
Abstract

A
A 59-year-old Caucasian male presented to the emergency department of our institutuion with a 10-h history of acute abdominal pain associated with fatigue, nausea, vomiting, and a temperature of 38.7oC. The patient's medical history included an appendectomy in childhood and orthopedic surgery a few years previously, as well as chronic obstructive pulmonary disease (COPD) from tobacco smoking.
On clinical examination the patient's abdomen was tender with diffuse guarding, absent bowel sounds, and a sizeable scar, apparently from a complicated appendectomy. His complete blood count on admission included a white blood cell count (WBC) of 16,000 ×109 cells /L, which increased 2 h later to 22,000. Ultrasonography and computed tomography (CT) revealed a large cystic mass that occupied most of the patient's right abdomen, displacing bowel loops (Fig. 1). At 6 h after the patient's admission and with a worsening of his status, laparotomy found a sizable abscess with a pseudocapsule inside the greater omentum, without any other inflammatory process being observed (Figs. 2 and 3). A partial omentectomy and debridement of fibrin deposits was done, and post-operative examination of the patient's abscess fluid showed an elevated CEA of 429.5 ng/mL (normal, <10 ng/mL in smokers). Microbiologic investigation isolated Pseudomonas aeruginosa. Pathology described the patient's abscess wall as consisting of reactive connective tissue, pus, multi-nucleated giant cells of foreign-body type, and cholesterol clefts near the abscess wall. Histologic findings were compatible with a fully developed omental abscess (Figs. 4–6).

Appearance on computed tomography (CT) of a large cystic formation, of 5×4×6.5 cm in the peritoneal cavity, with a thickened wall, in contact with the anterior abdominal wall and the right colon, accompanied by mesenteric inflammatory reaction.

Intraoperative photograph showing a sizable abscess with a pseudocapsule found inside the greater omentum.

