
Abstract
Abstract
Background:
Gastrointestinal mucormycosis is associated with high mortality rates. Appropriate and early antifungal therapy and prompt surgical intervention are essential.
Method:
Case report and literature review.
Results:
Nineteen case reports were reviewed describing adults with hematologic malignant tumors who developed intestinal mucormycosis and underwent surgery. The overall survival rate was 50%.
Conclusion:
Intestinal mucormycosis is an infection associated with a high mortality rate although adults with underlying hematologic malignant have improved outcomes compared with other groups.
G
Case Report
A 41-year-old male with acute lymphoblastic leukemia (ALL) 98 d status-post bone marrow transplant (BMT) presented with lower GI bleeding. Medical history included recurrent Clostridium difficile colitis and atrial fibrillation. Surgical history included a low anterior resection (LAR) and radiation for T3N1 rectal cancer seven years prior. The patient was taking prednisone (5 mg QD), voriconazole (200 mg BID), chlorothiazide (250 mg QD), acyclovir (400 mg BID), furosemide (20 mg BID), famotidine (20 mg BID), tacrolimus (1 mg BID), morphine sulfate controlled-release tablets (15 mg BID), and atovaquone (750 mg/mL oral suspension 10 mL QD), all by mouth.
In the emergency department he presented with hematochezia. Hemogram demonstrated a white blood cell count of 8.9×109cells/L (absolute neutrophil count 7.7), hematocrit of 21% and a platelet count of 112,000 109cells/L, and we initiated the massive transfusion protocol after he became unstable hemodynamically. After transient stabilization, computed tomography (CT) angiogram demonstrated active extravasation into the sigmoid colon with a fistula to the left common iliac artery (Fig. 1). Angiogram confirmed the common iliac artery (CIA)-to-sigmoid colon fistula. A 10 mm x 38 mm covered Atrium iCAST™ balloon-expandable stent (Hudson, NH) was deployed (Fig. 2). Completion angiogram demonstrated a patent common iliac artery with no further bleeding. Active resuscitation continued with 36 U of red blood cell concentrates, 26 U fresh frozen plasma (FFP), 7 U platelets, and 4 L of crystalloid transfused. Blood cultures on admission and hospital day (HD) four and five, and urine cultures on HD five, were negative. Repeat CT scan on HD five demonstrated persistent pneumatosis of the sigmoid colon and focal stenosis within the stent. Stent revision was performed given the focal high-grade stenosis. A 10 mm x 10 cm GORE Viabahn® stent (Flagstaff, AZ) was placed within the previous iCAST stent. Flexible sigmoidoscopy on HD seven demonstrated mucosal irregularity, diminished vascularity, pigment alterations and mucosal surface irregularities 20 to 25 cm from the anus. Biopsies showed branching, non-septated, fungal hyphae with invasion of surrounding tissue. Periodic acid-Schiff (PAS) and elastic Van Gieson stains did not demonstrate definitive vascular invasion. After fungal stains were available, the patient was started on amphotericin B (AmbB) lipid complex 400 mg IV every 24 h, caspofungin 150 mg IV every 24 h, and posaconazole 800 mg TID dosed according to concentrations. Tissue polymerase chain reaction (PCR) later revealed the organism to be a Rhizopus spp.

Computed tomography (CT) angiogram of left common iliac-to-sigmoid colon fistula showing active extravasation in saggital view (H). The patient's head is toward the top of the photo and his pelvis is at the bottom (F). Left is anterior (A).

Angiogram showing left common iliac fistula to sigmoid colon. The arrow points to the fistula. The patient's head is toward the toward the top of the photo and his pelvis is at the bottom.
After a multi-disciplinary meeting involving the patient and family, the decision was made to proceed with colon resection as the predicted risk of death without an operation was near 100%. As the CIA-covered stents could be a source of persistent infection, removal was planned along with revascularization. On HD 12 ileocectomy and completion colectomy, ileostomy, iliac stent removal and femoral–femoral bypass were performed. The bypass was performed first via separate incisions to provide blood flow to the left lower extremity and avoid inline left common iliac reconstruction. Contained anterior perforation of the patient's descending colon was noted at the region of the fistula, and the ascending colon was necrotic. Colon was resected down to the prior LAR colorectal anastomosis. The CIA, external iliac artery, and internal iliac artery were divided and diseased vessels and stents were removed (Fig. 3). Left nephrectomy was performed as the left kidney was noted to be boggy, congested, and the ureter was dilated with purulent fluid therein. The patient became coagulopathic and the abdomen was closed temporarily. End-ileostomy creation, AmbB abdominal irrigation, and abdominal closure occurred on HD 14. By HD 16 the patient was stable and transferred to the bone marrow transplant unit.
