes (∼species) in the samples ranged from 15 to 129. Additionally, the number of phyla ranged from 3 to 14 in the samples. There was little correlation between bacteria identified by NGS versus standard culture methods. The same predominant bacterial strain was identified by both culture and sequencing in only one of the 12 samples (8.3%). Correlations between days on ventilator and number of species was significant (r=0.74, p=0.006; r2=0.55).
Conclusions: Increasing diversity of the bacterial microbiome in BAL samples correlates with increased ventilator days. Bacteria identified via standard culture methods and NGS data were not well correlated.
RosenbergerLauraHranjecTjasaMcLeodMatthewPolitanoAmaniSawyerRobert
University of Virginia
MORTALITY ASSOCIATED WITH VENTILATOR-ASSOCIATED PNEUMONIA (VAP) HAS DECREASED OVER TIME
Background: VAP is the most common hospital-acquired infection in the intensive care unit (ICU). Experts suggest little progress has been made in outcomes from sepsis, since several novel interventions have failed.
Hypothesis: We nonetheless hypothesized that mortality following VAP has decreased over time due to general advances in pulmonary critical care.
Methods: All ICU-acquired, CDC-defined VAP episodes were prospectively identified between January 1997 and December 2008. Cases were divided into four time periods (1997–1999, 2000–2002, 2003–2005, 2006–2008) to compare outcomes over time. Chi-square analysis compared categorical variables between groups and a multivariable analysis determined independent predictors of death.
Results: 793 cases of VAP occurred during the study period. Demographics and outcomes are given in the table. The two most commonly isolated organisms were Staphylococcus aureus and Pseudomonas aeruginosa. APACHE II scores were stable over time, while mortality was significantly lower in period 4 when compared to periods 1 and 2 (p=0.004 and 0.009, respectively). The logistic regression model predicting death (c-statistic=0.859) revealed age (OR 1.04, 95% CI 1.02–1.05), APACHE II score (1.09, 1.04–1.13), white blood cell count (1.03, 1.00–1.06), presence of trauma (0.14, 0.09–0.23), transplant recipient (2.17, 1.03–4.60), transfusions (2.44, 1.06–5.63), pulmonary disease (2.21, 1.26–3.89), days of antibiotic therapy (0.97, 0.94–0.99), and treatment in period 4 (2006–2008) as compared to period 1 (1997–1999) (0.45, 0.24–0.85) were independent predictors of death. Treatment in the most recent time period yielded a 55% reduction in risk of death.
Conclusions: Over the last decade the mortality from VAP has decreased, likely due to general advancements in pulmonary critical care rather than any specific interventions. Whether these findings are true for other forms of severe infections deserves further study.
Demographics and Outcomes of VAP
Demographic/Outcome
1997–1999
2000–2002
2003–2005
2006–2008
VAP cases
211
200
190
192
APACHE II score
20.6±0.4
19.7±0.3
19.2±0.4
20.1±0.4
Trauma
133 (63.0)
131 (65.6)
127 (66.8)
140 (72.9)
Pulmonary disease
15 (7.1)
27 (13.5)
30 (15.8)
29 (15.1)
Antibiotic therapy, days
13.4±0.5
14.5±0.6
13.9±0.6
14.0±0.8
Crude mortality
54 (25.6)
49 (24.5)
39 (20.5)
27 (14.1)
Variables either mean±standard error or N (%).
StephenAndrewConnollyMichaelAdamsCharlesMonaghanSeanCioffiWilliamGreggSheaHeffernanDaithi
Brown University
THE DIFFERING MICROBIOLOGIC PROFILE OF VENTILATOR-ASSOCIATED PNEUMONIA (VAP) IN GERIATRIC VERSUS YOUNG TRAUMA PATIENTS
Background: VAP remains a significant risk among trauma patients. Geriatric individuals, the fastest-growing population, present with a unique set of confounders, including co-morbidites, baseline altered immune responses, and prior health care institutional exposure. These may predispose geriatric patients to a microbiological flora different to their younger counterparts. However, there is a paucity of literature pertaining to the microbiological profile of VAP in geriatric trauma patients.
Hypothesis: Geriatric trauma patients display a significantly different microbiological profile of VAP when compared with young patients.
Methods: Retrospective chart review of patients at a Level 1 trauma center with VAP over a 3-year period. Elderly patients were defined as those aged ≥65 years and young patients aged 18–65 years. Pneumonia was diagnosed using bronchoalveolar lavage (BAL) growth of >10,000 cfu/mL Polymicrobial pneumonia was defined as more than one organism with >10,000 cfu/mL. Time to diagnosis of VAP was time from admission to performance of BAL. Time to diagnosis, gram stain, and organism type were then compared between groups.
Results: 131 patients with VAP were included. There were 103 young (mean age 37.2 years) and 28 geriatric patients (mean age 73.1 years). Comparing geriatric to young patients, there was no significant difference in time to occurrence of pneumonia (10.3 vs. 8.5 days, p=0.42), rates of gram-positive (55.3% vs. 42.8%, p=0.28), rates of gram-negative (52.4% vs. 64.3%, p=0.29), rates of polymicrobial pneumonia (25% vs. 32%, p=0.64) and rates of MRSA pneumonia (17.9% vs. 7.8%; p=0.15). There were differences in most common organism type causing VAP between the groups. In geriatric patients, the three most common organisms were Staphylococcus aureus (28.6%), Enterobacter spp. (14.3%), and Pseudomonas (10.7%). In young patients the three most common organisms were S. aureus (48.5%), Haemophilus (20.4%), and Enterobacter spp. (15.5%).
Conclusions: VAP remains a common occurrence in trauma patients. Early appropriate empiric antibiotic coverage is essential to successful treatment. Despite presumed differences in health and underlying immune status geriatric patients display patterns in VAP similar to their younger counterparts. However, the most common causative organisms do differ between geriatric and young trauma patients who develop VAP.
KrpataDavidPauliEricKantersArielleNovitskyYuriRosenMichael
University Hospitals Case Medical Center
DOES NEGATIVE-PRESSURE THERAPY REDUCE SURGICAL SITE INFECTIONS FOLLOWING CONTAMINATED VENTRAL HERNIA REPAIR?
Background: Repair of large ventral hernias in the presence of bacterial contamination has a high rate of surgical site infections (SSI). Recent clinical and laboratory studies suggest that negative-pressure therapy (NPT) on closed surgical incisions may reduce the risk of SSI in high-risk populations.
Hypothesis: We hypothesized that NPT would reduce the risk of SSI in patients undergoing contaminated ventral hernia repair.
Methods: We retrospectively reviewed our prospectively collected database for patients undergoing Grade 3 (potentially contaminated) and Grade 4 (infected) large ventral hernia repairs with or without NPT. Patients with fistulae or undergoing anterior component separation were excluded. All patients underwent primary wound closure. In the NPT group, a vacuum dressing (VAC®, KCI, San Antonio, TX) was placed over the closed midline wound. Primary outcome measure was SSIs at 30 days post-operative.
Results: There were 119 patients identified for evaluation (70 standard wound dressing (SWD), 49 NPT). The groups were similar in age, sex, body mass index, co-morbid conditions (chronic obstructive pulmonary disease, diabetes mellitus, immunosuppressive medications, steroid use, or smoking) or number of prior abdominal operations or herniorrhaphies. The SWD group had a higher American Society of Anesthesiologists (ASA) score than the NPT group (3.0 vs. 2.8, p=0.01). Groups were similar in hernia defect size and operative time. There was no difference in the 30-day SSI rate between the two groups (25.8% SWD vs. 20.4% NPT, p=0.50) or in the distribution of major and minor SSIs (SWD: 6 major/12 minor vs. NPT: 2 major/8 minor, p=0.56). Factors associated with an increased risk of SSI included ASA (p=0.02), BMI (p=0.05), defect area (p<0.01), diabetes mellitus (p=0.01), and OR time (p<0.01).
Conclusions: In this retrospective, non-randomized study, the use of NPT in the setting of closed surgical incisions after potentially contaminated or infected large ventral hernia repair did not reduce the 30-day SSI rate. Although prophylactic NPT has reduced wound morbidity in some surgical populations, it does not appear to offer the same improvement in wound morbidity for high -isk contaminated and potentially contaminated cases of open ventral hernia repair.
MoffettJenniferAwadSamirAvellanedaAndresHicksStephanieSubramanianAnuradhaLiangMike
Baylor College of Medicine
OUTCOMES AND PREDICTORS OF SURGICAL SITE INFECTION (SSI) IN STOMA REVERSAL
Background: SSI is common with stoma reversal (SR).
Hypothesis: Identify predictors and evaluate outcomes of SSI in SR.
Methods: Retrospective review was performed of all SR from January 2005 to February 2011. Patients with SSI and no SSI were compared. Continuous data was compared by Student t-test; categorical data was compared by Fisher exact test or Chi square.
Results: 128 patients underwent SR; 46 (36%) patients had a SSI. Patients with SSI were more likely to have elevated HgA1c (6.5% vs. 5.9%, p=0.02), morbid obesity (BMI 31 kg/m2 vs. 27 kg/m2, p=0.01), thicker subcutaneous fat by CT (3.0 cm vs. 2.4 cm, p=0.03), history of facial dehiscence (15% vs. 4%, p=0.03), prior emergency surgery (74% vs. 55%, p=0.04), a colostomy (57% vs. 30%, p=0.005), an end-ostomy (61% vs. 41%, p=0.04), a midline laparotomy (74% vs. 56%, p=0.05), concurrent incisional hernia repair (24% vs. 9%, p=0.03), and elevated peri-operative glucose (154±6.6 mg/dL vs. 136±4.0 mg/dL, p=0.02). The SSI group had more seromas (17% vs. 4%, p=0.004), fascial dehiscences (15% vs. 2%, p=0.01), ICU admissions (35% vs. 17%, p=0.03), prolonged hospital stays (20 days vs. 9 days, p=0.02), readmission (33% vs. 13%, p=0.01), days to wound closure (91 days vs. 61 days, p=0.02), and re-operations (33% vs. 13%, p=0.01). There was a trend toward hernia formation in patients with SSI (stoma site 23% vs. 40%, p=0.08; midline incision (40% vs. 63%, p=0.16). There was no difference in patient satisfaction or functional status at late follow-up (2–78 months).
Conclusions: We identified five factors that are associated with SSI in patients undergoing SR: (1) complicated surgical history, (2) morbid obesity, (3) poorly controlled diabetes, (4) type of stoma, and (5) operative factors. Patients with none of these risk factors had a 12% SSI rate while patients with five risk factors had a 100% risk of SSI (Figure). Better glucose control, weight loss, laparoscopic end-SR, and interval hernia repair should be considered.
% Risk of SSI based upon risk score
CheadleGeraldCostantiniToddPutnamJamesHagenyAnne-MarieEliceiriBrianCoimbraRaul
University of California, San Diego
CHOLINERGIC SIGNALING IN THE GUT: A NOVEL MECHANISM IN BARRIER PROTECTION THROUGH ACTIVATION OF ENTERIC GLIAL CELLS
Background: Enteric glial cells (EGCs) play an important role in maintaining proper intestinal barrier function. We have shown that vagal nerve stimulation (VNS) increases EGC activation, which is associated with improved gut barrier integrity in an animal model of severe injury. Enteric neurons communicate with EGCs through nicotinic cholinergic signaling, which may represent a pathway by which VNS activates EGCs. This study seeks to further define the mechanism by which VNS prevents intestinal barrier failure following injury.
Hypothesis: We hypothesized that a nicotinic cholinergic agonist would increase EGC activation, resulting in improved intestinal barrier integrity using an in vitro model of intestinal injury.
Methods: Cultured EGCs were exposed to the nicotinic cholinergic agonist nicotine. Glial fibrillary acidic protein (GFAP) expression was measured by immunoblot to determine changes in EGC activation. Caco-2 cells were grown to confluence and incubated alone or in co-culture with EGCs. Cells were stimulated with Cytomix for 24 hours in the presence or absence of nicotine and barrier integrity was assessed by measuring permeability to 4kDa FITC-Dextran.
Results: Stimulation with nicotine resulted in EGC activation as demonstrated by a 3.5-fold increase in GFAP expression. Cytomix stimulation increased permeability in Caco-2 cells cultured alone or with EGCs. Treatment of stimulated Caco-2/EGC co-cultures with nicotine restored permeability levels similar to control (Figure, *p<0.05). Nicotine failed to prevent barrier permeability in Caco-2 cells alone.
Conclusions: Nicotine increased EGC activation and improved intestinal epithelial barrier function in an in vitro model of intestinal injury. The barrier-protective effects of nicotine appear to be mediated by activation of EGCs, as protection was lost on Caco-2 cells cultured alone. Therapies aimed at activating EGCs may have important clinical applications for improving intestinal barrier function in patients after injury.
ZangQunMartinezBobbieMaassDavid
University of Texas Southwestern
SEPSIS-INDUCED CARDIAC MITOCHONDRIAL DEFICIENCY INVOLVES ALTERED MITOCHONDRIAL LOCALIZATION OF TYROSINE KINASE CSRC AND TYROSINE PHOSPHOTASE Shp2
Background: Our previous research demonstrated that sepsis produces mitochondrial defects and increases mitochondrial oxidative stress in the heart.
Hypothesis: This study investigated the possible roles of mitochondria-localized signaling molecules, tyrosine kinase cSrc, and tyrosine phosphatase Shp2 in sepsis-induced cardiac mitochondrial damage using a rat pneumonia-related sepsis model.
Methods: Heart tissues were harvested from SD rats 24 hrs after septic challenge (intratracheal injection of Streptococcus pneumoniae, 4×106 CFU, or vehicle for controls), homogenized, separated into mitochondrial and cytosol fractions. Levels of cSrc and Shp2 were determined by Western blots. Levels of tyrosine phosphorylation of certain major mitochondrial proteins were determined by immunoprecipitation of mitochondrial fractions using anti-phosphotyrosine followed by Western blots using antibodies against mitochondrial structural proteins (porin, matrix cyclophilin D, and cytochrome C) and mitochondrial functional proteins (complex II subunit 30kD and complex I subunit NDUFB8). Mitochondrial complex I activities were measured using the mitochondrial fractions in the presence of recombinant active cSrc or Shp2.
Results: Significant decrease of cSrc and increase of Shp2 in cardiac mitochondria, in parallel with decreased tyrosine phosphorylation levels of mitochondrial structural and functional proteins, were evident 24 hrs after septic challenge. In vitro, active cSrc elevated mitochondrial complex I activities in the mitochondrial fractions isolated from sham and septic animals, whereas the effect of active Shp2 was opposite.
Conclusions: Our data suggest that alteration of mitochondria-localized signaling molecules cSrc and Shp2 constitutes a potential signaling pathway to regulate mitochondrial damage and functional deficiency in the heart during sepsis. (Supported by AHA Beginning-in-Aid Grant 09BGIA2220114.)
KimMosesChristleyScottAlverdyJohnLiuDonaldAnGary
University of Chicago
INVESTIGATING THE DYNAMICS OF BACTERIAL VIRULENCE IN NECROTIZING ENTEROCOLITIS WITH A MULTI-SCALE AGENT-BASED MODEL
Background: Necrotizing enterocolitis (NEC) is a leading gastrointestinal cause of death in neonates. We have used an agent-based model (ABM) to propose that the initial condition in the pathogenesis of NEC is immaturity of neonatal gut epithelial cells (NGEC) to manage oxidative stress (OS), and demonstrated that subsequent activation of NGECs through TLR-4 is necessary to generate the NEC phenotype.
Hypothesis: As no single pathogen has been associated with NEC, we investigate the dynamics of different virulence factors to identify the functional characteristics of potential pathogens.
Methods: An ABM of the neonatal gut was developed to include: NGECs, goblet cells (GC), submucosal cells, blood vessels, and bacteria. Host functions modeled include: cell respiration, apoptosis, tight junction metabolism, inflammation, necrosis, mucus production, and thrombosis. Bacterial virulence factors include: mucinase production, enhanced adherence, and cytotoxic exotoxin. Experiments included parameter sweeps of OS management, enteral feeding, and combinations of bacterial virulence factors. Population phenotypes observed at the end of each experiment were matched to established histological criteria.
Results: The ABM reproduced baseline behavior of nutrient metabolism, OS clearance, and apoptosis or inflammation. Cellular injury patterns emerged from patchy to full-thickness necrosis as OS clearance was decreased. We identified a sequence of bacterial virulence functions in simulations leading to NEC: 1) mucus barrier disruption, 2) increased bacterial adherence, and 3) cytotoxic factors. Interestingly, while leading to the most rapid and severe necrosis, the presence of cytotoxic factors was not necessary for the generation of NEC.
Conclusions: NEC is a complex process of cascading systems failure. Our ABM demonstrates that enteral feeding-induced fragility of NGECs could be propagated to full-thickness necrosis given the identified sequence of mucus depletion followed by bacterial contact. While bacterial production of cytotoxic factors led to aggressive necrosis, this function was not needed to generate the NEC phenotype. Our findings suggest that bacterial populations, irrespective of specific species, with the functional capacity to degrade mucus and increase adherence could be involved in the generation of NEC, while the production of cytotoxic exotoxins likely plays a smaller role in the clinical disease.
BellBrandonGrishinAnatolyFordHenri
Children's Hospital Los Angeles
BACTERIAL DIVERSITY IN FORMULA-FED VS. BREAST-FED RATS AND ITS POSSIBLE ROLE IN SUSCEPTIBILITY TO NECROTIZING ENTEROCOLITIS (NEC)
Background: Colonization of the gut by opportunistic pathogens is believed to be a key risk factor in NEC, a deadly intestinal inflammation in pre-term infants. However, much remains unknown about bacterial species associated with NEC. Exposure to maternal bacteria at birth and throughout breast feeding may be instrumental in the establishment of protective microbiota in the neonates. Conversely, formula feeding may increase the chance of colonization with opportunistic pathogens from the environment.
Hypothesis: Inoculation with normal maternal bacteria provides protection from NEC.
Methods: Timed pregnant rats were purchased from Charles River. Newborn rats were separated from their mothers and formula-fed (FF) once every 8 h. Following each feeding, rats were subjected to hypoxia for 10 minutes at 5% O2. Breast-fed (BF) rats were allowed to nurse with their mothers. On the 4th day of life, rats' terminal ileum was excised and sent for pathological grading. An additional 1 cm intestinal segment was homogenized in 500 μL sterile PBS to extract luminal content. Serially diluted luminal content samples were then plated on blood agar and plates were then incubated at 37°C for 24 h. Bacterial colonies were counted and classified into groups according to appearance. For each colony type, the V6-V8 hypervariable region of the 16S rRNA gene was sequenced and bacterial species identified using the NCBI BLAST algorithm.
Results: There is a significant variation in the microbial composition of breast-fed and formula-fed Charles River rats. Rats subjected to formula feeding and hypoxia showed complete ileal colonization by a single Escherichia coli strain in three separate litters. However, luminal content samples of breast-fed rats showed higher microbial diversity. Bacterial populations of breast-fed rats were predominantly Enterobacteriaceae represented by various strains of Escherichia and Shigella, with occasional presence of Staphylococcus and Cronobacter sakazakii as minor components.
Conclusions: Co-habitation with mothers may promote inoculation of neonatal rats with diverse maternally-derived Enterobacteriaceae, which in turn may play a role in the protective effect of breast feeding.
PierreJosephHeneghanAaronFelicianoRodrigoShanmuganayagamDhanansayanRoenneburgDrewKruegerChristianReedJessKudskKenneth
University of Wisconsin-Madison
ADDITION OF PROANTHOCYANIDINS TO INTRA-GASTRIC ELEMENTAL NUTRITION STIMULATES INTESTINAL GOBLET CELL SIZE AND FUNCTION
Background: Goblet cells (GCs) secrete mucin glycoproteins to protect the intestinal mucosa from bacterial attachment and invasion. Deficient glycoprotein mucin2 (MUC2) results in bacterial colitis. Cytokines IL-4 and IL-13, stimulate GC proliferation and mucin production. Enteral administration of an elemental nutrition (EEN) formula reduces lamina propria Th2 cytokines (IL-4) and impairs gut barrier function compared to chow. Proanthocyanidins (PACs) appear to palliate experimental colitis.
Hypothesis: Since PACs may prevent experimental colitis and our preliminary work demonstrates effects of EEN on GC, we hypothesized that EEN+ PACs would stimulate ileal IL-4 & IL-13, GC size and numbers, and luminal MUC2.
