
Abstract
Abstract
Background:
This study reviews our recent experience with deep neck infections in order to propose recommendations in selecting presumptive antibiotics according to imaging characteristics and identifying predisposing factors of life-threatening complications.
Methods:
The records of 161 patients treated for deep neck infections at the Department of Otolaryngology-Head and Neck Surgery, China Medical University Hospital from 2002 to 2012 were reviewed retrospectively. The demographic data, comorbidities, source of infections, complications, duration of hospital stay, imaging characteristics, and bacteriologic studies were evaluated. The involved neck space was determined by computed tomography (CT) scan with contrast. Complications included mortality and life-threatening conditions.
Results:
The most common cause of deep neck infections in our study was odontogenic infection (20.5%), followed by pharyngo-tonsillitis (18.6%), and lymphadenitis (10.5%). The most commonly involved neck space was the submandibular space (40.9%), followed by the carotid space (37.2%), and the para-pharyngeal space (33.5%). Gas formation was detected in 31 (19.3%) cases. Infections of the different neck spaces and patients with gas formation noted on CT scan showed a specific distribution of common microorganisms. Streptococcus spp. was the most common pathogen in submandibular/sublingual space infections. Klebsiella pneumoniae infection accounted for 53.1% of peri-tonsillar/para-pharyngeal space infections, and 40% of carotid space infections. When gas formation was noted on CT imaging, anaerobic infection was the most common pathogen. Chronic kidney disease, diabetes mellitus (DM), multiple space infection, and gas formation present on CT scan were independent predictors of complications (p<0.05).
Conclusion:
The imaging characteristics and microbiology of patients with deep neck infections are correlated and can facilitate the optimal selection of antibiotics. We can administer more precise presumptive antibiotics according to the identified involved neck space on CT scan. Patients with predisposing factors of life-threatening complications require early aggressive multi-disciplinary management to prevent severe sequelae.
D
The clinical consequence depends on the virulence of the causative pathogen, use of appropriate antibiotics, prompt surgical intervention, and individual immunity. The microbiology of deep neck infections is usually polymicrobial in nature, including both aerobic and anaerobic microorganisms. Appropriate empiric antibiotic treatment contributes to successful disease control. Imaging also plays a crucial role in confirming clinical diagnosis, locating extent of the disease, identifying complications, and monitoring disease progression. This study reviewed the imaging characteristics, microbiology, and clinical behavior of deep neck infections in order to propose recommendations in selecting presumptive antibiotics and identifying predisposing factors of life-threatening complications.
Patients and Methods
This was a retrospective study of patients who underwent surgical drainage for deep neck infection at the Department of Otolaryngology-Head and Neck Surgery of China Medical University Hospital between June 2002 and August 2012. Patients with head and neck cancer, superficial neck abscess, traumatic neck wound or iatrogenic neck wound infection, and peri-tonsillar abscess only treated with non-surgical treatment were excluded. Twenty patients who did not have sufficient data to complete the study were also excluded.
One hundred sixty-one patients were enrolled in this study. All patients underwent contrast-enhanced computed tomography (CT). Five millimeter slides from skull base to the upper mediastinum was obtained. The CT scan was extended to include the chest in cases of suspected mediastinitis. Demographic data, comorbidities, source of infections, complications, duration of hospital stay, imaging characteristics, and bacteriologic studies were reviewed. The involved neck spaces were categorized according to Levitt [1]: Peri-tonsillar space, para-pharyngeal space, submandibular space, parotid space, retropharyngeal space, masticator space, pre-vertebral space, pre-tracheal space, sublingual space, carotid space, temporal space, and danger space. Patients with involvement of two or more spaces were classified as multiple-space infections.
The associated facts with complications were analyzed statistically using χ2 test with 0.05 significance level. Fisher exact test was applied if the large sample size assumption was not held. Analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC).
Ethical considerations
The retrospective review of data was performed with strict discretion and confidentiality. All data was anonymized without any personally identifiable information. This study was reviewed and approved by the Institutional Review Board (IRB) of China Medical University Hospital.
Results
The 161 patients in this study included 104 males (64.6%) and 57 females (35.4%), with mean age of 45.4 y (range, 3 mo to 90 y). The age distribution is shown in Table 1. There were 83 patients (51.5%) with underlying systemic diseases, the most common of which was diabetes mellitus (DM; 61 cases, 37.9%). The demographic data and the associated systemic diseases are shown in Table 1. The duration of hospital stay ranged from 2 to 120 d. The mean duration of hospital stay was 13.96 d.
