
Abstract
Abstract
Background:
Blood stream infections (BSIs) are a common source of morbidity and death in hospitalized patients. We hypothesized that the proportions of bacteremia from gram-positive and fungal pathogens have decreased over time, whereas rates of gram-negative bacteremia have increased as a result of better central venous catheter management.
Methods:
All U.S. Centers for Disease Control and Prevention-defined BSIs in patients treated on the general surgery and trauma services at our institution between January 1, 1998, and December 31, 2009 were identified prospectively. These cases were analyzed on a yearly basis to compare rates of various infections over time. The Cochran-Armitage test for trend was used to evaluate categorical data, whereas the Jonckheere-Terpstra test for ordered values was used to analyze continuous data.
Results:
A total of 1,040 patients had 1,441 episodes of BSI caused by 1,632 strains of bacteria or fungi. There was no difference over time in the proportion of BSI among overall infections. Rates of BSI for gram-negative and fungal pathogens increased over time (p=0.03 and<0.0001, respectively), whereas rates of gram-positive BSI decreased (p<0.0001). Positive changes in anaerobic BSI approached statistical significance.
Conclusion:
Although our hypothesis was only partly true, over the last 12 y, our institution clearly has witnessed a shift in the types of organisms causing BSIs. There was a decrease in the rates of BSI caused by gram-positive pathogens with an associated increase in the rates of BSI of infections by fungal and gram-negative pathogens. Interventions to reduce institutional rates of BSI should include targeted therapies based on historical institutional trends.
H
Although there have been many publications relating to shifts in antimicrobial resistance or central venous line-associated BSIs (CLABSI) over time, there has been little effort to document shifts in the organisms and organism classes contributing to non-central line-related BSI. With improved adherence to contact precautions, full barrier procedural methods, and hand hygiene initiatives, we hypothesized that the proportions of bacteremia from gram-positive and fungal pathogens would have decreased over the last several years whereas gram-negative BSIs would have increased proportionally. We hypothesized further that the decrease in gram-positive and fungal BSIs would have resulted in lower overall rates of BSI.
Patients and Methods
We analyzed a prospectively collected and maintained surgical infections database that includes all cases of infection from the general surgical, trauma, and transplantation services at our institution. This database is maintained by a thrice-weekly patient review, including a chart reading, direct patient examination, as well as consideration of all laboratory, microbiology, radiology, and pharmacology reports. We used this database to identify all U.S. Centers for Disease Control and Prevention (CDC)-defined BSIs occurring between January 1, 1998, and December 31, 2009 [6]. Our goal was to evaluate the clinical BSI spectrum apart from those directly attributable to central line infections. Therefore, for the purposes of our study, all central line-related BSIs were excluded, but CLABSI were included, as these are not considered separate from other forms of BSI in our database. Polymicrobial BSIs were treated as a single BSI event, but each infecting organism was counted individually. Organisms are listed as described in the culture data and are not counted twice. Organisms listed in the more generic form (for example, Staphylococcus aureus instead of methicillin-resistant or methicillin-sensitive S. aureus) could not be classified further by our microbiology laboratory. Demographic information was analyzed on a per-infection basis. The rest of our analysis was performed on a per-organism basis.
Significant trends in demographic information for the study period also were analyzed. The Cochran-Armitage test for trend was used to evaluate categorical data, and the Jonckheere-Terpstra test for ordered values was used for continuous data. Reported p values for the Cochran-Armitage test are two-sided, whereas p values for the Jonckheere-Terpstra test are one-sided by definition. All continuous data are reported as the median and interquartile ranges. Data analysis was performed using SAS software, version 9.3 (SAS Institute, Cary, NC).
The total numbers of gram-positive, gram-negative, anaerobic, and fungal pathogens were evaluated for each year of the study. Trends in the proportion of isolated organisms per year were evaluated using the Cochran-Armitage test for trend with significance assigned p<0.05. A subgroup analysis was performed in a similar manner based on the place where the infection began (community, hospital, intensive care unit [ICU], or other), as well as its classification as hospital-acquired, community acquired, or healthcare-associated but not hospital-acquired. The “other” group consists largely of patients transferred to our facility or cases where the location could not be specified. Further analysis was carried out on each organism within each group.
