
Abstract
Abstract
Background:
The majority of infections treated by surgeons are nosocomial infections (NI). The frequency of these infections in relation to the organ operated on as well as the organisms involved are not well defined. Detailed knowledge of these issues is essential for optimal care of surgical patients. This study aimed to determine infection rates and the responsible pathogens after major elective surgery of the pancreas, liver, stomach, and esophagus.
Methods:
Between January 1, 2005 and August 31, 2007, the records of all patients of the Department of General, Abdominal and Vascular Surgery, University Hospital Magdeburg (Germany) with elective resection of the pancreas, liver, stomach, and esophagus were evaluated retrospectively. Study parameters were: Patient number, age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, indication for resection, operation duration, length of stay (LOS) in the intensive care unit (ICU) and in hospital, mortality, organ-related rate and kind of NI, and microbiologic spectrum. Nosocomial infections were defined as: Surgical site infection (U.S. Centers for Disease Control and Prevention [CDC] 1 or 2) and intra-abdominal infection (CDC 3), urinary tract infection, clinical sepsis, blood stream and catheter-related infection, respiratory tract infection, and pneumonia.
Results:
A total of 358 patients were included: 150 (42%) with pancreas resection, 91 (25%) with liver resection, 105 (29%) with gastric resection, and 12 (3%) with esophagus resection. Median LOS in the ICU for all groups was 48.8 h (interquartile range [IQR] 24.9–91.8 h), median LOS in hospital was 16 d (IQR 13–23 d), and in-hospital mortality was 4.5%. Patients with NI had significantly greater in-hospital death and prolonged stay in hospital and ICU (p<0.001). In 120 (33.5%) patients, one or more NI occurred (range, 83% in esophagus patients to 21% in liver patients). Intra-abdominal (16.5%) and surgical site infections (12.3%) were most frequent; 80.8% of the NI were culture-positive. The most frequent clinically relevant isolates were Escherichia coli (12.4%), coagulase-negative staphylococci (CoNS) (12.2%), and Enterococcus faecium (9.7%). The highest resistance rates were found for Staphylococcus aureus (methicillin-resistant S. aureus [MRSA] 29.4%) and Pseudomonas aeruginosa (23.5%).
Conclusions:
For patients undergoing elective surgery of the pancreas, liver, stomach, and esophagus, considerable differences in demographic factors, frequency, and kind of NI exist. The consequences of NI force surgeons to analyze pre-operative risk factors carefully, assess indications for operation thoroughly, and optimize all controllable parameters.
T
Patients and Methods
The records of all patients of the Department of General, Abdominal and Vascular Surgery, University Hospital Magdeburg (Germany) were evaluated retrospectively for the period from January 1, 2005 to August 31, 2007. A cohort of 414 consecutive patients with elective resection of the pancreas (n=152), liver (n=110), stomach (n=117), and esophagus (n=35) treated post-operatively in the surgical ICU was investigated. Exclusion criteria were radiotherapy or chemotherapy during the last 6 mos, previous surgery (less than 30 d), emergency case, infectious disease leading to resection, and concomitant infection.
Data collection was performed using a structured data entry form. The following study parameters were compared: Patient number, age, gender, BMI, history of smoking (smoker versus non-smoker), alcohol consumption (frequent use of alcohol versus no or rare use of alcohol), ASA classification, pre-operative stay in hospital, length of stay (LOS) in the ICU and in hospital, operation duration, in-hospital mortality, organ-related rate and kind of post-operative infection, and microbiologic spectrum.
Nosocomial (post-operative) infections were defined as: surgical site infection (U.S. Centers for Disease Control and Prevention [CDC] 1 or 2); intra-abdominal infections (CDC 3); urinary tract infection; clinical sepsis, blood stream infection, and catheter-related infection; and respiratory tract infection and pneumonia [8–10].
