
Abstract
Abstract
Background:
Macrolide-based treatment has been associated with survival benefit in patients hospitalized with community-acquired pneumonia (CAP). However, the influence of macrolide therapy in all patients hospitalized with pneumonia, including healthcare-associated pneumonia (HCAP), is unclear.
Methods:
Analysis of a retrospective single-center cohort.
Results:
Community-acquired pneumonia was present in 220 (22.5%) of all patients with pneumonia admitted through the emergency department of Barnes-Jewish Hospital, and HCAP was present in 757. Macrolide-based treatment was administered to 411 patients (42.1%). These patients were more likely to have CAP than were patients not receiving macrolide-based therapy (35.3% vs. 13.3%; p<0.001) and had lower scores on the CURB-65 tool, a measure of the severity of illness (2.4±1.5 vs. 3.1±1.3; p<0.001). Patients receiving macrolides also had a lower hospital mortality rate in univariable analysis (12.7% vs. 27.2%; p<0.001). A propensity score analysis showed that macrolide-based treatment was associated with a lower in-hospital mortality rate (adjusted odds ratio [AOR] 0.67; 95% confidence interval [CI] 0.54–0.81; p=0.043). Separate propensity score analyses of patients with CAP (AOR 0.20; 95% CI 0.11–0.34; p=0.003) and HCAP (AOR 0.81; 95% CI 0.65–1.01; p=0.337) produced discordant findings.
Conclusions:
Macrolide-based treatment was associated with better survival in patients hospitalized with pneumonia. The survival advantage appeared predominantly among patients with CAP.
P
Previous studies have suggested that morbidity and mortality rates are reduced with macrolide-based regimens in patients with CAP [4–7]. We are unaware of any analyses examining the impact of macrolide-based treatment in patients hospitalized with pneumonia that included both patients with CAP and those with HCAP. The increasing population of patients hospitalized with HCAP highlights the importance of determining the clinical significance or lack thereof of macrolide therapy for this important subgroup of patients [8]. Therefore, we conducted a study to determine whether macrolide-based treatment is associated with a survival benefit in a consecutive group of patients hospitalized with pneumonia of either type.
Patients and Methods
Study Design
A retrospective cohort analysis was performed of all patients admitted through the emergency department to Barnes-Jewish Hospital (1,250 beds) with a diagnosis of pneumonia over a 12-mo period (January–December 2010). We excluded patients transferred from other hospitals directly to the wards or to the intensive care unit (ICU). This study was approved by the Washington University School of Medicine Human Studies Committee.
Data Source
One of the investigators (RMR) identified potential study patients by the presence of either a primary or secondary International Classification of Diseases-9-CM code indicative of pneumonia. Patients with pneumonia were further identified using the definitions described below. The initial study database was constructed by merging patient-specific data from the automated hospital medical records and microbiology and pharmacy databases of the hospital.
Definitions
Diagnosis of pneumonia necessitated both signs and symptoms of infection (i.e., elevated white blood cell count or >10% band forms; fever or hypothermia; chest radiograph revealing an infiltrate[s]). One investigator (MHK), blinded to the determination of pneumonia, reviewed the chest images. The diagnosis of a bacterial infection required a positive culture of blood, pleural fluid, sputum, or the lower airways. We also considered a positive urinary antigen test for either Streptococcus pneumoniae or Legionella spp. as documentation of a bacterial infection.
A HCAP was defined as pneumonia in a patient admitted to the hospital with one of the following risk factors: (1) Residence in a nursing home, rehabilitation hospital, or other long-term nursing facility; (2) hospitalization within the immediately preceding 12 mo; or (3) receiving outpatient hemodialysis, peritoneal dialysis, wound care, or infusion therapy necessitating regular visits to a hospital-based clinic. We also determined the presence of an immunocompromised state, defined as being seropositive for the human immunodeficiency virus (HIV), active malignancy undergoing chemotherapy, or treatment with immunosuppressants (i.e., 10 mg of prednisone or equivalent or a similar agent daily for at least 30 d).
Antimicrobial treatment was classified as being appropriate if the initially prescribed antibiotic regimen was active against the identified pathogen, as judged by in vitro susceptibility testing. Patients with pneumonia attributed to Legionella spp. were defined as receiving appropriate treatment if their initial antibiotic regimen included a macrolide (e.g., azithromycin) or respiratory quinolone (e.g., moxifloxacin). Appropriate antimicrobial treatment had to be prescribed within 24 h of hospital admission.