Methods: Male ICR mice were randomized to chow, EEN alone, EEN+ Low (PAC 8 mg/kg BW), EEN+Mid (PAC 50 mg/kg BW), or EEN+High (PAC 100 mg/kg BW) for 5 days (10/group), 2 days after cannulation. Chow mice received saline IG. Ileal tissue was analyzed for IL-4, IL-13, and GC histology using PAS staining with GC calculated per villius and cell size using ImageJ analysis. Intestinal washes were analyzed for MUC2 by Western blot.
Results: EEN reduced IL-4 compared with chow. Compared with EEN, PACs increased IL-4 in Mid and High. ENN reduced IL-13 compared with chow (p=0.08). Mid and High increased IL-13 compared with EEN. EEN reduced GC/villi compared with chow, while all PACs doses increased GC/villi compared with EEN. GC Size decreased non-significantly with EEN compared to chow. All PAC doses increased GC size compared to EEN. EEN and Low decreased luminal MUC2 compared to chow. Mid and High increased luminal MUC2 compared to EEN or Low. (See table below.)
Chow
EEN
EEN+Low
EEN+Mid
EEN+High
Tissue IL-4 (pg/mg Protein)
6.22±1.17
4.48±1.5 A
4.98±2.48 C
5.81±2.23
7.00±1.92 B
Tissue IL-13 (pg/mg Protein)
11.37±4.68
7.54±2.77
10.95±4.36
11.83±3.7 B
13.94±4.72 B
Goblet cells/Villi
9.72±2.12
7.96±0.93 A
9.15±1.13 B, C
9.66±0.93 B
10.3±0.94 B
Goblet cell Size (um2)
10.57±1.03 μm2
9.18±1.60 μm2
12.45±2.27 μm2 B
12.38±2.42 μm2 B
11.81±2.08 μm2 B
Luminal MUC2
251±82
185±65 A, C
164±25 A, C
249±62 B
289±68 B
A, p<0.05 vs. chow; B, p<0.05 vs. EEN; C, p<0.01 vs. High.
Conclusions: PACs stimulate IL-4 & IL-13 levels in the ileum, and increase the number and size of goblet cells compared to enteral administration of an elemental glucose & amino acid solution. Mid- and High-dose PAC improves MUC2 in intestinal washes compared with EEN feeding alone. This work demonstrates that PACs stimulate GC hypertrophy and mucin secretion while normalizing cytokines associated with GC integrity.
Lomas-NeiraJoanneChenYapingHeffernanDaithiAyalaAlfred
Brown University
SHOCK/SEPSIS-INDUCED NEUTROPHIL INFILTRATION AND MORTALITY IS MEDIATED BY ANGIOPOIETIN (ANG)-2
Background: Loss of endothelial cell (EC) barrier function is a major component in the development of acute lung injury (ALI). Increased vascular permeability results in pulmonary edema as well as protein and inflammatory cell infiltrate. EC growth factors Ang-1 and −2, under physiological conditions, maintain vascular homeostasis via tightly regulated competitive interaction with the tyrosine kinase receptor, Tie2, expressed on ECs. When Ang-1/Tie2 binding predominates, vessel integrity and downstream pro-survival and anti-inflammatory signaling are promoted. Alternatively, when Ang-2 prevails, Ang-2/Tie2 plays a role in vascular remodeling and increased vessel permeability. Ang-2 is significantly elevated in plasma from patients with ALI/inflammation and in our hemorrhage/sepsis (Hem/CLP) model of ALI in mice. It has been proposed recently that the relative expression of Ang-1 to Ang-2 determines EC responsiveness. In addition, we have found that blockade of Ang-2 with an Fc fusion-protein Ang-2-specific inhibitor, L1–10 (Amgen), significantly increases survival (35% at Day 8) in our model.
Hypothesis: Based on these data we propose that Ang-2 plays a significant role in the development of ALI in our model.
Methods: To address this, L1–10 was administered (4 mg/kg b.w.) by s.c. injection at 3 different time points during Hem/CLP; immediately following Hem, (just prior to resuscitation) (post Hem); immediately following CLP (24 hours following Hem) (post CLP); or at both post Hem and post CLP. Ang-1 and -2, and MPO were measured in lung tissue homogenates.
Results: L1–10 treatment given at combined post Hem/post CLP time points significantly decreased lung tissue Ang-2 (vs. vehicle) compared to single treatments. Lung tissue MPO activity was significantly reduced in both the combined post Hem/post CLP and the post Hem time point treatments. Since no reduction in Ang-2 was measured in with the post sepsis treatment, the kinetics of Ang-2:Ang-1 in lung tissue homogenates was assessed at 0, 4, 12, 24 hours post Hem. This ratio peaked between 0 and 12 hours and, while still significantly higher than naïve controls, was decreased at 24 hours.
Conclusions: These findings, along with our survival study, demonstrate that Ang-2 release following Hem plays a significant role in shock induced priming for the development of ALI. Funded by SIS Foundation Junior Faculty Fellowship.
SmithAlexandraBrooksNatashaAl-mousawiAhmedFinnertyCelesteJeschkeMarc
Sunnybrook Research Institute
HEPATIC APOPTOSIS AND LIVER DYSFUNCTION POST-BURN IS MEDIATED BY C-JUN N-TERMINAL KINASE-2
Background: The trauma of a severe burn injury induces a hypermetabolic response that increases morbidity and mortality. Previously, our group showed that insulin resistance post-burn injury is associated with endoplasmic reticulum (ER) stress. Evidence suggests that c-jun N-terminal kinase (JNK)-2 may be involved in ER stress-induced apoptosis.
Hypothesis: Here, we hypothesized that JNK2 contributes to the apoptotic response after burn injury downstream of ER stress.
Methods: To test this, we compared JNK2 knockout mice to wild type mice after inducing a 30% total body surface area thermal injury. Animals were sacrificed after 1, 3, and 5 days. Inflammatory cytokines in blood were measured by ELISA. Hepatic ER stress and insulin signaling were assessed by Western blotting, and insulin resistance was measured by a peritoneal glucose tolerance test. Apoptosis in the liver was quantified by TUNEL staining. Liver function was quantified by an aspartate aminotransferase (AST) activity assay.
Results: ER stress increased after burn in both JNK2 and wild type mice, indicating that JNK2 activation is downstream of ER stress. JNK2 knockout did not affect serum inflammatory cytokines; however, the increase in IL-6 mRNA expression was prevented in the knockouts. Serum insulin did not significantly increase in the JNK2 knockouts. On the other hand, insulin signaling (PI3K/Akt pathway) and glucose tolerance tests did not improve in the JNK2 knockouts. As expected, apoptosis in the liver increased after burn injury in wild-type mice but not in JNK2 knockouts. AST activity revealed that liver injury improved more quickly in the JNK2 knockouts.
Conclusions: This study indicates that JNK2 is a central mediator of hepatic apoptosis and liver dysfunction after a severe burn.
DuaneThereseZuoJessicaWolfeLukeBearmanGonzaloStevensMichael
Virginia Commonwealth University
SURGEONS DON'T LISTEN: EVALUATION OF COMPLIANCE WITH ANTIMICROBIAL STEWARDSHIP PROGRAM (ASP) RECOMMENDATIONS
Background: An ASP was started to concurrently guide therapy in an effort to improve use and decrease selective pressure.
Hypothesis: To determine differences in interventions (int) and compliance (comp) to ASP recommendations (recs), based on specific surgical service.
Methods: Prospectively collected ASP data from 1/08 through 5/11 were evaluated to determine number of int required and response to int. Appropriate coverage (AC) recs were provided when organisms were uncovered, there was resistance to the regimen, or the antimicrobials were suboptimal. Selective pressure (SP) recs occurred when there was no indication for therapy, therapy was prolonged, there was unnecessary double coverage, or a narrower spectrum was indicated. Overall results for medical (med) and surgical (surg) services were compared with subsequent analysis based on surgical subspecialty.
Results: There were 2,326 interventions, of which 1,112 were for med and 1,214 were for surg. Recs were as follows: 246 AC med vs. 212 AC surg, and 866 SP med and 1,002 SP surg. Comp with recs were higher for med: AC: 90.7% (223/242) med vs. 82.1% (174/212) surg, p=0.0086; SP: 81.1% (702/866) med vs. 69.5% (696/1,002) surg, p<0.0001.
Conclusions: Surgical services demonstrate poor comp with ASP recs. All are less likely to de-escalate therapy as shown by more SP int. By identifying those services that are noncompliant, ASP can target their educational efforts to improve outcomes. Ideally such efforts would result in less int required, appropriate therapy from the onset, and more aggressive de-escalation of antimicrobials.
Compliance Based on Surgical Subspecialty
AC Comp
SP comp
Overall comp
Burn
1
100%(1/1)
16
84.21%(16/19)
85%
Cardiac
35
85.4%(35/41)
92
60.9%(92/151)
66.2%
General
8
72.7%(8/11)
66
64.7%(66/102)
65.5%
Gyn/Onc
5
83.3%(5/6)
20
80%(20/25)
80.6%
Gyn
0
0%(0/2)
5
50%(5/10)
41.7%
Neurosurg
45
88.24%(45/51)
92
73%(92/126)
77.4%
Ortho
15
83.3%(15/18)
48
77.42%(48/62)
78.8%
ENT
4
100%(4/4)
19
61.29%(19/31)
65.7%
Plastics
3
75%(3/4)
25
62.5%(25/40)
63.6%
Surg Onc
10
62.5%(10/16)
51
68%(51/75)
67%
Thoracic
7
77.8%(7/9)
24
77.42%(24/31)
77.5%
Transplant
6
85.7%(6/7)
68
66.67%(68/102)
67.9%
Trauma
32
85.1%(32/39)
84
77.78%(84/108)
78.9%
Urology
1
100%(1/1)
12
92.31%(12/13)
92.9%
Vascular
2
100%(2/2)
74
69.2%(74/107)
69.7%
MiscevicFilipWangYoudongHuiWingZhangHaiboSlutskyArthurRotsteinOriWenXiao-Yan
St. Michael's Hospital
ANTI-INFLAMMATORY DRUG DISCOVERY IN VIVO: USE OF THE ZEBRAFISH TO SCREEN COMPOUNDS FOR THEIR ABILITY TO INHIBIT NEUTROPHIL INFILTRATION
Background: An excessive local inflammatory response may lead to tissue injury and organ dysfunction following both infectious and non-infectious stimuli. New agents aimed at modulating this response may serve to improve outcome in these patients. The zebrafish has emerged as a powerful model organism for chemical genetic screens due to its close evolutionary proximity to humans, high fecundity, optical transparency during organogenesis, and external development. Using the transgenic mpx:GFP zebrafish strain, neutrophils can be visualized and tracked in vivo by fluorescence microscopy.
Hypothesis: We hypothesize that compounds inhibiting neutrophil migration may be developed as anti-inflammatory drugs.
Methods: We evaluated a previously reported model of neutrophil infiltration and its potential role in drug screening. This method induces inflammation chemically by immersing fish embryos in copper sulfate (known to injure neuromast cells) and is studied for neutrophil migration to the lateral line where neuromasts reside. Neutrophil counts were compared among three treatment groups of embryos incubated in embryo water with 1% DMSO containing either no compound, 10 μM ibuprofen, or 3 μM diclofenac, which are known non-steroidal anti-inflammatory drugs. Preincubation in the aforementioned compounds and a neuromast stain (50nM Mitotracker CM-X-Ros) was performed, after which treatment groups were transferred to 10 μM copper sulfate. Fish were then imaged and neutrophil infiltration was assessed along the lateral line.
Results: Co-localization of neuromasts and GFP-labeled neutrophils was revealed by staining of the neuromasts with Mitotracker dye. Compared with the positive control group (CuSO4 in 1% DMSO alone, n=19), both ibuprofen (n=18) and diclofenac (n=17) were shown to significantly limit neutrophil infiltration (p<0.05).
Conclusions: The results of this study suggest that copper sulfate-based inflammation assays are rapid and sensitive, and require minimal manual labor to perform. In future studies, the transgenic cldnB:GFP neuromast reporter zebrafish line can be crossed with the mpx:RFP neutrophil zebrafish reporter line to improve identification of neuromasts. As such, this methodology shows great potential for deploying automated, high-throughput chemical genetic screens for discovery of novel inflammation-modulating drugs.
PouliotJonathonDortchMarcusCreechC. BuddyMayAddison
Vanderbilt University
THE USE OF E-TEST MINIMUM INHIBITORY CONCENTRATION (MIC) VALUES TO DETERMINE VANCOMYCIN TREATMENT FAILURES IN A SURGICAL ICU POPULATION
Background: Vancomycin is considered the treatment of choice for methicillin-resistant Staphylococcus aureus (MRSA) infections. Recent data on vancomycin usage has indicated that MICs may be rising among strains of MRSA, which has resulted in increasing treatment failures. Utilizing MIC values determined by e-test, this study examines whether MIC values are predictive of vancomycin treatment failure in MRSA isolates obtained from a surgical ICU population.
Hypothesis: Higher vancomycin MIC for MRSA as measured by e-test is a predictor of treatment failure in surgical ICU patients.
Methods: A single-center retrospective cohort study was conducted in patients admitted to either a surgical or trauma ICU. Isolates were identified based on positive MRSA cultures that had been obtained from patients treated for infection; e-test susceptibility tests were done to determine MIC values. Isolates were then matched to clinical data related to vancomycin treatment course. Vancomycin failure was defined as positive MRSA culture while on therapy, change from vancomycin to another agent based on clinical judgment, or infection-related mortality during therapy.
Results: Of isolates identified, 66 MRSA isolates were identified as having vancomycin MIC data by e-test, with 55 (83.3%) of those isolates being treated with vancomycin. A majority of the isolates were obtained from bronchoalveolar lavage/sputum (63.6%) or blood (13.6%) cultures. Patients from whom the isolates were obtained were being cared for in the surgical ICU (65.2%) and trauma ICU (34.8%), and the mean admission APACHE II score was 18.8 for all evaluable patients. Vancomycin failure occurred with 28 cases, which was 51% of those treated with vancomycin. There was no statistically significant correlation between e-test MIC values and vancomycin treatment failure. A weak positive correlation was found between e-test MIC values and both ICU (r2=0.199, p<0.001) and hospital length of stay (r2=0.191, p<0.001).
Conclusions: According to the results, there did not appear to be a correlation between MIC values and vancomycin failure utilizing the e-test method of susceptibility identification. Although this included a small sample of isolates, this evaluation shows that there is a high incidence of vancomycin treatment failure in critically ill patients that may not be fully described by increasing MIC values.
HeffernanDaithiMonaghanSeanChungChun-ShiangCioffiWilliamGravensteinStefanAyalaAlfred
Brown University
THE INVARIANT NATURAL KILLER T-CELL (iNKT) RESPONSE IS ENHANCED IN CRITICALLY ILL SEPTIC GERIATRIC PATIENTS
Background: Sepsis is associated with a severe immunosuppression, especially lymphocyte loss and dysfunction. Regulatory T-cell populations are critical modulators of the immune response. Invariant natural killer T-cells (iNKT-cells) are known modulators of the anti-inflammatory aspects of the immune response. Although geriatric patients display baseline functional decline in several immune drivers, iNKT-cell numbers and their ability to be activated are believed to be preserved in both health and disease despite aging.
Hypothesis: We postulate that following sepsis iNKT-cell populations are preserved in geriatric compared with young patients.
Methods: 27 young (18–35 yrs), and 51 geriatric patients (≥65 yrs) ICU patients with a microbiologically confirmed diagnosis of sepsis were enrolled. Daily white blood cell count was collected clinically; study blood was drawn concomitantly. Blood was stained with monoclonal antibodies to detect CD3 (T-cells), anti-TCR-Vα-24 (invariant NKT-cells) and CD69 (marker of early cell activation). Both percentage and absolute number of cells present were then calculated. Blood from 10 healthy controls was also collected.
Results: As a group septic patients, when compared with healthy controls, displayed a marked leukocytosis (14.4 vs 6.4×109/L; p=0.001) and decreased CD3+ lymphocytes (7.4% vs. 26.1%; p=0.001). Septic patients displayed increased percentage of iNKT-cells (1.16% vs. 0.57%; p=0.02) leading to preservation of absolute number of iNKT-cells (11.6 vs. 8.86×106/L; p=0.10) Comparing geriatric to young patients, there was no difference in degree of leukocytosis (14.1 vs. 14.9×109/L; p=0.10), CD3+ T-cell percentage (7.0% vs. 7.9%; p=0.38) or absolute number (9.43 vs. 10.36×108/L; p=0.35), or CD69+ (activated) CD3+ T-cells (9.4% vs. 8.9%; p=0.08). iNKT-cells were increased in geriatric patients compared with young patients as a percentage of CD3+ T-cells (1.24% vs. 0.91%; p=0.04) and in absolute number (13.2 vs. 8.2×106/L; p=0.04). Further, iNKT-cells were significantly more activated (CD69+) in geriatric septic patients (20.9% vs. 10.7%; p=0.001).
Conclusions: iNKT-cells are known immune-suppressants and modulators of the counter-inflammatory response. iNKT-cells are increased and significantly more activated in geriatric compared with young septic patients. This finding expands our understanding of the dampened immune response seen in septic geriatric patients.
AgarwalAvinashCampolietoMicheleAllyWinstonDornHarryBraymanKenneth
University of Virginia
INTRAVENOUS IMMUNOGLOBULIN (IVIG) DOES NOT CONFER PROTECTIVE IMMUNITY AGAINST INFECTIONS IN DECEASED DONOR KIDNEY RECIPIENTS
Background: The impact of circulating donor-specific antibodies (DSA) in the setting of a negative cross-match is unclear. Previously sensitized patients will receive additional humoral immune-directed therapy if DSA are identified.
Hypothesis: We hypothesized that IVIG therapy would be protective against post- transplant infections via passive immunity.
Methods: We performed a single-center, retrospective analysis of deceased donor kidney transplant recipients from January 2009 to November 2011. Patients were stratified according to those without sensitization (I) and those with DSA and prior sensitization (II). Immunosuppression consisted of rabbit anti-thymocyte globulin and maintenance with tacrolimus, mycophenolate mofetil, and prednisone. Treatment patients (II) received rituximab and 2 g/kg IVIG, and were maintained on higher-dose prednisone. The primary outcome was infection (bacterial, viral, fungal) within 6 and 12 months. Univariate and log-rank statistical analysis was completed.
Results: A total of 140 adult patients underwent deceased donor kidney transplantation, with seven patients excluded due to early patient/graft loss. Group I consisted of 112 patients, while Group II consisted of 21 patients. There were no differences in patient or donor demographics except for follow-up (I: 540±220 days vs. II: 377±335 days; p=0.04). Patient survival was similar (I: 97% vs. II: 100%; p=ns). Death-censored graft survival was comparable (I: 98% vs. II: 95%; p=ns). There was no difference in acute cellular or humoral rejection. Six- (I: 42% vs. II: 39%; p=ns) and 12-month (I: 51% vs. II: 50%; p=ns) infection rates were similar, with no differences in fungal or bacterial infections. However, Group II had higher incidence of viral infections at 6 months (I: 4% vs. II: 22%; p=0.03). There was no difference in cytomegalovirus disease (I: 2% vs. 6%; p=0.38). BK viremia was higher in Group II (I: 3% vs. II: 17%; p=0.04). All of these patients have had BK treated successfully.
Conclusions: The preliminary data suggest that IVIG therapy does not appear to confer protective passive immunity for viral diseases, as patients receiving additional humoral immune-directed therapy had a higher incidence of viral infections. Further long-term follow-up and future studies will be necessary to assess the impact and benefit of these therapies in sensitized kidney transplant recipients.
FishmanJordanLevyGalXuDa-ZhoungLuQiDeitchEdwin
University of Medicine and Dentistry of New Jersey-New Jersey Medical School
THE INTESTINAL MUCUS LAYER IS A CRITICAL BUT UNRECOGNIZED COMPONENT OF THE GUT BARRIER
Background: Trauma-hemorrhagic shock (T/HS)-induced gut barrier failure has been shown to be important in the pathogenesis of SIRS, ARDS, and MODS. Recent studies have shown that the mechanisms underlying gut barrier failure include a luminal arm (mucus and pancreatic proteases) as well as a systemic arm (ischemia-reperfusion). Since little is known about the luminal arm of gut injury, we investigated the role of mucus in T/HS and tested the below hypothesis.
Hypothesis: Injury to the gut mucus layer is a critical factor in T/HS-induced gut injury and dysfunction.