Microbiologic samples were obtained in case of suspicion or signs of surgical site infection (sterile swab or tissue specimen); intra-abdominal infection (sterile swab or tissue specimen or sample from drain fluids); blood stream infection or sepsis (aerobic and anaerobic blood samples from a peripheral vein), patients with remaining central venous catheter (additional aerobic and anaerobic blood or tip of central venous catheter); urinary tract infection (sampling of aseptically obtained urine); pneumonia or pulmonary tract infection (bronchoalveolar lavage [BAL] or bronchial or transtracheal secretion); infected fluid collection (sterile puncture or drainage); and gastrointestinal tract infection (stool sample).
Additionally, microbiologic screening was performed for patients staying longer than 7 d in the ICU or with signs of sepsis. This included blood and urine samples and in cases of mechanical ventilation, aspiration of bronchial secretion; and in cases of surgical site complication, incision swabs. In case of positive samples, identification and antimicrobial resistance testing were performed.
For every patient and every type of infection, only the first isolate was analyzed to avoid duplicate strains. Microbiologic data were analyzed in detail for the following pathogens: Staphylococcus aureus, coagulase-negative staphylococci (CoNS), Enterococcus faecium, Escherichia coli, Pseudomonas aeruginosa, Enterobacter spp., Proteus spp., Klebsiella spp., Bacteroides spp., Streptococcus spp., Citrobacter spp., Candida albicans, Candida glabrata, and Candida krusei. All other microbes were summarized as non-specified pathogens.
Statistical analyses were performed using Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA) und PASW Statistics 19 (IBM Corporation, Armonk, NY). Descriptive statistics were calculated as frequency, median with 25th to 75th percentile (interquartile range [IQR]), minimum, and maximum. Dependence between categorical variables of patient groups was evaluated using the Fisher exact test. Because most continuous variables had a non-normal distribution, non-parametric tests were used. For homogeneity of data between groups, Kruskal-Wallis H-test was applied. If significant, post hoc pairwise analyses via Fisher exact test or Mann-Whitney U test and Bonferroni adjustment for multiple testing were performed. All other tests were performed deliberately to the full level of significance. Statistical significance was defined as a two-tailed p value of ≤0.05.
Results
For the period from January 1, 2005 to December 31, 2007, a total of 358 patients met the eligibility criteria. The cohort included 150 (42%) patients with pancreas resection, 91 (25%) with liver resection, 105 (29%) with gastric resection, and 12 (3%) with esophagus resection. Details concerning patient characteristics are given in Table 1.
Mann-Whitney U test with Bonferroni's adjustment for multiple testing.
Fisher exact test.
Data given as median with the 25th to 75th percentile.
BMI=body mass index; ASA=American Society of Anesthesiologists; LOS=length of stay; ICU=intensive care unit.
In 120 (33.5%) patients, one or more NI occurred. Esophagus patients were affected most often (83%) and liver patients were affected the least (21%). Manifestation of two different NI occurred in 30 (8.4%) patients, three in 14 (3.9%) patients, four in four (1.1%) patients, and all five analyzed NI in one (0.3%) patient. The frequency of multiple NI differed between organ groups (p<0.001; Fig. 1).
