
Abstract
Abstract
Background:
Extended-spectrum β-lactamase (ESBL)-producing Escherichia coli are of increasing concern as a cause of healthcare-associated infections.
Study Design:
Using a matched case-control design, demographics, antibiotic use, and relevant surgical data were obtained for 173 cases (ESBL E. coli surgical site infections, [SSI]) and 173 controls (antibiotic-susceptible E. coli SSI) in an oncology hospital in Mexico City. Conditional logistic regression modeling was used to calculate odds ratios (OR).
Results:
The mean age of patients was 53.6 years, 214 (62%) were female. Demographics and comorbidities were similar between groups. Although antibiotic prophylaxis was common among both cases and controls (84% and 89%), more than one-half of cases (53%) were given prophylaxis outside the recommended window or were exposed for more than 24 h in comparison to 29% of controls. Patients who received untimely (OR=3.13, 95% confidence interval [CI] 1.5-6.4) and discontinued inappropriately (OR 6.38, 95% CI=2.5-16.2) prophylaxis were more likely to develop an ESBL SSI. In addition, patients with an organ/space infection compared with superficial had a higher rate of a resistant infection (OR 4.2, 95% CI 1.3-13.9). Among patients not given timely or appropriately discontinued prophylaxis, post-operative cephalosporin use (OR 3.3, 95% CI 1.4-7.7) was associated with ESBL E. coli SSIs.
Conclusions:
The appropriate timing and duration of perioperative antimicrobial prophylaxis were associated with lower risk of ESBL E. coli in SSIs. Even though compliance to antimicrobial prophylaxis guidelines is of the utmost importance, reduced exposure to cephalosporins may also potentially decrease the risk of ESBL SSI.
I
Bacteria that produce ESBL have been found with increasing prevalence across both community and healthcare settings. Patients colonized unknowingly in the community may therefore contribute subsequently to patient-to-patient transmission. More specific risk factors known to increase risk of ESBL in hospitalized patients include severe co-morbidities/illness, excessive or prolonged use of antibacterial agents, surgical intervention/invasive procedures, long pre-infection hospital or intensive care unit stay, and use of catheters [3,5,7,9,10]. These factors were observed in several studies, although prior antibiotic therapy was identified as the most prominent independent factor associated with ESBL acquisition.
Surgical site infections (SSI), accounting for more than 20% of HAIs, are reported after about 2% of operations [11]. Aside from the evidence that many of these are preventable, the added task of treating an ESBL Escherichia coli SSI is a major clinical challenge. For the infected patient, treatment options are limited and the risk of mortality or morbidity increases [12]. A SSI is particularly detrimental for immunosuppressed cancer patients when life-saving treatment may have to be postponed. In addition, oncology patients often require antimicrobial therapy, which may increase the risk for the emergence of resistance. However, few studies have described the incidence and risk factors for antibiotic-resistant SSIs among oncology patients [13].
The overall incidence of SSI at the National Cancer Institute of Mexico (INCan) has been steady since 2008, but the proportion of SSI caused by ESBL E. coli has increased. More than one-half (56.1%) of all SSI occurring between 2008 and 2012 were caused by E. coli, 37.1% of which were ESBL E. coli. On average, the yearly incremental increase in the proportion of SSI caused by ESBL E. coli was 3.5% during this time. In addition, the proportion of resistant versus susceptible E. coli infections also increased from 39% in 2008 to 69% in 2012. Because of this increase in ESBL E. coli SSI at the INCan, the aim of this case-control study was to examine the risk factors associated with ESBL E. coli infection compared with antimicrobial susceptible E. coli among surgically treated cancer patients.
Patients and Methods
Study population and case definition
The INCan is a 135-bed referral teaching hospital located in Mexico City for adult patients with cancer. There are approximately 170,000 annual medical visits (more than 800 each day) and more than 3,500 operations performed each year. Patients in this hospital are generally middle-aged adults, 78% being more than 40 years old, and 57.2% are female. Breast and cervical cancer are the two most common neoplasms (13.5% and 7.6% respectively), followed by other gynecological neoplasms (12%), prostate (5.1%) and testicle cancer (4.7%). More than one-half of patients have advanced stages of disease.
