
Abstract
Abstract
Background:
Staphylococcus aureus (S. aureus) is isolated frequently from surgical site infections and other soft tissue infections. There are limited data examining the prevalence of methicillin resistant S. aureus (MRSA) among Egyptian patients after surgery. The current study determined the prevalence of MRSA isolated from surgical site and soft tissue infections at Minia University Hospital (MUH), determined their susceptibility to β-lactams and other antimicrobials, and examined their mecA gene expression.
Methods:
A total of 208 hospitalized patients attending the General Surgery Department at MUH were enrolled and all had skin and soft tissue infections (SSTIs) of different causes. These 208 patients (143 males and 65 females) were suffering from surgical site infection (SSI; n=82), diabetic foot (n=52), abscess (n=45), or burn (n=29) infections. Samples were cultured on different media for isolation and identification of S. aureus and the isolates were screened for antibiotic susceptibility. All MRSA isolates were tested by polymerase chain reaction to detect the mecA gene responsible for methicllin resistance.
Results:
241 Staphylococcal species represented the most common isolates (64.8%) among 371 collected isolates from the 208 patients. Out of the 241 staphylococcal isolates, 127 were S. aureus (61% of the total patients). The prevalence of S. aureus among SSI, diabetic foot, abscess, and burn patients were 59%, 75%, 56%, and 52%, whereas that of MRSA was 16%, 17%, 13%, and 10%, respectively. MRSA isolates (n=31; 15% of patients) showed multiple resistance to at least one member of the antimicrobial groups tested with an average resistance to 6.6±1.9 antimicrobial groups. Polymerase chain reaction data showed that only 29 isolates of the MRSA isolates (94%) were positive for mecA gene.
Conclusions:
Staphylococcus aureus isolates are the major pathogens responsible for wound and surgical site infections at MUH and MRSA are a potential threat for wound patients in Egypt.
S
There are limited data examining the prevalence of MRSA among Egyptian patients after surgical interventions. In this regard, several reports examined the prevalence of MRSA among Egyptian patients with scant data among those undergoing surgery. For example, MRSA was detected in 18.9% of blood stream infections at Assuit University Hospital [3], in four of nine isolates (44%) from nosocomial infections reported in the PEARLS study [4] and in 52% in the ARMed study [5]. Also, 51% of 93 isolates, collected from blood cultures, urine, and infected wounds of patients and from the anterior nares of interns, nurses, and medical students at Ismailia General Hospital, were methicillin-resistant [6]. In addition, community-acquired MRSA was reported in four of 121 children (3%) with skin and other superficial infections [7] and in 58% of 60 opioid addicts in Egypt [8]. These data suggest that there is a need to examine MRSA prevalence among wound patients to determine if MRSA is a potential hazard to Egyptian patients undergoing surgical procedures. Importantly, there is a continuous need to monitor the prevalence and changes in the antimicrobial susceptibility patterns of S. aureus as well as other organisms that cause surgical complications for a better management of the patients [9]. Prevalent worldwide, MRSA is an important cause of nosocomial infection, resulting in increased morbidity and mortality in the hospital settings worldwide [10]. Because of the major role of staphylococci as a cause of nosocomial infections, this study was conducted to determine the prevalence of S. aureus in skin and soft tissue infections (SSTIs) among patients at Minia University Hospital (MUH) and determine their susceptibility patterns to β-lactams and other antimicrobial groups. Another objective of the present study was to determine the prevalence of MRSA among the isolates and also examine the possible genetic origin of methicillin resistance of these MRSA isolates.
Patients and Methods
From November 2007 until August 2010, a total of 208 subjects (143 males and 65 females) of different age groups ranging from two months to 79 years were enrolled into the study. The study protocol was approved by the Dean of Faculty of Medicine and the director of MUH and each subject consented prior to participation in the study. Parents of children included in the study approved their participation. The mean age (±SD) of the study subjects was 44.4±15.8 yr. Sterile swabs were used to collect the samples from hospitalized patients in the General Surgery Department at MUH. Specimens were selected randomly from different infected skin and soft tissues sites; surgical site infection (SSI; n=82), diabetic foot (n=52), abscess (n=45), and burn (n=29).