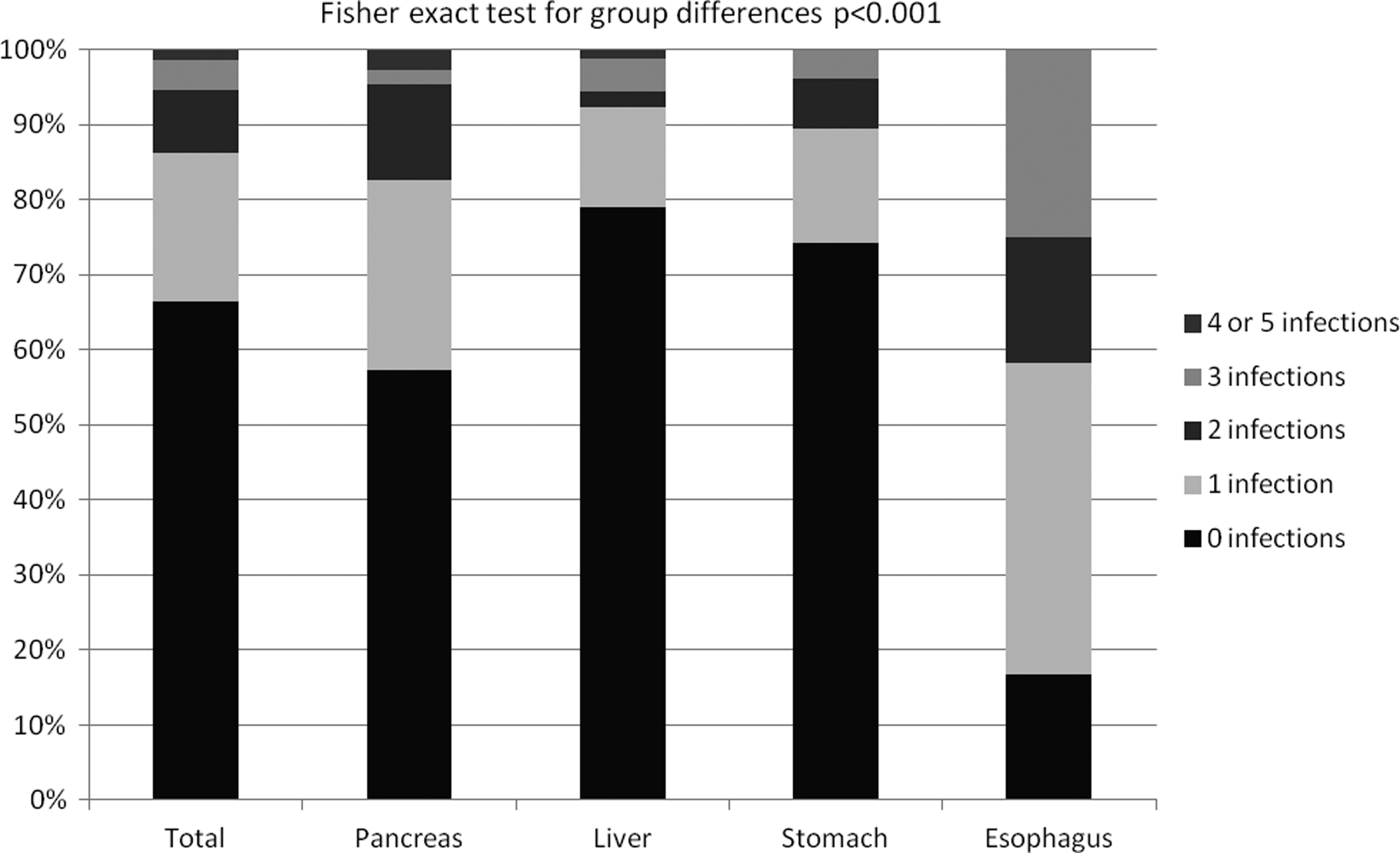
Rate of post-operative nosocomial infections. (Fisher exact test for group differences p<0.001).
Intra-abdominal infection (CDC 3) was the most frequent infection in the analyzed cohort (16.5%). The distribution of NI differed considerably between the organ groups. In liver patients, surgical site infection (CDC 1 or 2) was most common (12.1%). Blood stream or catheter-related infection occurred in 50% of patients in the esophagus group and in 15.2% in the stomach group. The leading cause of post-operative infections in the pancreas group was an intra-abdominal infection (CDC 3; 22%). Differences in the distribution of all kinds of NI were significant between organ groups. Details are given in Table 2.
Fisher exact test and Bonferroni's adjustment for multiple testing.
CDC=definition of surgical site infection according to the U.S. Centers for Disease Control and Prevention.
Occurrence of NI had a statistically significant effect on clinical outcome. With the exception of the esophagus group, NI led to an increased rate of in-hospital death and prolonged ICU and hospital stays. Detailed data are given in Table 3.
Two-tailed p for *Fisher exact test.
Mann-Whitney U test.
Data given as median with the 25th to 75th percentile.
NI=nosocomial infection; LOS=length of stay; ICU=intensive care unit.