Results
We identified 1,040 patients with 1,441 blood stream infections and isolated 1,632 organisms over the study period. Rates of BSI as a proportion of all infections during the study period were between 11.2% and 14.6% (p=0.84 for the proportion of BSIs compared with other types of infections). The BSI rates per 100 admissions ranged from 17.9 to 26.1. Table 1 lists trends in demographic information for the study period on a per-infection basis. A lower proportion of BSIs occurred in transfusion recipients and trauma patients, whereas transplant patients made up a larger proportion over time. There were no differences in the number of elderly (age >65 years) or patients with human immunodeficiency virus infection over the study period. The rate of corticosteroid use increased with time. Community-acquired infection rates decreased over time, whereas healthcare-associated, non-community acquired BSI rates increased. The mean mortality rate over the study period was 22% and did not differ with time. Fungal BSI was associated with the highest mortality rate. Demographic information organized by organism class is provided in Table 2.
Analysis of trend for continuous variables obtained via the Jonckheere-Terpstra test with associated one-sided p values. Trends in discrete variables are analyzed via the Cochran-Armitage test with associated two-sided p values.
Continuous variables are expressed as medians with 25%–75% interquartile range (IQR). Discrete variables are listed as the number of occurrences with percent.
Infection rate (per 100 admissions).
Adu=admissions; APACHE=Acute physiology and Chronic Health Evaluation; ASSOC=associated; ACQ=acquired.
Continuous variables are expressed as medians with 25%–75% interquartile range in parentheses. Discrete variables are listed as the number of occurrences with percent. Tests represent trends in proportions of infections. All p values are two-sided.
adm=admissions APACHE=Acute Physiology and Chronic Health Evaluation.
Gram-negative and fungal infections constituted increasing proportions of the total BSI, whereas gram-positive BSI decreased over the study period (Fig. 1). A similar pattern was identified for hospital-acquired infections. Gram-positive infections in the ICU fell, whereas fungemia increased (Table 3). Gram-positive infections declined on the wards, but no other trends were noted for this location.
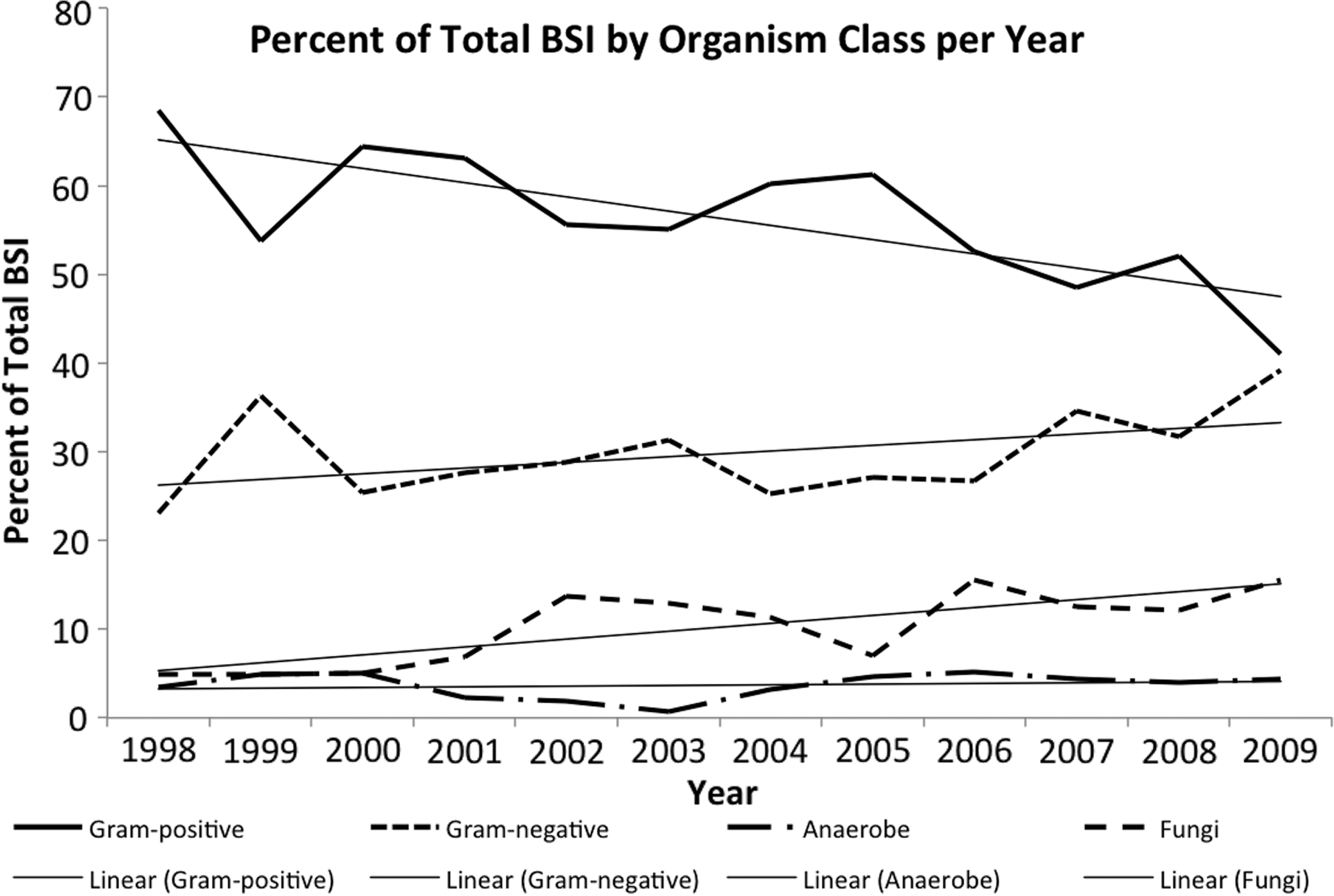
Changes in gram-negative, fungal, and gram-positive blood stream infections over the study period.