Specimen of omental abscess after excision.
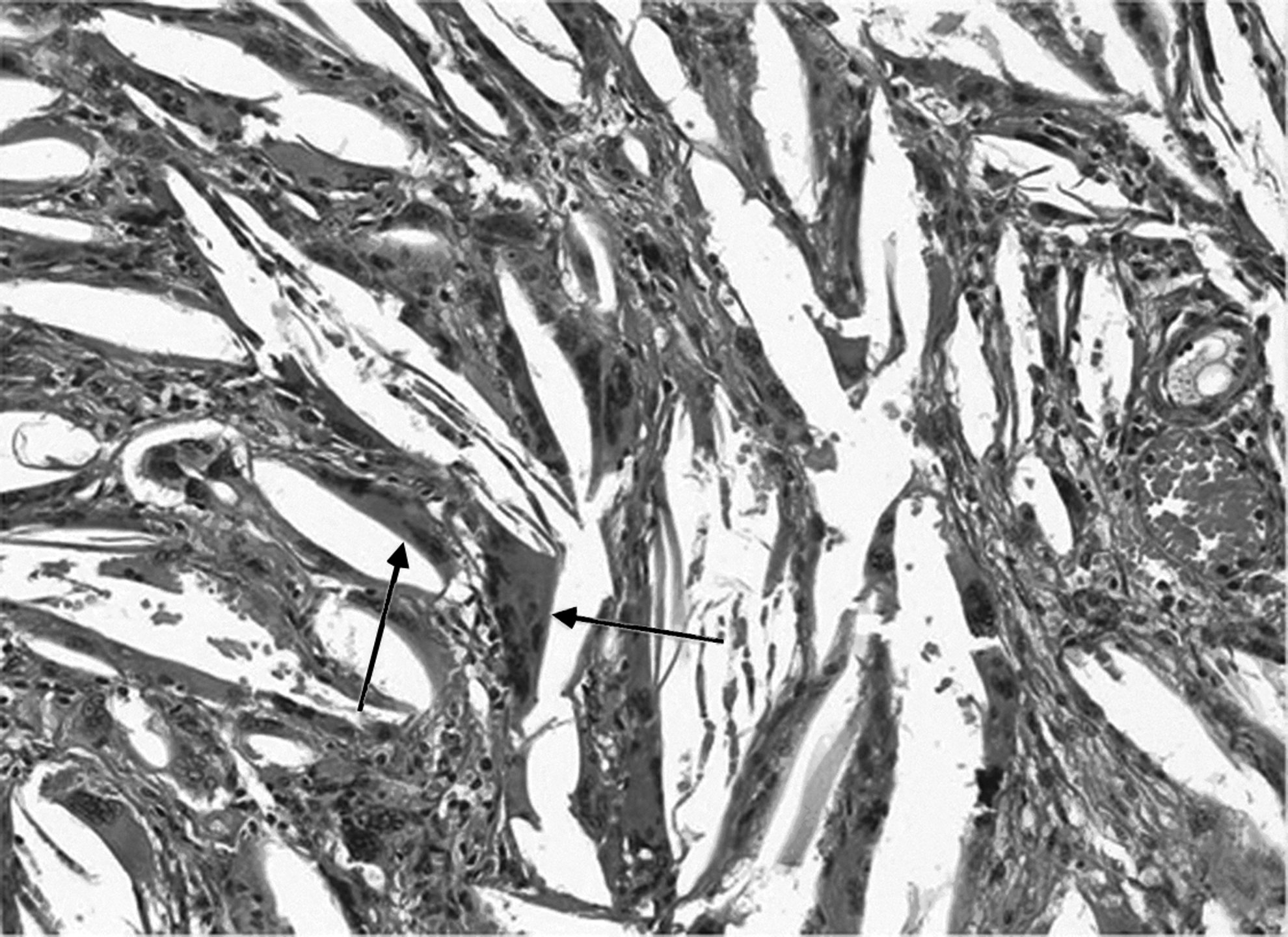
Foreign-body-type multi-nucleated giant cells phagocytosing cholesterol crystals (arrows).
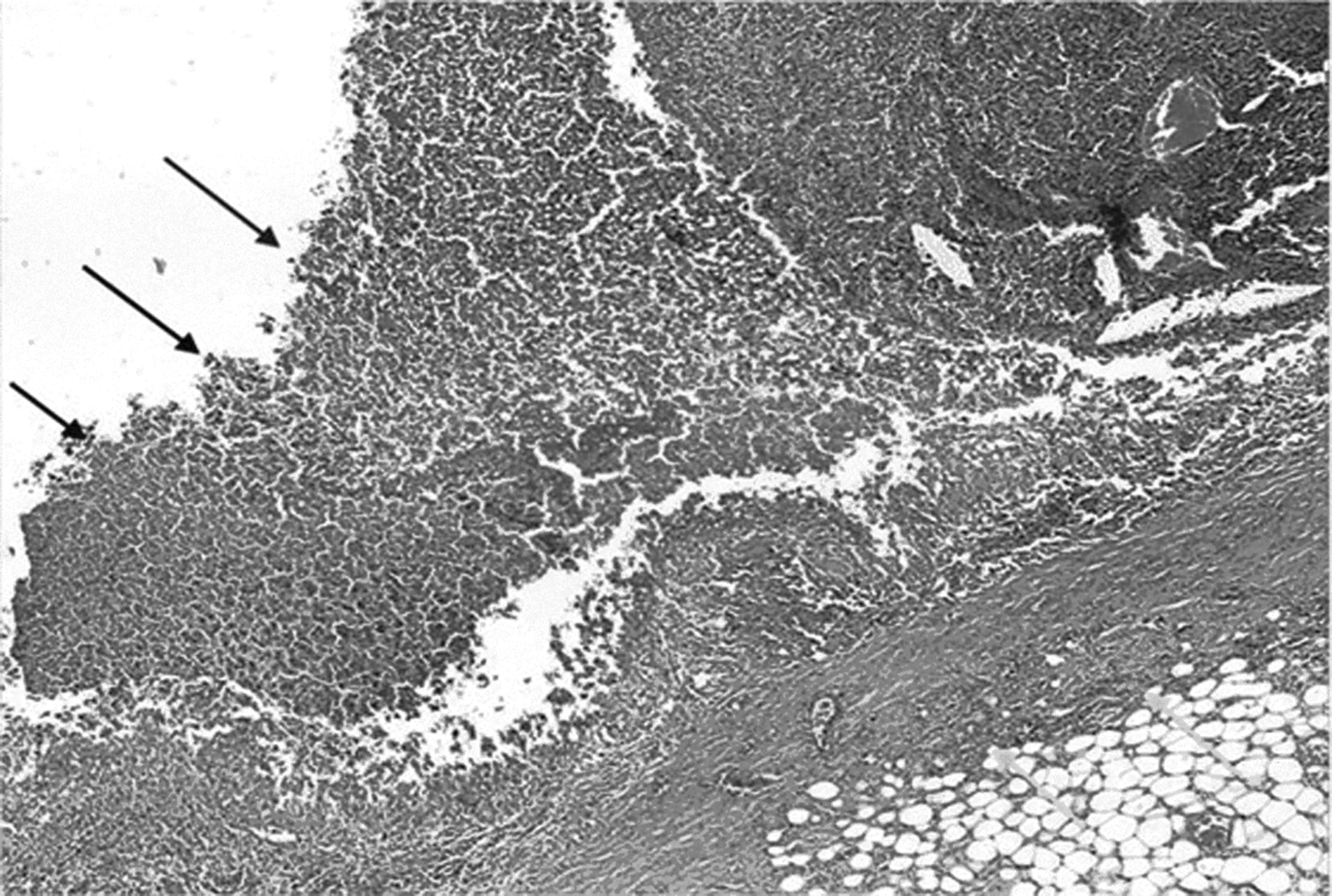
Pus in omental abscess. Arrows: Abscess wall (reactive connective tissue capsule).

