
Abstract
Abstract
Background:
We studied the influence of morphology and type of material of abdominal wall prostheses in the avoidance of bacterial adhesion in acute and chronic mesh infections.
Methods:
Three different types of prostheses were compared: 1) High-density polypropylene monofilament mesh (PMM); 2) low-density PMM; and 3) prostheses composed of low-density polypropylene and a non-porous hydrophilic film (composite prostheses). Microbial adhesion tests were performed using reference strains of Staphylococcus aureus 15981, Staphylococcus epidermidis ATCC 35984, Mycobacterium abscessus DSM 44196, and Mycobacterium fortuitum ATCC 13756 using a protocol described previously.
Results:
Both Staphylococcus spp. and M. fortuitum strains showed lower adherence to PMM. Mycobacterium abscessus also exhibited lower adherence to composite prostheses. Both Mycobacterium spp. strains had lower adherence than Staphylococcus spp. strains for all materials except for low-density PMM. Mycobacterium fortuitum showed higher adherence to composite prostheses than M. abscessus, whereas the latter species had higher adherence to high-density PMM than M. fortuitum.
Conclusion:
Depending on the type of bacteria, collagen-coated hydrophilic prostheses with a large surface increased bacterial adherence significantly. These differences should be taken into consideration when choosing a mesh graft, which limits infection in abdominal wall reconstruction.
A
The presence of foreign material decreases the number of bacteria needed to produce an infection [4,5,12]. As a part of this process, bacterial adhesion to implanted biomaterial surfaces and subsequent proliferation and biofilm development are key steps in the pathogenesis of infection. Bacterial adherence on surfaces is influenced by the wettability of the material, bacterial species, and material type [1]. Specific chemical surface interactions between microorganisms and biomaterial or its conditioning film can strengthen or reduce adhesion (electrostatic forces generated by a net charge distribution on both the biomaterial surface and the bacterial wall, attractive acid-base interactions, and weaker Lifshitz-Van der Waals forces) [13,14].
Substantial differences exist between the available surgical meshes, which include type of material, amount of yarns, and type of construction [1]. Each of these unique structural components can have a great effect on the mesh surface area and chemistry and influence the ability of bacteria to adhere to the material [5,8,12]. Although several types of synthetic mesh exist, polypropylene monofilament mesh (PMM) and dual-facing mesh made of polypropylene and a resorbable hydrophilic film (composite prostheses) are used commonly [7].
Surgical site and implant contamination usually occur at the time of surgery and in the early post-operative period. Current conventional infection prevention therapies have not been successful in reducing the rate of surgical site infections [4]. Staphylococcus aureus and Staphylococcus epidermidis are prevalent skin flora, and are responsible for more than 90% of surgical site infections, including mesh-related infections [4,8]. The interaction between these bacteria and various graft materials has been studied previously in several reports [7,15,16].
Rapidly growing mycobacteria (RGM) are environmental organisms that can be considered opportunistic pathogens. The members of the Mycobacterium fortuitum and Mycobacterium abscessus complexes are the RGM species isolated most frequently in human infections [17,18]. Many diseases caused by these organisms have been associated with biomaterial-related surgical procedures, such as orthopedic prostheses, peritoneal dialysis catheters, vascular catheters, and prosthetic heart valves [19]. Some times they are the cause of infection in chronic abdominal wall prostheses [8,20]. In this in vitro study, we compared the adhesion of Staphylococcus spp. and RGM on three different prostheses used for abdominal surgery procedures.
Materials and Methods
Materials
Dual-facing prostheses made of polypropylene and a resorbable hydrophilic film (Parietene composite; Sofradim Production, Trévoux, France) were compared against polypropylene monofilament meshes of 1) high-density (Surgipro; Norwalk, CT) and 2) low-density (Parietene, Covidien), in order to study their respective patterns of adherence.