Bacterial identification
Collected swabs were cultured on mannitol salt agar (Becton Dickinson, Franklin Lakes, NJ) and nutrient agar (Oxoid, England) then incubated at 37°C for 24 h and examined microscopically using gram stained smears. The cultures were characterized, and sub-cultured for separation of mixed colonies on mannitol salt agar and blood agar. Catalase and coagulase tests were performed for identification of all the isolates following standard procedures [11].
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed on Mueller-Hinton agar (Oxoid Ltd., Basingstoke, United Kingdom). The minimum inhibitory concentrations (MICs) were determined by agar dilution method according to the guidelines of the Clinical Laboratory Standards Institute (CLSI) [12] to determine the sensitivity and resistance of the isolates to β-lactams and other antimicrobials. An antimicrobial susceptibility test for MRSA was done by disk diffusion method using oxacillin disks [13] and confirmed by MIC testing. The following antimicrobial agents were used: Ampicillin and chloramphenicol; amoxicillin and cefotaxime; oxacillin, ampicillin/sulbactam, ciprofloxacin, ofloxacin, gatifloxacin, levofloxacin, clindamycin, and tetracycline (Sigma, USA); cephalexin, and cefuroxime; cefoperazone, cefepime; amoxicillin/clavulanic acid; gentamicin; amikacin; norfloxacin and vancomycin; erythromycin; and rifampicin. Disc diffusion test was also used as a confirmatory test for oxacillin resistance as described [14] with an inhibition zone ≤10 mm indicating oxacillin-resistance, ≥13 mm indicating oxacillin-sensitivity and 11–12 mm, intermediate resistance.
Detection of mecA gene by polymerase chain reaction (PCR)
This test was performed to detect the mecA gene among the isolates of the study. The primers used in the PCR had the following sequence: Forward primer: 5′ TAG AAA TGA CTG AAC GTC CG 3′ and Reverse primer: 5′ TTG CGA TCA ATG TTA CCG TAG 3′ (Midland Certified Reagent Company, Midland, TX). The primers correspond to nucleotides 179 to 198 and nucleotides 332 to 312 of the mecA gene, respectively, thus yielding an amplicon of 154bp [15]. Deoxyribonucleic acid (DNA) extraction and experimental protocol was performed as recommended by the manufacturer (Fermentas, Thermo Fisher Scientific, Waltham, MA). After initial denaturation at 95°C for five minutes, the samples were subjected to 30 cycles of denaturation at 95°C for one minute, annealing at 47°C for 30 seconds and extension at 72°C for 30 seconds. A final extension step was performed at 72°C for five minutes. Following PCR, aliquots of the reaction mixtures were analyzed by electrophoresis on a 2% agarose gel containing ethidium bromide (0.2mg/ml), in the presence of a 100-bp ladder (Fermentas) as a DNA molecular weight marker.
Results
Isolation and identification of S. aureus isolates
In this study, we identified 241 staphylococcal species that represented the most common isolates (64.8%) among the 371 collected strains from the 208 patients. Out of the 241 staphylococcal isolates, 127 were S. aureus (61% of the total patients). The collected data (Fig. 1) show that the highest prevalence of S. aureus was observed in diabetic foot ulcers (75%; 39 isolates) followed by surgical site infection (58.5%; 48 isolates) and abscess infections (55.6%; 25 isolates) then burn discharges (51.7%; 15 isolates). On the other hand, the prevalences of MRSA (as determined below) among SSI, diabetic foot, abscess, and burn patients were 15.8%, 17.3%, 13.3%, and 10.3%, respectively (Fig. 1). The 31 MRSA isolates represent 15% prevalence among the 208 patients.