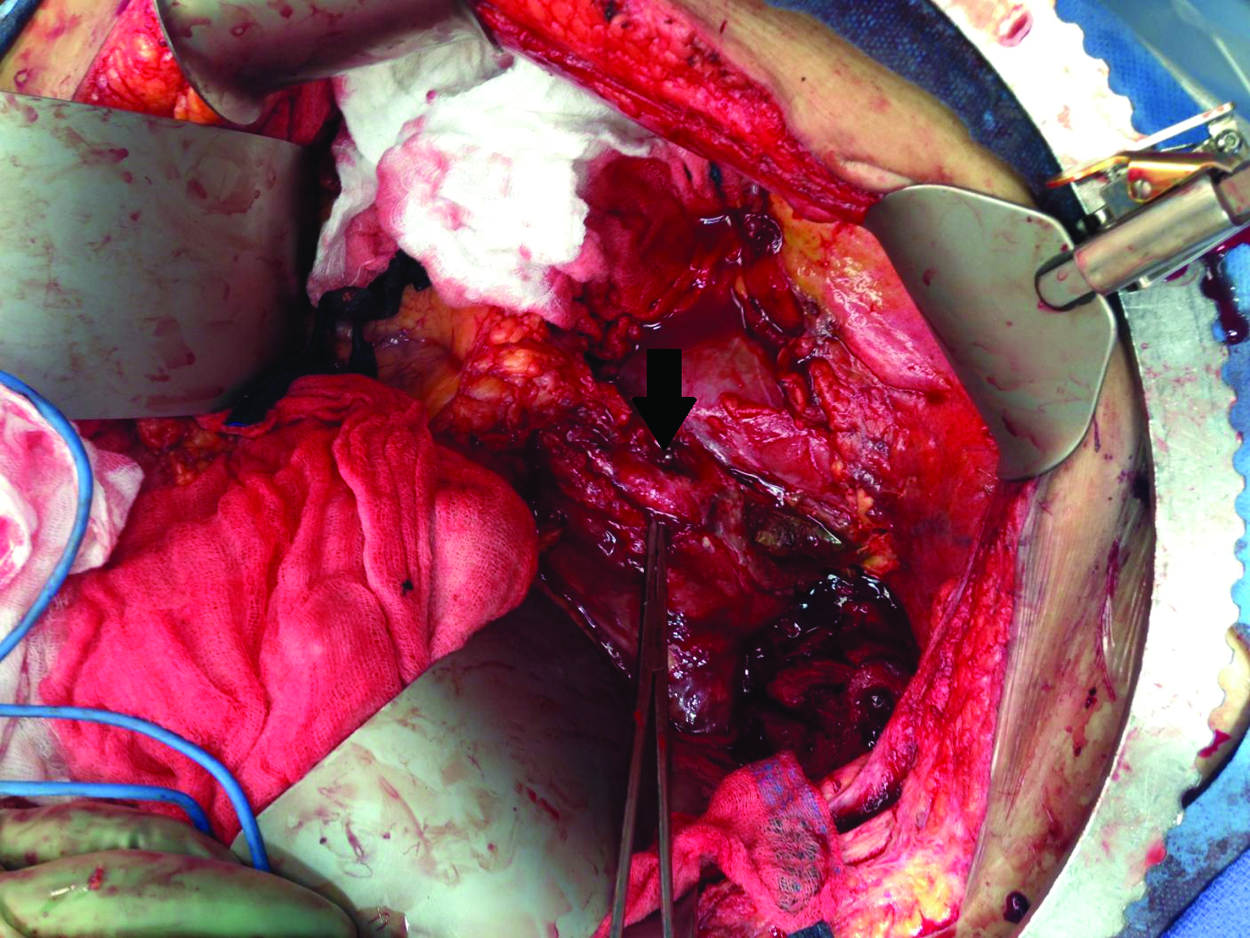
Left common iliac artery involvement by mucormycosis. The arrow points to a right angle clamp encircling the artery with exposed stent. The patient's head is toward the top of the photo and his pelvis is at the lower edge. Color image is available online at www.liebertpub.com/sur
Pathologic evaluation of the colon and ileum revealed extensive ulceration and necrosis with fungal hyphae, with extension into the left kidney and common iliac artery. Sequence analysis of D2 and ITS regions using the ABI PRISM® 3100 Genetic Analyzer (Grand Island, NY), and comparison to the CBS-KNAW© (Utrecht, The Netherlands), and Genbank® (Bethesda, MD) databases confirmed a Rhizopus spp. A Rhizopus spp. with the following anti-fungal minimum inhibitory concentrations (MIC) by broth microdilution was obtained after culture: AmbB B 0.5 mcg/mL, itraconazole 0.5 mcg/mL, posaconazole 0.5mcg/mL, and voriconazole 4 mcg/mL. No further speciation was performed. Blood cultures on HD 19 revealed no growth. On HD 45, a seroma was noted in the right groin and after exploration and AmbB irrigation, this wound was covered with a pedicled rectus femoris flap. Operative cultures did not demonstrate hyphae.
The patient was transitioned to a triple anti-fungal regimen: AmbB lipid complex 12.5 mg/kg every 48 h, caspofungin 150 mg IV every 24 h, and posaconazole 600 mg po QAC and QHS. Two months later graft-versus-host disease (GVHD) prophylaxis consisting of prednisone 20 mg po daily and mycophenolate mofetil 500 mg po G12H was restarted. Gastrointestinal function returned and he was discharged home 53 d after his initial operation with plans to continue triple anti-fungal therapy for one year.
Literature Review
Given the paucity of information regarding outcomes after surgery for gastrointestinal mucormycosis in adults with a hematologic malignant tumor, we performed a literature review. A PubMed search was performed using the following terms: Gastrointestinal, stomach, colon, small intestine, rectum, ileum, jejunum, stomach, duodenum, zygomycosis, mucormycosis, malignancy, Mucorales, and Rhizopus. Inclusion criteria included all English-language articles in peer-reviewed journals after 1980 describing patients with gastrointestinal mucormycosis, a hematologic malignant tumor, and who