All surgical/abscess cultures are analyzed by the hospital microbiology laboratory. Susceptibilities to antimicrobial agents are determined according to criteria of the Clinical Laboratory Standards Institute (CLSI). We defined a SSI if any of the following conditions were met: (1) A physician identified the SSI in the patient's chart, (2) the operation registry indicated a SSI, or (3) the HAI surveillance system reported the SSI according to U.S. Centers for Disease Control and Prevention (CDC) definition criteria [14]. Duplicate cultures of a SSI identified previously were excluded from analysis, and ESBL-producing infections were defined as those resistant to third-generation cephalosporins [4,5,15].
Cases were patients who developed a SSI, as defined by the CDC [16], with an ESBL E. coli detected up to 90 d after operation (or one year in the case of prosthesis implantation) between Jan 2008 and Dec 2012. Controls were SSI with an antimicrobial susceptible E. coli detected up to 90 d after the operation (or one year in the case of prosthesis implantation) between January 2008 and December 2012.
Data collection
Following approval from the Columbia University Medical Center Institutional Review Board and INCan, we obtained data on SSI through review of patient medical records, surgical registry, and HAI surveillance data, using standardized definitions and forms. Patient demographics, risk factors present at admission, and exposure history for each infection were extracted from medical records. Prior exposure data were collected from patient records up to three months before operation, with the exception of cancer treatment history, which was obtained from chemotherapy and radiation records up to a year before operation. Information on post-exposures were collected from records dated between operation and the day of onset of the SSI. Data for operation-related parameters were collected primarily from the surgical registry, and surveillance reports were used as a supplement when information was missing from the registry.
Microbiology information was taken from laboratory records. In brief, strain identification was performed by automated methods (Phoenix 100, Becton Dickinson, Franklin Lakes, NJ). Standard antibiotic panels for agents active against gram-negatives (including beta-lactams, aminoglycosides, and quinolones) were used. Strains showing high resistance to one or more third-generation cephalosporins were identified as potential bearers of ESBL enzyme activity. Confirmation by disk synergy testing of ceftazidime in the presence and absence of clavulanic acid was conducted intermittently as resistance to≥3 third generation cephalosporins (ceftazidime, cefepime and ceftriaxone) has a high correlation (>0.90) with ESBL enzyme activity. On a regular basis, standard strains of E. coli (ATCC25922, American Type Culture Collection, Rockville,) were used as positive and negative controls, respectively [4–6]. The Microbiology Laboratory has monthly external validation through PACAL, a Mexican Institution certified for quality assurance evaluation in medical laboratories.
In 2008 the infection control staff initiated the surveillance of ESBL E. coli. The HAI surveillance data were collected by trained nurses from the Infectious Diseases Department. All SSIs were classified by type of infection as defined by the CDC as either superficial incisional, deep incisional, or organ/space [14].
Risk factors
Demographics
Age, gender, and body mass index were collected from the physical exam performed shortly before operation, and history of diabetes mellitus, hypertension, and smoking status were also recorded.
Antibiotics
Exposure to antibiotics was defined as an antibiotic prescribed either orally or intravenously for a period longer than 24 h. The types and number of antibiotics administered before and after operation but before the onset of infection were recorded. Susceptibility patterns of aminoglycosides, carbapenems, and fluoroquinolones were recorded as well as whether infections were caused by E. coli alone or if the infection was poly-microbial.
Data on antibiotic prophylaxis exposure were retrieved from surgical records. We determined whether patients had received appropriate prophylactic antibiotics by referencing hospital guidelines for each type of operation. For those given prophylaxis, we collected data on the antibiotic used as well as whether it was administered between 20–60 min before the surgical incision and discontinued within 24 h after operation. Hence, for each prophylactic antibiotic we recorded four factors: whether prophylaxis was indicated according to hospital guidelines and, if so, whether it was the appropriate antibiotic and started and stopped at the appropriate time. In cases where any of these four conditions was not met, the patient was described as receiving inappropriate prophylaxis.