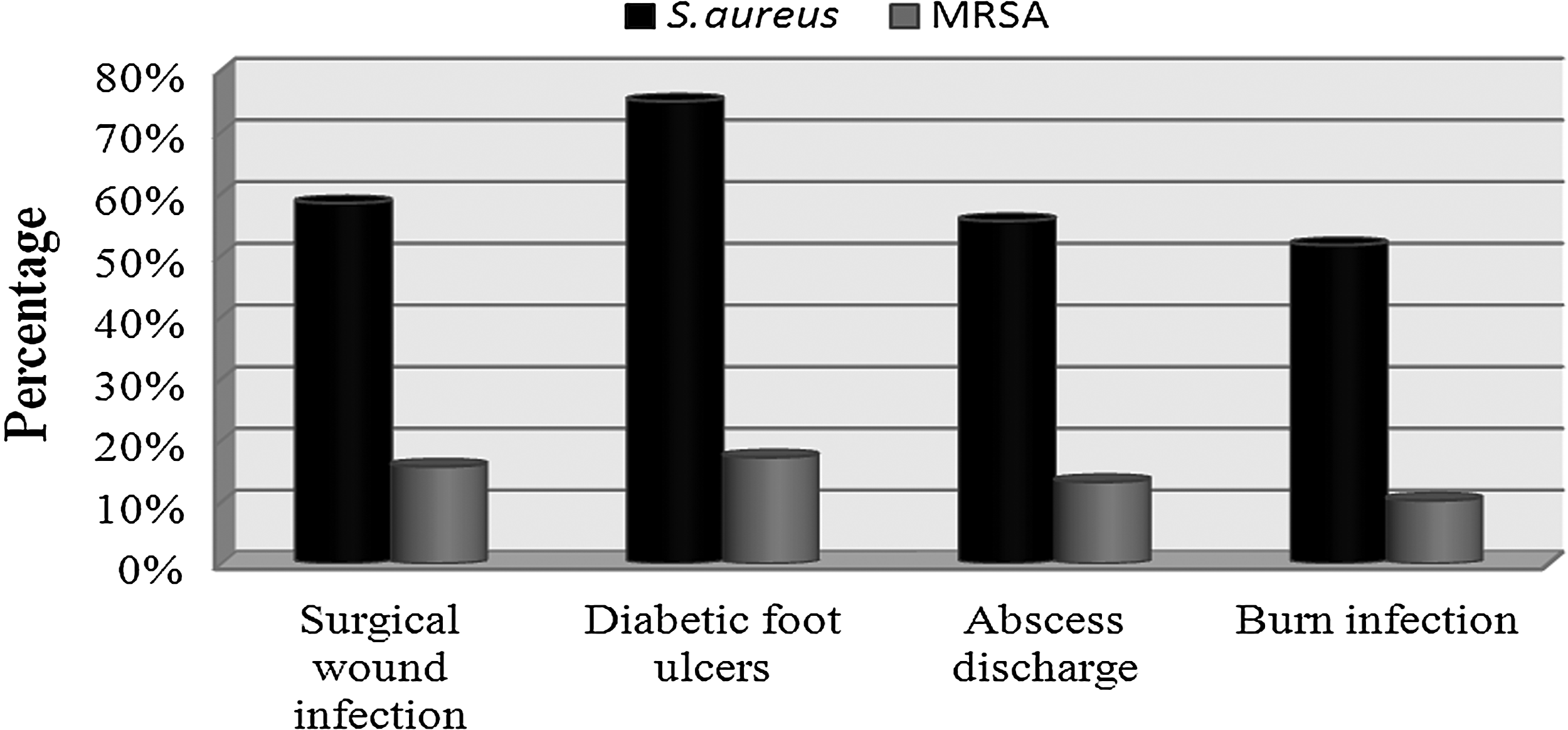
Prevalence of staphylococcal and MRSA species isolated from patients suffering from different wound infections at Minia University Hospital (MUH) (surgical site infection [n=82], diabetic foot [n=52], abscess [n=45], or burn [n=29] infections).
Antibiotic susceptibility of S. aureus isolates
It is important to monitor the sensitivity of the bacterial strains causing soft tissue infection in the local settings of MUH for the better management of the patients. Therefore, the identified S. aureus isolates were tested against a panel of different antimicrobial agents representing the different antimicrobial groups as described in the Patients and Methods section. The 127 S. aureus isolates showed moderate resistance to oxacillin (24%), cefotaxime (25%), ampicillin-sulbactam (29%), amoxicillin/clavulanic acid (32%), cefoperazone (34%), cefepime (44%), and cefuroxime (53%). On the other hand, these isolates exhibited high resistance to ampicillin (87%), amoxicillin (82%), and cephalexin (65%). The lowest resistance was to vancomycin (1.5%), amikacin (2%) and gatifloxacin (4%). Table 1 shows the resistance profile, MIC90 and MIC50 to β lactams and other antimicrobial agents. Methicillin resistant S. aureus isolates (MRSA) were 31 of these 127 isolates (24%).
