
Abstract

A 64-
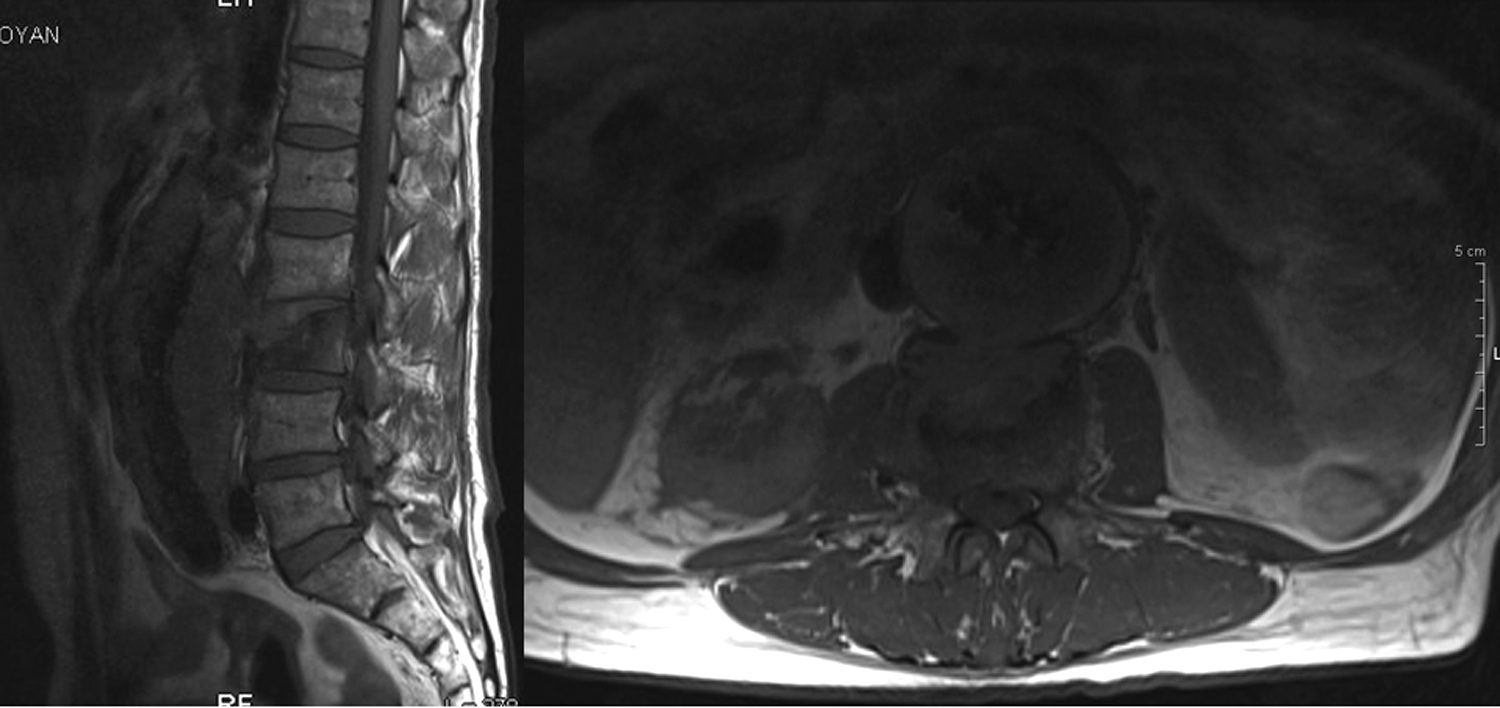
Sagittal (left) and axial (right) T1-weighted magnetic resonance (MR) images of the lumbar spine show pathologic signal intensity and wedging of the L3 vertebral body, and continuous abnormal soft tissue of similar signal intensity extending from the posterior aneurysmal sac to L3 vertebral body. The aortic lumen, within the mass, is irregular, with flame-shaped areas of pointing contrast suggesting inflammatory infiltration into the aortic wall.
Infection of an abdominal aorta endovascular graft is rare, ranging from less than 1% to 6%. Continuous spread of the infection to the spine is even more rare [1,2]. Endovascular grafts may be infected by hematogenous spread from a distant source such as the urinary tract, contamination at initial implantation, from an aorto-enteric fistula, or by microorganisms from the native arterial thrombus or arteriosclerotic plaque. The majority of infections occur from bacterial contamination of the peri-graft space at the time of original graft placement, or during subsequent endovascular procedures. The most common causative organisms are Staphylococcus aureus and Escherichia coli [1,2]. Consideration of laboratory, imaging studies, and cultures is important for the diagnosis.
Computed tomography is the study performed most commonly for the assessment of the entire endovascular graft. Both intravenous and oral contrast media may be necessary to identify the graft lumen and the relation to adjacent structures [3]. Computed tomography has a sensitivity greater than 95% and specificity in the range of 85% when the criteria of peri-graft fluid, peri-graft soft tissue attenuation, ectopic gas, pseudoaneurysm, or focal bowel wall thickening are used [4]. However, in the early post-operative period, it may be difficult to distinguish graft infection from normal post-operative changes with CT. Peri-graft air is not pathognomonic of graft infection until 4–7 wks after surgery, and peri-graft fluid may be present without infection up to 4 mo after surgery [5]. Magnetic resonance imaging is more accurate than CT for the diagnosis of intra-abdominal graft infections because of its superiority for discrimination of tissue planes, particularly in the retroperitoneum, and greater sensitivity in the detection of small amounts of peri-graft fluid. Magnetic resonance imaging may differentiate peri-graft fluid and inflammatory changes of surrounding structures from acute and chronic hematoma, and reconstruction of multiple tissue planes is performed more easily [3]. Radioisotope scans with labeled leukocytes or immunoglobulin may confirm the presence of infection and outline its extent. Indium is considered more accurate than gallium because of greater background levels caused by nonspecific intestinal uptake of gallium. However, false-positive studies are common in the first 3–4 mo post-operatively because of normal peri-graft inflammation [5]. Arteriography is of limited value for the diagnosis of vascular graft infections because of false-negative results when native vessels are not involved in the infectious process. Sinography may demonstrate communication with the prosthetic graft, however, a negative study does not preclude the presence of infection. Gastrointestinal endoscopy should be considered in any patient with a gastrointestinal bleeding source after aortic grafting for the possibility of an aortoenteric fistula [5]. Computer tomography-guided aspiration cultures may document the occurrence of infection. However, a negative result, especially when obtained with a fine-needle biopsy does not exclude infection. Surgery is the treatment of choice for patients with infected endovascular grafts. Spondylitis is usually treated non-operative; if spinal stability is compromised, a spinal stabilization procedure should be considered. If the patient's condition allows, infected grafts should be explanted, necrotic soft tissue should be debrided, and appropriate vascular reconstruction with graft replacement or extra-anatomical bypass should be performed [1,2]. Endovascular procedures may be an option, however, they have been associated with a substantial risk of complications (40%) compared with open vascular surgery (8%). The high mortality associated with open and endovascular surgical procedures is the main indication for non-operative management of infected endovascular grafts with percutaneous drainage of abscess, and long-term antibiotics [1–5].