Operation and hospital-related factors
Procedures were categorized as breast, gynecologic, gastrointestinal, urologic, head/neck, bone/extremities, abscess drainage, or other operation. The duration of the operation (min), bleeding (mL) and operation category (clean, clean-contaminated, contaminated, or dirty) were recorded [17]. Data regarding cancer treatments up to a year before the operation were categorized as chemotherapy or radiation exposure. Prior hospitalization data within the three months before the operation was classified by the reason for hospitalization (additional operation, infection, or other treatment). Length of stay was expressed by the number of inpatient days, including the day of operation. We also recorded whether patients were discharged from the hospital and readmitted subsequently. If a second surgical procedure was required, the reason (bleeding, dehiscence, infection, or other) and the duration in days between the operations were recorded. Additional hospital-related information obtained was whether an infectious disease consultation occurred and whether an infection at a different body site was present prior to development of the SSI. If the previous infection was caused by E. coli, the site of infection was noted as blood, urine, or respiratory.
Analysis
We used SAS software, version 9.3 (SAS Institute, Cary, NC) for the analysis. Between January 2008 and December 2012, 175 patients had at least one ESBL E. coli SSI (cases) and 183 patients had at least one susceptible E. coli SSI (controls). Cases and controls were matched as closely as possible on time at risk; that is, number of days between operation and onset of infection. A maximum of eight days difference (or 20 d in the case of prosthesis implantation) between a case and control resulted in a total of 173 patient pairs (n=346).
Univariate analyses of each parameter were performed to assess ranges, distributions, and frequencies. Continuous parameters with a non-normal distribution were either transformed to logarithms or analyzed with non-parametric tests. Parameters from matched cases and controls were compared using the McNemar test, Wilcoxon test, or paired Student t-test for discrete, non-normally continuous, and normally distributed continuous parameters, respectively. Parameters with p<0.10 in the univariate analyses were included in forward stepwise conditional logistic regression modeling. Patients given optimal treatment, for example, prophylaxis between 20–60 min before incision, prophylaxis discontinued within 24 h after operation, were used as reference groups to calculate odds ratios. To calculate the odds ratio for the specific type of infection (deep, organ/space), patients with superficial incisional SSI were used as the reference group.
Results
Risk factors
Demographic and general hospital-related descriptors are presented in Table 1. Age and body mass index (BMI) were similar between cases and controls. Cases were on average 53±15 years of age with a BMI of 26±5.5 kg/m2 versus controls who were 54±13 years with a BMI of 27±5.8 kg/m2. Although cases were more often males and had slightly lower rates of diabetes mellitus and hypertension, these differences were not statistically significant. A significantly higher portion of cases (72.3%) had received no cancer treatment in the previous year when compared with controls (56.1%); controls were more likely than cases to have had chemotherapy treatment (11.6% vs. 9.3%) and radiation (32.4% vs. 18.5%, p<0.002).
Readmission after surgical hospitalization but prior to SSI.
Patients undergoing gastrointestinal-related procedures were significantly more likely to have an ESBL SSI when compared with patients undergoing other surgical procedures. In contrast, cases that were least likely had undergone a breast-related operation versus any other procedure. Duration of operation (211 min [SD±125] vs. 192 min [SD±119]) was not significantly different between cases and controls. On average, cases had a longer total length of hospital stay (p<0.02) and higher blood loss (p<0.04) than controls. Surgical procedures of controls were significantly more likely to be categorized as clean and presented with more superficial incisional SSIs, compared with cases; history of prior hospitalizations was not significantly different between cases and controls.