In 27.1% of patients, at least one positive microbiologic result was found. For all isolates, E. coli (12.4%), CoNS (12.2%), and E. faecium (9.7%) were the most frequent. The highest rates of antibiotic-resistant isolates were found for S. aureus (29.4% MRSA) and P. aeruginosa (23.5% ciprofloxacin-, imipenem-cilastatin, meropenem-, piperacillin-tazobactam, or ceftazidime-resistant). Fungal isolates were classified as C. albicans (8.6% of all isolates), C. glabrata (3.0%), and C. krusei (0.2%). Details are given in Table 4. Most positive isolates could be found in drains (27.4%) and incisions (16.5%; Fig. 2).
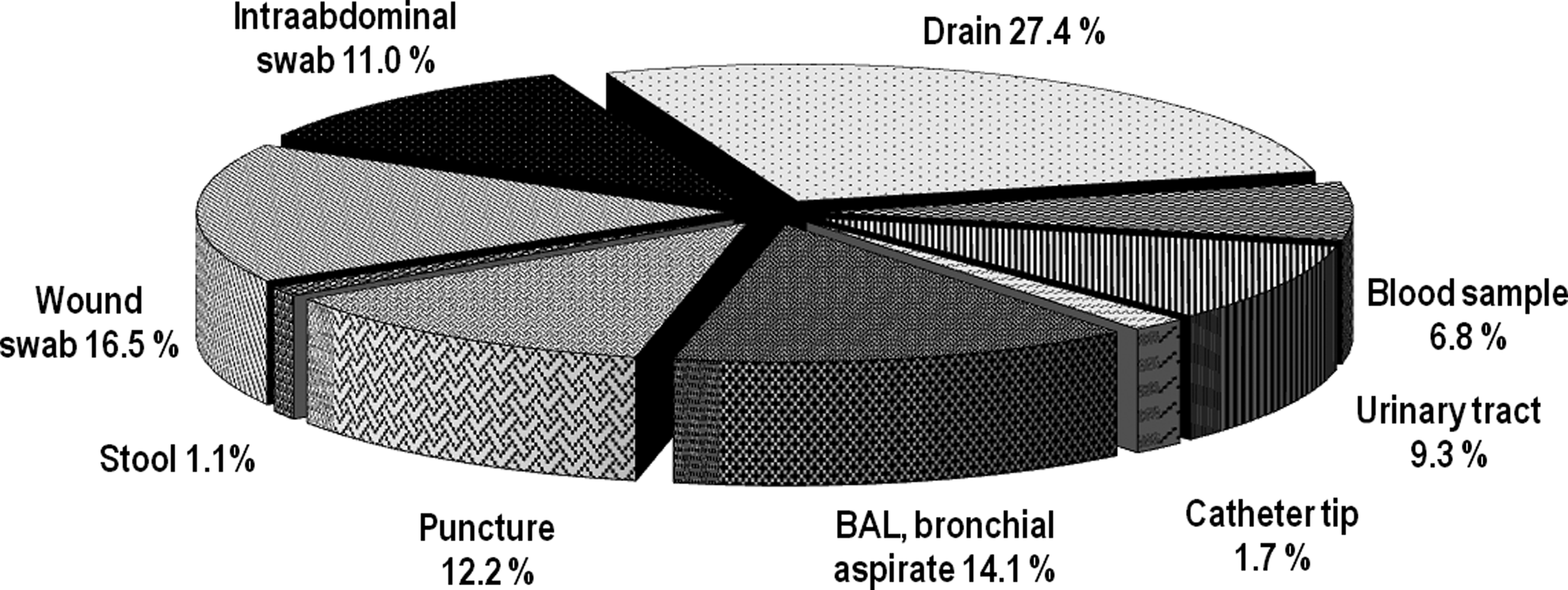
Localization of positive isolates.
Fisher exact test and Bonferroni's adjustment for multiple testing.
n=number of isolates; ABR=antibiotic resistance.
Differences between organ groups for the distribution of pathogens were only significant for P. aeruginosa (p=0.037). This pathogen occurred most often in the pancreas group (64.7%; Table 4).