underwent surgery. Exclusion criteria included transplant patients or patients less than 18 y of age. References in all papers were evaluated for additional cases. The studies were evaluated for the following parameters: Age, gender, tumor type and associated chemotherapy, pre-existing neutropenia, other co-morbidities, whether voriconazole was used for prophylaxis, number of days from admission to surgical intervention, symptoms before surgery, operation performed, number of re-operations performed, the infecting organism, other co-infecting organisms, the primary focus of infection, anti-fungal regimen, and survival data.
Nineteen published cases met inclusion and exclusion criteria [7–21] (see Table 1). Median age was 48 y (range, 21 y to 61 y) and 50% of patients were male. The ileum and cecum (11/20) were the most common sites of infection, followed by the descending colon and sigmoid colon. The most common associated tumor was ALL (9/20) followed by acute myelogenous leukemia (AML) (6/20). Fifty percent (10/20) of patients survived to discharge or the end of followup; of these, six (30%) were followed for 6 mo or more.
c ara-C=cytarabine; A=asparaginase; CA=cytosine arabinoside; clo=clofarabine; cyc=cyclophosphamide; d=daunorubicin; Dexa=dexamethasone; ida=idarubicin; met=methotrexate; P=prednisolone; pred=Prednisone; T=thioguanine; tac=tacrolimus V=vincristine.
Discussion
Originally reported as a cause of human disease in 1885, fungi of the class Zygomycetes, order Mucorales, are ubiquitous in nature [3,5,22]. The most common Mucorales are of the genera Rhizopus, Lichtheimia [23–25] and Mucor, with Rhizopus oryzae being the most common human pathogen (>70%) [3,5,24–26]. Acute angioinvasive disease typically occurs in five locations: Rhino-orbital cerebral (44%–49%), pulmonary (10%–11%), disseminated (6%–12%), cutaneous (10%–16%) and gastrointestinal locations (2%–11%) [2,3]. Despite the infrequency of gastrointestinal mucormycosis the consequences of an infection in the abdomen can be devastating with mortality rates as high as 85%–90% [1,4]. Although surgeons are unlikely to be the primary team responsible for these patients' care, it is essential to understand expected outcomes in order to provide appropriate recommendations to the primary team and patient-care decision makers.