Methods: Male Sprague-Dawley rats underwent trauma (laparotomy) and hemorrhagic shock (MAP 30–35 mm Hg for 90 minutes followed by reinfusion of shed blood and a 3 hour observation window). Sham rats were subjected to trauma but not hemorrhagic shock. Mucus from the terminal 30 cm of the distal ileum was collected, processed, and analyzed. Reactive nitrogen intermediate (RNI)-mediated damage was measured using an ELISA for nitrated tyrosine residues. Reactive oxygen species (ROS)-mediated damage was measured via ELISA for oxidized carbonyl derivatives. Total antioxidant capacity (global capacity to respond to oxidant-mediated damage) was measured via ELISA. Gut permeability was measured by the passage of intraluminaly injected FD4 across the gut wall into the blood stream. Additional segments of the distal ileum were fixed and stained to visualize and quantify the mucus layer and intestinal villus injury.
Results: T/HS increased intestinal permeability (FD4), and this loss of gut barrier function correlated with histologic evidence of loss of mucus layer and villus injury (Table). Loss of gut barrier function and histologic damage correlated with an increase in ROS- and RNI-mediated mucus damage and loss of mucus antioxidant capacity.
Conclusions: These results support the hypothesis that injury to the mucus layer is a critical factor in T/HS-induced gut dysfunction and injury. Additionally, this is the first study to document that T/HS-induced intestinal reperfusion causes ROS- and RNI- mediated injury to the mucus layer.
WuXiuwenRenJiananHansemanDennisSolomkinJoseph
Nanjing University
HOW MUCH DO ANTIBIOTICS HELP? A META-ANALYSIS OF OUTCOME FROM APPENDIX-DERIVED PERITONITIS (PAP) BEFORE ANTIBIOTICS
Background: The effect size of antibiotic therapy for intra-abdominal infection is not well defined because randomized trials have used a non-inferiority, active control design. We performed a meta-analysis of outcome from purulent diffuse peritonitis from appendicitis (PAP) reported prior to, and then after the introduction of sulfa compounds.
Hypothesis: Sulfa therapy would show a significant improvement in outcome without the need for adjustment for other care elements (fluid resuscitation, McBurney incision, appendix removal) during the study period.
Methods: All studies reporting outcome from appendicitis from 1896 to 1959 were reviewed using standard database search strategies. We employed meta-regression models with mid-year of each study's time span as the explanatory variable to capture heterogeneity. P values≤0.05 were interpreted as indicating statistical significance.
Results: We found 128 studies suitable for analysis. We identified a plateau effect in survival based upon prior adoption of urgent operation, intravenous fluid replacement, and use of McBurney incisions. The trend analysis showed little if any decline in mortality from PAP during the pre-antibiotic era (Figure). The effect of sulfa therapy was noted in 5 comparative studies, all using a pre-/post-design. Mortality in the control arm was 29.6±14.5% vs. 5.3±3.5% in the sulfa-treated arm, a five-fold reduction. The overall risk difference was -0.146 (95% CI-0.267, -0.025), p<0.0001. Clinical trials focusing on age >50 years, a major risk factor for death in the pre-sulfa era, demonstrated an even more profound benefit.
Conclusions: Antimicrobial therapy plays an important role in the treatment of patients with PAP. As the first widely used antibiotic, sulfa drugs significantly improved outcomes for patients with PAP, without coverage of anaerobic organisms.
BaghelKavitaRajSaloniChandraAbhijitSrivastavaRajeshwar
CSM Medical University
TNF-β NCO1 POLYMORPHISM AND SEPSIS SUSCEPTIBILITY IN SURGICAL PATIENTS
Background: Postoperative sepsis remains a significant cause of morbidity and mortality. Genetic factors have role in the pathogenesis of sepsis. Tumor necrosis factor (TNF) is believed to be a cytokine central to pathogenesis of sepsis. The TNF-β Nco1 polymorphism is associated with increased mortality rate in severe sepsis.
Hypothesis: The study aimed to analyze TNF-β Nco1 polymorphism in relation to postoperative sepsis outcome.
Methods: The study group consisted of 153 patients undergoing major elective surgery (surgical time >1 hour, requiring general anesthesia or respiratory assistance). Blood samples were obtained for DNA isolation and genotyping for TNF-β polymorphism by analyzing restriction fragments of an Nco1-digested DNA fragment using PCR. All patients were followed for 1 month following surgery for evidence of sepsis as determined by guidelines from Bone et al. Genotypes were then related to the occurrence of postoperative sepsis.
Results: The overall allele frequency for TNF-β genotype was 0.32 for TNFB1 and 0.68 for TNFB2. In TNF-β genotype, homozygous recessive TNFB1 were 17 (11.1%), heterozygous TNFB1/TNFB2 were 63 (41.2%), and homozygous dominant TNFB2 were 73 (47.7%). 125 patients showed an uncomplicated postoperative recovery, while sepsis developed in 28 patients. Genotype distribution in patients with an uncomplicated clinical course was significantly different from that of patients with postoperative sepsis. Development of postoperative sepsis was significantly higher in patients homozygous for the allele TNFB2. When compared with patients carrying at least one TNFB1 allele (TNFB1 homozygous and heterozygous genotype), TNFB2 homozygosity was associated with an OR of 3.39 (95%CI 1.4–8.3, p=0.005) for the development of severe sepsis. Compared with the heterozygous genotype, the OR for homozygous TNFB2 was 5.5 (95%CI 1.78–17.33, p=0.001). Although the small number of TNFB1-homozygous surgical patients makes their risk estimate less accurate, the data indicate that both homozygous genotypes possess a significantly increased susceptibility for development of postoperative sepsis compared with the heterozygous genotype.
Conclusions: The Nco1 polymorphism within the TNF-β gene influences postoperative sepsis outcome. TNFB1 and TNFB2 homozygotes have a higher risk of developing postoperative infection; although the TNFB2 homozygous genotype is more significantly associated with development of postoperative sepsis.
Poster Presentation Abstracts
PoroykoValeriyKohlhappFredRodriguezAlexUlanovAlexanderAlverdyJohnLiuDonaldGuevara-PatiñoJosé
The University of Chicago
CHANGES OF INTESTINAL MICROBIOTA IN A MURINE MODEL OF METASTATIC BREAST CANCER
Background: Microbiome has recently received attention in connection to microbe-mediated malignancy, but the relationship between host and microbiota is bi-directional. Change of the host's physiological or immunological status affects the structure of the host-associated microbial communities.
Hypothesis: Here we hypothesize that the development of a tumor will affect the structure of the host's intestinal microbiota. The objective of this study is to examine the dynamics of the intestinal microbiota during tumor development.
Methods: BALB/c male mice (n=32) were housed in groups (3–4 animals) for 12 weeks, upon receiving from Jackson Laboratories. One-half of the mice were challenged with a metastatic breast cancer cell line 4T1 (105) in the mammary fat pad, while the control group received RPMI injection. The experimental group mice developed palpable tumors at day 7. Stool samples were collected from each mouse before injection (-7d), and 7 and 17 days after injection. Microbial community structure was evaluated by terminal restriction fragment length polymorphism (TRFLP) technique. Statistical analysis was performed using R, Simka, and Primer 6 statistical software.
Results: Multidimensional scaling (MDS) demonstrated separation of control and treatment groups starting -7d, the dynamics of microbiota during the course of study, and similarity of microbiota for the mice housed in a same cage. ANOVA analysis confirmed the differences between groups and temporal dynamics within groups, but suggested stronger change related to tumor challenge. When control and treatment groups were analyzed separately using principal component analysis (PCA), we determined the set of operational taxonomic units (OTUs) changing during the study; among them, 3 were found changing in tumor group only. ANOVA analysis confirmed closer relation between microbiota at day -7 and 7 in control group, while in the treatment group microbiota of 7d and 17d was more similar and separated from -7d time point, emphasizing tumor-related changes in microbial community.
Conclusions: We evaluated the effect of malignant growth on intestinal microbiota. We were able to separate changes related to tumor development from the aging-related dynamics in control group, and suggested several individual OTUs to be involved in response to tumor progression. Future direction involves microbial community profiling by sequencing to determine taxonomic assignment of tumor-responding bacteria.
KimMosesZaborinaOlgaAlverdyJohn
The University of Chicago
FASCIA TRIGGERS BACTERIAL VIRULENCE AND MAY PLAY AN IMPORTANT ROLE IN THE PATHOGENESIS OF SOFT TISSUE INFECTION AFTER MUSCLE INJURY
Background: With tissue trauma, rates of infection remain high and are commonly caused by hospital pathogens such as P. aeruginosa and MRSA.
Hypothesis: A major factor in this response is microbial virulence activation occurring in response to host factors. Our project aim was to develop a mouse model to identify host factors that trigger virulence expression in the presence of traumatic muscle injury.
Methods: For our control group, C57BL/6 mice underwent sterile skin incision, exposure of the rectus muscle, 15 min exposure to a bacteria, irrigation, and skin closure. For muscle injury groups, a needle driver was used to create three foci of rectus muscle injury prior to bacterial exposure. Bacteria were prepared by mixing sterile mouse feces with either 105 CFU P. aeruginosa or 107 CFU MRSA. On post-op day (POD) 7, mice were euthanized and observed for clinical soft tissue infection, defined as purulence within the wound. In-vivo bacterial growth was assessed on PODs 1, 3, and 7 by photon-camera imaging and in separate parallel mice by quantitative culture. To determine components that activated bacterial virulence, ex-vivo studies were performed by homogenizing mouse tissues (skin, fascia, muscle) and evaluating their ability to trigger P. aeruginosa virulence, as judged by pyocyanin production.
Results: On POD 7, infection rates were significantly higher in mice with muscle injury vs. controls (80% vs. 10%) for P. aeruginosa (n=20/group, p<0.001; Fig 1a) and MRSA (n=5/group, p=0.001). Photon imaging showed attachment and growth to sites of injury by P. aeruginosa, although there was no significant difference in quantity on POD 3 (n=5, p=0.14). Ex-vivo tissue experiments demonstrated significant increases in pyocyanin production when P. aeruginosa was exposed to all host tissues (n=8–10/group versus control, p<0.001) with greatest increase seen with fascia (Fig 1b).
*p<0.001 vs. control media.
Conclusions: Muscle injury is associated with a high rate of clinical tissue infection despite equal bacterial exposure and early growth rates. This may be due in part to activation of bacterial virulence in response to injured host tissues, especially fascia.
PontarelliElizabethFranklinAshantiGrishinAnatolyFordHenri
Children's Hospital Los Angeles
PURIFICATION OF THE P-GLYCOPROTEIN (PGP)-INDUCING COMPONENT OF BREAST MILK
Background: It is well established that breast-fed neonates have a decreased incidence of necrotizing enterocolitis (NEC). Pgp is a transmembrane protein that is protective against intestinal inflammation in a bacteria-dependant manner. Our previous work established that breast milk induces expression of Pgp in the intestinal epithelium and that Pgp is protective against NEC in an animal model.
Hypothesis: Our goal is to identify the Pgp-inducing factor of breast milk and establish a purification strategy.
Methods: Breast milk was donated by healthy lactating mothers. Whole milk underwent crude purification via centrifugation, pH adjustment, and precipitation by ammonium sulfate. This crude fraction was then processed through the cation-exchange resin Q-Sepharose, and eluted with increasing concentrations of NaCl. The active fraction was then placed in a medium-pore gel filtration column for size exclusion chromatography. At each step, fractions were administered to SW480 cells and Pgp expression was confirmed on Western blot. Protein composition was evaluated with Coomassie staining, and total protein was measured with spectrophotometry.
Results: Crude purification decreased the total protein content of the sample from 7.67 g to 44 mg. Following ion-exchange chromatography, the active sample totaled 6 mg of protein and contained 15–20 proteins visible on Coomassie staining. The active sample after gel filtration contained 1.7 mg of protein with 4–6 bands between 50 and 250 kDa on staining. Mass spectroscopy of this sample revealed 12 proteins.
Conclusions: We have successfully fractionated human breast milk and identified a semi-pure sample that induces Pgp expression. The small number of proteins in the active sample will undergo further evaluation. The Pgp-inducing factor of breast milk is potentially a preventive strategy for prophylaxis against NEC.
Proteins present in active fractions after each stage of purification. Coomassie stained polyacrylamide gel.
GopalakrishnanVissaganKimMosesAlverdyJohnAnGary
The Johns Hopkins University
DYNAMIC KNOWLEDGE REPRESENTATION OF HOST-MICROBE DYNAMICS IN SURGICAL SITE INFECTION (SSI) USING AN AGENT-BASED MODEL
Background: SSIs are a major source of post-operative morbidity. SSI and healing are complex and integrated processes, and investigating the pathogenesis of SSI requires first characterizing the cellular/molecular mechanisms present in normal wound healing and then exploring conditions that may lead to infection. Dynamic knowledge representation of these mechanisms can aid in developing an integrated understanding of the processes leading to infection. We utilized an agent-based model (ABM) of the cellular/molecular dynamics of a surgical wound to investigate the effects of bacterial virulence activation on the pathogenesis of SSI.
Hypothesis: We hypothesize that the pathogenesis of SSI is accentuated by variable bacterial virulence.
Methods: An ABM of muscle wound healing was developed with agents representing muscle cells (both normal and damaged), neutrophils, macrophages, natural killer cells, myoblasts, and abstracted blood vessels. Abstracted bacterial agents had variable virulence, represented by their reproduction rate and ability to damage tissue. Simulated experiments (t=21 days) varied wound size, bacterial inoculum, and bacterial virulence to characterize tipping points between healing, abscess formation, and invasive infection.
Results: The ABM reproduced recognized steps of muscle wound healing: the initial influx of neutrophils to the wound, the formation of pus, phagocytosis by macrophages, myogenesis, and the down-regulation of various immune elements. A parameter sweep of wound size and initial bacterial load demonstrated thresholds for abscess formation and invasive infection. Increased bacterial virulence potential lessened both the threshold wound size and initial bacterial load for abscess development.
Conclusions: Wound infection and healing is a complex process that involves multiple levels of control governing the entrance and clearance of responding cells. The introduction of bacteria with variable virulence greatly affected the dynamics of the development of persistent infections. Given the known ability of host factors to activate bacterial virulence, the presence of bacteria with this capability are may play a critical role in the development of SSI, and suggests that interdiction aimed at reducing virulence activation may represent a viable therapeutic strategy.
WITHDRAWN
WITHDRAWN
LockwoodAlissaRahbarAryanAbrahamPrasadPatkaJohnCurzioKarenRabinovichMarinaChesterKatleenHuangVanthidaWilliamsBrianChaarMitchellMorseBryanSalomoneJeffreyButterfieldJillLodiseThomas
Parkland Health and Hospital System
PHARMACOKINETIC AND PHARMACODYNAMIC EVALUATION OF DORIPENEM IN CRITICALLY ILL TRAUMA PATIENTS WITH SEPSIS
Background: Doripenem, a carbapenem antibiotic, is used to treat gram-negative infections in the ICU. No data exist on the pharmacokinetics (PK) of this drug in the critically ill trauma population with sepsis. Patients with trauma tend to be younger with fewer co-morbidities. They are hypermetabolic and often receive aggressive fluid resuscitation, resulting in increased renal clearance of drugs and a larger volume of distribution. As a consequence of these differences in PK parameters, standard doses could result in sub-optimal time above the minimum inhibitory concentration (T>MIC).
Hypothesis: To evaluate the pharmacokinetics and pharmacodynamics of doripenem in a population of critically ill trauma patients with sepsis
Methods: We designed a prospective, open-label, steady-state PK study in a convenience sample of adult trauma patients admitted to the surgical critical care service with a diagnosis of sepsis who required empiric antimicrobial therapy. Following informed consent, eligible patients were administered doripenem 1 g intravenously (over 4 h) every 8 h for a total of 3 doses. Serum levels were drawn prior to the administration of the 3rd dose and at 1, 2 and 4 h after administration of the 3rd dose. Monte Carlo simulation of 9,999 patients was used to calculate probabilities of achieving appropriate PD targets. IRB approval was obtained.
Results: Thirty patients were recruited for the study; however data from only 27 patients were evaluable. Results are as follows: Mean Vd (L) – 28.52±16.01, Mean CL (L/h) – 16.94±11.4, Mean t1/2 (h-1)−1.47±2.24. Table demonstrates the probability of achieving the appropriate PD target.
Conclusions: Compared to healthy volunteers, trauma patients have a higher Vd and CL. Based on this study, higher doses of doripenem are necessary to achieve appropriate concentrations in these patients.
% Probability of Attaining PK/PD Target
%T>MIC
MIC (mcg/ml)
30
40
50
0.25
100
100
100
0.5
100
100
99.99
1
99.97
99.97
99.94
2
99.81
99.77
98.99
4
96.81
95.35
88.97
8
72.74
65.25
52.39
16
22.53
17.62
12.63
32
1.56
1.13
0.83
WITHDRAWN
WITHDRAWN
BadalRobertBouchillonSamuelJohnsonAaronHackelMeredithHobanDaryl
International Health Management Associates, Inc.
EPIDEMIOLOGY AND ANTIMICROBIAL SUSCEPTIBILITY OF PATHOGENS ISOLATED FROM INFECTIONS OF THE GALLBLADDER-SMART 2002–2011
Background: The Study for Monitoring Antimicrobial Resistance Trends (SMART) has monitored activity of amikacin (AK), ampicillin-sulbactam (AS), cefepime (CPE), cefotaxime (CFT), cefoxitin (CFX), ceftazidime (CAZ), ceftriaxone (CAX), ciprofloxacin (CP), ertapenem (ETP), imipenem-cilastatin (IMP), levofloxacin (LVX), and piperacillin-tazobactam (PT) vs. aerobic gram-negative bacteria (GNB) from intra-abdominal infections since 2002. This report summarizes susceptibility and epidemiology for key IAI pathogens from infected gallbladders globally.
Hypothesis: Local extended-spectrum beta-lactamase (ESBL) rates must be taken into account to optimize empiric therapy of gallbladder infections.
Methods: 4,627 GNB were collected from infected gallbladders by 146 labs in 40 countries from 2002 to 2011. Minimum inhibitory concentrations (MICs) were determined by broth microdilution, and interpreted using Clinical and Laboratory Standards Institute guidelines. Susceptibility rates (%S) for isolates were determined for species with ≥10 isolates.
Results: One-half of the study isolates came from 5 countries: Taiwan (809); China (434); Spain (416); U.S. (408); and India (291). There was a gender bias toward men (57%) vs. women (43%). Overall ESBL+rate was 19.2% of 3,119 E. coli, Klebsiella spp., and P. mirabilis. The susceptibilities of the top 10 isolates are listed in the Table.
Conclusions: ETP, IMP, and AK were the most active in vitro against GNB from gallbladder infections; 3rd/4th-generation cephalosporins and fluoroquinolones were usually <90% active. Given the wide variations in regional ESBL+rates, therapy for gallbladder infections should take into account local ESBL+rates since only IMP, ETP, and AK inhibited most of these pathogens.
TessierJeffreySirkinMaxwellWolfeLukeDuaneTherese
Virginia Commonwealth University
TRAUMA AFTER TRANSPLANT: HOLD THE ANTIBIOTICS
Background: No data exist related to transplant patients who suffer trauma. Since transplant patients have multiple co-morbidities and are immunosuppressed, we were concerned that they would be at higher risk for complications, particularly infections. Additionally, antimicrobial (Abx) use tends to be much higher in transplant than in trauma so we believed it would be important to determine if these patients would require a different approach to treatment.
Hypothesis: To determine if transplant patients (TP) have worse outcomes, particularly infections, than their non-transplant (NTP) counterparts after trauma.
Methods: A retrospective review was performed on trauma patients from 2006–2010. All patients with transplants were included and compared by 1:3 propensity matching to their non-transplant counterparts. Data for the groups were compared to determine differences in outcome.
Results: There were 17 TP (13 renal, 2 liver, 1 renal/liver, 1 renal/pancreas) compared to 51 NTP. They were matched for injury severity score (ISS), age, and gender with most having blunt trauma (82.4% (14/17) TP vs. 90% (46/51) NTP, p=0.50). The groups had a similar initial Glasgow Coma Scale score GCS (13.2±4.5 TP vs. 13.9±2.5 NTP, p=0.6)0, lactate (2.0±1.8 mmol/L TP vs. 2.3±1.5 mmol/L NTP, p=0.39), and base deficit (-1.5±4.0 TP vs. 0.6±3.0 NTP, p=0.21). Co-morbidities were more common in the TP group (Table). The groups had similar lengths of stay (days) (ventilator: 0.1±0.3 TP vs. 0.4±1.6 NTP, p=0.90; ICU: 0.2±0.6 TP vs. 2.4±5.9 NTP, p=0.16; hospital: 5.2±6.8 TP vs. 7.5±10.2 NTP, p=0.86) and both had 2 deaths (p=0.26). Overall complications were similar (52.94% (9/17) TP vs. 62.75% (32/51) NTP, p=0.57) and there were only 2 infections, both in the NTP group (p=1.0). 59% of TP vs. 39% NTP received Abx with the average number of days of Abx treatment being 8.35 TP vs. 3.9 NTP.