Antibiotic use and resistance patterns
In addition to cephalosporin resistance, significantly more isolates from cases than controls were resistant to amikacin (3.3% and 1.6%, respectively, p=0.7), gentamicin (63.7% and 28.5%, respectively, p<0.0001), and ciprofloxacin (92.8% and 51.5%, respectively, p<0.0001), but not carbapenems (2.3% and 0.6%, respectively, p=0.37). The classes of antibiotics used preoperatively up to three months before, peri-operatively, and following the operation, but before onset of SSI are summarized in Table 2. Controls were significantly more likely than cases to receive no antibiotics preoperatively (70.5% and 57.8%, respectively, p=0.01) and post-operatively (45.1% and 19.1%, respectively, p<0.001). Further, 43.9% of cases received cephalosporin post-operatively (prior to infection) as compared with 23.7% of controls (p<0.001). Cases received more classes and greater numbers of antibiotics in comparison to controls (p<0.002).
+Following operation but prior to onset of infection.
Difference between cases and controls, p<0.03;
Difference between cases and controls, p<0.001.
Among patients given prophylaxis, controls were significantly more likely than cases to have the antibiotic administered and discontinued during the appropriate time frame. Cases were also significantly less likely to receive appropriate prophylaxis, including the appropriate antibiotic and the time when it was discontinued (Table 3).
Up to 3 months before operation.
Following operation but prior to onset of infection.
Readmission factors
Thirty-four percent of patients were re-admitted, with no difference between cases and controls. Of those with readmission, 52 cases (79%) and 35 (66%) controls required a second surgical procedure for complications following the index operation (p=0.1). Complications included bleeding (27.6%), dehiscence (23.0%), infection (32.2%), or other complications (17.2%), but there were no differences between cases and controls in types of complications or in the duration between the index operation and readmission.
Factors associated with ESBL infection