Although the sample size was small, there appears to be improved survival after surgery in the adult population with hematologic malignant tumors when compared with other populations who develop GI mucormycosis (50% survival vs. 15% survival) [3]. Survival among patients with GI mucormycosis in this population appears to be equivalent to that of the adult solid organ transplant population, which also has a reported 50% survival with both anti-fungal therapy and surgery [26]. Interestingly, patients who underwent surgery were more likely to have ALL than AML, which is more common in patients with mucormycosis [1].
After initial resuscitation the first goal in the management of patients with mucormycosis is to control co-morbidities and minimize immunosuppression. Corticosteroids should be stopped if possible and euglycemia and normal acid-base status attained to optimize extant neutrophil function [4]. The second goal is initiation of rapid and appropriate anti-fungal therapy. The only licensed antifungal agent for the treatment of mucormycosis remains amphotericin B deoxycholate [4,5]. Newer, lipid formulations of amphotericin B (LFABs) have a more tolerable side effect profile with less associated nephrotoxicity [5]. No studies have evaluated the efficacy of LFABs compared with amphotericin B in a GI mucormycosis model. Although posaconazole has demonstrated reliable activity against Mucorales species in vitro, dosing can be challenging and it is not recommended for primary therapy [4,5]. Echinocandins have shown promise when combined with LFAM [4]. Colistin (polymyxin E) has also been shown to have in vitro antifungal activity against Mucorales. However, after exposure to colistin, rapid re-growth of fungus has been observed upon discontinuation [27].
Appropriate and adequate surgical resection should be considered early in the management of patients with GI mucormycosis. In this review, the ileo-cecal region was the most common GI site affected. This location in patients with hematologic malignant disease presents a clinical challenge for surgeons as typhilitis and early mucormycosis appear similar radiographically [28,29]. If hemodynamically stable neutropenic patients present with abdominal pain and CT findings consistent with typhilitis, surgery is deferred typically unless perforation, obstruction, or uncontrollable GI bleeding is present. By contrast, surgical intervention should be prompt and aggressive if mucormycosis is suspected given the predilection for local tissue destruction and angioinvasion. This therapeutic dilemma highlights the need for surgeons to collaborate closely with the primary teams caring for these patients.
Definitive diagnosis of zygomycosis is dependent upon histopathologic, cytopathologic, or direct microscopic evaluation of affected tissue and organs [26]. There are no circulating antigen tests and testing for 1,3 β-D-glucan is generally negative; biologic specimens from clinically involved sites are required for diagnosis [5]. All surgical specimens should undergo fungal stain and culture, which when combined increase diagnostic yield 15%–20%; care should be taken to avoid crushing fragile Zygomycetes [10,30]. Blood cultures are of no benefit when evaluating for Zygomycetes as they are almost always negative (as in the presented case) and should raise suspicion of contamination [5,26]. Key findings on direct microscopy and histopathology include thick-walled, refractile hyphae 6–30 microns in diameter with wide-angle (∼900) branching; these findings must be considered important even if culture is negative [10]. Culture is challenging and the minimum incubation time is three to five days, so anti-fungal therapy should not be delayed while awaiting culture results [31].
This study has two major limitations. As this is a retrospective review of published cases in patients healthy enough to undergo surgery, selection bias is present. Second, small sample size limited comparisons of variables of patients who survived after surgery and those who did not.
Conclusion
Whereas gastrointestinal mucormycosis is rare, it has a high associated mortality rate. However, survival of adult patients with underlying hematologic malignant tumors who undergo surgery is better than that of patients with GI mucormycosis as a whole, and equivalent to solid organ transplant recipients. Whereas the majority of these patients with abdominal pain will not have GI mucormycosis, the surgical team must be aware of mucormycosis and be prepared to offer recommendations on surgical interventions and anticipated outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.