Statistics
Discrete variables were expressed as counts (percentage) and continuous variables as mean±standard deviation (SD) or medians with the 25th–75th percentile interquartile range (IQR). The X2 test or Fisher exact test was used for categorical variables and the Student t-test or the Mann–Whitney U test for continuous variables as appropriate. Multivariable stepwise logistic regression analysis was used to assess the impact of explanatory variables on outcome (in-hospital death). To avoid spurious associations, only variables with a relation in univariable analysis (p≤0.1) or a potential plausible relation to the outcome were entered in the logistic regression models.
In addition, the effectiveness of macrolide therapy on the hospital mortality rate was estimated further using propensity scores. These scores were estimated by fitting a logistic regression model. The covariates included in the propensity score model were those measured previous to macrolide treatment having a potential impact on outcome: Age, CURB-65 score, Charlson comorbidity score, gender, chronic obstructive pulmonary disease (COPD), congestive heart failure, chronic renal disease, hematologic or malignant disease, solid tumor, diabetes mellitus, immunosuppression including the presence of human immunodeficiency virus (HIV), dementia, recent hospitalization, admission from a nursing home, and antibiotic treatment within the previous 90 d. Propensity score quintiles were derived, and boxplots of the estimated propensity scores for macrolide-treated and -untreated patients within each quintile of the propensity scores were plotted to assess the validity of the analysis. Finally, we fitted a logistic model for in-hospital death, including as covariates the propensity score and macrolide treatment. Results are presented as adjusted odds ratios (AORs) and 95% confidence intervals (CIs). Additionally, we repeated these analyses for the subgroups of patients with CAP and HCAP. Finally, we performed a logistic regression analysis for the subgroup of patients receiving macrolide therapy to determine the factors associated with survival. For all analyses, p values<0.05 were considered significant. We used SPSS for Windows 19.0 (SPSS, Chicago, IL) for all analyses.
Results
Nine hundred seventy-seven consecutive patients with pneumonia admitted to Barnes-Jewish Hospital in 2010 were included in the study. The mean age of the patients was 60.5±16.9 y (range 17–102 y) with 544 men (55.7%) and 433 women. Approximately three-quarters of the patients were hospitalized with HCAP (77.5%), and the remainder had CAP. The average CURB-65 score, a measure of illness severity was 2.8±1.4 (median 3.0; 25th and 75th percentiles 2.0 and 4.0).
Macrolide-based therapy was administered to 411 patients (42.1%). Clarithromycin was given to one patient and azithromycin to 410 patients (99.8%). Patients receiving macrolide-based therapy were statistically younger, were more likely to be African-American, had lower CURB-65 and Charlson comorbidity scores, were less likely to have dementia or be in a bed-bound state, and were less likely to require hemodialysis than patients who did not receive a macrolide-based regimen (Table 1). Patients treated with macrolides were also significantly less likely to be immunosuppressed, have had a recent hospitalization, have been admitted from a nursing home, and have HCAP than patients not treated with a macrolide. The number of HCAP risk factors was statistically lower for patients receiving macrolides (1.3±1.2 vs. 2.0±1.1; p<0.001). Hospital length of stay was significantly shorter for patients receiving macrolide-based therapy (10.2±12.3 d vs. 12.7±15.0 d; p=0.005).
CURB-65=
Abbreviations: COPD=chronic obstructive pulmonary disease; HCAP=healthcare-acquired pneumonia; HIV=human immunodeficiency virus.
The pathogens associated most commonly with pneumonia were methicillin-resistant Staphyloccocus aureus (MRSA)(22.7%), S. pneumoniae (19.1%), Pseudomonas aeruginosa (19.1%), methicillin-sensitive S. aureus (MSSA) (14.1%), and Haemophilus influenzae (8.0%) (Table 2). Patients receiving macrolide-based therapy were significantly more likely to be infected with Legionella spp., Haemophilus influenzae, S. pneumoniae, and other Streptococcus species than patients not receiving a macrolide. Patients not receiving macrolide-based treatment were more likely to be infected with Escherichia coli, Klebsiella pneumoniae, MRSA, and Pseudomonas aeruginosa. Polymicrobial infection occurred in 139 patients (14.2%) and was less common in patients treated with macrolides. Secondary bacteremia developed in 336 patients (34.4%) with similar occurrences in patients treated with and those not receiving a macrolide drug.