Cholesterol clefts near abscess wall (cholesterol crystals that created the clefts were dissolved during specimen preparation). Histologic findings were compatible with a fully developed omental abscess.
An isolated primary inflammatory lesion of the greater omentum is a rare condition. Knoop et al., from 1999–2001, reported four cases of such lesions, manifesting clinically as an acute abdomen with a palpable mass. Two of the cases involved torsion of the omental pedicle, with the remaining two cases representing an entity called paracolic pseudotumor omentitis [3].
Intra-abdominal abscesses can be difficult to diagnose. Their ultrasonographic diagnosis is made difficult by the super-imposition of air-filled loops of bowel. Computed tomography is the imaging modality of choice for intra-abdomonal abscesses, and is most useful in determining the nature and anatomic correlations of a primary omental abscess, but in a number of cases can create diagnostic pitfalls [4]. The literature also reports elevated concentrations of tumor markers in the aspirates of simple abdominal cysts. These markers are hypothesized to be secreted into the intracystic fluid by epithelial cells originating from these cysts [5]. The finding of intra-abdominal cystic lesions suggestive of abscesses related clinically to an acute abdomen should make the operating surgeon suspicious of unusual conditions such as a primary omental abscess (POA). Nor does the presence of elevated concentrations of CEA in a specimen of abscess fluid, which is likely to have been obtained pre-operatively through ultrasound or CT-guided aspiration, necessarily suggest neoplasm, as was the case in our patient with a benign primary omental abscess.
Our experience with the rare clinical entity of a benign primary omental abscess raises two important teaching points: (1) A complete abdominal exploration for a potential etiology of an omental abscess is essential; and (2) elevated concentrations of CEA produced by such an abscess are neither sensitive nor specific for the presence of a tumor, making careful surgical pathologic examination of omental abscess mandatory after its excision.