Values listed per 100 admissions. Tests represent trends in proportions of infections.
GP=Gram-positive; GN=gram-negative; AN=anaerobe, F=fungi.
All p values are two-tailed and were obtained via the Cochran-Armitage test for trend.
The decline in overall gram-positive rates is attributable almost entirely to declining rates of infections with Staphylococcus epidermidis, most of which were caused by methicillin-resistant organisms (MRSE). The rate of vancomycin-resistant Enterococcus faecium (VRE) infection increased over the study period. Rates of infection by Pseudomonas aeruginosa and Acinetobacter decreased, whereas Klebsiella pneumoniae contributed an increasing proportion of gram-negative BSI infections. There were no statistically significant trends in anaerobic BSI over the study period. Candida glabrata became the predominate fungal isolate over time, and C. albicans and other yeast isolates declined. The most common organisms in each class, excluding anaerobes, are listed in Table 4. Full results per organism are listed in Supplemental Tables A–D.
All p values are two-tailed and were obtained via the Cochran-Armitage test for trend.
Values listed per 100 admissions.
MRSE=methicillin-resistant Stephylococcus epidermis; MRSA=methicillin-resistant S. aureus; VRE=vancomycin-resistant Euterococcus; CNS=coagulase-negative staphylococci.
After observing the trends in fungal isolates, we performed a post-hoc analysis to identify trends in our administration of fluconazole and fluoroquinolones. We identified no trend in our usage of fluoroquinolones over the study period. We did, however, find a striking trend toward greater fluconazole usage (3.3% in 1998 to 31.4% in 2009; p<0.0001). Further analysis to correlate corticosteroid use with C. glabrata candidemia did not show a statistically significant difference (21.0% vs. 21.6%; p=0.93). However, we demonstrated a significant association between receipt of fluconazole and lower rates of C. glabrata compared with other Candida species (69.8% vs. 52.9%; p=0.04).
Discussion
Although the number of BSIs was fairly steady over time, our analysis revealed a long-standing trend toward decreasing gram-positive infections. This reduction was attributable almost entirely to a lower number of infections with S. epidermidis (mostly MRSE), whereas S. aureus and MRSA rates remained steady (Table 4). This finding is contrary to published reports of declining S. aureus and MRSA rates [1, 7, 8]. Other reports have noted decreasing rates of infections with coagulase-negative staphylococci [9]. This trend was noted for all hospital-acquired infections, occurring in both the ICU and the hospital ward.
Decreasing rates of BSI caused by S. epidermidis probably are attributable to lower rates of CLABSI. Well-established interventions, such as promotion of hand hygiene, emphasis on sterile technique for line placement, and prompt removal of unneeded central venous lines and peripherally placed lines for long-term use all contribute to lower rates of infection by these organisms [7,10]. However, our findings are more indicative of a shift in the background flora of our institution. Our hospital instituted full barrier protocols for all central line insertions in 2004. The remainder of our full bundle, including procedural checklists, chlorhexidine skin cleanser, procedure “full stop” capabilities for nursing staff, and catheter maintenance procedures, was not formally instituted until 2009. Our central line bundle now guides the insertion, maintenance, and dressing care for all central lines. Therefore, full barrier precautions, more than other interventions, contributed to the lower rates of CLABSI and subsequently overall gram-positive BSI.