Abbreviations: ESBL=extended-spectrum β-lactamase; MRSA=methicillin-resistant Staphylococcus aureus; MSSA=methicillin-sensitive S. aureus.
The overall hospital mortality rate was 21.1% (n=206). The rate was lower among macrolide-treated patients (12.7% vs. 27.2%; p<0.001). In-hospital death was associated with older age, greater CURB-65 and Charlson comorbidity scores, whereas race, end-stage liver disease, hemodialysis, immunosuppression, recent hospitalization, admission from a nursing home, and HCAP (Table 3). The number of HCAP risk factors was statistically greater among nonsurvivors (2.0±1.2 vs. 1.6±1.2; p<0.001). The hospital length of stay was similar for nonsurvivors and survivors (12.2±19.6 d vs. 11.5±12.1 days; p=0.495). Kaplan-Meier curve analysis demonstrated that hospital survival was significantly greater for macrolide-treated patients (both CAP and HCAP), and the survival difference was more pronounced for the CAP subgroup (Fig. 1). There was no difference in survival of the HCAP patients receiving and not receiving macrolide-based therapy.
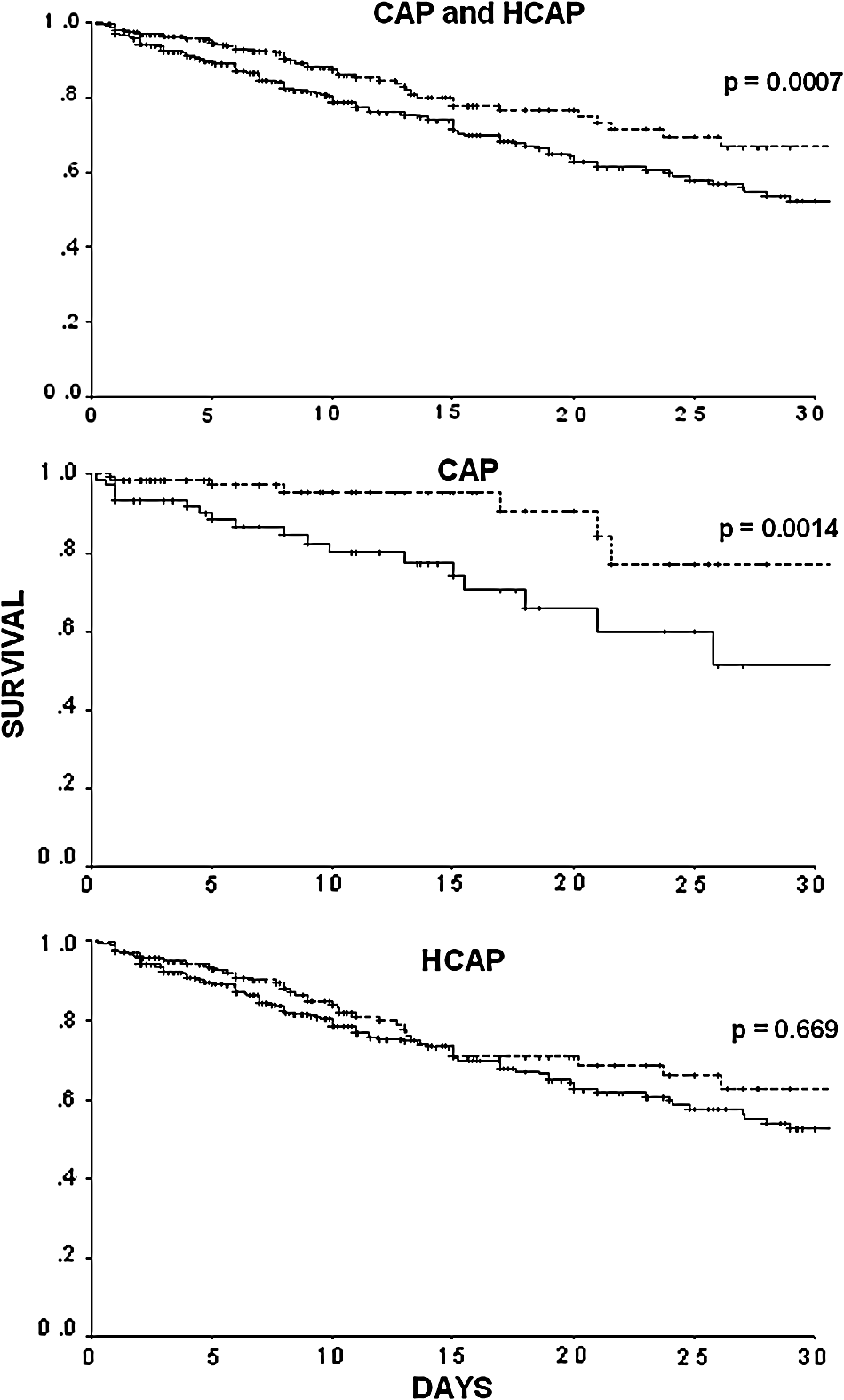
Kaplan-Meier curves for patients with community-acquired pneumonia (CAP) and healthcare-associated pneumonia (HCAP) receiving macrolide-based (broken line) and non-macrolide-based (solid line) regimens.