In the multi-variable analysis summarized in Table 4, antimicrobial prophylaxis not administered 20–60 min prior to surgical incision (OR 3.1, 95% CI 1.5-6.4) and inappropriate discontinuation of antibiotics after 24 h of application (OR 6.4 95% CI 2.5-16.2) were predictors of ESBL E. coli SSI. In addition, patients with organ/space infections had a higher rate of ESBL SSI (OR=4.2 95% CI 1.3-13.9) after adjusting for prophylactic predictors (Fig. 1). In a sub-analysis of patients who received prophylaxis outside the 20–60 min window or for longer than 24 h, use of cephalosporin before infection but after operation (OR 3.3 95% CI 1.4-7.7) was a predictor of ESBL SSI.
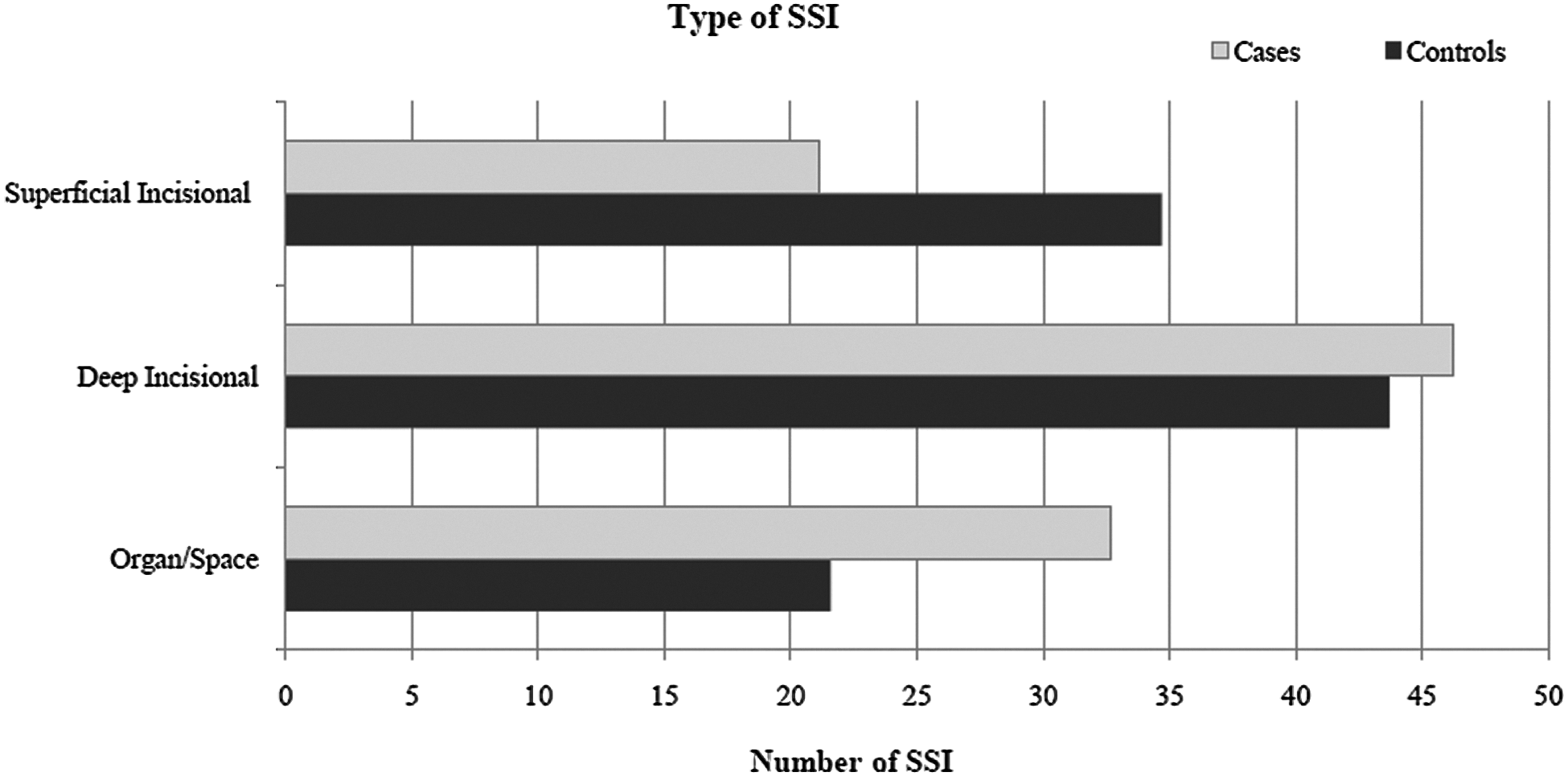
Patients with organ/space infections had a higher rate of ESBL SSI (OR 4.2 95% CI 1.3–13.9) after adjusting for antibiotic prophylaxis predictors.
Following operation and prior to the onset of infection.
OR=odds ratio; 95% CI=95% confidence interval.
Discussion
Operation is a cornerstone in cancer management. Patients with cancer have a higher risk of surgical complications; advanced tumor stages, complexity of the procedure, low serum albumin concentration, obesity, and pre-operative chemo-radiation have been associated with poorer post-operative outcomes. Local adverse factors (e.g., obstruction) as well as immunosuppression may increase further the risk of infectious and non-infectious complications [18–23]. As such, the treatment and care of infection among this population is a priority.
Infections caused by antibiotic-resistant bacteria, especially by the “ESKAPE” pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumanii, Pseudomonas aeruginosa, and Enterobacter species), continue to challenge clinicians, epidemiologists and microbiologists worldwide, and cause morbidity and mortality [24,25]. These and other antimicrobial-resistant organisms have been associated with higher charges, longer length of stay, and increased death rates [26]. With antibiotic resistance increasing worldwide, the risk of SSI caused by resistant pathogens is a serious health threat to cancer patients. At the study hospital, the problem is particularly severe among gram-negative infections because the proportion of antibiotic resistance has increased consistently over the last five years. In particular, ESBL E. coli, having increased in incidence by 118% between 2008 and 2012, has become a primary concern.