Gram-negative BSI is a highly morbid condition associated with a greater degree of illness, as indicated by greater Acute Physiology and Chronic Health Evaluation II scores. They are commonly found in conjunction with intra-abdominal infection, with Escherichia coli being the most common pathogen [3]. Although our E. coli BSI rates were stable over the study period, our rates of K. pneumoniae rose during this time. Blood stream infections caused by Pseudomonas aeruginosa and Acinetobacter deceased. We noticed a significant increase in the proportion of nosocomial gram-negative bacteremia that was not associated with a particular location in the hospital, although the proportion of in-patient gram-negative BSI approached significance. Aung et al. reported an increase in community-acquired BSI, which was not observed in our study. However, those authors did have a near-significant increase in in patient BSI, as seen in our results [8]. The exact cause of this increase in gram-negative BSI remains unclear.
Other authors have pointed to an aging population as a cause of higher rates of gram-negative BSI [11, 12]. However, our patients with gram-negative BSI were not statistically older than the other groups, and the median age for BSI remained stable throughout the study period. Albrecht et al. reported a similar increase in gram-negative BSI, which was correlated with greater hospital-wide utilization of levofloxacin. However, our fluoroquinolone utilization remained stable over the study period [13]. Further study will be required to evaluate what impact, if any, shifting trends in anti-microbial utilization have on the spectrum of BSI pathogens in our institution.
Candidemia is associated with the highest rate of mortality. The increase in fungemia was confined to our intensive care unit. An increasing rate of C. glabrata BSI was the primary driver of the higher fungal BSI rate. Non-albicans candidemia traditionally has occurred in elderly and immunocompromised patients [14]. In our study, older patients were more likely to have C. glabrata fungemia; however, both the median age and the proportion of patients above age 65 y have been stable over time. Corticosteroid use increased dramatically during the study period, but steroid exposure was associated with lower rates of fungemia and was not significantly associated with C. glabrata candidemia.
We had anticipated the increase in fungal BSI to be associated with the growing transplant population. However, a smaller percentage of fungemias than infections with other organisms occurred in this population. Therefore, changes in our demographics do not appear to be the primary driver of this pathogenic shift. Similar trends in rates of fungal infection have been demonstrated elsewhere, although the most common Candida species differs by institution [13,15–18]. One study found blood transfusion to be an independent risk factor for non-Candida albicans fungemia [19]. Their findings correlate with our demonstration that patients who received any blood transfusions had a greater risk of fungal BSI. Contrary to the earlier findings, however, our transfusion rates are falling, yet our rates of C. glabrata continue to increase. The greater duration of use of antibiotics is not an unexpected finding, given the longer incubation periods for fungal cultures.
We identified an increase in fluconazole use over the study period, which appears to verify our previous findings demonstrating an association between higher rates of C. glabrata infection and increasing utilization of fluconazole [17]. Surprisingly, we also demonstrated lower rates of C. glabrata in patients who received fluconazole compared with other fungal isolates. Fluconazole use has received mixed reviews as a cause of non-albicans candidemia, with studies supporting both sides of the debate [15,17,20–25]. Our findings add to the dispute in this area. It is possible that patient-level fluconazole exposure correlates with hospital-level emergence of non-albicans species without affecting the infection patterns of the individual patient.
We noted no significant trends in either direction for non-nosocomial BSI, including bacteremia originating from the community. These data suggest that the community pathogenic flora remained largely unchanged over the study period.
Our study has several fundamental limitations. First, our data, although collected prospectively, were analyzed retrospectively, making it difficult to obtain insight into the scenarios regarding individual infections. Second, we are reporting findings from a single institution and therefore, depending on the pathogenic flora at other institutions, our findings may not be generalizable. However, we believe that the decrease in S. epidermidis as a result of better central venous catheter management is likely to be similar to other institutions where central venous line bundles have reduced the rates of CLABSI.
Conclusions
Our initial hypothesis proved to be only partly correct. Although the number of BSI from gram-positive skin flora has decreased with better central line management, the overall number of BSIs has remained stable. Furthermore, the pathogenic flora originating from the community has been stable over this same time period. Further discussion of intervention to reduce healthcare-associated infections and BSI in particular, and the high rates of mortality associated with them, should take into account the spectrum of pathogenic bacteria at each institution. Historic institutional trends should be considered when planning interventions to lower rates of BSI. Unfortunately, it appears that reducing BSI caused by skin pathogens by curtailing the rates of CLABSI is unlikely to impact the mortality rate from this complication significantly.
Author Disclosure Statement
Funding for this study was provided by National Institutes of Health grant T32 AI078875.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.