Co-morbidities
TP
NTP
p-value
Cardiac
29.4%(5/17)
7.84%(4/51)
0.04
Hypertension
88.2%(15/17)
27.5%(14/51)
<0.001
Dialysis
64.7%(11/17)
1.96%(1/51)
<0.001
IDDM
17.7%(3/17)
1.96%(1/51)
0.05
Immuno-suppression
82.4%(14/17)
1.96%(1/51)
<0.001
Conclusions: When equally matched for degree of injury, TP and NTP patients have similar outcomes. There also appears to be no difference in infectious complications, yet more TP had exposure to more days of antibiotics. Similar protocols should apply to both groups to avoid overuse of antimicrobials and ensure maintenance of susceptibility patterns.
ANTIMICROBIAL ACTIVITY OF THE NEW CEPHALOSPORIN CEFTAROLINE TESTED AGAINST BACTERIAL ISOLATES FROM SURGICAL SKIN AND SKIN STRUCTURE INFECTIONS IN USA MEDICAL CENTERS (2008–2011)
Background: Ceftaroline, the active form of ceftaroline fosamil, is a cephalosporin with in vitro activity against many common gram-positive and -negative bacteria, including methicillin-resistant (R) S. aureus (MRSA), multidrug-R streptococci, and commonly isolated (non-extended-spectrum beta-lactamase (ESBL)-producing) Enterobacteriaceae.
Hypothesis: To assess the activity of ceftaroline and comparator agents against pathogens isolated from surgical skin and skin structure infections (SSSI).
Methods: Clinically significant strains (1/patient) were consecutively collected from 64 USA medical centers from 2008–2011 and tested for susceptibility (S) by reference Clinical and Laboratory Standards Institute (CLSI) broth microdilution methods against ceftaroline and >20 antimicrobials available for treatment of surgical SSSI.
Results: 1,564 strains were tested. Ceftaroline was very active against oxacillin-S S. aureus (MSSA; MIC90, 0.25 mcg/mL) and MRSA (52.4%; MIC90, 1 mcg/mL). Against MSSA, ceftaroline was 16-fold more potent than ceftriaxone, and the highest ceftaroline MIC was only 0.5 mcg/mL. 97.9% and 100.0% of MRSA were inhibited at ≤1 and ≤2 mcg/mL of ceftaroline, respectively. β-hemolytic streptococci (BHS) were very S to ceftaroline, and the highest ceftaroline MIC was only 0.03 mcg/mL among Groups A and B BHS. Ceftaroline was also active against coagulase-negative staphylococci (CoNS) (MIC90, 0.5 mcg/mL), including methicillin-R strains, and 4-fold more potent than ceftriaxone against viridans group streptococci. High R rates to levofloxacin and clindamycin were observed among MRSA and CoNS. Ceftaroline activity against most common Enterobacteriaceae (MIC50/90, 0.12/4 μg/mL) was similar to ceftriaxone and ceftazidime. ESBL phenotypes were observed in 8.5% of E. coli and 9.5% of Klebsiella spp., and all cephalosporins tested showed limited activity against these strains (See Table below).
Number of isolates (cumulative %) inhibited at ceftaroline MIC (μg/mL) of:
Organism (no. tested)
≤0.015
0.03
0.06
0.12
0.25
0.5
1
2
4
S. aureus (731)
-
-
2(0.3)
51(7.3)
281(45.7)
224(76.3)
165(98.9)
8(100.0)
-
MSSA (348)
-
-
2(0.6)
51(15.2)
278(95.1)
17(100.0)
-
-
-
MRSA (383)
-
-
-
-
3(0.8)
207(54.8)
165(97.9)
8(100.0)
-
β-haemolytic strep (231)
192(83.1)
36(98.7)
3(100.0)
-
-
-
-
-
-
Group A (72)
71(98.6)
1(100.0)
-
-
-
-
-
-
-
Group B (119)
96(80.7)
23(100.0)
-
-
-
-
-
-
-
Others (40)
25(62.5)
12(92.5)
3(100.0)
-
-
-
-
-
-
CoNS (80)
1(1.3)
0(1.3)
17(22.5)
11(36.3)
30(73.8)
17(95.0)
4(100.0)
-
-
Viridans group strep (55)
20(36.4)
25(81.8)
6(92.7)
2(96.4)
0(96.4)
2(100.0)
-
-
-
E. faecalis (82)
-
-
-
-
-
-
21(25.6)
42(76.8)
14(93.9)
Enterobacteriaceae (385)
1(0.3)
21(5.7)
101(32.0)
95(56.6)
67(74.0)
29(81.6)
20(86.8)
9(89.1)
4(90.1)
E. coli (141)
-
12(8.5)
50(44.0)
35(68.8)
17(80.9)
5(84.4)
4(87.2)
2(88.7)
2(90.0)
Klebsiella spp. (85)
1(1.2)
3(4.7)
21(29.4)
26(60.0)
20(83.5)
4(88.2)
1(89.4)
2(91.8)
1(92.9)
Enterobacter spp. (56)
-
1(1.8)
5(10.7)
14(35.7)
18(67.9)
7(80.4)
2(83.9)
0(83.9)
1(85.7)
Conclusions: Ceftaroline exhibited potent activity against gram-positive bacteria, including MRSA, and many Enterobacteriaceae. Ceftaroline appears to be an optimal agent for the treatment of patients with surgical SSSI in USA hospitals.
PasupuletiLathaSifriZiadMohrAlicia
University of Medicine and Dentistry of New Jersey-New Jersey Medical School
IS EXTENDED ANTIBIOTIC PROPHYLAXIS NECESSARY FOLLOWING PENETRATING TRAUMA TO THE THORACOLUMBAR SPINE WITH CONCOMITANT INTRAPERITONEAL INJURIES?
Background: Prolonged courses of broad-spectrum antibiotics are often cited as the standard of care for prevention of infectious complications of thoracolumbar (TLS) fractures following penetrating abdominal trauma. Perforation of a hollow viscus in addition to a TLS injury is thought to be associated with a high incidence of spine infection.
Hypothesis: Since an increasing prevalence of multi-drug resistant organisms is associated with overuse of antibiotics, this study seeks to define the actual risk of infection of the spine in patients with TLS fractures and intraperitoneal injuries following penetrating trauma.
Methods: A retrospective review of 60 patients with penetrating abdominal trauma and concomitant TLS fracture was performed. In addition to demographics, level of TLS fracture, associated spinal cord injury (SCI), need for operative intervention, presence of concomitant hollow viscus injury, type and duration of antibiotic coverage were collected. In addition, associated infectious complications were reviewed. Spine infections were defined as spinal or paraspinal abscess, osteomyelitis, or meningitis. Intra-abdominal infections were defined with positive peritoneal cultures.
Results: All 60 patients (mean age 27±9 y) had an exploratory laparotomy and one or more TLS fractures. 53% had a SCI in addition to their fracture. 35 (59%) patients had one or more hollow viscus injuries, 11 (18%) had solid organ injury alone; 14 (23%) had neither. All but one patient received perioperative antibiotics. 49 (82%) patients received 24 h of antibiotics. 6 (10%) patients received 48 of antibiotics, and 5 (8%) patients received 3–5 d of antibiotics. Three patients received operative intervention of their TLS fracture. There was only one spine infection in a patient with an isolated solid organ injury. Twenty-five percent had an intra-abdominal infection and 80% occurred in patients with hollow viscus injuries. Average clinical follow-up was 18 months.
Conclusions: In this study, 92% of patients received antibiotics for 48 h or less with no increased incidence of spine infections. Bacterial colonization of the vertebrae was not higher with penetrating viscus injury. There is insufficient evidence to support the use of prolonged antibiotic coverage to prevent spine infection in patients with penetrating abdominal trauma or hollow viscus perforation.
WITHDRAWN
PontarelliElizabethNosanovLaurenMaIrenePierceJames
Children's Hospital Los Angeles
APPENDICITIS IN CHILDREN WITH COGNITIVE DEFICITS
Background: Appendicitis is one of the most common surgical diseases in children, and patients with cognitive deficits pose a significant diagnostic challenge. Alterations in communication, perception, and cognition may affect diagnosis and perioperative course. Presently limited data are available on patients with appendicitis and cognitive deficits.
Hypothesis: We hypothesize that children with cognitive deficits who develop appendicitis have diagnostic delays and increased complications.
Methods: We reviewed all patients with a diagnosis of appendicitis between July 1, 2004 and October 15, 2010 at our institution. Patients with pervasive developmental disorders (autism, Rett syndrome, childhood disintegrative disorder), mental retardation, and infantile cerebral palsy were included in our definition of cognitive deficit (CD). We evaluated diagnosis, treatment, and complications.
Results: Of 1,467 children with appendicitis, 23 patients had CD. Demographics were similar in both groups. At presentation, reports of nausea, vomiting, and diarrhea showed no significant difference, but patients with CD less often reported abdominal pain (78% vs. 94%, p=0.002). Physical exam in children with CD more frequently revealed no tenderness (17% vs. 7%, p=0.05) or diffuse rather than localized tenderness (26% vs. 13%, p=0.065). CT scans were performed in almost all patients with CD (91% vs. 57%, p=0.008) and frequently showed abscesses (39% vs. 14%, p=0.004). Laboratory values (WBC and CRP) showed no statistical difference. Treatment strategy showed that children with CD had more non-operative management (35% vs. 12%, p=0.008) and more open appendectomies (26% vs. 8%, p=0.001). Patients with CD had surgery more than 24 h after admission 73% of the time compared to 54% in non-CD patients (p=0.10). Post-operative complications occurred in 32% of CD patients and 13% of the general cohort (p=0.10).
Conclusions: Our data confirm that patients with cognitive deficits have atypical presentations of appendicitis and more frequently require additional imaging. They often present with abscesses and subsequently undergo non-operative management. The higher rate of open appendectomy is likely due to prior abdominal operations in patients with CD (i.e., ventriculo-peritoneal shunt, tube gastrostomy). While CT scans were performed frequently on patients with CD, this did not appear to improve time to OR. Additional evaluation of CT scan timing may reveal that earlier imaging could improve operative delay.
LevyShaunaJohnsonElizabethWilliamsKarenWellsMeredithTaylorKimberleeKaoLillianHolzmann-PazgalGalitLallyKevinTsaoKuoJen
University of Texas Medical School at Houston
PROTOCOLIZED TREATMENT OF APPENDICITIS LEADS TO DECREASED COST WITHOUT INCREASED INFECTIOUS COMPLICATIONS
Background: Treatment protocols applied to common diseases such as appendicitis can lead to decreased cost and hospital length of stay (LOS). Surgical site infections (SSI) are the most common complication that occurs among appendicitis patients. The relationship between treatment protocols and patient outcomes including complications such as SSI has not been clearly evaluated.
Hypothesis: We hypothesize that protocolized treatment of simple appendicitis does not increase infectious complications, as cost and LOS decrease.
Methods: An observational study was performed on pediatric patients undergoing appendectomy for simple appendicitis. The protocolized treatment of simple appendicitis was introduced with a pilot protocol while surgical housestaff and nurses received protocol training. An initial protocol began after training completion. A multi-disciplinary team (housestaff, pediatric infectious diseases, nursing, and case management) evaluated the initial protocol after three months and created a revised protocol. During a 30-day post-operative SSI surveillance program, patients were prospectively monitored for SSIs, emergency room (ER) visits, and infectious readmissions. Additional outcomes included hospital LOS and hospital cost. χ2 analysis was used to compare the complication frequencies.
Results: Of the 312 appendicitis patients, 179 patients underwent appendectomy for simple appendicitis. The frequency of infectious complications did not significantly change with the different protocols (p>0.05) (Table). The baseline LOS was 35.65 h and hospital cost per patient was $7,175. Protocolized treatment shortened LOS by 36%. The average total hospital cost per patient decreased by $1,630, with total cost savings of $291,591.
Pilot versus Initial protocol p>0.05 by χ2 analysis.
Pilot versus Revised and Initial versus revised protocol p>0.05 by χ2 analysis.
Conclusions: Protocolized treatment for simple appendicitis does not lead to an increase in infectious complications but does lead to shorter LOS and decreased cost.
RajSaloniBaghelKavitaChandraAbhijitSrivastavaRajeshwar
CSM Medical University
FLUID RESUSCITATION USING ENTERAL ROUTE IS A SAFE AND EFFECTIVE ALTERNATIVE TO PARENTERAL RESUSCITATION
Background: A convenient and easy alternative to intravenous fluid administration is to give fluids through the normal functioning gut. Although not common, this practice has significance in mass causalities and some elective situations. This study determines the feasibility of enteral resuscitation as an alternative to standard intravenous therapy in hydration of patients having obstructive jaundice and its effect on endotoxemia.
Hypothesis: There is no difference in fluid resuscitation using the enteral route in comparison to Parenteral.
Methods: 60 patients with obstructive jaundice schedules for endoscopic biliary drainage were randomized into three equal groups A, B, and C. Group A received 4 L fluid via the enteral; group B received 4 L intravenously route over 48 h. Group C received no extra fluid other than usual oral liquid diet. Vital parameters, urine output, serum bilirubin, serum creatinine, creatinine clearance, electrolytes, and endotoxin levels were monitored.
Results: Significant improvement in blood pressure was observed in groups undergoing fluid resuscitation (groups A and B). None had any evidence of chronic kidney disease prior to intervention, and renal function remained normal post-intervention. The average urine output for group C was significantly less than other two groups. Febrile events and electrolyte abnormalities were found more in group B, however statistically insignificant. Significant decrease was observed in endotoxin concentrations in all groups, although the decrease was maximum in the enteral group (A).
Conclusions: In surgical obstructive jaundice undergoing endoscopic drainage, we found that adequate preoperative fluid resuscitation can be successfully achieved using the enteral route. Fluid given by the enteral route may be helpful in improving blood pressure, and reducing postoperative septic complications and endotoxemia.
KimPeterSullivanDeniseMcCallLathanPraneviciusMindaugas
Albert Einstein College of Medicine
REGIONAL ANESTHESIA ADMINISTERED BY A MULTI-DISCIPLINARY PAIN SERVICE REDUCES COLORECTAL SURGICAL INFECTIONS
Background: Surgical infections plague the management of colorectal surgery, with the incidence ranging from 10%–25%. Surgical site infections (SSI) and urinary tract infections after elective colorectal procedures increase morbidity, length of stay, readmissions, and cost. Poor pain control and the use of narcotics may induce immunosuppression and increase the risk of infections. Novel techniques are needed to reduce the high rates of post-operative infections associated with colorectal surgery, particularly SSI.
Hypothesis: We hypothesized that the management of peri-operative pain by a dedicated multi-disciplinary pain service (MDPS) using epidural anesthesia in addition to general anesthesia with daily pain evaluations would reduce infection rates, readmissions, and time to initiation of oral diet.
Methods: A retrospective review of elective, non-emergent, primary colorectal surgery cases from two municipal hospitals (Bronx, NY) were evaluated via electronic medical records. Usage of epidural and regional anesthesia techniques, peri-operative infections, readmissions, and time to initiation of oral diet were recorded from January 2009 to July 2011. Elective, non-emergent colorectal surgery cases that incorporated epidural anesthesia with post-operative management by the Anesthesia Pain service were defined as MDPS cases. Data were collected and compared using Chi-square univariate analysis.
Results: Sixteen of 70 (22.9%) cases of colorectal surgery performed without epidural anesthesia and MDPS resulted in a peri-operative infection. Specific infections included SSI (14), C. difficile colitis (2), bacteremia (1), and urinary tract (2). Only 1 of 22 (4.5%) cases performed with MDPS resulted in a SSI (Chi-square=4.2; p=0.04). Readmissions were reduced from 14% to 4.5% (Chi-square=1.7; p=0.19). There was no significant difference in time to initiation of oral diet.
Conclusions: Epidural anesthesia and management of peri-operative pain by a multi-disciplinary pain service may decrease the incidence of surgical infections and readmissions in colorectal surgery.
SnyderJasonThomasAlexandraKeibelLaurenPetrosyanMikaelNadlerEvanBurdRandallQureshiFaisal
Children's National Medical Center
TRANSUMBILICAL LAPAROSCOPICALLY-ASSISTED APPENDECTOMY (TULAA): A COST-EFFECTIVE PROCEDURE FOR APPENDICITIS IN CHILDREN
Background: Laparoscopic appendectomy (LA) is the preferred method for appendectomies in children. TULAA is an alternative method that reduces cost and affords similar minimally invasive benefits. However, the complication rate of TULAA, specifically surgical site infections (SSIs), is not clear. We compared clinical outcomes and costs associated with TULAA and LA.
Hypothesis: We hypothesize that TULAA will have comparable clinical outcomes to LA, and lower cost.
Methods: Single-institution, retrospective review of all appendectomies from FY09 to FY11 (n=743) was performed after IRB approval. LOS, operative time, and postoperative complications were collected. Material costs were obtained. Student t-test and Fisher exact test were used. p<0.05 was significant.
Results: There were 434 acute (58.4%), 274 perforated (36.9%), and 35 normal appendices (4.7%). 105 TULAA's, 610 LA's, 6 conversions, 7 open, and 15 interval appendectomies were performed. There were no differences in demographics, LOS, or operative time between TULAA and LA. Similarly, there were no differences in SSIS or post-operative complications (4.8% vs. 1.6%, p=0.056, 9.5% vs. 8.7%, p=0.71). We then compared TULAA and LA based on severity of appendicitis (Table). There were no differences seen, however, children undergoing TULAA for perforated appendicitis had a higher rate of SSI without being significant (8.3% vs. 1.3%, p=0.07). Material costs for TULAA were lower than LA ($628 vs. $1,025, p<0.05).
Acute TULAA
Acute LA
p-value
Perforated TULAA
Perforated LA
p-value
Number
78
352
24
230
Age
10.2 yrs
11.2 yrs
0.03
8.00 yrs
9.20 yrs
0.14
% Male
61.5
59.66
0.80
14 (58.3%)
150 (65.2%)
0.51
Operative Time
40.9 min
44.0 min
0.20
52.33 min
56.16 min
0.47
Length of Stay
1.63 days
1.91 days
0.27
5.08 days
4.78 days
0.70
Wound Infections (%)
3 (3.9%)
7 (2.0%)
0.40
2 (8.3%)
3 (1.3%)
0.07
Abdominal Abscesses (%)
1 (1.3%)
1 (0.3%)
0.33
3 (12.5%)
29 (12.6%)
1
All Post-op Complications (%)
5 (6.4%)
12 (3.4%)
0.21
5 (20.8%)
41 (17.8%)
0.78
Conclusions: TULAA is a viable cost-saving option for appendicitis in children, with no apparent difference in outcomes compared to LA. If all LA at our institution were done via TULAA, there would be a potential cost savings of $242,170 over 3 years. There is a higher, but not statistically significant, rate of SSI in perforated appendicitis with TULAA, and this will require further study.
KevorkianNoubarRennieChadWangHuaZhangHaidiAsarianArmandPappasPeter
The Brooklyn Hospital Center
SEVERE AND FULMINANT CLOSTRIDIUM DIFFICILE COLITIS AND THE TIMING OF SURGICAL INTERVENTION: A SYSTEMATIC REVIEW OF THE LITERATURE
Background: Colonization with Clostridium difficile presents clinically in a spectrum of severity ranging from asymptomatic carrier to severe and fulminant disease. Colectomy can be curative but carries a high mortality rate. Currently recommended indications for surgery include impending multiple organ failure and toxic megacolon. Patients presenting with these symptoms have high mortality rates after surgery, indicating the need for earlier intervention.
Hypothesis: Patient at high risk of disease progression based on demographic, clinical, and laboratory variables might have a survival benefit with surgical resection prior to developing signs of fulminant disease.
Methods: A systematic literature search was undertaken for the period 1990 to 2011 using Medline and Ovid databases with search terms C. difficile, pseudomembranous colitis, and colectomy. Primary studies were included for analysis. Variables associated with progression towards fulminant disease and prognoses were graded according to level of supporting evidence. A meta-analysis of the variables was carried out.
Results: Ninteen primary studies met our inclusion criteria; four were multi-center while the rest were single-institution investigations. No prospective, randomized, case-controlled study elaborating on an ideal time for colectomy was identified. Variables found to predict progression toward fulminant disease and higher mortality include: advanced age (p=0.006), elevated WBC count (p=0.0002), underlying co-morbidity, medications imparting immunosuppression (p=0.02), and multiple organ failure as evidenced by altered mental status and a need for vasopressor support (p=0.00001).
