
Abstract
Abstract
Introduction:
Clostridium difficile infection of the small bowel, or C. difficile enteritis (CDE), is an uncommon condition. Cases reported previously have been described in patients with inflammatory bowel disease (IBD), compromised immune systems, or a history of colectomy or small bowel surgery.
Case Description:
We present a case of fulminant CDE causing abdominal compartment syndrome following a routine outpatient inguinal hernia repair. This patient developed multiple organ failure dysfunction syndrome requiring surgical abdominal decompression and a small bowel resection. This case highlights the challenges in the diagnosis of CDE, particularly in patients with intact colons and unusual presentations.
Discussion:
A high index of suspicion is required, as early recognition of CDE is essential in reducing morbidity and mortality. This case report is followed by a review of the current literature on CDE, with a focus on the complexities inherent in the identification of this problem and the decision-making process for surgical intervention.
C
Abdominal compartment syndrome (ACS) is a well-described surgical emergency occurring in a variety of settings, including trauma and intra-abdominal infection, and resulting in hypoperfusion of abdominal organs [7,8]. The ACS has been reported in association with C. difficile colitis [9], but to our knowledge, this is the first reported case in the setting of CDE. It is generally believed that C. difficile does not have a predilection for infection of the small bowel. However, receptors for C. difficile toxin A have been identified in human small bowel [1]. Here, we present a case of severe CDE, which occurred in a patient with no previous intestinal surgery, and was associated with the development of ACS.
Case report
A 49-year-old male developed fulminant CDE following a laparoscopic inguinal hernia repair. The patient was an otherwise healthy male, with no prior surgery, who underwent a routine outpatient laparoscopic bilateral inguinal hernia repair and received one dose of perioperative cefazolin. He was readmitted four days later with nausea, vomiting, and a computed tomography (CT) scan consistent with a small bowel obstruction. He underwent exploratory laparotomy. The distal ileum was thickened, but no mechanical obstruction was identified, and the bowel appeared viable. No bowel resection was performed and the abdomen was closed. He again received one dose of pre-operative cefazolin.
Over the next 24 h, he continued to decompensate and developed a severe metabolic acidosis, acute kidney injury, and respiratory failure. He underwent a second-look laparotomy six hours later. Again, no areas of ischemia or obstruction were found, and his abdomen was closed. Subsequently, the patient had one loose bowel movement which was sent for C. difficile antigen enzyme-linked immunosorbent assay (ELISA) testing and returned positive. He was started on IV metronidazole. However, despite this, the patient deteriorated and developed profound multiple organ dysfunction syndrome and shock requiring multiple vasopressors.
He was transferred subsequently to a tertiary-care facility. On arrival he was found to have acute kidney injury with anuria, respiratory failure, and progressive lactic acidosis. On physical examination, his abdomen was firm and distended, with concurrent elevated peak airway pressures (50 cm H2O). In addition, he demonstrated marked venous congestion of his chest wall, upper extremities, and face. Bladder pressure measurements between 35–40 mm Hg were obtained, confirming intraabdominal hypertension. These findings were consistent with ACS, and he underwent emergent decompressive laparotomy. The operative findings included dilated small bowel with areas of gross ischemia. One hundred eighty centimeters of small bowel were resected and the patient was left in discontinuity with temporary abdominal dressings in place for planned re-exploration. Of note, the patient's colon was completely decompressed, well-perfused, and without edema. At the time of bowel resection, a sample of enteric contents from the distal ileum was sampled, and also found to be positive for C. difficile by ELISA. The patient's vasopressor requirement resolved over the next 24 h. Enteric vancomycin was administered via nasogastric tube, in addition to parenteral metronidazole. He was re-explored and washed out two days later and underwent hand-sewn anastomosis of his small bowel six days later. Because of persistent bowel edema and retraction of his fascia, his abdominal wall could not be closed initially. He returned to the operating room three more times for sequential closure of his fascia using negative-pressure dressings [10]. Complete fascial closure was achieved by day 12. His renal dysfunction resolved slowly and he was discharged 30 d after his bowel resection, tolerating a regular diet.