Of 120 patients with NI, 97 (80.8%) had at least one positive microbiologic finding. Rates for analyzed NI were: surgical site infection, 86.4% (n=38); intra-abdominal infection, 81.4% (n=48); pneumonia and pulmonary tract infection, 81.8% (n=18); clinical sepsis, blood stream, and catheter-related infection, 97.4% (n=38); and urinary tract infection, 79.5% (n=31).
Finally, all isolates were counted individually. A variety of species isolated could be observed between the groups. In the liver group, seven gram-positive, three gram-negative, and four Candida species were found. Pancreas patients displayed the largest variety for all pathogens: 21 gram-positive, 23 gram-negative, and six Candida species. For stomach patients, 15 gram-positive, 11 gram-negative, and three Candida species were found, and for esophagus patients, six gram-positive, nine gram-negative, and one Candida species could be isolated.
Discussion
In this study, one-third of patients developed one or more NI. Even though all operations could be classified as complex, rates of NI differed from 21% for liver patients to 83% for esophagus patients. Furthermore, the distribution of types of NI differed significantly between groups. This underlines the importance of a thorough analysis of post-operative NI.
For objective comparison of surgical procedures from different specialties and of different complexity, several scores and classifications have been proposed [11–13]. Infection rates for patients with complex procedures are estimated between 2.9% and 13.0% [12]. These classifications are easy to apply but might not reflect the actual risk for post-operative complications properly. Our data presume that actual surgical site infection rates are higher. This is consistent with other data: pancreas resection, 17%–45% [2,14,15]; liver resection, 8.6%–21% [16–19]; and gastrectomy, 6.2%–16.8% [20–23]. Wu et al. [24] showed pancreatoduodenectomy and hepatectomy with resection of more than two segments being independent factors for major post-operative complications. Despite both being complex surgical procedures, the odds ratio (OR) differed notably (3.77, p=0.0006 for pancreatoduodenectomy versus 1.08, p=0.03 for hepatectomy).
Post-operative NI are important for outcome considerations after operations. We demonstrated a statistically significant effect of NI on clinical outcome. Only for the esophagus group was the sample size too small to reach significance. The increase of the in-hospital death rate is the most important issue to investigate thoroughly for NI among pre-operative risk factors. Perioperative management of NI should be as important as the surgical procedure itself. Furthermore, prolonged treatment duration caused by NI increases cost.
A number of pre-, intra-, and post-operative risk factors have been identified [3,4,12,25,26]. Many cannot be influenced prior to surgery but help in risk estimation. This seems essential because in some cases, post-operative treatment might not be helpful to prevent infectious complications [27]. To exclude some of the established risk factors, we included only patients with elective surgery undergoing complex procedures without prior radiotherapy or chemotherapy or acute infections. However, analysis of demographic factors has already displayed differences among the four groups for age, alcohol consumption, indication for resection, ASA classification, and pre-operative LOS in hospital. All of these factors might affect the incidence of NI [26].
Differences in the distribution of NI depending on the organ operated on have been published by several authors. For pancreas resection, indication for surgery (malignant versus benign disease) is probably an important factor. Chu et al. [2] found differences for intra-abdominal (13.2% versus 7.5%) and surgical site infections (23.6% versus 10.0%) in operations for adenocarcinoma of the pancreas and chronic pancreatitis, respectively. This might be caused by cancer-related immunosuppression. The rates of surgical site infections are comparable with our data (18%), but in our data intra-abdominal infections occurred more frequently (22%), even though only 55% of our patients had pancreas carcinoma. Intra-abdominal infections were mainly caused by anastomotic leakage and post-operative pancreatitis.
Clinical sepsis, blood stream or catheter-related infection, as well as pneumonia and respiratory tract infections occurred most often after resection of the stomach and esophagus. In both groups, malignancy was the only reason for resection. Patients with gastrectomy were oldest and needed the longest parenteral nutritional support. This might explain the high rate of catheter-related infection and pneumonia.