Conclusions: Owing to the nature of the disease, it is unlikely that a randomized, prospective, case-controlled study will be undertaken to determine an appropriate time for colectomy in severe and fulminant C. difficile colitis. Cose-to -deal timing can be achieved by identifying patients at risk of progression toward fulminant disease, close surgical follow-up, and limited tolerance for failure of medical therapy. The data available do not allow for statistical validation of many of the determinant variables hypothesized as being significant. Further studies are required in this regard.
ToKathleenCherry-BukowiecJillEnglesbeMichaelShijieCaiTerjimanianMichaelNapolitanoLena
University of Michigan
EMERGENT VS. ELECTIVE CHOLECYSTECTOMY: CONVERSION RATES AND OUTCOMES
Background: Laparoscopic cholecystectomy (LC) is the procedure of choice for treatment of cholelithiasis/cholecystitis. Conversion rates (CR) to open cholecystectomy (OC) are reported as 5–15% in elective cases, and up to 25% in patients with acute cholecystitis. We sought to examine the CR in a tertiary-care academic hospital and compare complications and outcomes in elective and emergency cholecystectomy.
Hypothesis: Conversion rates on the Non-Trauma Emergency (NTE) surgery service are higher than on elective general surgery services, and are associated with higher mortality.
Methods: Prospective data were obtained for cholecystectomy patients from: (1) the NTE database, which included all emergent cholecystectomies performed on the NTE service 1/1/2008–12/31/2009; and (2) Michigan Surgical Quality collaborative (MSQC) database with a random sample of 20–30% of all operations performed 1/1/2005–12/31/2010. Patient characteristics, CR, and outcomes were compared for emergent and elective cases.
Results: Of 1,708 NTE admissions, 1,202 patients required surgical intervention, and 279 patients (23%) underwent cholecystectomy [217 LC (77.8%), 16 OC (5.7%), 46 LC converted to OC (16.5%)]. NTE cholecystectomy patients were 65.6% female, mean age 45.4 years (18–91), with mean hospital length of stay (HLOS) 4.9 d. OC-HLOS was greater (4.0 LC, 7.9 LC to OC, 8.7 OC, p<0.001). Hospital mortality was 0.35% and CR was 17.5%. In the MSQC database, 772 patients underwent cholecystectomy, with 672 elective and 100 emergent cases. MSQC cholecystectomy patients were 67.4% female, mean age 47.5 y; mean OC-HLOS was greater (6.8 OC vs. 4.6 LC, p=0.006 T-test). Hospital mortality was 0.65% (0.6% elective, 1.0% emergent), and CR was 9.1% in elective cases and 14.9% in emergent cases. (See table at the top of page S-28.)
MSQC Cholecystectomy
Non-Trauma Emergency Cholecystectomy
Elective (672)
Emergent (100)
All n=279
LC n=217 (77.8%)
LC to OC n=46 (16.5%)
OC n=16 (5.7%)
LC n=557
OC n=115
LC n=80
OC n=20
Female Gender (%)
183 (65.6%)
154 (71%)
20 (43.5%)
9 (56.3%)
402 (72.2%)
52 (45.2%)
56 (70%)
10 (50%)
Mean Age, years (Range)
45.4±17.5 (18–91)
43.8±17.5 (18–91)
51.1±17.3 (19–85)
50.2±14.7 (26–74)
45.9±16.1 (18–92)
57.0±15.0 (19–85)
42.1±17.1 (18–93)
61.5±18.8 (26–94)
Mean Operative Time, minutes (Range)
169.0±61.3 (75–439)
156.7±51.9 (74–439)
216.7±63.3 (131–411)
199.1±93.8 (94–424)
96.7±39 (28–288)
155.9±65.3 (52–364)
109.6±39.0 (51–232)
140.8±40.5 (55–220)
Mean HLOS (days)
4.9±5.0
4.0±4.0
7.8±6.7
8.7±6.4
4.6±4.8
6.2±4.1
4.6±13
10.2±10.5
Morbidity (%)
–
–
–
–
2.53%
2.38%
5%
5%
Mortality (%)
1 (0.35%)
0
0
1 (6.25%)
0.3%
0.3%
1%
0
Conclusions: In NTE patients requiring cholecystectomy, CR is almost 2-fold higher [17.5% NTE vs. 9.1% elective (p=0.0041 Fisher)], but is lower than in previous published reports (25%), and is associated with longer operative times and HLOS but no difference in mortality.
KuoYen-HongKuoYen-LiangAhmedNasimDavisJohn
Jersey Shore University Medical Center
ALCOHOL ABUSE INCREASED MORTALITY ON PATIENTS UNDERGOING ELECTIVE COLECTOMY
Background: Excessive alcohol consumption affects the immune system. However, the impact from co-morbid alcohol abuse on the clinical outcomes of patients who undergo elective colectomy on a population basis are unknown. The purpose of this study was to assess the association between chronic alcohol abuse and the surgical outcomes of colectomy by using a population-based discharge database.
Hypothesis: Chronic alcohol abuse will increase the risk of in-hospital mortality for patients undergoing elective colectomy.
Methods: A retrospective cohort study was conducted to include adult patients (age≥18 years) who underwent elective colectomy during 2002–2006, using data from the U.S. Nationwide Inpatient Sample. The disease status and procedures were categorized according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The elective colon surgery group was comprised of patients with a primary diagnosis of diverticulosis of the colon without hemorrhage (ICD-9-CM codes: 562.11 and 562.12) or malignant neoplasm of the colon (ICD-9-CM codes: 153.x, where x represents the possible digits within this ICD-9-CM code category); with procedures of partial excision of the large intestine (ICD-9-CM codes: 45.7x), or total abdominal colectomy (ICD-9-CM code: 45.8) or intestinal anastomosis (ICD-9-CM codes: 45.9x). In-hospital mortality was the outcome of interest. Multiple logistic regression models were used to assess the association between chronic alcohol abuse with mortality while controlling for confounding factors.
Results: A total of 88,229 patients underwent elective colectomy. The overall in-hospital mortality rate was 1.15%. Patients with co-morbid alcohol abuse (0.98%) were younger (mean [standard deviation]: 62.2 [14.4] vs. 65.0 [12.2] years, p<0.00001), and less likely to be female (19.5% vs. 52.7%, p<0.00001). The overall mortality rate was higher (3.2% vs. 1.1%, p<0.00001) as compared with the patients without an alcohol abuse history. By multivariable logistic regression, history of alcohol abuse was significantly associated with increased mortality (odds ratio 3.63, 95% confidence interval 2.23–5.91], p<0.00001) when controlling for age, gender, diabetes mellitus, heart failure, and anemia.
Conclusions: This study demonstrated that patients with co-morbid alcohol abuse who undergo elective colectomy have a higher risk of in-hospital mortality.
AhmedNasimKuoYen-HongPhDDavisJohn
Jersey Shore University Medical Center
IMPACT OF TIMING OF LAPAROTOMY ON OUTCOME IN BLUNT COLO-RECTAL INJURY
Background: Blunt colo-rectal injuries are relatively uncommon. Computed tomography of the abdomen and pelvis can diagnose intra-abdominal injuries in most cases. However, in some cases the diagnosis can be challenging. Delay in diagnosis and management result in increased morbidity and mortality.
Hypothesis: There is no significant difference in terms of mortality or total length of hospital stay whether the patient underwent laparotomy within, or more than 4 h after, blunt colo-rectal injury.
Methods: A retrospective analysis from 2002–2008 was performed from a single Trauma Center registry. Patients admitted to the trauma center with a primary diagnosis of colo-rectal injury from a blunt mechanism were included in the study. Patients were then divided into two groups based on the timing of the laparotomy (≤4 h or >4 h). Patients' demography, clinical information, and outcomes were compared between groups. Data are summarized as mean±standard deviation, proportion, or percentage.
Results: Twenty-one patients were admitted with the primary diagnosis of blunt colorectal injuries. Fifteen of 21 (71%) patients underwent laparotomy within 4 h, and only six of 21 (29%) underwent laparotomy more than 4 h after admission. There were no significant differences between groups in terms of age (p=0.98), gender, injury severity score [ISS] (p=0.68), initial systolic blood pressure (p=0.06), or initial temperature (p=0.24). There was a significant difference in terms of total hospital length of stay (p=0.04). There was no significant difference of in-hospital mortality (p=0.2).
Conclusions: Timing of laparatomy did not have any significant impact on mortality. There was a significant difference in terms of total hospital length of stay.
Characteristics
Laparotomy </= 4 hours N=15
Laparotomy>4 hours N=6
p-values
Age (years)
29.6±0
29.8±6.67
0.98
Sex {Female}
26%
16%
1.0
ISS
17.93±0
20.5±9.40
0.68
Initial Initianl Systoloc Blood Pressure [mmHg]
101.46±0
140.16±23.41
0.57
Initial Temperature (F)
97.18±0
98.2±1.09
0.24
Total Hospital length of stay (days)
4.86±0
19.66±19.47
0.004*
In-Hospital Mortality
4/15
0/6
0.2
LawrenceJohn
University of Vermont
SURGICAL TREATMENT OF TYPHOID PERFORATION IN CHILDREN
Background: Typhoid fever is an illness caused by Salmonella enterica, serovar Typhi, which remains endemic in much of the developing world. The most common surgical complication is intestinal perforation, typically of the ileum. In children who present with overt peritonitis from perforation, surgical options have included primary repair of the perforation, resection of the diseased intestine with anastomosis, or diversion by creation of an intestinal stoma. While stoma creation may seem more practical in the face of peritonitis, the lack of access to intravenous nutrition and stomal appliances in the developing world, as well as the need for reoperation, make this approach very challenging. Conversely, the risk of leakage from repairs or following an anastomosis is also considerable in the setting of an ill child with diffuse peritonitis. Mortality for typhoid perforation remains high in this fragile population, regardless of the option selected.
Hypothesis: Surgical treatment of typhoid-induced ileal perforation in children can be optimized by primary repair of the perforation reinforced with an omental patch.
Methods: A retrospective chart review was performed of a single surgeon's experience over a three-month period in treating children with typhoid perforation of the ileum. The surgical technique employed consisted of exploratory laparotomy, lavage of the peritoneal cavity with saline, and repair of the perforation with interrupted sutures. All repairs were reinforced with an omental patch; broad-spectrum antibiotics were utilized both to treat peritonitis and the underlying causative infection. Parameters specifically assessed were age, length of hospitalization, associated complications, and survival.
Results: Four pediatric patients were treated for typhoid ileal perforation; ages ranged from 8 to 14 years. All patients survived and were discharged from the hospital. Although post-operative fever and prolonged ileus were common, the only major complication was in one patient, who developed a post-operative obstruction from adhesions requiring re-operation 51 days after his initial procedure. The average hospital stay was 26.6±7.2 days.
Conclusions: This small series suggests that in the surgical treatment of typhoid perforations in children in settings of limited resources, routine use of an omental patch to reinforce a site of primary repair may represent a means to optimize outcomes.
SweringenHeather VanOssKatherine VanAlexanderJ. WesleyEdwardsMichael
University of Cincinnati
INSTITUTIONAL OBSERVATIONS OF BACTERIAL COLONIZATION OF OPERATING ROOM SURFACES AND PERSONNEL ATTIRE
Background: Surgical site infections (SSI) are a significant source of morbidity and mortality amongst surgical patients. Standard measures have been implemented to minimize the transfer of organisms from operating room personnel to the patient. These measures include sterile gloves, gown, masks, and draping; and antiseptic cleansers used at the surgical site of the patient and for cleansing hands and arms of personnel. Operating rooms are cleansed to prevent transmission of organisms from case to case.
Hypothesis: We assessed the microbial densities on operating room surfaces and personnel attire at our institution in an effort to further delineate the effectiveness of decontamination at selected sites.
Methods: Petrifilm Aerobic Count Plates and Petrifilm Staph Express Count Plates (3M, St. Paul, MN) were used for sampling of different surfaces. Plates were made according to manufacturer's instructions and applied directly to the surface in question for sample collection. Plates were allowed to incubate for twenty-four hours and colony counts were assessed. Statistical analysis was performed using the Student t-test.
Results: A total of 518 samples were taken from flat surfaces and personnel attire in the operating room. Flat surfaces included anesthesia equipment, operating room equipment, and the floor, revealing overall low levels of bacterial growth, averaging <10 colony forming units (CFU)/20 cm2. Personnel attire, as expected, revealed higher levels of microbial contamination, with personal hats and uncovered shoes having the highest counts, averaging 50–60 CFU/20 cm2. When compared to disposable shoe covers and hats, there was a statistically significant difference in levels of microbial contamination (p=0.01 and p=0.02, respectively). Masks worn during operative procedures showed a low level of organisms present on the outside of the mask, averaging 25 CFU/20 cm2, although these levels were significantly less than both the staphylococcal and aerobic samples taken from the inside of the masks (p<0.01 for both).
Conclusions: Bacterial transfer from personal attire of staff in the operating room is a concern as a possible source for transmission to patients undergoing surgical procedures. Further research is necessary to determine the validity of interventions such as more tightly-fitted masks, changing masks after a set duration of time, or utilization of shoe covers and disposable caps over personal surfaces.
WangHuaSinghAwinderSuraniAleemGriffithLarryGoAlanAsarianArmandPappasPeter
The Brooklyn Hospital Center
SURGICAL SITE INFECTION (SSI) IN BREAST CANCER PATIENTS AND ITS IMPACT ON LONG-TERM SURVIVAL-A RETROSPECTIVE STUDY FROM A NEW YORK CITY COMMUNITY HOSPITAL
Background: The reported incidence of SSIs after surgery for breast cancer is between 3% to 15%. These rates are high compared to other clean surgical procedures.
Hypothesis: SSIS in post-operative breast cancer patients are related to surgery type and affect long-term survival.
Methods: This is a retrospective analysis of prospectively collected data from the cancer registry, from 1997 to 2010. SSI cases within 1 year after operation were identified using ICD-9-CM diagnosis codes for SSI and complications. The investigation was divided into two groups: non-SSI and SSI. Multiple factors were compared between SSI and non-SSI groups using SPSS. Survival probabilities were analyzed with Kaplan-Meier life table techniques using Epi Info. Univariate and multivariable analyses were performed to estimate hazard ratios using the Cox proportional hazard model.
Results: 1,244 breast cancer patients underwent surgery with 93 documented SSIs. The overall infection rate was 7.5%. Age at diagnosis was 58.74±16.19 years and 60.64±16.19 years in the SSI and non-SSI groups, respectively (p=0.211). No significant differences were observed in ethnicity, tumor histology grade, pathological stage, tumor location, tumor size, hormone receptor distribution, lymph nodes examined, lymph node positivity, co-morbidities, or hormone and radiation therapy between the groups. In the SSI group, a higher percentage of patients underwent a total or modified radical mastectomy (38.70% vs. 31.83% (p=0.003) in non-SSI group). Similarly, a higher percentage of patients received chemotherapy (11.24%, SSI vs. 5%, non-SSI, p<0.013). Kaplan-Meier analysis indicated significant differences in the 5- and 10-year survival rates (80.71% vs. 69.76%; 66.26% vs. 54.49% in the non-SSI and SSI groups, respectively (p=0.002). Cox proportional hazard ratio was 1.72 (95% CI 1.00–2.47).
Conclusions: Our data indicate that SSIs are associated with the type of surgery performed and post-operative chemotherapy administration. SSIs are associated with a decrease in survival. These data strongly suggest that immunosuppressed patients who develop an SSI will have higher mortality. Immune function should therefore be a consideration before the initiation of chemotherapeutic agents.
HedrickTraciSawyerRobertFrielCharles
University of Virginia
THE MORBIDITY OF A WOUND: DEFINING SURGICAL SITE INFECTION (SSI) IN COLORECTAL SURGERY
Background: Increasingly, SSI is being tied to quality and pay for performance parameters. However, the incidence of SSI following colon and rectal surgery varies widely. According to the national ACS NSQIP data, there is a 9% incidence of deep and superficial incisional SSI following colorectal surgery. However, many previous studies, including our own prior data, report the incidence to be much higher.
Hypothesis: We hypothesize that NSQIP underestimates the incidence of SSI following colorectal surgery.
Methods: Elective intra-abdominal colon and rectal procedures with a clean-contaminated wound classification performed at a single institution between January 1 and May 1, 2011 were queried. All cases were examined retrospectively by a single attending surgeon for the presence of a deep or superficial incisional SSI. These data were compared to the institutional NSQIP data with regard to deep and superficial SSI.
Results: Seventy-one cases met inclusion criteria. There were 6 SSIs identified by NSQIP, representing 8.4% of cases. Upon further review by the surgeon, 4 wounds were left to heal by secondary intention initially. Of the remaining 67 patients, there were 2 superficial SSI treated with antibiotics only, and 17 deep SSI that were opened and packed in the 30-day postoperative period, representing a 26.7% incidence of SSI. Lack of attending documentation and subjective differences in chart interpretation accounted for most discrepancies between surgeon and NSQIP SSI capture rates.
Conclusions: The definition of a SSI in colon and rectal surgery is subjective and difficult to discern from the medical record. Additionally, there are discrepancies in defining SSI between chart reviewers, even when applying CDC definitions. There is significant morbidity and increased health care cost incurred by care of the open wound, regardless of whether the patient meets strict CDC criteria for SSI when the wound is opened, or if the wound is left open initially. Given the discrepancy in defining SSI in colorectal surgery patients, it may be more logical to track the percentage of wounds that heal by secondary intention or require treatment with antibiotics following colorectal surgery rather than to rely on poorly reproducible and subjective definitions.
YuHollyMardekianJackSiuGordonZitoEdwardGirgentiDouglas
Pfizer, Inc.
STAPHYLOCOCCUS AUREUS INFECTION RATES AND RISK FACTORS ACROSS SEVEN INPATIENT SURGICAL SUBGROUPS IN THE UNITED STATES
Background: Postoperative S. aureus infection leads to adverse clinical and economic outcomes for patients. However, limited data are available comparing variances of S. aureus infection across multiple surgical subgroups.
Hypothesis: S. aureus infection rate varies widely across 7 major surgical subgroups and correlates strongly with baseline risk factors (e.g., co-morbidities).
Methods: The analysis used the 2009 Nationwide Inpatient Sample of 1,050 hospitals from 44 states, representing a 20% cross section of U.S. hospital admissions. The 7 surgical subgroups included cardiothoracic, vascular, general, gynecologic/genitourinary, neurosurgical, orthopedic, and plastic surgeries. S. aureus infection rates and risk factors associated with infection were estimated. Multivariable statistics adjusted for sampling weights, controlling for age, gender, race, payer source, co-morbidities, admission type, and hospital characteristics.
Results: In total, 6,894,989 admissions involved at least 1 of 7 surgical subgroups among patients age ≥18 years. S. aureus infection was reported as a discharge diagnosis in 61,783 admissions, or 0.90 per 100 admissions (95% CI 0.85–0.94). Fifty-one percent of all S. aureus infections were due to methicillin-resistant S. aureus (MRSA). For both S. aureus and MRSA, rates varied significantly across surgical subgroups. Major risk factors associated with infection included surgery types (Table), numbers of co-morbidities (odds ratio (OR)=1.66, 95% CI 1.62–1.69), and non-elective admissions (OR=3.23, 95% CI 2.98–3.51).
Surgical Subgroup
S. aureus Infection Rate (% of Admissions)
MRSA rate (% of S. aureus infections)
Odds Ratio for S. aureus Infection
Overall
0.90
50.71
N/A
Cardiothoracic
1.11
44.63
3.36 (2.87, 3.92)
Vascular
3.06
61.83
9.61 (8.30, 11.12)
General
1.13
54.43
4.20 (3.72, 4.75)
GYN/GU
0.12
56.34
Reference
Neurosurgery
1.86
38.61
13.21 (11.42, 15.29)
Orthopedic
0.35
48.28
2.42 (2.08, 2.81)
Plastics
5.42
54.03
32.41 (27.67, 37.96)
Conclusions: S. aureus infection rates vary significantly across surgical subgroups and are influenced by numbers of patient co-morbidities and emergent or non-elective patient status. Increased attention to effective infection control strategies should be considered for surgical subgroups with increased inherent infection risk and for individual patients at increased risk for infection.
AntoniouAlexanderFleshnerPhillipTowfighShirin
Tufts University
SURGICAL SITE INFECTION RATES ARE SIMILAR FOR LAPAROSCOPIC-ASSISTED AND OPEN COLORECTAL PROCEDURES
Background: One of the main benefits of laparoscopic surgery as compared to open surgery is reduction in surgical site infection (SSI). In colorectal surgery, SSIs are among the highest in general surgery. Laparoscopy has shown favor and the technique of laparoscopy-assisted colorectal surgery-using a hand-port or a laparotomy to perform part of the surgery-has gained popularity. No studies have analyzed differences in SSI between purely laparoscopic and laparoscopy-assisted colorectal surgery.