Pathologic examination
On macroscopic examination, the resected small bowel was markedly dilated. The serosal surface was dusky with prominent vascularity. The wall of the small bowel ranged from 0.1 to 0.2 cm thickness and was edematous (Fig. 1). The mucosa was tan-pink and dusky when examined in its fresh state. Scattered foci of gelatinous membrane were noted. No obvious necrosis was identified. Sections through the gelatinous membrane showed a layer of luminal mucin, and necrotic debris, and mixed with mononuclear inflammatory cells attached to the necrotic mucosa (Fig. 2A&B). There was a relative lack of neutrophil inflammation in the pseudomembrane. Random sections of the remaining small bowel showed diffuse mucosal damage that was characterized by dilation of lacteals, blunting of villi, separation of surface epithelial cells from the lamina propria, and sloughing of surface epithelial cells at the tip of villi (Fig. 3A–C). There were atrophic glands (regenerative glands), crypt epithelial apoptosis, and mild hyalinization of the lamina propria in the areas affected most severely. In addition, there was submucosal hemorrhage and degeneration of muscularis propria (Fig. 3D). The overall histopathologic feature was most consistent with ischemic enteritis. No thromboembolic findings were present in the mesenteric vasculature.
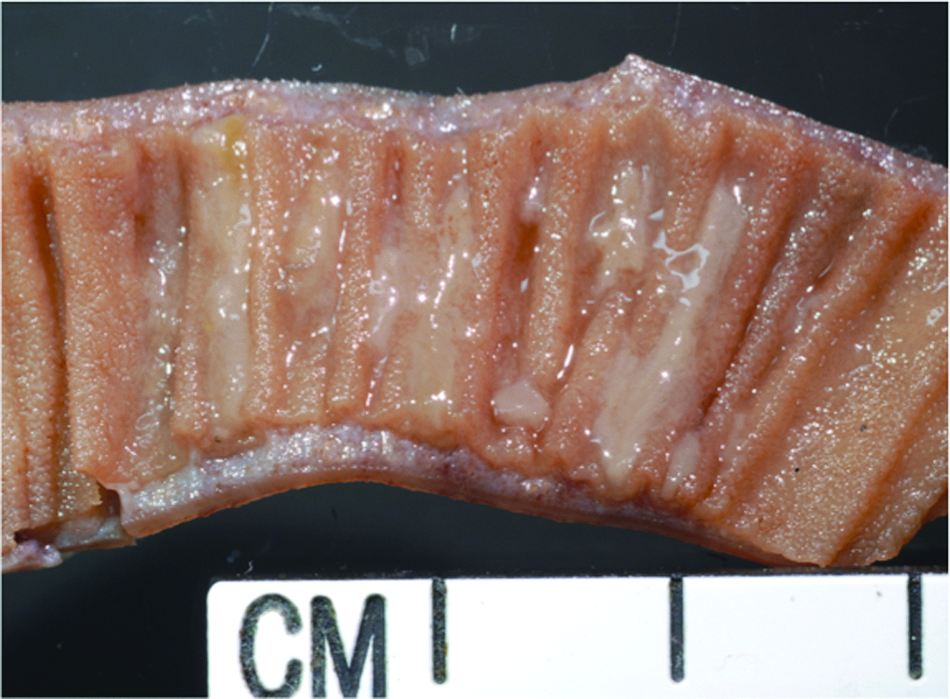
Macroscopic examination of the resected small bowel shows marked, diffuse edema, and focal pseudomembrane formation. Color image is available online at www.liebertpub.com/sur
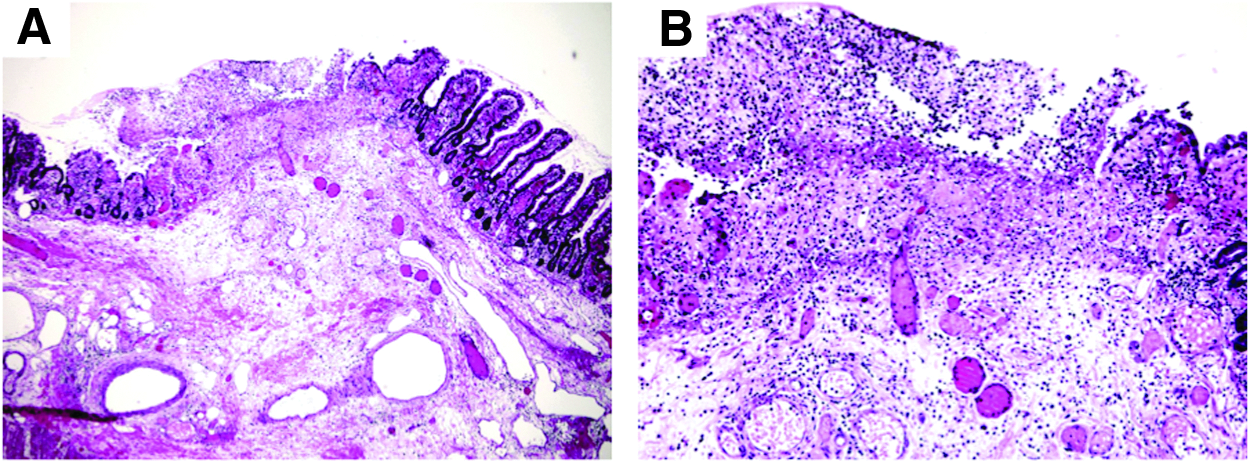
Histologic examination of area with pseudomembrane.
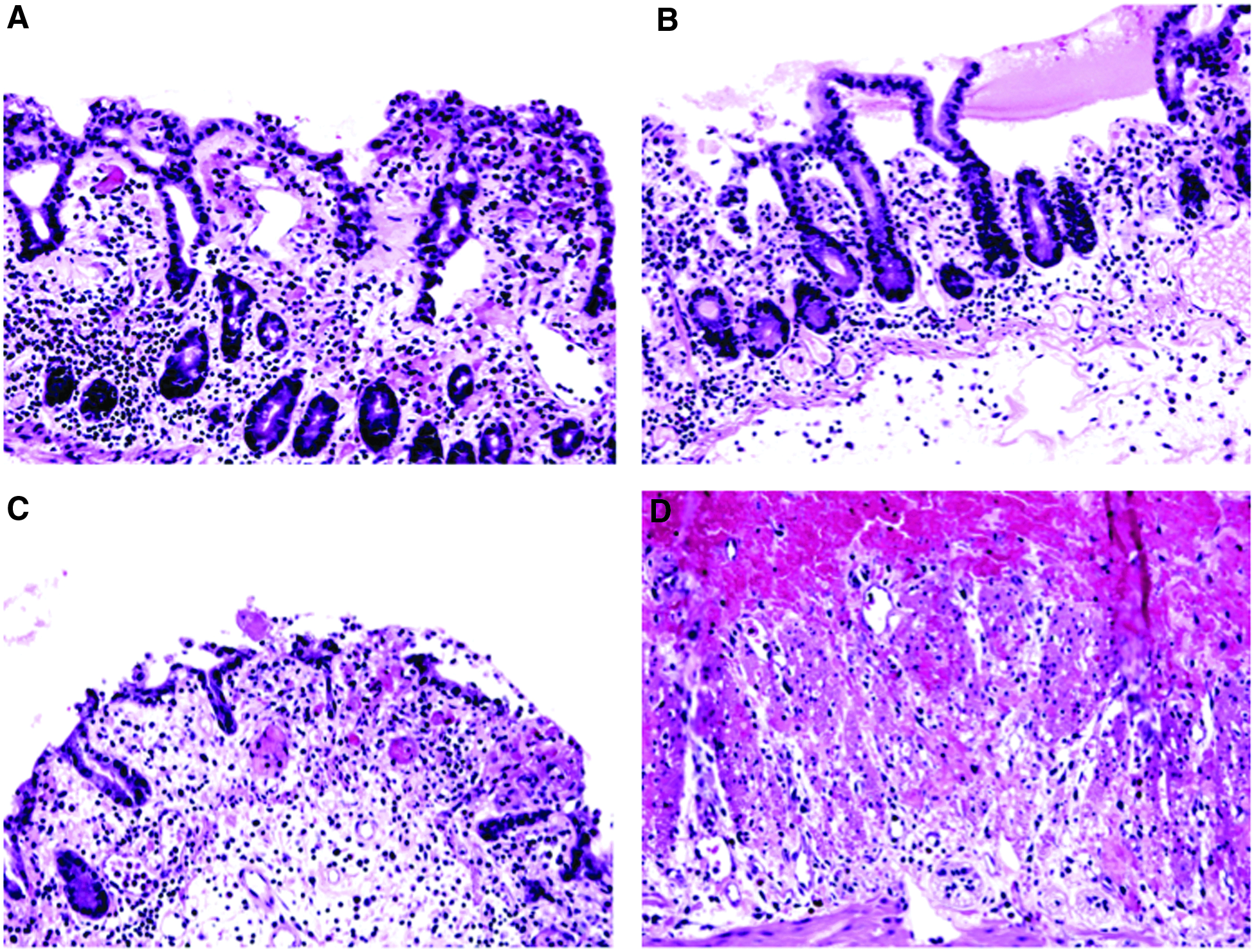
Histologic examination of random small bowel section.
Discussion