The etiologies of deep neck infections were identified in 95 patients (59.0%). The most common cause was odontogenic infection (33 cases, 20.5%), followed by pharyngo-tonsillitis (30 cases, 18.6%), lymphadenitis (17 cases, 10.5%), sialoadenitis (nine cases, 5.6%), foreign body (3 cases, 1.9%), thyroglossal duct cyst (1 case, 0.6%), brachial cleft cyst (1 case, 0.6%), and tuberculosis (one case, 0.6%).
Computed tomography scans performed on all cases helped identify the involved neck space and the extent of infection. The most commonly involved neck space was the submandibular space (66 cases, 40.9%), followed by the carotid space (60 cases, 37.2%) and the para-pharyngeal space (54 cases, 33.5%). Eighty-six cases (53.4%) presented with multiple neck space infection. Gas formation was detected in 31 (19.3%) cases.
All patients underwent surgical drainage of their neck abscesses. Pus samples were sent for aerobic and anaerobic cultures. The bacterial growth in the pus was 139 patients (86.3%), including 47 (29.2%) with polymicrobial infections. The isolated pathogens and their incidences are shown in Table 2. The distribution of isolated pathogens in three most commonly involved spaces and patients with gas formation on CT scan are shown in Figures 1 and 2. Klebsiella pneumoniae was the pathogen cultured most commonly in the patients with DM. The culture rate of K. pneumoniae in patients with DM was significantly higher than in those without DM (52.46% versus 18%, p<0.0001).

Distribution of common microorganisms in different spaces.

Distribution of common microorganisms in gas formation noted on computed tomography (CT) imaging.
Anaerobic organism in our study including Fusobacterium spp., Peptostreptococcus spp., Clostridium bifermentans, Bacteroides fragilis, Bifidobacterium spp., Veillonella spp., Prevotella intermedia, Propionibacterium acnes.
Of the 161 patients, 39 (24.2%) had complications. Airway distress was the most frequent complication (20 cases, 12.4%), followed by pleural effusion (18 cases, 11.3%), pneumonia (16 cases, 9.9%), septic shock (15 cases, 9.3%), mediastinal involvement (13 cases, 8.1%), and necrotizing fasciitis (nine cases, 5.6%). Four patients died from septic shock (mortality rate, 2.5%). All had multiple systemic diseases, including DM and hypertension in all patients, chronic kidney disease in one patient, chronic obstructive pulmonary disease in one patient, and congestive heart failure and liver cirrhosis in one patient. Factors associated with complications were analyzed and variables significantly associated with complications are shown in Table 3. There were no statistically significant differences in complication rates among different body mass index values, etiologies, and isolated pathogens.
Significant differences are represented in boldface.
Discussion
In this study, odontogenic infection is the most common cause of deep neck infection, followed by pharyngo-tonsillitis. This result is consistent with available literature [2,3]. Odontogenic infection usually spreads continuously from the mandible into the submandibular/sublingual space. This space lies between the mucosa of the floor of the mouth and the superficial layer of deep cervical fascia below. Dental (peri-apical) infection generally breaks through the lingual cortex of the mandible and appears in this space [4].
Odontogenic infection is usually responsible for submandibular/sublingual space infection, whereas infections originating from the tonsils and pharynx are usually related to para-pharyngeal space infections [5]. These findings explain why the submandibular/sublingual and peri-tonsillar/para-pharyngeal spaces are the most frequently involved spaces in our study.
The carotid space was also a frequently affected space in this study. The carotid space is located posterior to the para-pharyngeal space and is usually responsible for deep neck infection in children, which is commonly related to cervical lymphadenitis. This infection is usually well-controlled by intravenous antibiotic therapy [6]. Para-pharyngeal space infection tends to liquefy fat components and form large quantities of pus. Because of the lack of definitive boundaries, para-pharyngeal space infections can spread rapidly to the surrounding spaces and may cause fatal complications including airway compromise, jugular vein thrombosis, Lemierre syndrome, Horner syndrome, mediastinitis, and carotid artery hemorrhage [7–9]. The submandibular space infection is separated by the mylohyoid muscle. If the infection extends to the bilateral supra- and infra-mylohyoid spaces, it is so-called Ludwig angina, which can lead to rapidly progressive airway obstruction [10].