The S. aureus isolates collected from 208 wound patients at Minia University were tested for their resistance to different antimicrobial agents shown
MIC=minimum inhibitory concentration.
Resistance profile of methicillin resistant S. aureus to β-lactams and other antimicrobials
It was important to determine if the MRSA isolates, from patients at MUH, were, also, resistant to other antimicrobial agents. In this regard, the 31 MRSA isolates showed absolute resistance to ampicillin and amoxicillin (100%; Table 2). High resistance were recorded to amoxicillin-clavulinic acid (87%), cephalexin (84%), ampicillin-sulbactam (81%), cefoperazone (77%), cefotaxime (74) cefuroxime (74%), erythromycin (70.9%), tetracycline (90.3%), clindamycin (67.7%), and chloramphenicol (61.3%). Table 2 shows the resistance profile, minimum inhibitory concentration (MIC)90 and MIC50 of MRSA isolates to β lactams and two other antimicrobial groups. As shown, as with the overall 127 S. aureus isolates, the lowest resistance of MRSA isolates was to vancomycin (3%), amikacin (10%) and gatifloxacin (7%). Interestingly, most of the MRSA isolates (n=31) showed multiple drug resistance to at least one member of the antimicrobial groups tested with an average resistance to 6.6±1.9 groups of the nine antimicrobial groups tested (Table 3).
The 31 methicillin resistant S. aureus isolates collected from 208 wound patients at Minia University were tested for their resistance to different antimicrobial agents. The percentage of sensitive, intermediate sensitive and resistant isolates, the MIC50 and MIC90 are shown.
MIC=minimum inhibitory concentration.
R: Resistant, S: Sensitive, I: Intermediate sensitive
The 31 methicillin resistant S. aureus isolates collected from 208 wound patients at Minia University were tested for their resistance to different antimicrobial agents as described in the Patients and Methods section. The resistance profile for each isolate is shown.
PCR detection of mecA gene in MRSA isolates
To test the genetic mechanism of resistance of MRSA isolated in this study, we examined the presence of mecA gene that confers resistance of the isolates using the PCR technique as described in the Patients and Methods. An amplicon of 154bp was considered indicative for the presence of mecA gene. An example of the PCR detection of mecA is shown in Figure 2. The overall PCR data showed that 29 isolates of the 31 MRSA isolates (93.5%) were positive for the presence of mecA gene whereas only two isolates (6.5%) were negative.
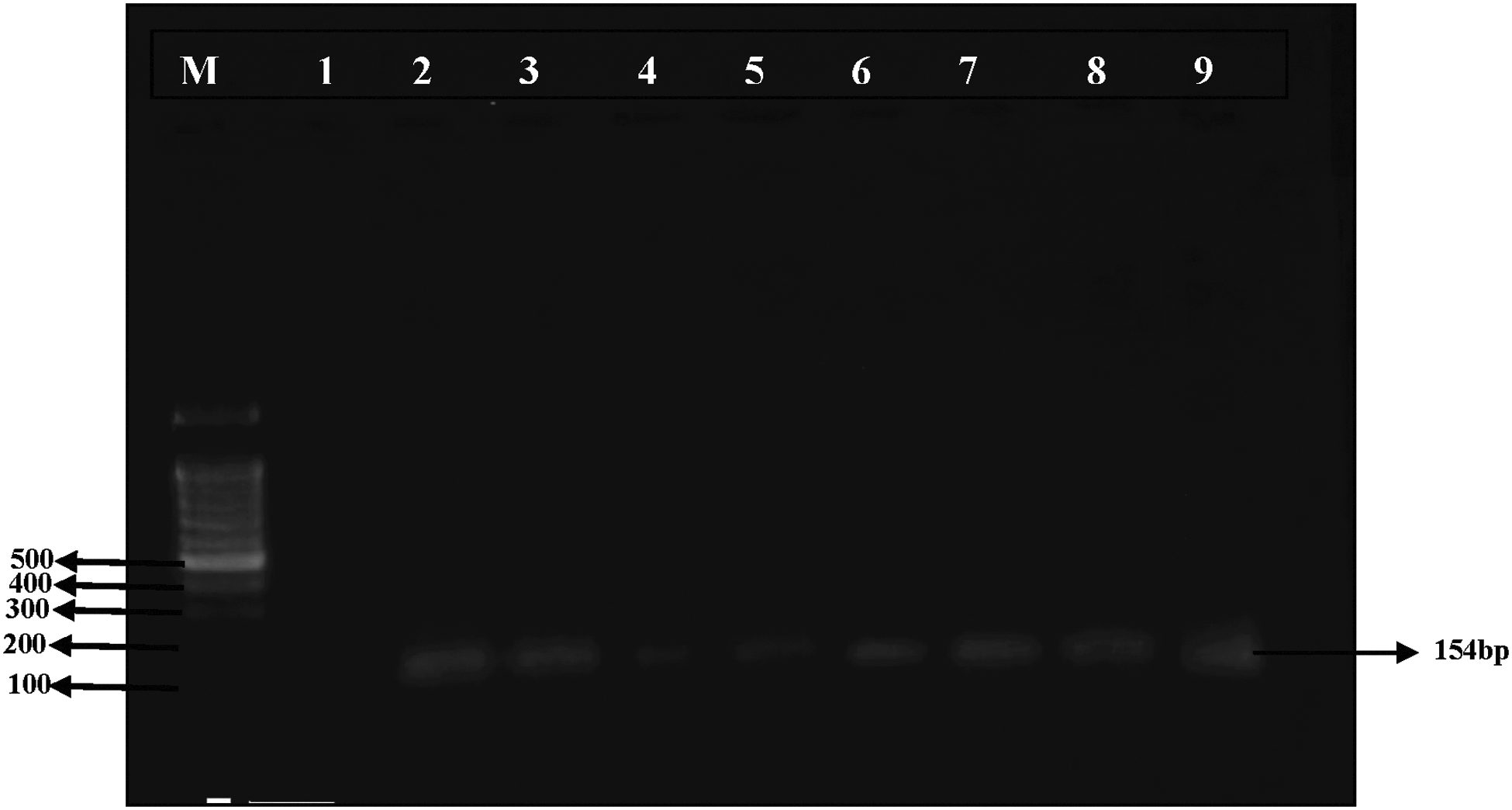