Clostridium difficile produces two toxins, A and B, which play a role in the pathogenesis of disease. Animal studies have shown toxin A to be an enterotoxin that elicits increased intestinal permeability, fluid secretion, and inflammation, and causes severe disruption of the intestinal epithelium [11]. Studies on human colon biopsy specimens have shown that toxin A causes epithelial cell rounding, detachment, and apoptosis [2] and forms a characteristic pseudomembrane under endoscopic or macroscopic examination and has therefore, been named pseudomembranous colitis historically. In human beings, the colon is the main site of C. difficile infection, but receptors for CD toxins have been isolated from the human small bowel, with substantial variability in small bowel toxin binding among individuals [1]. Animal studies have demonstrated C. difficile induced enteritis because of binding of toxin A to receptors in the small bowel [11–13]. In addition, as was demonstrated previously in transplanted human intestinal xenografts [14], C. difficile toxin B is a potent inflammatory enterotoxin and may contribute to intestinal damage in CDE.
In the case of our patient, there was diffuse epithelial injury involving the mucosal surface and the crypt epithelium, with mild hyalinization of the lamina propria. The pseudomembrane was patchy and there was no neutrophil inflammation. Indeed, these features are also consistent with ischemic injury secondary to ACS. However, the patient's rapid development of ACS following a routine outpatient procedure is unusual without an underlying inciting condition. A positive ELISA for C. difficile toxin on a sample obtained from the ileum, diffusely edematous small intestine, a normal appearing colon at the time of surgery, and the pathologic findings above suggest that this patient may have developed sepsis and ACS in the setting of CDE. In