Four Covidien strains were studied: S. aureus 15981 [21,22], S.epidermidis ATCC 35984, M. abscessus DSM 44196 and M. fortuitum ATCC 13756 [19]. All are described as in vitro biofilm-forming strains; reference S. aureus strain is methicillin-susceptible and the S. epidermidis strain is methicillin-resistant.
Growth media and incubation conditions
Mycobacterial strains were grown at 30°C on Middlebrook 7H10 agar (Becton Dickinson, Franklin Lakes, NJ) supplemented with glycerol for 7 d, and were later grown in Middlebrook 7H9 broth (Becton Dickinson) supplemented with Tween-80 0.01%v/v for 5 d at 30°C. No media changes were performed during the incubation period. Staphylococcus aureus 15981 [21] and S. epidermidis ATCC 35984 were grown overnight at 37°C on tryptic soy agar containing sheep blood 5% v/v, and were grown subsequently in tryptic soy broth (bioMerieux, Marcy d'Etoile, France) at 37°C for 1 d.
Evaluation of bacterial attachment
To evaluate bacterial attachment, the protocol described by Zamora et al. [23] was modified as described below. Sterile meshes (size of approximately 1 cm×1 cm) were immersed separately in tubes containing 2.5 mL of phosphate-buffered saline (PBS) (Sigma, St Louis, MO) and were incubated at 37°C for 24 h. The PBS was then replaced by 2.5 mL of bacterial inoculum, adjusted previously to a 0.5×McFarland standard (108 CFU/mL). After incubation for 90 min at 37°C, the inoculum was removed and replaced by sterile PBS. The tubes were then incubated for 24 h at 37°C. Next, the meshes were washed three times with sterile distilled water to remove non-adherent bacteria and were then placed in 2.5 mL of sterile PBS and sonicated at low power for 5 min in a Bandelin Sonorex TK-52 sonicator (Schalltec GmbH, Mörfelden-Walldorf, Germany). Attached bacteria were quantified by preparing 1:10 serial dilutions from the sonicate and streaking 100 mL of each dilution on Middlebrook 7H10 agar plates. The plates were incubated at 30°C for 7 d and the colonies were then counted. Attachment of S. aureus and S. epidermidis was quantified by the same procedure, except that the sonicate was streaked on tryptic soy agar containing sheep blood 5% v/v and the plates were incubated for 24 h at 37°C. All experiments were performed in triplicate.
Data analysis
The Mann-Whitney U/Wilconxon tests were used for statistical multiple comparisons of the average total bacterial counts between two species, and the Kruskal-Wallis test was used for more than two species. EPI-Info software (version 3.5.1 (CDC, Atlanta, GA) was used to perform statistical analyses.
Results
Bacterial adhesion of Staphylococcus spp. collection strains
The adherence results (Fig. 1) indicated that both Staphylococcus strains showed lowered adherence to PMM (p<0.0001, Kruskal-Wallis test). Staphylococcus spp. showed lowered adherence to low-density PMM (p<0.0001, Kruskal-Wallis test). There were no statistical differences between high-density PMM and composite prostheses for S. aureus (p=0.185, Kruskal–Wallis test) and S. epidermidis (p=0.7573, Kruskal–Wallis test). When we compared the adhesion of both strains, the difference between the adhesion of S. aureus and S. epidermidis was not statistically significant (p>0.0001, Kruskal-Wallis test).