CURB-65=
Abbreviations: COPD=chronic obstructive pulmonary disease; HCAP=healthcare-acquired pneumonia; HIV=human immunodeficiency virus.
A logistic regression analysis adjusted for severity of illness (CURB-65, Charlson comorbidity score) and potential confounding factors (congestive heart failure, COPD, dementia, end-stage liver disease, diabetes, solid tumor, lymphoma, leukemia, HIV infection, age, gender, recent hospitalization, admission from a nursing home, immunosuppression, and previous antibiotic administration) found that macrolide use was significantly associated with survival (AOR 0.63; 95% CI 0.52–0.77; p=0.021). Similarly, the propensity score analysis found macrolide use to be significantly associated with a lower mortality rate (AOR 0.67; 95% CI 0.54–0.81; p=0.043). The overlapping of the propensity scores for macrolide-treated and non-macrolide-treated patients within each propensity score quintile reinforced the validity of the propensity score analysis (Fig. 2). Propensity score analysis for the subgroup of patients with CAP demonstrated macrolide use to be associated with a lower mortality rate (AOR 0.20; 95% CI 0.11–0.34; p=0.003); however, for the subgroup with HCAP, there was no demonstrable effect of macrolide treatment on the mortality rate (AOR 0.81; 95% CI 0.65–1.01; p=0.337).

Box plots of propensity score quintiles (Q) for patients with and without macrolide-based therapy.
A logistic regression analysis of the subgroup of patients receiving macrolide therapy identified only two independent predictors of a lower mortality rate despite including all identified co-morbidities and the individual HCAP risks. Absence of mechanical ventilation (AOR 0.33; 95% CI 0.25–0.44; p<0.001) and lower CURB-65 scores (one-point decrements)(AOR 0.52; 95% CI 0.44–0.61; p<0.001) were independently associated with a lower mortality rate among macrolide-treated patients (Hosmer-Lemeshow goodness-of-fit p=0.783).
Discussion
We demonstrated that the use of macrolide-based therapy was associated with a lower risk of in-hospital death among consecutive patients admitted to the hospital with pneumonia. However, our sensitivity analysis suggests that this benefit is seen primarily in patients with CAP, not those with HCAP. Not surprisingly, the distribution of pathogens in patients with CAP and HCAP differed, with S. pneumoniae being the predominant bacterium isolated in patients with CAP and S. aureus and P. aeruginosa being the most common bacterial pathogens associated with HCAP. We also found that among patients treated with macrolides, only mechanical ventilation and CURB-65 scores predicted the risk of death.
Previous studies have demonstrated the potential benefit of macrolide-based therapy in patients with CAP. Asadi et al. conducted a meta-analysis that included 23 studies and 137,574 patients with CAP [7]. Overall, macrolide use was associated with a statistically significant mortality reduction compared with nonmacrolide use. However, there was no survival advantage, and study heterogeneity was reduced when analyses were restricted to randomized trials or to patients treated with guideline-concordant antibiotics (macrolide/beta-lactam or respiratory fluoroquinolones). Another recent meta-analysis reviewed 28 studies of CAP, with the main objective being to estimate the mortality rate and the proportion with treatment failure using regimens containing atypical antibiotic coverage compared with those that had typical coverage only [9]. There was no difference in the mortality rates between the atypical-drug arm and the non-atypical arm. The atypical arm showed an insignificant trend toward greater clinical success and a significant advantage in bacterial eradication, which disappeared when evaluating methodologically high-quality studies alone. Taken together, these meta-analyses, as well as other clinical studies, suggest that guideline-based coverage of atypical pathogens in CAP may be most important in determining clinical outcomes, including the mortality rate and bacterial eradication [7,9,10].