contrast to other cases that have thus far been presented in the literature, this is a patient who was not immunosuppressed and who did not carry a diagnosis of IBD. He received only one dose of perioperative antibiotics, and, yet, presented with diarrhea and sepsis, and tested positive subsequently for C. difficile toxin.
Vigilance for CDE, with appropriate testing and prompt treatment, may aid in improving the clinical outcomes of these patients. In patients with underlying risk factors, such as IBD, immunosuppression, or a previous colectomy, appropriate clinical signs and symptoms should prompt concern for CDE. This diagnosis is more challenging in patients with an intact colon, where the typical features of leukocytosis, diarrhea, and abdominal pain may suggest C. difficile colitis, but involvement of the small bowel may not be apparent. Increased severity of presentation, including shock, or the presence of a small bowel obstruction with wall thickening on imaging may suggest CDE [6,15], but confirmation of diagnosis would be challenging. Laboratory testing, either by polymerase chain reaction (PCR) or ELISA, would confirm the presence of C. difficile toxin, but would not provide information regarding the extent of gastrointestinal tract involvement. In general, treatment would be the same regardless of the presence or absence of enteritis. An attempt at medical treatment would be made, with surgical intervention reserved for patients who develop fulminant disease. However, the presence of enteritis may put patients at higher risk of requiring surgical intervention, and early recognition may lead to earlier surgical intervention, with perhaps improved outcomes. In addition, clinicians should be aware of unusual presentations, such as ACS, which may manifest in patients with underlying CDE.