In consideration of the relatively common involvement of the three abovementioned spaces and risk of severe sequelae, the distribution of common microorganisms in these spaces was analyzed. To avoid confusing results and interpretation difficulties, two-or-more-space involvement was excluded from analysis; for example, submandibular/sublingual space involvement were patients with abscess formation at submandibular or sublingual space only without other space involvement. Infections of the different neck spaces show a specific distribution of common microorganisms, similar to the findings by Lee and Kanagalingam [11]. Because few studies describe this finding, this study provides a guide to facilitating optimal selection of presumptive antibiotics.
Empiric antibiotics are administrated before the definitive results of pus or blood cultures become available. Thus, antibiotics should cover against most of the potential microorganisms in deep neck infections. Early start of appropriate antibiotics at the stage of cellulitis can prevent abscess formation [12]. Initial broad-spectrum antibiotics will be replaced by an antibiotic based on the pathogen identified and its antibiotic susceptibility.
The most common anti-microbial regimen prescribed to the patients in this study is intravenous amoxicillin with clavulanic acid (co-amoxiclav). As documented previously, it has coverage against the common pathogens in deep neck infections because more than two-thirds of etiologies are β-lactamase–producing pathogens [13,14]. However, K. pneumoniae infection accounts for 53.1% of peri-tonsillar/para-pharyngeal space infections and 40% of carotid space infections in our study. The high prevalence of decreased susceptibility to co-amoxiclav among K. pneumoniae isolates is demonstrated in early studies and most K. pneumoniae are susceptible to narrow-spectrum cephalosporins [15]. This implies that as the selection of presumptive antibiotics for infections of the peri-tonsillar/para-pharyngeal and carotid spaces should be modified. Prompt CT reading can facilitate the optimal selection of presumptive antibiotics by identifying the involved neck space.
Gas formation is a clue to diagnosis of anaerobic infection [16]. However, few studies have analyzed the bacteriologic pattern of deep neck abscess with gas formation. The present study demonstrates the link between anaerobic isolates and gas formation present on imaging. This information is likely to contribute to prompt identification of potential anaerobic infections and the initiation of appropriate antibiotics.
Treatment of deep neck infections consists of adequate anti-microbial therapy, early surgical drainage of the abscesses, and appropriate management of complications. Surgical drainage is indicated in patients with extensive multiple neck space abscesses, impending complications, infection in immunocompromised patients, or clinical deterioration despite adequate antibiotic use. Non-operative medical treatment can be applied in patients with cellulitis, small amount of abscess (<3 cm), no involvement of danger space (a neck space lies between the alar and prevertebral fascias, the two divisions of the deep layer of deep cervical fascia, and extends from the skull base down into the mediastinum to the level of the diaphragm. Infection here tends to spread inferiorly and resulting in mediastinitis), no impending complication, and no predisposing factors of life-threatening complications [17,18]. The study of Mayor et al. [19] reported successful non-operative medical treatment in 90.32% (28/31), whereas Boscolo-Rizzo et al. [20] reported 226 patients (61.9%) who responded effectively to intravenous anti-microbial therapy alone. Adequate empiric antibiotic selection is more important in patients who can be treated by non-operative treatment because no pus culture is available in this group. Our results may help physicians to apply adequate presumptive antibiotics by identifying involved spaces and gas formation on CT scan. Based on our data and other existing literature, we elaborated an algorithm (Fig. 3) for managing deep neck infections.