Hypothesis: Laparoscopy-assisted SSI rates are more comparable to open than purely laparoscopic procedures.
Methods: All patients undergoing colorectal procedures from October 2010–October 2011 were followed for 30 days postoperatively. SSIs were categorized as superficial, deep, or organ space. Patient factors analyzed included age, body mass index, wound classification, ASA class, diabetes, and smoking. Perioperative factors analyzed included operative time, temperature, glucose, length of stay, steroid administration, bowel preparation, antibiotic use, and blood transfusion. All operative reports were analyzed for operative technique.
Results: Of the 486 study patients, 287 (59%) were open, 181 (37%) were laparoscopy-assisted, and 18 (4%) were pure laparoscopic. SSIs developed in 75 patients (15%). The SSI rate is highest in the open group (18%) with a step-wise decrease in SSIs observed with lap-assisted (12%) and purely laparoscopic procedures (6%). Purely laparoscopic procedures had significantly lower SSI rates than open (p=0.047); however, SSI rates for laparoscopy-assisted procedures were not significantly different from open procedures (p=0.076). Purely laparoscopic procedures had only had superficial SSIs, with no deep or organ/space infections. No other patient or perioperative factor resulted in a significant increase in SSI except for perioperative blood transfusion (p=0.02).
Conclusions: This is the first report studying differences in SSI rates between laparoscopic and laparoscopic-assisted colorectal procedures. We show that laparoscopy-assisted colorectal procedures are similar to open procedures in their SSI rates (12.2% vs. 18.1%). Studies comparing outcomes in laparoscopic and open colorectal procedures should analyze laparoscopic and laparoscopy-assisted procedures separately to provide accurate risk stratification of the population.
CarterStaceyAwadSamirClappMarissaHicksStephanieAvellanedaAndresSubramanianAnurandaLiangMike
Baylor College of Medicine
SURGICAL SITE INFECTION (SSI) IN LAPAROSCOPIC VENTRAL HERNIA REPAIR (LVHR)
Background: Compared to open repair, LVHR is associated with fewer SSI. Few reports have documented factors that place patients at increased risk of developing SSI after LVHR.
Hypothesis: The aim of this study was to evaluate outcomes in patients with SSI following LVHR and identifying characteristics predictive of SSI.
Methods: From January 2000 to December 2010, 201 patients underwent LVHR (median age, 58 years) at two institutions. Clinical history, outcomes, satisfaction, late post-operative pain, and functional status (Activities Assessment Scale; AAS) were analyzed. Continuous data was analyzed using unpaired Student t-test; Fisher exact test was used to compare categorical data.
Results: Of the 201 patients who underwent LVHR, twenty patients (9.9%) had a SSI with a mean follow-up of 33 months (range, 7–134). Most of the SSI were superficial (n=18,90%), while two patients (10%) had deep or organ/space infections. The pre-operative characteristics were similar in both groups (SSI vs. no SSI), with the exception of prior abdominal operations in the SSI group (median 2 vs. 1, p=0.02). Neither the type of mesh used, a history of diabetes, nor tobacco use were associated with SSI. UTI (19% vs. 5%, p=0.01) and seroma formation (45% vs. 17%, p=0.006) were more common in the SSI group. Hospital stay was significantly longer for patients with SSI (5±2 days vs. 2±0.2 days, p=0.001). Patients with SSIs were more likely to develop eventration (75%) compared to patients without a SSI (46%, p=0.02); however, the recurrence rate and need for reoperation was similar between the groups. Patient satisfaction (8.1±0.3 vs. 6.5±0.7, p=0.03), cosmetic satisfaction (8.1±0.3 vs. 6.3±0.2, p=0.02), late post-operative pain scores (2.6±0.3 vs. 4.5±1.0, p=0.04), and overall AAS scores (15.0±1.2 vs. 20.0±3.3, p=0.17) were worse in patients with SSI.
Conclusions: Only the number of prior abdominal operations was predictive of SSI in LVHR (Figure). Urinary tract infections, seromas, and eventration were associated with SSI following LVHR.
MoffettJenniferAvellanedaAndresLiangMikeSubramanianAnuradhaAwadSamir
Baylor College of Medicine
MICROBIOLOGY OF SURGICAL SITE INFECTIONS (SSI) IN PATIENTS UNDERGOING STOMA REVERSAL
Background: SSI are common after stoma reversal (SR).
Hypothesis: The purpose of this study was to assess the microbiology profile, antimicrobial susceptibility, and adequacy of the pre-operative prophylactic antibiotic in SR.
Methods: A retrospective review was performed of all SR at a single institution from January 2005 until February 2011. The prophylactic antibiotic administered and the microbiology of cultures that were obtained were reviewed.
Results: 128 patients underwent SR. Forty-six (36%) patients had a SSI, of whom 25 patients (54%) were cultured. All patients received appropriate prophylactic antibiotics; 89% were given ertapenem. 26 microorganisms were isolated from the cultures obtained. Gram-positive bacteria were the most common pathogens identified (72%): of these, Enterococcus (50%: Enterococcus spp. 33%, VRE 6%, Enterococcus faecalis 6%, Enterococcus avium 6%) was the predominate isolate, follow by methicillin-resistant Staphylococcus aureus (MRSA, 27%), methicillin-sensitive S. aureus (MSSA,16%), and S. epidermidis (6%). Gram-negative bacteria were isolated in 32% of cultures. Of these, Pseudomonas spp. (38%) was the predominate isolate, follow by E. coli (26%), Proteus spp. (12%), Klebsiella spp. (12%) and Acinetobacter spp. (12%). In patients who received ertapenem, 36% of the isolated pathogens were resistant to ertapenem. In patients who received ertapenem for prophylaxis, there was a trend toward more SSI (36% vs. 21%, p=0.37) compared to patients receiving other prophylactic antibiotics.
Conclusions: Gram-positive pathogens were the most commonly isolated organisms in patients with SSI following SR. There is increased Enterococcus and MRSA with SR compared to other bowel procedures in which ertapenem was used as the prophylactic antibiotic (Table). In addition, Pseudomonas infections were also encountered. Ertepenem may not be the optimal prophylactic antibiotic for patients undergoing SR. This may be inherent to SR or related to prior ertapenem use. This warrants further investigation.
SinghAwinderWangHuaSuraniAleemGriffithLarryGoAlanAsarianArmandPappasPeter
The Brooklyn Hospital Center
SURGICAL SITE INFECTION IN COLORECTAL CANCER PATIENTS AND ITS IMPACT ON SURVIVAL-A RETROSPECTIVE STUDY FROM A NEW YORK CITY COMMUNITY HOSPITAL
Background: Colorectal surgery is associated with some of the highest rates of infective complications and surgical site infections (SSIs). The aim of this study was to assess the prevalence of SSI after elective operations for colorectal cancer, analyze factors associated with postoperative infections, and investigate the prognostic significance of postoperative infections on outcome of survival.
Hypothesis: SSIs in post-operative colorectal cancer patients are related to surgery type and have effects upon survival.
Methods: We performed a retrospective case-control study with subjects selected from a cohort of colorectal surgery patients from the cancer registry from 1997 to 2010. SSI cases within 1 year after operation were identified using ICD-9-CM diagnosis codes for infection and complication. The investigation was divided into non-SSI and SSI groups for data analysis. Risk factors between SSI and non-SSI groups were analyzed using SPSS. Survival probabilities were analyzed with Kaplan-Meier life tables using Epi Info. Univariate and multivariable analyses were done to estimate hazard ratios using the Cox proportional hazard model.
Results: 817 patients underwent surgery with 99 documented SSIs, for an infection rate of 13.79%. Age at diagnosis was 65.06±13.59 years and 67.44±12.84 years in the SSI and non-SSI groups (p=0.545). There was no significant difference in ethnicity, tumor histology grade, pathological stage, tumor location, tumor size, lymph nodes examined, positive lymph nodes, or radiation therapy between the groups. A higher percentage of hemicolectomies (57.58%) was observed in SSI group comparing with 50.4% in the non-SSI group (p=0.01); a higher rate of SSIs presented in patients with diabetes (21.43%) vs. those with no diabetes (9.15%) (p<0.002). The incidence of SSI was 11.24% in post-operative chemotherapy patients vs. 5% in non-chemotherapy patients (p<.001). Kaplan-Meier survival analysis demonstrated no significant difference in survival in SSI versus non-SSI in colorectal patients (p=0.67).
Conclusions: SSI in colorectal patients is associated with patients with diabetes and those undergoing hemi-colectomy or post-operative chemotherapy. Development of an SSI does not negatively affect survival.
PunchLaurieKhanMansoorStansburyLynnScaleaThomasHenrySharon
University of Maryland, R Adams Cowley Shock Trauma Center
ANATOMIC VARIATION IN THE INCIDENCE OF MONOMICROBIAL INFECTION IN NECROTIZING SOFT TISSUE INFECTION OF THE EXTREMITIES
Background: Necrotizing soft tissue infection (NSTI) is described as a predominantly polymicrobial infection (Type I), with Type II infections characterized by a single organism or a staphylococcal/streptococcal combination, limited to Group A beta-hemolytic Streptococcus. Methicillin-resistant Staphylococcus aureus (MRSA) is now recognized as an additional significant pathogen.
Hypothesis: The possible relationship between the microbiologic profile and anatomic location of the NSTI has not been widely explored.
Methods: We undertook a retrospective chart review of patients admitted from 2002–2009 to the Soft Tissue Service of our Level I trauma center who had upper extremity (UE) NSTIs requiring surgical debridement, and a smaller comparison group admitted from 2008–2009 with lower extremity (LE) NSTIs from 2008–2009. Surgical management, microbiology, co-morbidities, postoperative complications, and mortality were assessed using chi-square analysis with significance assumed at p<0.05.
Results: A total of 108 patients were identified, 65 with UE and 43 with LE NSTI. Overall mortality was 10.8% (12/108), with no difference between groups, and almost all (11/12, 91%) who died had myonecrosis. Amputation was required in 7/65 (11%) UE and 6/43 (14%) LE patients. Necrotizing cellulitis was present in 2/108 (1.9%) patients; necrotizing adiposities in 20/108 (18.5%); necrotizing fasciitis in 45/108 (41.2%); and myonecrosis, in 42/108 (39.9%). More advanced infection, in the form of myonecrosis, was more common in UE patients, 30/65 (46.1%) vs. 12/43 (27.9%) in LE (p=0.03). Overall, 59% (64/108) of patients had documented Type II infections. However, UE NSTI was associated with a higher incidence of Type II infection, 46/65 (70.1%) vs. 18/43 (41.7%) in LE (p=0.0014). In UE patients, the most common pathogens were Group A beta-hemolytic streptococci (17/65, 25%) and MRSA (15/65, 24%). Clostridium spp. was isolated from three UE patients but was not identified in the LE group. Recent intravenous drug use was reported by 24/65 (37%) UE patients but was not associated with an increased incidence of Type I or Type II infections or myonecrosis.
Conclusions: UE NSTI in our study was associated with an increased incidence of Type II infections, advanced tissue invasiveness, and a higher rate of Group A beta-hemolytic Streptococcus than has been previously reported. Further evaluation of the anatomical variation in the microbiology of NSTI is warranted.
WITHDRAWN
MetwalliOmarPhatakUmaLewDebbieEscamillaRichardKaoLillian
University of Texas-Houston
PRACTICING STAGED AMPUTATIONS IN DIABETICS: IS IT TIME FOR REVISION?
Background: Wound complications are common after amputations for diabetic foot infections.
Hypothesis: The goal of this study was to determine whether 1- or 2-stage below-the-knee amputations (BKAs) provide better outcomes in a population of medically underserved diabetic patients.
Methods: A retrospective chart review of 190 diabetic patients who underwent a BKA over a period of 52 months (January 2007 to April 2011) at Lyndon B. Johnson County Hospital in Houston, TX, was performed. Outcomes included mortality, surgical site infection, flap necrosis, and hospital length of stay. SPSS software (version 19) was used to perform descriptive, univariate and multivariable regression, and propensity score analyses.
Results: By univariate analysis, there were no significant differences in surgical site infections or flap necrosis between patients receiving 1-stage (N=63) or 2-stage (N=127) BKAs (20.6% vs. 26.8%, p=0.36). Despite the fact that sicker patients underwent single-stage BKA (Table), multivariable regression analysis revealed that ischemic heart disease was associated with a decreased risk of surgical site infection (OR 0.21, 95% CI 0.60–0.74, p=0.015), but that type of surgery had no effect (OR 1.41, 95% CI 0.68–2.91, p=0.36). There was no significant difference in the length of hospital stay. However, surgical site infections were correlated with longer lengths of stay (OR 9.184, 95% CI 5.593–12.775, p<0.001). Propensity score analyses could not be performed secondary to lack of sufficient overlap between the propensity score distributions.
Variable
Single Stage (n=63, %)
Two Stage (n=127, %)
P
Gender
Male
38 (60)
95 (75)
0.04
Female
25 (40)
32 (25)
Race
White
7 (11)
15 (12)
0.56
Black
23 (37)
45 (35)
Hispanic
32 (51)
67 (52)
Other
1 (2)
0 (0)
Smoker
38 (60)
64 (50)
0.20
Comorbidities:
Ischemic heart disease
20 (32)
19 (15)
0.01
Stroke
2 (3)
10 (8)
0.21
Chronic kidney disease
20 (32)
23 (18)
0.03
PVD
20 (32)
36 (28)
0.63
Hypertension
52 (83)
99 (78)
0.46
Previous amputation
36 (57)
65 (51)
0.44
Post-operative Outcome
Wound Infection
13 (21)
34 (27)
0.36
Flap necrosis
8 (13)
9 (7)
0.20
Mortality
1 (2)
1 (1)
0.61
Demographics, co-morbidities, and outcomes in 1-stage versus 2-stage BKAs.
Conclusions: There was no significant difference in the risk of surgical site infection, flap necrosis, or length of hospital stay with one vs. two-stage BKAs. Further prospective randomized trials are necessary to determine the optimal method of treatment for diabetic patients requiring amputation.
GordonIanResnickKarenWilliamsRussellWilsonSamuel Eric
University of California-Irvine
CAN POLYTETRAFLUOROETHYLENE (PTFE) REMNANTS BE LEFT AFTER REMOVAL OF INFECTED GRAFTS?
Background: PTFE vascular grafts for hemodialysis access have an approximately 10% risk for infection, and a lower risk with arterial bypass. Current practice is to remove all PTFE material when infected to avoid the risk of recurrent sepsis and exigent hemorrhage at the arterial anastomosis. Maintaining patency of the native artery when removing all PTFE can be technically challenging. Our practice has been to divide infected grafts close to the arterial anastomosis and oversew the remnant to patch the artery. We retrospectively examined results of this strategy in patients with graft infections who had remnants of PTFE left at the arterial anastomosis to determine if subsequent infection occurred.
Hypothesis: PTFE remnants can be safely left behind at the arterial anastomosis.
Methods: We reviewed electronic medical records of all patients at one hospital undergoing removal of infected PTFE grafts from 2000 to 2011. Operative, follow-up, and clinic notes and microbiology labs were reviewed for recurrent sepsis, anastomotic bleeding, or excision of the PTFE remnant.
Results: 32 patients were identified between 2000 and 2011 who had infected PTFE grafts removed. 1 patient had 3 separate graft infections, 7 had 2 graft infections, and 24 had only 1 graft infection. 28 grafts were arteriovenous dialysis shunts and 12 were arterial bypasses for lower extremity ischemia. For 16 arterial anastomoses the entire PTFE graft was removed, and in 28 a remnant of oversewn PTFE was left at the anastomosis. Positive cultures were present in 21 of 23 of the cases where PTFE was left at the arterial anastomosis. Mean follow-up was 31 months. Of the 28 cases with PTFE remnants, only 2 required further surgery. 1 patient bled at a radial artery anastomosis 16 days after closure with a PTFE margin and had the remnant removed and the artery ligated. A 2nd patient's incision dehisced 15 days after removal, exposing the brachial artery with a PTFE remnant patch. The wound was closed, with a vein patch used to replace the PTFE. In both cases no further intervention was required. Healing without subsequent intervention for recurrent graft infections was achieved in 26 of 28 (93%) cases where a PTFE remnant was attached to the artery.
Conclusions: Leaving PTFE remnants in continuity with arterial anastomoses during removal for infection can be safely performed. This management strategy is a reasonable option when reconstruction of the artery after complete graft removal is difficult or risky.
PhatakUmaLewDebbieEscamillaRichardKaoLillian
University of Texas-Houston
SURGICAL EXPLORATION IN PATIENTS WITH SUSPECTED NECROTIZING SOFT TISSUE INFECTION
Background: Operative exploration is still the gold standard for diagnosis of necrotizing soft tissue infections (NSTIs). However, reliable factors that can distinguish them from other severe soft tissue infections are unknown.
Hypothesis: The purpose of this study was to determine whether any distinguishing factors could identify patients who do not warrant surgical exploration to rule out a NSTI.
Methods: A retrospective review was conducted of prospectively collected data on patients who presented to a county hospital with a suspicion of a NSTI. Data were collected regarding patient demographics, co-morbidities, admission vitals and laboratory results, possible inciting events, and hospital course. The laboratory risk indicator for necrotizing fasciitis (LRINEC) was calculated for each patient sans C-reactive protein (CRP). SPSS software (version 19) was used to perform statistical analyses.
Results: Fifty-one percent of patients (25/49) had a NSTI as defined by the operating surgeon. Those with NSTIs had an increased length of stay (19.9±21.2 days vs. 7.4±3.2 days, p=0.01), received more operative interventions (3.8±3.3 vs. 0.5±1.0, p<0.001), and had an increased risk of death (16% vs. 4%, p=0.28). Of the non-NSTI patients, 14 received incision and drainage, 6 were explored, 2 were debrided, and 1 received amputation. Analysis of presenting characteristics did not reveal any significant distinguishing factors for NSTI. Radiologic studies such as plain film and CT scans also did not distinguish NSTIs.
Conclusions: Within a population of severely ill patients with soft tissue infections, there were no distinguishing presenting factors for NSTIs. In patients with suspected NSTI, surgical exploration is still indicated, particularly as an operative intervention may still be warranted. The definition of an NSTI may also need to be refined given the overlap with other severe soft tissue infections.
NSTI (n=25)
Non-NSTI (n=24)
P
Age
48.39±12.07
49.48±9.14
0.73
Admission Vitals:
Systolic BP (N=48, NSTI n=27)
121.41±25.87
133.57±27.95
0.12
Diastolic BP (N=48, NSTI n=27)
66.67±15.55
76.90±17.59
0.04
Heart rate
101.64±24.72
105.48±20.62
0.57
Respiratory rate (N=47, NSTI n=27)
20.11±4.54
23.20±12.54
0.24
Temperature (C)
37.21±0.87
37.63±1.04
0.13
Presentation Labs:
WBC
16.93±8.98
12.98±5.05
0.08
Sodium
131.82±5.96
133.48±5.69
0.33
Sodium (adjusted for glucose)
133.34±6.03
134.72±5.28
0.41
BUN
26.75±20.23
23.14±15.67
0.50
Creatinine
1.62±1.15
1.51±0.85
0.72
Glucose
194.79±137.53
177.33±114.94
0.64
Lactic Acid (N=25, NSTI n=15)
3.58±3.38
3.79±2.43
0.87
Base Deficit (N=9, NSTI n=6)
−5.00±7.127
−3.33±4.16
0.72
LRINEC (no C-reactive protein)
3.82±2.18
3.43±1.86
0.51
Presenting factors in patients with NSTI versus non-NSTI.
WITHDRAWN
WITHDRAWN
AhmedNasimKuoYen-HongKuoYen-LiangDavisJohn
Jersey Shore University Medical Center
TREND AND OUTCOME OF NECROTIZING FASCIITIS
Background: Necrotizing fasciitis (NF) is a rare but rapidly progressing soft tissue infection. It is associated with very high morbidity and mortality if emergent surgical debridement is not performed. The purpose of the study was to evaluate the trend and outcome (mortality) of NF using the National Inpatient Sample (NIS) database.
Hypothesis: The trend and the mortality associated with NF would be increased over the period of time.
Methods: A retrospective cohort analysis was performed using NIS databases. Patients who were admitted for treating NF during 2000–2006 were identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code of 728.86 as the primary diagnosis. Incidence and mortality were the outcomes of interest. Linear regression was used to evaluate the linear trend over the years.