Detection of amplification products of MRSA mecA gene by PCR. PCR amplification of mecA gene was carried out as described in the Subjects and Methods section. The lanes shown are as follows: M: 100-bp ladder; lane 3-9 are mecA positive samples while lane 1 is negative control and lane 2 is positive control.
Discussion
In this study, we showed that staphylococcal species represented the most common isolates (64.8%) from 208 SSTIs patients at MUH. Out of the 241 staphylococcal isolates, 127 were S. aureus, of which 31 were MRSA. The prevalences of S. aureus among SSI, diabetic foot, abscess, and burn patients were 59%, 75%, 56%, and 52%, whereas those of MRSA (n=31; 15%) were 15.8%, 17.3%, 13.3%, and 10.3%, respectively. The MRSA isolates showed multiple drug resistance to at least one member of the nine antimicrobial groups tested with an average resistance to 6.6±1.9 antimicrobial groups. The PCR data showed that 29 of the MRSA isolates (94%) were positive for mecA gene. Several aspects of these data warrant further discussion.
We showed that S. aureus was highly prevalent among SSTI patients at MUH (>50%). In this regard, the common gram-positive organisms isolated from wound amd soft tissue infections were S. aureus, hemolytic streptococci and S. pyogenes [16]. Several studies [16–19] revealed that S. aureus was among the common pathogens isolated from surgery patients with signs and symptoms indicative of surgical site infections. On the contrary, the frequency of S. aureus reported in the present study was higher than that reported by others [20–22], in that S. aureus represented only 22–25% of swabs from wound and SSTIs infections.
The S. aureus isolates reported in this study were completely resistant to ampicillin and amoxicillin (100%), and these results are similar to the other findings [23], where S. aureus isolates were 97% resistant to ampicillin. In another report, 80.5% of S. aureus isolates were resistant to ampicillin [24], a rate that is close to our data. The present study suggested differential resistance rates against cephalosporins; where the isolates were resistant to cephalexin, cefuroxime, and cefoperazone at rates of 65%, 53%, and 34%, respectively. These rates are lower than that of another report [25] that showed resistance rates against cephalexin and cefuroxime of 98% and 89%, respectively. On the other hand, lower resistance rates (compared with ours) to cephalexin (17%) and cefuroxime (33%) were reported [26]. In regard to cefotaxime, 27% resistance rate was demonstrated [27], which is similar to ours (25%). It was reported that cefotaxime and amoxicillin-clavulanate remained the most effective single agents [28]. These two agents also had a low resistance in our study (∼30%).