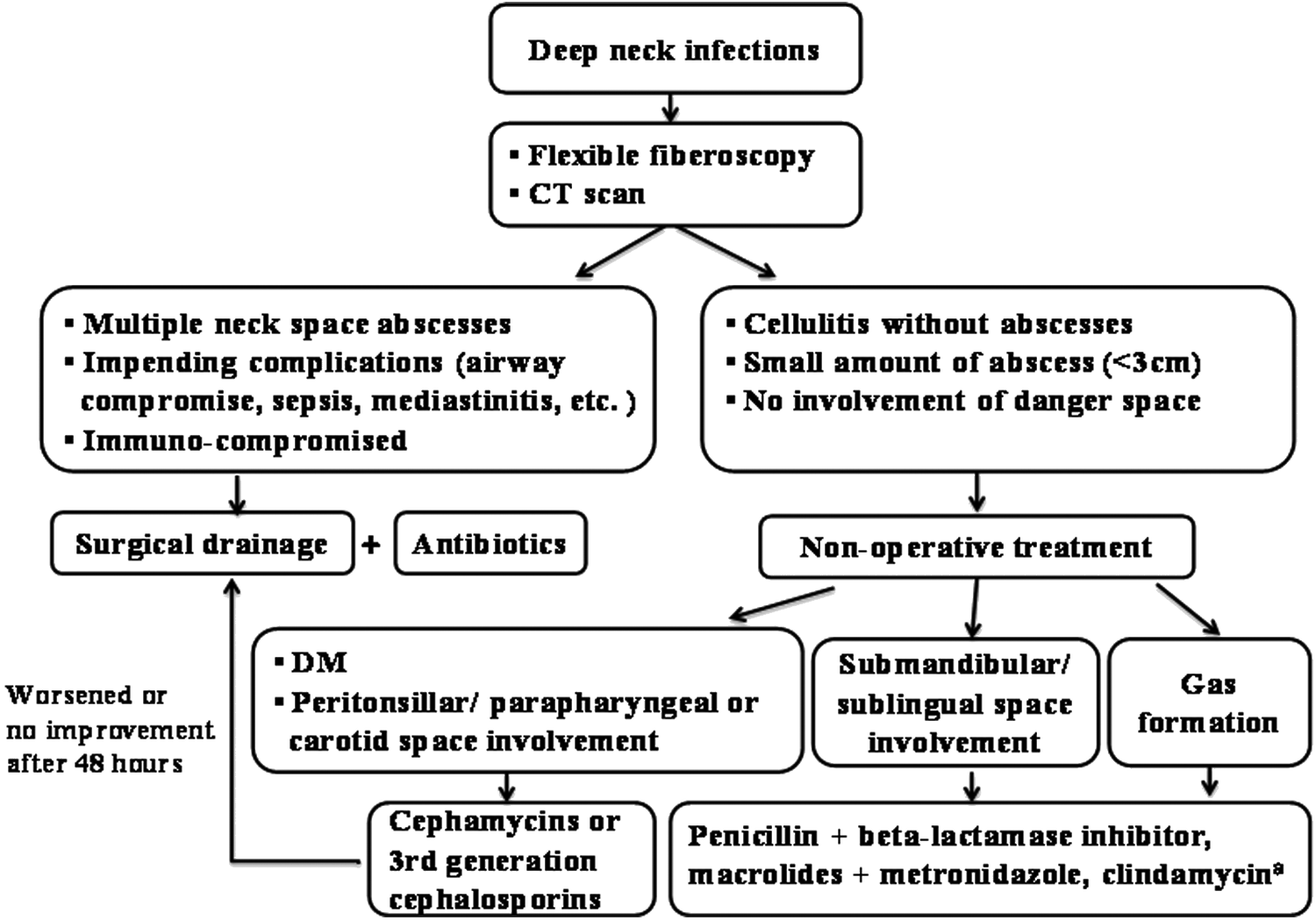
Treatment algorithm in deep neck infections. aClindamycin may no longer be considered a first-line antibiotic in deep neck infections. Clindamycin resistance among strains of Bacteroides fragilis has increased more than 10 y, and current resistance rates reach 20%–50% or more worldwide [20]. CT, computed tomography; DM, diabetes mellitus.
Diabetes mellitus is the most common co-morbidity in this series. Patients with diabetes mellitus are more susceptible to bacterial infections, more likely to develop complications, and have longer hospital stay compared with patients without diabetes because of the dysfunction in polymorphonuclear neutrophil bactericidal function, cellular immunity, and complement activation [21,22]. As has been reported previously [11,23], there was also a close association between DM and K. pneumoniae in our study. The host defense against K. pneumoniae depends on the host's macrophage function, which is impaired in hyperglycemia [24]. Aggressive control of blood glucose concentration in plasma is imperative in treating patients with diabetes with deep neck infection [25].
The limitations of this study included its retrospective, nonrandomized design. Patients who did not undergo surgical drainage were excluded from this study because no pus culture was available for pathogen analysis and low positive rate of blood culture. This may produce selection bias in terms of disease severity. Our study showed specific bacteriologic patterns in different neck space infection and gas formation noted on CT scan. The result was partially similar to the Asian study [11]. Other geographic regions could experience different bacteriologic patterns among patients with neck infections, as has been previously reported [11]. Thus, further studies could be warranted to determine the patterns observed in Western patients.
Conclusions
This study corroborates the specific bacteriologic patterns in different neck space infection and gas formation noted on CT scan. The imaging characteristics and microbiology of patients with deep neck infections are correlated and can facilitate the optimal selection of antibiotics.
Footnotes
Acknowledgments
This work is supported by CMUH-DMR-103-25 and NSC 101-2314-B-039-013-MY3.
Author Disclosure Statement
None of the authors has any conflicts of interest to disclose.