Results: In 2000, the weighted national discharge was 4,604 patients. The number reached the peak at 6,010 in 2004 (Figure). There was no linear trend over the years (p=0.28). When the weighted mortality rates were estimated, the highest one was 11.80% in 2005. It reached the lowest rate of 6.02% in 2006. There was a significant linear trend to reduction over the years (-0.85% per year, p=0.03).
Conclusions: The in-hospital mortality rates of treating necrotizing fasciitis reduced over the studied years.
WITHDRAWN
GuidryChristopherRosenbergerLauraHranjecTjasaDaviesStephenMcLeodMatthewPolitanoAmaniRiccioLinSawyerRobert
University of Virginia
VARIATIONS IN ISOLATED ORGANISMS OF BLOOD STREAM INFECTIONS OVER TIME
Background: Blood stream infections (BSI) are a common source of morbidity and mortality for hospitalized patients.
Hypothesis: We hypothesized that the proportions of bacteremia from gram-positive (GP) and fungal pathogens would decrease while rates of gram-negative (GN) bacteremia would increase.
Methods: All CDC-defined blood stream infections occurring in patients treated on the general surgery and trauma services were retrospectively identified between January 1, 1998 and December 31, 2009 at our institution. These cases were divided into four equal time periods each consisting of 3 years (ex.1998–2000) to compare rates of infection over time. Fisher Exact test was used for analysis of infection rates.
Results: 1,453 cases of blood stream infections were identified during the study period. Rates of infection based on organism class are provided in the table. Rates of infection from GP organisms decreased (p<0.0001) while rates of fungal and GN infections increased (p<0.0001 for fungal; p=0.021 for GN). Overall mortality, APACHE II score, and length of stay were unchanged.
Conclusions: While our hypothesis was only partly confirmed, over the last 12 years our institution has witnessed a shift in the types of organisms causing blood stream infections. We have identified a decrease in the rates of BSI from GP pathogens with an associated increase in the rates of BSI from fungal and GN pathogens. We believe that decreased overall rates of catheter-related BSI (e.g., due to increased sterile catheter care, improved site choice) may cause an associated decrease in GP BSI, although we are unable to demonstrate this association at this time. While we may consider a decrease in the rate of catheter-related BSI to play a role in this shift, the exact cause is a matter of further clinical investigation.
Organisms
1998–2000
2001–2003
2004–2006
2007–2009
p-value
Isolated (Total)
395
437
370
444
GP
253 (64.1%)
255 (58.4%)
219 (59.2%)
212 (47.7%)
>0.0001
Fungal
20 (5.1%)
50 (11.4%)
42 (11.4%)
60 (13.5%)
>0.0001
GN
110 (27.8%)
128 (29.3%)
97 (26.2%)
157 (35.4%)
0.021
MooreLauraDipasupilEdmundoHolcombJohnKozarRosemary
The University of Texas-Houston
VENTILATOR-ASSOCIATED PNEUMONIA (VAP) IN THE ELDERLY TRAUMA PATIENT: THERE'S NO PLACE LIKE HOME
Background: The aging of the population has led to an increase in the number of elderly trauma patients (pts). The development of infection has been linked to cognitive impairment & functional disability in the elderly. The impact of infectious complications in elderly trauma pts, specifically VAP, has not been evaluated.
Hypothesis: We hypothesized that elderly trauma pts with VAP would have worse outcomes than their younger counterparts.
Methods: Infection Control data was used to identify all VAP in pts admitted to our Trauma Intensive Care Unit (STICU) from 8/01/03 to 05/31/11. Demographics, mechanism, injury severity score (ISS), hospital (HLOS) & ICU length of stay (ILOS), discharge status, and mortality were obtained for all pts using local trauma registry data. Pts were divided into two groups: Age<65 y& age≥65 y. Data are expressed as mean±standard deviation (SD). χ2 was used to compare the two groups, p≤0.05 significant.
Results: During the study period, 6,116 trauma pts were admitted to our STICU. Of these, 5,428 were <65 y & 688 were ≥65 y. VAP occurred in 142 pts. The average age of the study cohort was 40.6 (±19.26) & the averageinjury severity score (ISS) was 30.3 (±13.6). Males accounted for 76%, and 86% had a blunt mechanism. Outcomes data of the groups are listed in the table. Mortality for all STICU admissions <65 y was 8.3%, and 19.7% for pts ≥65 y (p<0.001). There was no difference in the % male, % blunt, VAP incidence or ILOS between groups. Elderly pts had a lower ISS but a higher mortality than younger patients (p<0.05). Pts≥65 y with VAP had a higher mortality than pts ≥65 y without VAP (36.8% vs. 18.8%, p=0.07). Elderly pts were less likely to go home or to rehab, and more likely to go to a long-term acute-care (LTAC) or skilled nursing (SNF) facility as compared to younger pts.
Conclusions: Elderly trauma pts who develop VAP have higher mortality rates despite lower ISS than their younger counterparts. The majority of elderly trauma pts with VAP were discharged to an LTAC or SNF, suggesting that long-term functional recovery may be poor. Additional study of the long-term outcomes of this population is needed.
KunacAnastasiaSifriZiadMohrAliciaLaveryRobertLivingstonDavid
University of Medicine and Dentistry of New Jersey-New Jersey Medical School
10-YEAR REVIEW OF ISOLATED SEVERE TRAUMATIC BRAIN INJURY (TBI); WHAT IS THE IMPACT OF VERY EARLY TRACHEOSTOMY?
Background: Pneumonia rates in head-injured patients requiring mechanical ventilation are high, yet the Centers for Medicare and Medicaid Services (CMS) has suggested that hospital-acquired pneumonia (HAP) should not be reimbursed. Early tracheostomy (trach) has been recommended to decrease pneumonia (PNA) rates in patients with severe TBI.
Hypothesis: We hypothesized that very early trach compared to standard trach times in patients with isolated severe TBI would decrease HAP rates, but would not impact community-acquired pneumonia (CAP).
Methods: 10-year retrospective review of trauma patients admitted to the ICU with isolated severe TBI (head abbreviated injury score (AIS)≥4, no other AIS>1). Timing of trach was defined as very early: days 0–3; early: days 4–6; standard: day≥7. PNA was defined as a documented PNA along with positive respiratory cultures (BAL with ≥104 organisms or tracheal aspirate with many organisms plus neutrophils). Demographics, duration of mechanical ventilation (MV), ICU and hospital length of stay (LOS) were collected. CAP occurred in the first 72 hours post-admission, and HAP day 4 and beyond. A student t-test or chi-square test was used as appropriate.
Results: A total of 115 patients with isolated severe TBI underwent trach from 1/01–12/10. PNA rate was 68% (CAP 24%, HAP 44%). All 3 groups had a similar GCS (7.8) and head AIS (4.7) on admission. Incidence of CAP was similar regardless of timing of trach. Those who underwent a standard trach day ≥7 trended toward a higher rate of HAP and a longer duration of MV compared to those who underwent early or very early trach. There was no significant difference in LOS or mortality among the 3 groups.
Conclusions: Patients with isolated severe TBI requiring trach had a very high overall PNA rate (68%). CAP rates in this patient population were 24% and were independent of timing of trach, but patients who underwent very early trach (day 0–3) trended towards lower rates of HAP compared to standard timing of trach. Those who underwent very early trach also benefited from earlier liberation from MV but not shorter ICU or hospital LOS. Prospective studies are needed to confirm if very early trach in patients with severe TBI can significantly reduce HAP.
Timing of Tracheostomy
MV M (95% CI)
CAP %
HAP %
ICU LOS M (95% CI)
H LOS M (95% CI)
Day 0–3 N=26
9 (6–13)
27%
31%
16 (11–20)
29 (22–36)
Day 4–6 N=53
11 (10–12)
27%
43%
14 (12–17)
33 (20–45)
Day≥7 N=36
15 (13–17)*†
16%
53%††
18 (15–20)
32 (27–38)
*P<.05 vs. Day 0–3
P=NS
††P=.053 vs. Day 1–3
P=NS
P=NS
†P<.05 vs. Day 4–6
McLeodMatthewSawyerRobertRosenbergerLauraHranjecTjasaPolitanoAmani
University of Virginia
IN-HOSPITAL INFECTIONS FOLLOWING TRAUMATIC SPLENIC INJURY: DOES MODE OF MANAGEMENT MATTER?
Background: Splenectomy is associated with a low life-long risk of overwhelming post-splenectomy infection. Thus, the management of traumatic splenic injury has continued to evolve into less invasive interventions such as embolization and bed rest.
Hypothesis: We hypothesized that the rate of in-hospital infection in splenectomized patients is greater than those undergoing embolization or bed rest.
Methods: All traumatic splenic injuries involving significant parenchyma injury (grade II to V) were identified from January 2001–September 2010. Cases were divided into three treatment cohorts: splenectomy (SPL), embolization (EMB), and bed rest (BR). Chi-square analysis compared infection rates among the three groups.
Results: 263 severe traumatic splenic injuries were identified. The highest rate of infection was seen after SPL, followed by BR, then EMB (Table, p-values: SPL versus EMB=0.01, SPL versus BR=0.07, and EMB versus BR=0.18). The most common site of infection was the lungs, and the most commonly isolated organisms within SPL and EMB were E. coli, S. epidermidis, and S. aureus. The most commonly identified organisms in BR were E. coli and E. faecium.
Demographics and Outcomes after Traumatic Splenic Injury
Management
Splenectomy n=83
Embolization n=29
Bed rest n=151
ISS (mean)
32+/−13
27+/−12
24+/−10
APACHE II
18.2+/−1.6
18.2+/−0.9
14.1+/−1.2
Infections
36 (43%)
5 (17%)
47 (31%)
Transfused prior to infection
30 (83%)
2 (40%)
34 (72%)
Conclusions: Splenectomy was associated with the greatest risk of in-hospital infection, and embolization was associated with fewest infections. In-hospital infection rates are potentially associated with parenchyma loss as well as other interventions. A prospective study is needed to confirm that early embolization can lead to fewer in-hospital infectious complications after traumatic splenic injury because of the preservation of splenic parenchyma and the avoidance of transfusions and bed rest.
ContiDavidSiparskyNicoleColaneriJeannieDellehuntRachelGallichioMichael
Albany Medical College
ASSOCIATION OF LEWIS BLOOD-GROUP PHENOTYPE WITH RECURRENT URINARY TRACT INFECTION IN WOMEN TRANSPLANT RECIPIENTS
Background: Urinary tract infection (UTI) is a frequent complication in women after transplantation. Blood group antigens, found on the surface of urothelial cells, affect bacterial adherence and UTI susceptibility. In the general population, women with Lewis phenotypes, Le (a+b-) and (a-b-) are at increased risk for recurrent UTI compared to women of the Le (a-b+) erythrocyte phenotype. This association has not been studied in transplant recipients with multiple risk factors for UTI.
Hypothesis: Lewis antigens are not synthesized by erythoblasts, but rather by epithelial organs and kidneys and adsorbed onto the erythrocytes. Thus, the donor phenotype may affect Lewis antigen expression on urothelial cells of the recipient and UTI susceptibility. We analyzed the impact of recipient and donor Lewis phenotype on the UTI rate in women transplant recipients.
Methods: Between 1/1/03 and 12/31/10 renal transplants were performed in 152 women at our center. Recipient and donor Lewis phenotypes and UTI data were collected retrospectively. UTI was defined as 100,000 cfu/mL on urine culture with either fever, chills, dysuria, pyuria, or transplant tenderness.
Results: Overall, a single UTI developed in 63/152 women (41%), with 35 women (23%) suffering recurrent UTI. Results based on recipient Lewis typing is as follows: In the 100 recipients who were Le (a-b+), a single UTI developed in 43 (43%) with 25 (25%) suffering from a recurrent UTI. The incidence of a single UTI (38%) and recurrent UTI (19%) were similar in the 52 women who were Le (a+b-) or (a-b-), p=NS. Analysis of UTI results based on donor Lewis typing revealed different results. In 101 women who received a kidney from a Le (a-b+) donor, 37 (37%) developed a single UTI and 17 (17%) recurrent UTI. This compared to an incidence of single UTI 51% (p=0.14) and recurrent UTI 35% (p=0.02) in 51 recipients of a Le (a+b-) or (a-b-) donor kidney.
Conclusions: UTI is a frequent complication in women after renal transplantation. Recipient Lewis phenotype is not a risk factor for UTI. However, donor phenotypes of Le (a+b-) and Le (a-b-) are associated with a trend towards an increased rate of single UTI and a significantly increased risk of recurrent UTI. Our data indicate that aggressive screening or prophylactic measures are indicated in these high-risk patients to prevent the untoward consequences of recurrent UTI.
DaviesStephenGuidryChristopherPolitanoAmaniRosenbergerLauraMcLeodMatthewHranjecTjasaSawyerRobert
University of Virginia
ASPERGILLUS INFECTIONS IN TRANSPLANT AND NON-TRANSPLANT SURGICAL PATIENTS
Background: Aspergillus infections are associated with immunocompromised states, such as transplantation, and hematological malignancy. Although Aspergillus infections occur primarily in transplant recipients among surgical patients, they are occasionally found in non-transplant recipients and may be associated with mortality.
Hypothesis: We hypothesized that Aspergillus infections in non-transplant patients are not uncommon, are associated with critical illness, and mortality is similar to that within transplant patients.
Methods: Retrospective analysis of a prospective database from 1996–2010 was performed. Institutional review board approval was obtained. Patients with cultures positive for Aspergillus were identified. Demographics, co-morbidities, and outcomes (death, total days of antibiotics, and hospital length of stay) were compared between non-transplant and transplant recipients (with approximately 150 transplants/year in our center). Continuous data were evaluated using the Student t-test. Categorical data were evaluated using chi-square analysis.
Results: Twenty-three patients were identified as having Aspergillus infections (11 transplant patients and 12 non-transplant patients). The transplant patients included: 1 kidney, 2 kidney/pancreas, and 8 liver recipients. The two groups were similar regarding patient demographics and co-morbidities, with the exception of APACHE II score (transplant 23.6±8.1 vs. non-transplant 16.8±6.1, p=0.03), Acute Physiology Score (16.6±8.3 vs. 9.2±4.1, p=0.02), steroid use (91.0% vs. 25.0%, p=0.003), and percentage of infections acquired in the ICU (27.3% vs. 83.3%, p=0.01). The most common site of infection in both groups was the lung. There was no significant difference in the number of days from admission to treatment (16.7±19.8 vs. 19.0±14.6, p=0.76) or hospital length of stay following treatment (33.3±39.5 vs. 38.8±49.0, p=0.77). There was no significant difference in mortality between the groups (54.5% vs. 33.3%, p=0.41).
Conclusions: Although Aspergillus infections among surgical patients have been historically associated with solid organ transplantation, our data suggest that others may also be significantly susceptible, especially those that are ventilated, within the ICU, or hospitalized for prolonged duration. Surgical intensivists should be familiar with the diagnosis and treatment of Aspergillus infections even in the absence of an active transplant program.
DavisJohnKuoYen-HongPhDAhmedNasimKuoYen Liang
Jersey Shore University Medical Center
CHANGES IN THE POSTOPERATIVE INFECTIOUS PATHOGENS BETWEEN 2001 AND 2006
Background: Postoperative infections cause an increased length of hospital stay resulting in wastes of valuable healthcare resources. Efforts have been devoted to reduce the preventable infections. However, postoperative infection rates remian increased in the past years.
Hypothesis: The purpose of this study was to characterize the change in the postoperative infectious pathogens.
Methods: A survey of postoperative pathogens was conducted by using the 2001 and 2006 Nationwide Inpatient Sample. Adult patients (age≥18 years) who underwent elective colectomy and had a postoperative infection were the population of interest. The disease status and procedures were categorized according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). A postoperative infection was defined as a patient with the ICD-9-CM code of 998.59. The corresponding infectious pathogens were also identified. The chi-square test was used to compare the distributions between two different time periods.
Results: A total of 347 postoperative infections were reported in 2001 (171 [49%] from teaching hospitals; 176 from non-teaching hospitals), while 465 incidents were reported in 2006 (262 [55%] from teaching hospitals; 211 from non-teaching hospitals). Among the infections occurring in teaching hospitals, 119 of 171 (70%) did not report the corresponding infectious pathogens in 2001, and 198 of 262 (76%, p=0.21) did not report in 2006. When considering only those patients with a reported infectious pathogen, Unspecified Septicemia NOS (ICD-9-CM: 038.9) increased 22%, followed by Other Staphylococcus (ICD-9-DM: 041.19, 3%), and Other Specified Septicemias (ICD-9-CM: 038.8). For the non-teaching hospitals, 113 of 176 (64%) did not report a corresponding infectious pathogen in 2001, and 132 of 211 (63%, p=0.82) did not report in 2006. When considering only those patients with a reported infectious pathogen, the Unspecified Septicemia NOS (ICD-9-CM: 038.9) increased 13%, followed by the Clostridium difficile Pseudomembranous Colitis (ICD-9-CM: 008.45, 5%) and Streptococcal Septicemia (ICD-9-CM: 038, 3%).
Conclusions: This study identified the infectious pathogens that may be associated with the high incidence of postoperative infection. The patterns were different between teaching and non-teaching hospitals.
RodriguezCarlosDunneJamesTribbleDavidWellsJustinFlemingMarkWarkentienTylerWeintrobAmyMaloneDebra
Walter Reed National Military Medical Center
TRIALS AND TRIBULATIONS; THE EXPEDITED DEVELOPMENT OF AN INVASIVE FUNGAL INFECTION (IFI) CLINICAL PRACTICE GUIDELINE (CPG)
Background: From Jul09–Nov11, IFI was suspected or identified in 75 of 2,755 casualties admitted to a U.S. military medical center. In Jul09 an autopsy determined a patient's death to be from disseminated angioinvasive Aspergillus terreus. This index case alerted us to the possibility that other cases may follow. After 3 successive IFI patients, our first hospital-based CPG was instituted. Since that time, our surgical pathologists gained expertise at optimizing histopathological fungal detection methods, decreasing turn-around times, and optimizing clinical mycology methods to isolate and identify species. The CPG targets soft tissue and intra-abdominal IFI. Risk factors for IFI were assessed; minimization of risk was emphasized. IFI-specific pharmaceutical and non-pharmaceutical treatments are included in the CPG.
Hypothesis: Trauma-associated IFI in previously immunocompetent patients is associated with a reported mortality rate of 25%. Recently case reports are being published more often in the trauma literature. Providing an IFI CPG with supportive data will help update and standardize methods to diagnose and treat IFI, leading to better patient outcome.
Methods: In addition to review of electronic health records, interviews with clinicians involved in the development of the IFI CPG were utilized to describe its development. Clinical, pathological, microbiological, and pharmacological data were reviewed to characterize affected patients. Predefined IFI case definitions modified from the European Organization for Research and treatment of Cancer (EORTC)/National Institute of Allergy and Infectious Diseases Mycoses Study Group (MSG) Consensus Group were used to classify infection status.
Results: All patients with IFI (meeting case criteria or suspected) were male with a mean age of 24 y and injury severity score (ISS) of 23. Mortality rate was 4%; mean ICU LOS was 13 days; mean HLOS, 48 days. More than one-half the patients (42/75, 56%) met histological criteria for IFI. IFI was suspected in 44% of patients clinically; however never proved by histology (gold standard for IFI diagnosis). Changes in surgical practice as related to treatment of non-necrotic tissue abnormalities may have led to improvement in tissue salvage.
Conclusions: IFI is a deadly resource-intensive disease to combat. Use of our CPG may have led to better outcomes in our patient population; however weaknesses still exist and maturation of the CPG must progress as our experience continues. Significant diagnostic challenges persist and better diagnostic tools must also be developed.
HranjecTjasaRosenbergerLauraPolitanoAmaniRiccioLinMcLeodMatthewGuidryChristopherDaviesStephenSawyerRobert
University of Virginia
WHAT IS THE PROGNOSTIC VALUE OF LEUKOCYTOSIS IN SURGICAL INFECTIONS?
Background: Elimination or treatment of physiologic stressors including bacterial infections; myocardial, pulmonary or cerebral infarctions; neoplasms, traumatic injuries and many others, results in normalization of leukocyte count within days.
Hypothesis: We hypothesized that persistent leukocytosis (despite treatment) may be predictive of secondary infections and would result in worse outcomes, mainly mortality.
Methods: Data collected prospectively at a single tertiary care center were analyzed retrospectively for all surgical patients admitted from 12/96 to 09/10 and followed until hospital discharge. Reference range for normal white blood cell (WBC) count was 4–11 k/μL. Univariate (chi square, Student t-test, Mann-Whitney U) and multivariable analysis (logistic regression) were used to evaluate the data.