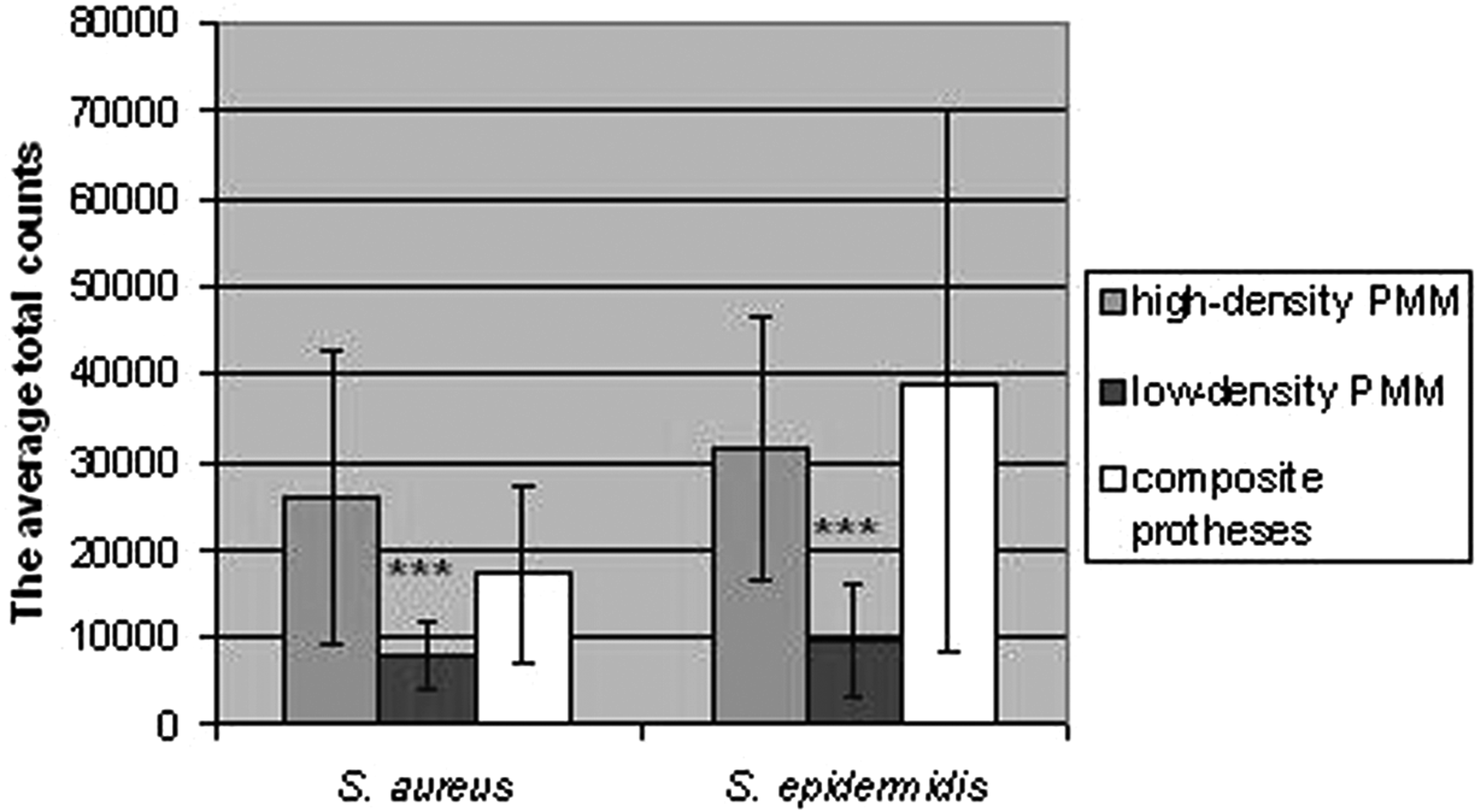
Numbers of attached bacteria of Staphylococcus aureus and Staphylococcus epidermidis (colony-forming units) to 1) high-density polypropylene monofilament mesh (PMM), 2) low-density PMM, and 3) composite prostheses.