Clostridium difficile infection has a broad range of severity, ranging from the asymptomatic carrier state to toxic fulminant colitis requiring emergent surgery. Mortality rates increase with the severity of the disease state. Numerous factors have been identified that may play a role in the degree of severity, including strain type, host co-morbidity, prior antibiotic use, and use of acid suppressive medication. Although some of these factors have been substantiated by research, others are still in the process of being investigated. It has been proposed that CDE may be more severe than colitis. However, given the difficulty in diagnosis, particularly in patients with intact GI tracts, this would be difficult to prove.
The case that we have presented here has brought up several questions regarding C. difficile infection. Firstly, does an alteration in gastrointestinal motility contribute to the development of CDE? Wee et al. described the CT findings in four patients with CDE confirmed pathologically [6]. Mesenteric stranding, ascites, small bowel distension, and mural thickening are prominent features on CT exam. These findings are not specific, and can also be observed in the setting of bowel ischemia. In addition, bowel distension is a hallmark feature of bowel obstruction or ileus. This leads to a question of whether slowing or stasis within the GI tract may promote C. difficile colonization. Patients who have undergone surgery within 30 d are at increased risk for the progression of C. difficile to fulminant disease [16]. Decreased GI motility that is common in the post-operative period, particularly in patients using narcotics for pain control, may allow for the proliferation of C. difficile and toxin production, leading to clinical worsening.
Furthermore, C. difficile infection recurrence is common, with much recent research focused on how to clear the infection and restore normal GI flora. In response, several new medical therapies have emerged, including rifaximin and fidaxomycin [17], which both show improvements in recurrence rates. Fecal transplant has also been proposed as novel therapy in the setting of recurrent C. difficile infection. Is it possible that the small intestine acts as a reservoir for C. difficile infection? Kralovich et al. published a case report in 1997 of a patient who developed fulminant C. difficile ileitis in a defunctionalized segment of ileum following jejuno-ileal bypass surgery, suggesting that this segment of small bowel was serving as a reservoir for C. difficile infection [18]. If the small intestine does indeed act as a reservoir, perhaps therapy should be targeted at eradication of C. difficile from the small intestine, as this might help to prevent recurrences and progression to fulminant disease. Mortality rates following colectomy remain high at 33% [19]. On multivariable analysis, this was associated mainly with host factors, such as advanced age and underlying comorbid conditions. However, addressing CDE, if present at the time of laparotomy, may improve outcomes and guide medical treatment following surgical intervention.
As of yet, no study on the extent of gastrointestinal tract involvement in the setting C. difficile infection has been performed, and as such, we have no correlation with impact on progression to fulminant disease or mortality. Although guidelines exist for the treatment of C. difficile colitis, guidelines for the treatment of CDE have not been established. In the future, defining the extent of C. difficile infection may aid in tailoring treatment of this infection, ensuring that all sites along the GI tract are clear and that normal flora has been restored. This may also help to direct therapy to distinct regions of the GI tract, for example using enemas for colonic involvement and oral therapies when the small bowel is involved. In addition, if indeed the site of involvement is associated with severity, defining the extent of involvement may be useful in determining which patients would benefit from early surgical intervention. The case presented in this report is far from straightforward. Although CDE was diagnosed clinically, the pathologic specimens were equivocal for infectious versus ischemic colitis. We present this case to highlight an unusual and dramatic presentation of what we believe was CDE, as well as to bring up some interesting questions regarding the complexities of C. difficile infection. Future studies on CDE may further elucidate its clinical importance and guide early diagnosis and treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.