Other investigators have found mixed results with the use of macrolides in the treatment of community-based respiratory infections. Martín-Loeches et al. used a propensity score analysis and found that macrolide-based treatment was not associated with a better survival rate in critically ill patients with viral pneumonia attributed to influenza virus H1N1 [11]. However, recent studies in COPD [12], cystic fibrosis [13,14], bronchiolitis obliterans syndrome [15], and asthma [16] suggest that macrolides may confer benefit to patients with community-based respiratory illnesses that are at least partially attributed to respiratory infections for their pathogenesis. In addition to their antimicrobial properties, macrolides have been believed to benefit patients with inflammatory lung diseases, including CAP, through anti-inflammatory mechanisms. Azithromycin significantly reduces airway neutrophilia and interleukin-8 mRNA expression [17]. The anti-inflammatory and immunomodulatory activity of macrolides purportedly contribute to their successful use as therapeutic agents for chronic lung diseases, including cystic fibrosis and diffuse panbronchiolitis [18].
Recent increasing rates of macrolide resistance in S. pneumoniae have brought into question the overall utility of this class of antibiotics for use in CAP [19]. However, macrolides have antimicrobial activity against P. aeruginosa in eukaryotic media through increased uptake and reduced efflux of the drug despite high minimum inhibitory concentrations (MICs) on conventional media (cation-adjusted Mueller–Hinton broth) [20]. Despite these observations, the reported beneficial influence of macrolide therapy on outcomes in acute pneumonia is still observed primarily in CAP [7]. The potential antimicrobial influence of macrolides on P. aeruginosa may explain, in part, their efficacy in patients with cystic fibrosis and other chronic lung diseases [13,14].
Our current study has several major limitations. First, we restricted our analysis to patients with microbiologically confirmed bacterial infection. This likely contributed to the smaller number of patients with CAP compared with HCAP [21]. We have shown previously that patients with culture-negative HCAP do as well with traditional CAP treatment as with treatment targeting HCAP [22]. It is possible that had we included culture-negative patients in our study, we might have seen a mortality benefit with macrolide therapy in patients with HCAP. Moreover, it is possible that some of our positive cultures from the respiratory tract reflected colonization rather than true infection. This seems to be a lesser concern, however, given the adjudication of the radiographic criteria and the relatively large percentage of patients with concomitant positive blood cultures. Second, the criteria for HCAP are somewhat arbitrary and have been disputed as markers of antibiotic resistance in patients presenting with pneumonia [23]. Third, we modified our criteria for HCAP from the 2005 American Thoracic Society/Infectious Disease Society of America guidelines by including patients with hospitalization up to one year earlier [24]. This was done because of the limited number of good-quality studies reporting on the relation of timing of prior hospitalization and antibiotic exposure to subsequent development of antibiotic-resistant infections and the results of a recent meta-analysis suggesting that the effects of previous antibiotic prescription on resistance emergence were conspicuous for as long as 12 mo after exposure [25].
It is important to note that we did not evaluate systematically for concomitant viral infection. Given the possibility that some patients with acute viral infections will present with pneumonia, we may have diluted the influence of macrolide therapy, especially among patients with HCAP, given the recent Spanish experience [11]. It also is possible that the difference in outcomes associated with macrolide therapy between patients with CAP and those with HCAP was attributable to some underdetermined confounding factor. For example, there were more patients with immunosuppression in the HCAP group, which may have influenced the patients' response to macrolide therapy. Finally, all nursing home patients do not appear to be the same. Previous investigators have shown that among nursing home patients, prior antibiotic administration and daily living activity are the best predictors of infection with HCAP pathogens [26]. However, we captured the presence of a bed-bound state and prior antibiotic exposure in our analysis, so our assessment of the nursing home patients should have been complete in this regard.
In conclusion, our data suggest that macrolide therapy is most effective in patients with CAP, and we could not demonstrate any influence of these drugs on the survival of patients with HCAP. This suggests that the use of macrolides in pneumonia should be based on the published guidelines that recommend their use when a clinical or epidemiologic suspicion of infection with atypical pathogens exists, primarily in patients with CAP [3]. The clinical use of risk factors to identify patients at risk for HCAP may assist clinicians in detecting patients who are unlikely to benefit from macrolide therapy.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest in relation to this work. Dr. Kollef's efforts were supported by the Barnes-Jewish Hospital Foundation.