For esophagus resection, the longest pre-operative stay in hospital and the highest percentage of patients classified as ASA 3 (66.7%), as well as the longest operation time, the longest time in the ICU, and the highest complexity of surgery might explain the exceptionally high rate of post-operative infections compared with the other groups [28]. Still, we found an overall morbidity rate of approximately 80% in the small group of 12 patients compared with 50% in a large cohort of 17,395 esophagectomies from Connors et al. [5].
Surgeons must be aware of a variety of pathogens and their antibiotic resistance [7,20]. Although the sensitivity of microbiologic screening is only 46%, it is superior to clinical and laboratory findings [1]. In the present study, we found a rate of 80.8% of NI with positive culture.
We demonstrated the frequency of the most clinically relevant microbes in relation to the organ group. Group differences were only significant for P. aeruginosa. This might be because of the high rates of intra-abdominal infections in the pancreas and esophagus groups and use of intra-abdominal and intra-thoracic drains. Coagulase-negative staphylococci was most common in the stomach, pancreas, and esophagus groups, which correlated with clinical sepsis and blood stream and catheter-related infections.
A large study including 2,457 surgical infections demonstrated remarkable differences in relation to the frequency of infections, locations, and involved pathogens, as well as antibiotic resistance [6]. The most common sites were the abdomen, lung, and incisions; the most common isolates were S. epidermidis, S. aureus, and C. albicans. Eggimann et al. [26] compared infection rates and the pathogens involved for several infection surveys in ICUs. They confirmed the importance of infection location for the micro-organisms involved [26]. Blood stream infections were mainly caused by CoNS, surgical site infections by S. aureus, respiratory tract infections by P. aeruginosa and S. aureus, and urinary tract infections by E. coli and Candida spp.
The variety of pathogens in relation to the infection site presents another problem. At least two types of NI were verified in 13.7% of patients, some of them occurring simultaneously. Thus, initial antibiotic treatment should cover all relevant pathogens. Fungal infections comprised nearly 14% of all infections. This is alarming because an association of fungal infections with mortality has been reported in up to 20% of cases [29]. The highest rate of antibiotic resistance was found for S. aureus (MRSA 29.4%) and P. aeruginosa (23.5%). In 2001, Sawyer et al. [6] reported higher rates of resistant organisms in a general and trauma surgery cohort: S. aureus (49%) and P. aeruginosa (51%). However, antibiotic resistance depends on a variety of factors, e.g., manner of counting isolates, geographic location and type of hospital, location of onset of infection, type of ward, location of infection, and course of time [1,6,7,26,30,31]. In-hospital mortality ranged from 2.2% to 8.3%. This was strongly correlated to the frequency of NI and LOS in the ICU and in hospital. Comparable data have been reported for pancreas resection (1.7%–8%) [2,32–34], liver resection 1.9%–3.5% [27,35,36], gastrectomy 0.9%–6.9% [37,38], and esophagectomy 6.2%–9.8% [5,39,40]. Aust et al. [41] estimated the risk of death in relation to the complexity of surgical procedure. For patients with grade 5 (pancreatoduodenectomy) and grade 4 (esophagectomy) complexity, generic patient risk factors still contribute to operative mortality but are dominated by the issue of the complexity of the procedure. On the contrary, patient risk factors predominate over the operative intervention as a cause for operative mortality for grade 3 and lower (major biliary and gastric surgery). Duron et al. [42] analyzed the risk factors for death in major digestive surgery and found an OR of 4.48–6.5 (p<0.001) for deep incisional surgical site infections, the most frequent NI in our study.
Conclusion
For patients undergoing elective surgery of the pancreas, liver, stomach, and esophagus, considerable differences in demographic factors, frequency, and site of NI, as well as involved pathogens exist. In this context, classifications for post-operative risk estimation have their limitations and might not reflect “true” risks and outcome measures for specific procedures. Nonetheless, they are helpful for a standardized, objective, and reproducible assessment of surgical research and comparison among centers worldwide. The consequences of NI force surgeons to analyze pre-operative risk factors carefully, assess indications for operation thoroughly, and optimize all controllable parameters. The management of NI is a crucial part of surgical treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.