In this cohort we also found high rate of resistance to fluoroquinolones, consistent with reports from our hospital and other institutions in Latin America [27–29]. In the ESBL group, fluoroquinolone resistance was 92.8%. Co-associated resistance to fluoroquinolones is common in ESBL E. coli, as it is mediated by different resistance mechanisms, such as, plasmid encoded Qnr proteins [30]. Resistance for aminoglycosides although higher in cases than in controls, was similar to other reports. Amikacin showed potent activity in vitro, followed by gentamicin [31, 32].
Prophylactic antibiotics in operations are currently an important part of good perioperative care. Their efficacy has been demonstrated in clean-contaminated operations and in some clean procedures (e.g., cardiac operation, joint replacement) [33, 34]. For patients at the hospital, inappropriate time of application and duration of prophylaxis were important factors leading to this risk. In our patients, the most important predictor of ESBL E. coli was prophylaxis continued for more than 24 h after operation, and, the initiation of the prophylactic agent without the time window frame (within one hour of the incision). In some reports, antimicrobial prophylaxis not administered within one hour of the surgical incision has been linked to increased rates of surgical infections [35–41] and higher risk of antibiotic resistance [35–37] but to our knowledge, its association with ESBL E. coli SSI has not been reported previously.
After controlling for prophylaxis factors, patients with an organ/space SSI (clean-contaminated abdominal or pelvic operations) were at higher risk of ESBL E. coli. In African countries and India, similar findings have been reported [42, 43]. In patients undergoing liver transplantation, SSI caused by gram-negative organisms are amongst the most common infections, and ESBL E. coli SSI has been found in up to 40% of infected patients [44]. In contrast to the latter, infections in patients undergoing breast operation were primarily superficial and less likely to be caused by ESBL E. coli.
Chemo-radiation before operation has been used preoperatively in the study institution for many years in patients with locally advanced breast cancer who do not respond to neo-adjuvant chemotherapy. In this series, SSI caused by susceptible E. coli were more common in superficial incisional SSIs, many of which were in patients undergoing clean operations, mainly breast. This likely explains the higher proportion of radiation use among controls.
In a previous study from our hospital, among patients with hematologic malignant tumors, hospitalizations within three months of the infection and use of cephalosporins during the previous month were associated with an increased risk of ESBL E. coli blood stream infections [45]. In this current analysis, the use of cephalosporins before infection but after operation was a predictor of ESBL SSI (OR 3.3 95% CI 1.4-7.7). In the study institution, the availability of antibiotics has been limited for a few classes, and cephalosporins have been used widely in surgical patients. Unfortunately, second-generation cephalosporins have frequently been prescribed inappropriately after operation with the belief that longer use of “prophylactic antibiotics” is safer. We hypothesize that the overuse of this specific antibiotic is at least partially responsible for the high rate of cephalosporin-resistant infections.
Cases had longer length of stay compared with controls. Patients with ESBL E. coli infections frequently had undergone gastrointestinal-related procedures and spent more days at the hospital after operation, as is expected in these procedures. This subset of patients also had more organ/space SSIs.
Limitations
The major limitation of this study was its retrospective nature. Data collection and chart review were dependent on the availability and clarity of information from hospital records. Data regarding antibiotic use or risk factors present prior to hospital admission were not available and might bias the information, but we believe that this occurred randomly, as was the prescription of antibiotics during the post-operative period, even outside of the Institution. In any case, bias of measurement was toward the null.
Conclusions
The incidence of ESBL infections is increasing at the INCan and reflects the recent trend occurring worldwide, particularly in developing countries [46–48]. For oncology patients who are exposed commonly to antibiotics, assuring compliance to prophylaxis guidelines and assessing their efficacy are major priorities. Ongoing surveillance of antibiotic resistance patterns of organisms associated with SSI along a strict standardized program on antibiotic prophylaxis would provide a better understanding of key prophylactic antibiotics and the risk of resistance.
Footnotes
Acknowledgments
We thank Bertha Garcia Pineda and Silvia Sandoval Hernandez for their assistance.
Author Disclosure Statement
No competing financial interests exist.