Bacterial adhesion of Mycobacterium spp. collection strains
Mycobacterium fortuitum showed lowered adherence to high-density PMM (p<0.0001, Kruskal-Wallis test; Fig. 2) and M. abscessus to composite prostheses (p<0.0001, Kruskal-Wallis test). Regarding PMM, M. abscessus showed low adherence for high-density mesh (p<0.0001, Kruskal-Wallis test). There were no statistical differences between low-density PMM and composite prostheses for M. fortuitum (p=0.145, Kruskal–Wallis test). The difference between the adhesion of the two mycobacterial strains was statistically significant (p<0.0001, Kruskal-Wallis test) for high-density PMM and composite prostheses.
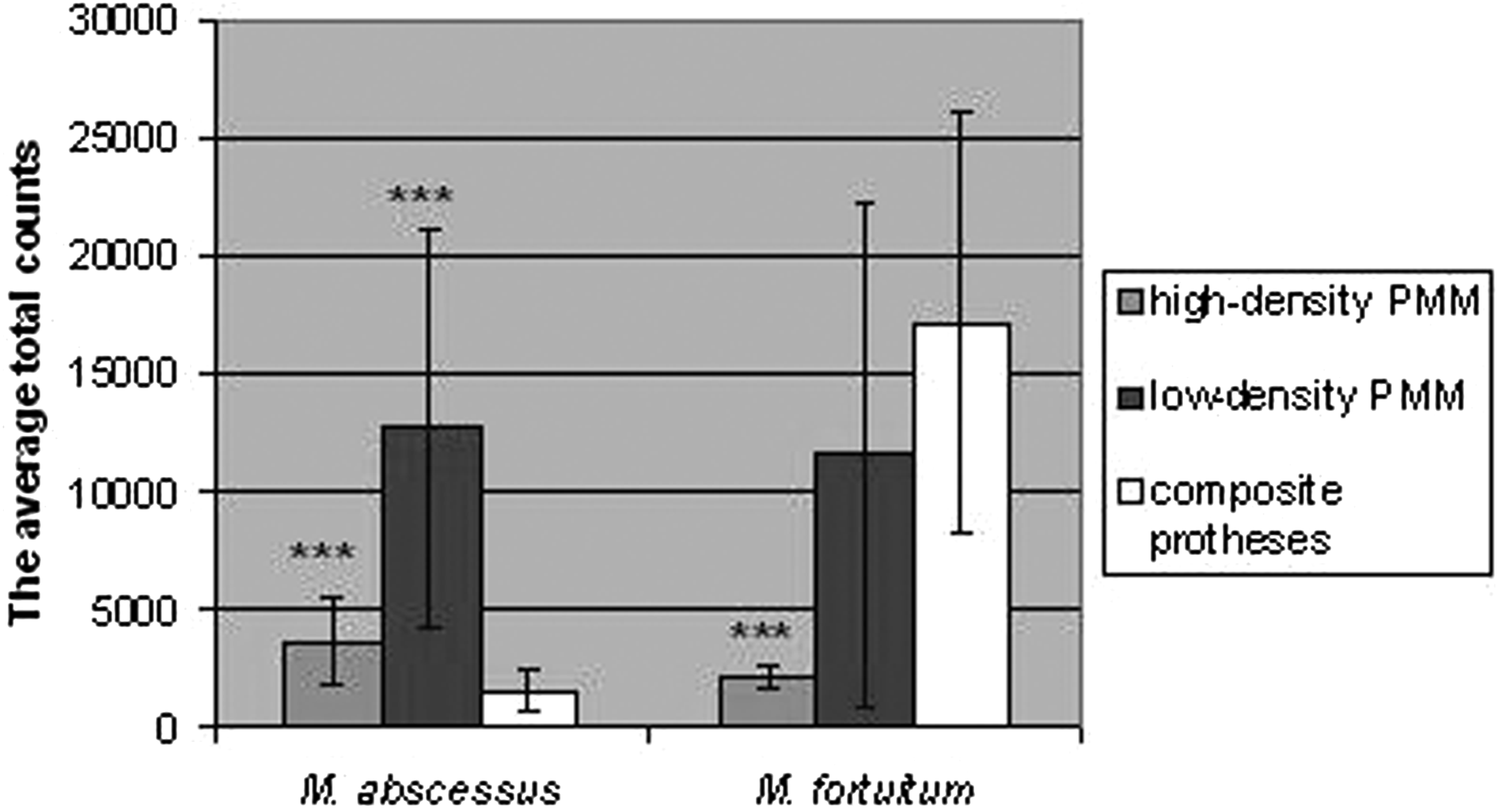
Numbers of attached bacteria of Mycobacterium abscessus and M. fortuitum (colony-forming unit) to 1) high-density polypropylene monofilament mesh (PMM), 2) low-density PMM, and 3) composite prostheses.