A major hospital pathogen in human medicine [29], MRSA is the main cause for various infections throughout the world as it responsible for many community-acquired, endemic and epidemic nosocomial colonization and infections, and is of concern not only because of its resistance to methicillin but also because it is resistant generally to many others chemotherapeutics [30]. As mentioned previously, there are limited data examining the prevalence of MRSA among Egyptian patients after surgical interventions. The rate of MRSA in our study (24% of the S. aureus isolates) was lower than that of several reports showing a 50–68% resistance to methicillin [31–35]. However, similar rates of methicillin resistance were reported by other studies [27, 36]. Also, a lower methicillin resistance rate was reported [37]. There was no significant difference in susceptibility of MRSA (7.7%) and MSSA (8.7%) for tested β-lactams [38], whereas the pattern of antibiotic susceptibility differed significantly between MRSA and MSSA isolates. Multiple-drug resistance was common and only few antibiotics were active against these isolates [37], and this was similar to our findings. We showed that MRSA isolates were resistant to multiple drugs with resistance to at least one member of the antimicrobial groups tested with an average resistance to 6.6±1.9 antimicrobial groups. In this regard, MRSA were 100% resistant to penicillin, ampicillin, and amoxicillin; 97.8% were resistant to cephalexin; and 88.9% to cefotaxime [25]. These resistance rates were similar to ours. Altogether, multi-drug resistant MRSA is a potential health hazard to Egyptian patients undergoing different surgical procedures.
In this study, PCR was used to detect mecA gene in the 31 MRSA isolates. Twenty-nine isolates (93.5%) were positive for mecA gene whereas two isolates (6.5%) were negative. These two isolates were resistant to oxacillin at the borderline of the inhibition zone and were thus termed “moderately resistant S. aureus (MODSA).” This finding agreed with the published data [39] that showed that out of 15 MRSA isolates, 13 MRSA isolates expressed mecA gene by PCR typing in addition to beta lactamase enzyme production. This is, also, in agreement with another study [40] that reported that resistance in S. aureus mainly involves two mechanisms for the expression of β-lactamase and mecA gene. Methicillin resistance in staphylococci is mediated by the mecA gene, which encodes for the penicillin-binding protein 2A (PBP2A) resulting in reduced affinity for the β-lactam antibiotics including the penicillinase-resistant penicillins. Regarding the presence of mecA gene among the resistant isolates, a report showed that 32 MRSA isolates were initially identified by disk diffusion method, then the PCR confirmed that only 30 isolates (93.8%) were positive for the presence of mecA gene [41]. These data are similar to ours. However, a more recent study showed that all MRSA isolates (n=32) contained the mecA gene [42]. From the above data, we speculate that the two isolates that were negative for mecA gene had other resistance mechanism(s) (e.g., reduced drug accumulation or altered target site). Another possibility is that we could not detect the mecA gene by the used methodology.
In summary, this study shows that staphylococcal isolates are the major pathogens responsible for soft tissue infections at MUH, and the isolates showed high resistance to β-lactams. Multi-drug resistant MRSA isolates found at MUH and other localities in Egypt is one of the most important problems for the control of wound infections. mecA gene was responsible for methicillin resistance in ∼94% of the MRSA isolates. In conclusion, S. aureus isolates are the major pathogens responsible for wound infections and MRSA is a potential threat for wound patients in Egypt. Our data suggest that amikacin, gatifloxacin, and vancomycin are currently the best treatment available for MRSA strains in our community.
Footnotes
Acknowledgments
We thank the staff members of Surgery Department at Minia University Hospital for helping with the collection of samples. Also, we thank Prof. M.A. Elrehany (Biochemistry Department, Minia Faculty of Medicine) for his help with the PCR testing.
Author Disclosure Statement
No competing financial interests exist. All authors of this manuscript have nothing to declare regarding the data presented in this study. This study was supported by funds from Minia University and personal funds.