Results: A total of 5,846 patients acquired 13,054 infections over the 14-year study period. Mean maximum WBC count for non-survivors was higher at 16.8±0.3 as compared to 13.9±0.1 for survivors, p<0.0001. Overall, 1,496 (11.5%) infections were followed by death with persistent leukocytosis carrying a 1.8-fold (95% CI 1.7–1.9) increased unadjusted risk of dying, and persistently low leukocyte count carrying 1.1 (1.1–1.2)-fold increased mortality as compared to patients with normalized leukocyte count. After adjusting for age, gender, location of acquired infection (ICU, ward, home), trauma involvement, APACHE II score, and site of infection, persistent leukocytosis was associated with almost 4-fold increased risk of death (OR 3.96, 95% 3.3–4.7). Shorter time to leukocyte normalization was associated with improved outcomes (5.1±0.1 for survivors vs. 6.1±0.3 for non-survivors, p<0.004) and was seen most frequently in patients who did not develop a secondary infection: 3.9±0.1 days for patients without vs. 7.8±0.2 days for patients with secondary infection, p<0.0001.
Conclusions: Persistent leukocytosis or leukopenia and prolonged time to WBC normalization in surgical patients may be a sign of ongoing stress response, which ultimately results in patient demise. Furthermore, if WBC count does not normalize within 8 days (on average), there is a significantly higher association with a second infection.
Cherry-BukowiecJillRaghavendranKrishnanBrierleyKristinParkPaulineNapolitanoLena
University of Michigan
HEPCIDIN AND ANEMIA IN SURGICAL CRITICAL CARE
Background: Anemia is common in ICU patients and the pathophysiology is “anemia of inflammation” resulting in impaired iron regulation and reduced rate of erythropoiesis. Hepcidin, a hepatic peptide, is the key regulator of iron homeostasis, and is decreased by iron deficiency & tissue hypoxia. Hepcidin is upregulated by iron excess and inflammation, resulting in iron sequestration in macrophages and anemia. We sought to investigate hepcidin concentrations in critical care.
Hypothesis: Critical illness-induced inflammation induces high hepcidin concentrations resulting in suppressed erythropoiesis and anemia.
Methods: Prospective cohort study of anemic ICU patients. Exclusion criteria included pre-existing anemia, use of erythropoietin (EPO), immunosuppressant or cytotoxic drugs, renal failure requiring renal replacement therapy, and pregnancy. Time-dependent changes in serum hepcidin (validated competitive ELISA) were performed and correlated with hemoglobin/hematocrit (Hb/Hct), degree of anemia, and inflammatory response measurements.
Results: ICU patients (n=80) were 80% male, mean age 58.6±15.5 y, admission mean APACHE 14, mean SOFA score 4.5, mean MOD score 2.2, mean ICU & hospital LOS were 4.38 and 8.2 days. Transfusion was required in 17 (21%) pts ( mean 2 units). 30-day mortality was zero. Infections were present in 14 (17.5%) pts (2 pneumonia,1 sepsis, 6 UTI,1 C. difficile, 6 surgical site infections). Mean serial hepcidin serum levels decreased on day 3 by 32% and on day 7 by 42% from baseline (p=0.004 by repeated measures ANOVA) associated with a 2-fold increase in reticulocyte count (p=0.007) and a decrease in IL-6 levels (p=0.02). EPO and Hgb/Hct did not change. Hepcidin was correlated with IL-6 and IL-12.
Conclusions: Hepcidin concentrations are increased on ICU admission, and decrease over the ICU stay. Decreased hepcidin concentrations are associated with increased reticulocyte response and decreased inflammatory response reflected by decreased IL-6 concentrations, but not with anemia resolution.
Mean
SD
Range
Normal Range
Correlation with Hepcidin
Iron ug/dL
75.31
50.79
10–248
33–150 μg/dL
−0.287543109
TIBC ug/dL
242.49
42.28
129–362
220–440 μg/dL
−0.293996383
Ferritin ng/mL
254.24
268.86
9.3–1554.4
18–320 ng/mL
0.477953692
Folate ng/mL
13.09
5.18
3.4–23.6
>3.0 ng/ml
−0.124302696
Vit B12 pg/mL
432.41
231.84
108–1562
211–911 pg/mL
−0.121111209
TSF mg/dL
186.42
43.79
77–320
168–348 mg/dl
−0.328019367
CRP mg/dL
4.41
5.59
0.1–27.9
0.0–0.6 mg/dL
0.28794499
EPO
64.86
80.48
6–524
2–29 mU/mL
−0.068573792
Retic %
1.33
0.51
0.51–3.41
25.60–104.00 B/L
−0.125862837
Hgb g/dL
10.12
1.33
7.2–12.3
13.5–17.0 g/dl
−0.002795194
Hct %
29.39
4.12
20.7–36.2
40.0–50.0 %
−0.085575309
Hepcidin
195.245
175.96
10.01–1366.36
17–286 ng/ml
–
IL-4
0.39125
0.19
0.01–0.89
0.01–3.00 pg/ml
−0.150362759
IL-6
49.09
42.61
1.51–180.71
0.02–9.00 pg/ml
0.348380884
IL-8
21.54
56.24
0.81–84.65
0.08–116.00 pg/ml
−0.04983025
IL-10
13.18
18.71
0.02–106.80
0.10–2.00 pg/ml
−0.075913411
IL-12
2.96
1.14
0.04–4.94
0.10–6.00 pg/ml
0.865394032
IFN-gamma
11.73
13.60
0.63–89.15
0.60–124.00 pg/ml
−0.119490101
MCP-1
60.24
60.71
2.25–311.90
2.00–48.00 pg/ml
−0.016196616
MIP-1 alpha
12.97
21.47
0.15–71.29
0.01–2.00 pg/ml
0.109834572
MIP-1beta
30.94
32.00
2.41–181.11
1.70–47.00 pg/ml
−0.119671384
Rantes
469.01
290.82
107.67–1402.36
100.00–2282.00 pg/ml
−0.13989606
TNF-alpha
22.05
35.23
0.05–120.83
0.10–98.00 pg/ml
−0.403584747
HerronThomasMonaghanSeanGravensteinStefanCioffiWilliamAyalaAlfredHeffernanDaithi
Brown University
THE ASSOCIATION BETWEEN INFLAMMATORY AND HEMODYNAMIC RESPONSE IN GERIATRIC TRAUMA PATIENTS
Background: Trauma mortality is often related to delayed infectious complications and multiple organ failure. A sympathetic response to trauma can afffect both hemodynamics and the inflammatory response. Presenting hemodynamics are often considered the most important predictor of mortality. However, the combined effect of hemodynamic compromise and the presenting inflammatory state may indeed offer a better indicator of survival following trauma. There is a paucity of literature on the additive effect of sympathetic drive on hemodynamics and on the leukocyte response in geriatric trauma patients
Hypothesis: The leukocyte response will have additive effects upon the impact of hemodynamic presentation of geriatric trauma patients.
Methods: A retrospective review of prospectively collected data from a level 1 trauma center over 5 years. Geriatric patients were defined as those aged 65 years and older. Charts were reviewed for age, gender, presenting heart rate, blood pressure, first white cell count (WCC), Injury Severity Score (ISS), and mortality. Tachycardia was defined as heart rate >100 beats/min and hypotension was defined as a systolic blood pressure <100 mm Hg. A hypo-inflammatory response was defined as a WCC of ≥10.0×109/L on first WCC. Patients were divided based on the presence or absence of leukocytosis.
Results: 1,924 geriatric patients were admitted over the 5 years, with an average ISS of 12.1. 64% (1,236) of patients had a lack of leukocytosis on presentation. There was no difference between leukocytosis and non-leukocytosis patients with respect to age (80.2 vs. 79.9; p=0.90) male gender (38% vs. 41%; p=0.60), ISS (12.8 vs. 11.4; p=0.20) or presenting hypotension (4% vs 4.9%; p=0.30). In patients with no leukocytosis, there was no added effect of tachycardia upon mortality (8.8% vs. 8.4%; p=0.40). The presence of a leukocytosis increased mortality in normocardic patients (13.2% vs. 8.8%; p=0.0096). Patients with both tachycardia and leukocytosis had the highest mortality of all groups (20.1% vs. 13.2%; p=0.00001).
Conclusions: Geriatric patients remain very susceptible to the effects of both hemodynamic compromise and the effects of an inflammatory response to trauma. Hemodynamics remains a cornerstone in the prognosis and management of trauma patients. Physicians need to be cognizant of the additive effects of the inflammatory response to trauma, as denoted by a presenting leukocytosis.
RiccioLinPolitanoAmaniLakeDougRosenbergerLauraMoormanRandallSawyerRobertCallandJ. Forrest
University of Virginia
Background: To date, there have been no studies that demonstrate the ability of vital sign data, including heart and respiratory rate characteristics, to predict the development of infection.
Hypothesis: We hypothesized that vital sign characteristics in critically ill adult trauma and surgical ICU patients predict the risk of ICU-acquired pneumonia (IAP).
Methods: We obtained a sample of patients with ICU-acquired pulmonary infection, as defined by the U.S. Centers for Disease Control and Prevention. Timing of the IAP event was defined as the date and time of the intervention, in this case administration of antibiotics. We then retrieved the bedside monitor data of all patients included in our data set during the 24 hours prior to the event. We first utilized univariate analyses to identify individual, joint, and clinical parameters of interest. We then combined these parameters into one model utilizing multivariable logistic regression. From these, we calculated ROC curves and predictiveness curves. A p-value of 0.05 was significant.
Results: From June 2010 to September 2011, there were a total of 1,168 admissions in the database with 2,927 days of data. 102 lung infections were identified. 40 patients had adequate vital sign data for at least 24 hours prior to the event of pneumonia. 75% were trauma patients with an average APACHE II score of 21. Crude mortality was 2.5%. 58% of patients were mechanically ventilated. The 3 most common organisms isolated were P. aeruginosa, S. pneumoniae, and H. influenzae. Results are described in the Figure.
Predictiveness (left) and ROC curves for individual, joint, clinical and combined models.
Conclusions: Analysis of vital sign parameters has great potential to change and improve the care of critically ill patients. We have shown that it is possible to develop models that can predict diseases before they are evident. Continued work in this field will allow the advantage of early detection, early intervention, and prevention of potentially catastrophic events.
PolitanoAmaniRosenbergerLauraMcLeodMatthewHranjecTjasaDossettLesleMayAddisonSawyerRobert
University of Virginia
CYTOKINE LEVELS IN PATIENTS WITH AND WITHOUT FUNGAL INFECTIONS
Background: Interventions targeting specific immune responses to infections have yet to be successful, likely due to heterogeneity of sites, patient factors, and pathogens. Previous studies have suggested that Candida infections are associated with increased IL-1, -6, and -8 expression, and that elevated IL-4 and -10 expression contributes to mortality.
Hypothesis: We hypothesize that ICU -acquired Candida infections are associated with specific elevations in cytokines, including IL-1, -8, -10, and TNFα, when compared to bacterial infections.
Methods: ICU-acquired infections were identified in trauma/surgical patients. Serum samples collected within 48 h of diagnosis were analyzed for IL-1, -2, -4, -6, -8, -10, -12, IFNγ, GM-CSF, and TNFα by ELISA. Demographics, outcomes, and cytokine levels were compared using independent samples t-test, χ2, and Mann-Whitney U tests.
Results: 933 infections were identified, including 138 with Candida or yeast isolated. Demographics and outcomes are shown. Patients with fungal infections had elevated IL-8 and GM-CSF (52.5 [15.5, 99.7] vs. 32.0 [11.6, 71.5], p=0.011; 2.7 [2.7, 6.8] vs. 3.4 [2.7, 9.0], p=0.009). Positive fungal cultures were significantly more common in patients with abdominal, urine, skin structure, or catheter-associated infections, and significantly less common in lung infections (p<0.007 for all). Mortality did not differ by presence of fungi. However, patients with fungal infections who died had significantly elevated IL-1, -8, and -10 expression (p<0.03 for all). Patients without fungi who died had elevated IL-4, -6, -8, -10, and TNFα (p<0.02 for all).
Conclusions: Cytokine expression varies according to specific bacterial pathogens in animal models. Our data show that IL-8 and GM-CSF expression differs between infected patients with and without fungi. In addition, the cytokine response differs significantly in patients who die, suggesting a dysregulated immune response in these patients. Further studies are required to determine whether these changes are site- or species-specific, and to evaluate potential targeted interventions.
Fungus (n=138)
No Fungus (n=795)
p-value
Age
55.2±1.4
47.3±0.6
<0.001
APACHE II Score
18.4±0.6
17.3±0.2
0.098
ICU to Infection (days)
11.9±1.4
8.8±0.3
0.027
ICU LOS (days)
12.5±1.6
9.7±0.4
0.014
Mortality
32 (23.2)
132 (16.6)
0.061
Mean±standard error or n (%).
JeschkeMarcCheungAlisonHiyamaYaekoHarrisonRachaelSmithAlexandra
Sunnybrook Health Sciences Center
WHY IS THE POST-BURN OUTCOME OF ELDERLY PATIENTS SO POOR? INSIGHTS FROM INFLAMMATORY CYTOKINE AND METABOLIC HORMONE PROFILING
Background: Post-burn outcomes in elderly patients are extremely poor and have not improved much over the last decades. In order to improve post-burn morbidity, we believe it is imperative to determine the underlying mechanisms driving the pathophysiological responses, which will allow us to design better treatment for elderly patients.
Hypothesis: We hypothesized that the poor clinical outcome of elderly patients could be related to their inflammatory response or changes to their metabolic requirements.
Methods: We analyzed all acute burn admissions from 1995–2005 in our database. We separated them into adults (<55 years old, n=1168) and elderly (≥55 years old, n=447). We analyzed and compared the two groups in terms of burn severity, co-morbidities, complications, and outcome. We also analyzed the plasma composition for a panel of inflammatory cytokines and metabolic hormones from 10 adults and 13 elderly patients using the multi-analyte Milliplex platform (Millipore, Billerica, MA).
Results: There were no significant differences in burn severity in terms of %TBSA (15% for <55 yo vs. 17% for ≥55 yo). The proportion of patients with inhalation injury was slightly higher in the elderly group (13.4% vs. 19.0%). Although there were more elderly patients who had one or more pre-existing medical condition at admission (34.4% vs. 74.9%, p<0.05), the incidence of cellulitis, graft infections, and thrombosis complications during their hospital stay was not significantly different between the groups. Incidence of pneumonia, bacteremia, sepsis, and acute kidney injury were significantly higher in elderly patients, p<0.05. Consistent with the clinical findings, profiles of inflammatory cytokines and metabolic analytes revealed that elderly with burns >20% TBSA exhibited higher levels of circulating pro-inflammatory cytokines and altered metabolic profiles indicating a hyper-inflammatory and hyper-metabolic response.
Conclusions: The altered levels of plasma cytokines and metabolic hormones implicate a connection between insulin resistance, organ function, and immuno-potency of burn patients. These data suggest that the altered metabolic and inflammatory response of elderly patients post-burn may be related to their vulnerability to sepsis or organ failure.
RiveraFernandoBurrisAgnesLiuMing-MeiMineiJoseph
University of Texas=Southwestern
EVALUATION OF NEUTROPHIL CD64 AS A MARKER OF SEPSIS IN BURN PATIENTS
Background: Studies have shown that CD64 expression can be used as a diagnostic marker of infection and sepsis. The ability of CD64 expression on the neutrophil membrane to indicate infection in burn patients has not been evaluated.
Hypothesis: Neutrophil CD64 expression will allow us to differentiate patients with infection.
Methods: Patients admitted to the burn unit at Parkland Hospital, with >15% total body surface area (TBSA) burn injuries or inhalation injury were prospectively enrolled. Clinical data were collected daily. Blood was taken at different time points and CD64 expression was measured in 49 burn patients at different time points using flow cytometry focused on quantitation of antibodies bound per cell (QuantiBRITE).
Results: 45 patients were enrolled, of those 17 developed sepsis. There were no clinical or demographic differences between sepsis and no-sepsis patients. CD64 expression on neutrophils was significantly increased in patients with sepsis at each time point when compared with no-sepsis patients. CD64 was not detected in healthy volunteers. The calculated optimal cutoff value for CD64 was 4,074 antibody-phycoerythrin molecules bound/cell.
Conclusions: Quantitative expression of granulocyte CD64 expression is a useful indicator of infection in burn patients.
RodriguezNoeFinnertyCelesteCalhounBrendanHawkinsHalHerndonDavid
University of Texas Medical Branch/Shriners Hospitals for Children
FUNGAL WOUND INVASION IS ASSOCIATED WITH INCREASED MORTALITY IN PEDIATRIC BURN PATIENTS
Background: Fungal wound infections are uncommon but a potentially lethal complication of severe thermal injury.
Hypothesis: The occurrence of fungal wound invasion (FWI) after thermal injury will increase mortality.
Methods: The records of 2,846 patients with thermal burns admitted to a single burn center (1998–2008) were reviewed. Analyses accounted for total burn size (TBSA, percentage body surface area), full-thickness burn size (FTBS, percentage body surface area), age, inhalation injury, gender, and fungal status category. Fungal colonization and infection were determined histopathologically.
Results: Criteria for inclusion were met by 2,846 patients. Each patient's fungal status category was defined according to the deepest level of fungal involvement observed during the hospital course: no fungus (2,497 patients), fungal wound colonization (FWC, 208 patients), or FWI (141 patients). Mean TBSA (20%, 47%, 61%, respectively) and mortality (1.51%, 6.15%, 23.89%, respectively) varied significantly among fungal status groups. Logistic regression was used to detect significant independent associations. FWI was associated with higher TBSA. Mortality was associated with TBSA, FTBS, inhalation injury, FWI, and age. Unlike FWI, FWC was not independently related to mortality, the greater observed mortality in FWC being explained by other variables such as TBSA.
Conclusions: FWI accompanies larger burns and is associated with mortality in burn patients, particularly in those with TBSA 30% to 60%. This association is independent of burn size, inhalation injury, and age.
HaithLinwoodYoungChristineAckermanBruceReigartCynthiaStair-BuchmannMeganPattonMaryGuildayRobertNelsonStephenRavrebyWilliam
The Nathan Speare Regional Burn Treatment Center, Crozer-Chester Medical Center
EVALUATION OF NASAL METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS (MRSA) POLYMERASE CHAIN REACTION (PCR) AS A SCREENING TOOL IN BURN CENTER PATIENTS
Background: Chronic carriers (CC) of MRSA are decolonized (D) to prevent MRSA spread. Screening MRSA carriage by culture or nasal swab (NS) MRSA PCR and D with mupirocin ointment is recommended to reduce MRSA burden and prevent MRSA infections. We test all admissions and at discharge with NS PCR. MRSA NS PCR-positive patients (PT) are D for infection control. NS PCR testing was investigated for efficacy in finding MRSA colonization and preventing subsequent MRSA infection.
Hypothesis: NS PCR finds patients at risk for MRSA post-admission infection.
Methods: This IRB-approved study looked at data for 23 months from January 2010 to November 2011, with evaluation of NS screening after August 1, 2006. Data were analyzed to determine normal distribution. Student T-test was used for data stratified by presence or absence of infection or NS MRSA PCR testing; significance set at 0.05.
Results: Our center admits nearly 450 patients/year. Interim analysis identified 75 patients CC MRSA (11 patients with previous cultures and 46 patients with admission- positive NS MRSA PCR). 18 additional patients converted to MRSA-positive. Burn injury was involved in 70 patients, and 5 patients were diagnosed with toxic epidermal necrolysis. For 18 patients the initial NS PCR was negative, there was conversion to positive with NS PCR in 7 patients at discharge, positive cultures in 9 patients, and 2 patients remained PCR-negative. Demographic analysis by NS PCR status showed no difference in the groups. Stratification by MRSA-positive NS or culture vs. negative PCR and negative culture noted a difference in length of stay (p<0.05) 27.5±31.4 days vs. 11.9±16.1 days. Total body surface area burn was 19.2±22.6% vs. 8.9±11.3% for positive and negative MRSA groups, respectively (p<0.05). MRSA-positive cultures were obtained in 36 patients (48%), for which erythromycin-clindamycin sensitive (ECS) MRSA was isolated at least once in 20/36, suggesting community-acquired MRSA (CA-MRSA).
Conclusions: NS MRSA PCR does not distinguish between ECS MRSA and hospital-acquired MRSA. 20 of 36 patients with positive MRSA culture had at least one isolate of ECS MRSA, indicating likely CA-MRSA. Assessment of the D program suggests that D may have prevented positive MRSA cultures in 16 of 31 admissions to the burn center with NS MRSA PCR-positive screening. This group of 75 patients represents 8.3% of all BTC admissions.