Comparison between Staphylococcus spp. and RGM
Rapidly growing mycobacterium showed lower adherence than strains of Staphylococcus spp. for all abdominal wall prostheses (p<0.0001, Kruskal-Wallis test), except for low-density PMM. There were no statistical differences between bacterial adherence for this material (p=0.875, Kruskal-Wallis test).
Discussion
We compared three commercially available surgical meshes in an in vitro infection model using microorganisms isolated from acute and chronic infections. Bacterial adherence on surfaces is influenced by the wettability of the material, bacterial strain, and material type [24].
Wettability depends either on the surface material or on the conditioning film on the substratum surface. Presence of high water contact angles on the mesh indicates a hydrophobic surface, which theoretically reduces the bacterial colonization of the meshes. Polymers, such as polypropylene or polytetrafluoroethylene, are hydrophobic, but collagen is hydrophilic [25]. For Staphyloccocus spp. and M. fortuitum, the PMM showed an immediate decrease in bacterial adhesion when compared to prostheses with a hydrophilic surface (Parietene composite).
Staphyloccocus aureus and S. epidermidis showed low adherence to low-density PMM. The increased surface area of a high-density PMM promotes the adherence and persistence of bacteria in the implant bed, although this alone is not enough to create a clinically symptomatic infection. According to these results, low-density mesh seems to increase the risk of infection by Mycobacterium sp.
Mycobacterium abscessus showed low adherence to composite prostheses. There are molecular mechanisms of bacterial attachment to host protein-coated biomedical implants. These interactions involve specific surface proteins, called bacterial adhesins, which recognize specific domains of host proteins deposited as a film on indwelling devices, such as fibronectin, fibrinogen, fibrin, albumin, or collagen [26]. Natural material such as collagen has been reported to serve as a potential binding site for S. aureus [27,28].
In summary, our data show that abdominal wall prostheses with a large and collagen-coated surface increase bacterial adherence for Staphylococcus spp. bacteria, which are responsible for over 90% of surgical site infections. These results suggest that low-density monofilament hydrophilic meshes could have a low infection rate [29].
The same does not hold for RGM. Depending on the type of RGM and the properties of the abdominal wall prostheses (morphology and composition), its adherence could change significantly. However, our results must be integrated with caution, because we have not tested clinical isolates of bacteria, which can have different properties than reference strains, because these latter are adapted to artificial cultures. More research is necessary in this sense, and also in order to evaluate other species involved in mesh infections, such as Enterobacteriaceae or Pseudomonas aeruginosa.
As more than one million mesh implants are used per year globally, improvements made in the materials in order to minimize infection would be of great importance. These results and others obtained in the future should be taken into consideration when choosing a mesh graft for abdominal wall repair.
Footnotes
Acknowledgment
The authors thank Mr. Oliver Shaw for his help with language edition.
Author Disclosure Statement
This study was sponsored by the program CONSOLIDER-Ingenio 2010 CSD2008-00023-FUNCOAT and by the Surgery Department of the Fundacion Jimenez Diaz. Meshes were provided free of charge by the manufacturers. Doctor Esteban has received travel and research grants from Pfizer, Novartis, and Wyeth. No competing financial conflicts exist for all other authors.